
What Is the Hypoplastic Left Heart Syndrome?


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. The Historical Background to the Syndrome
3. Morphological Considerations
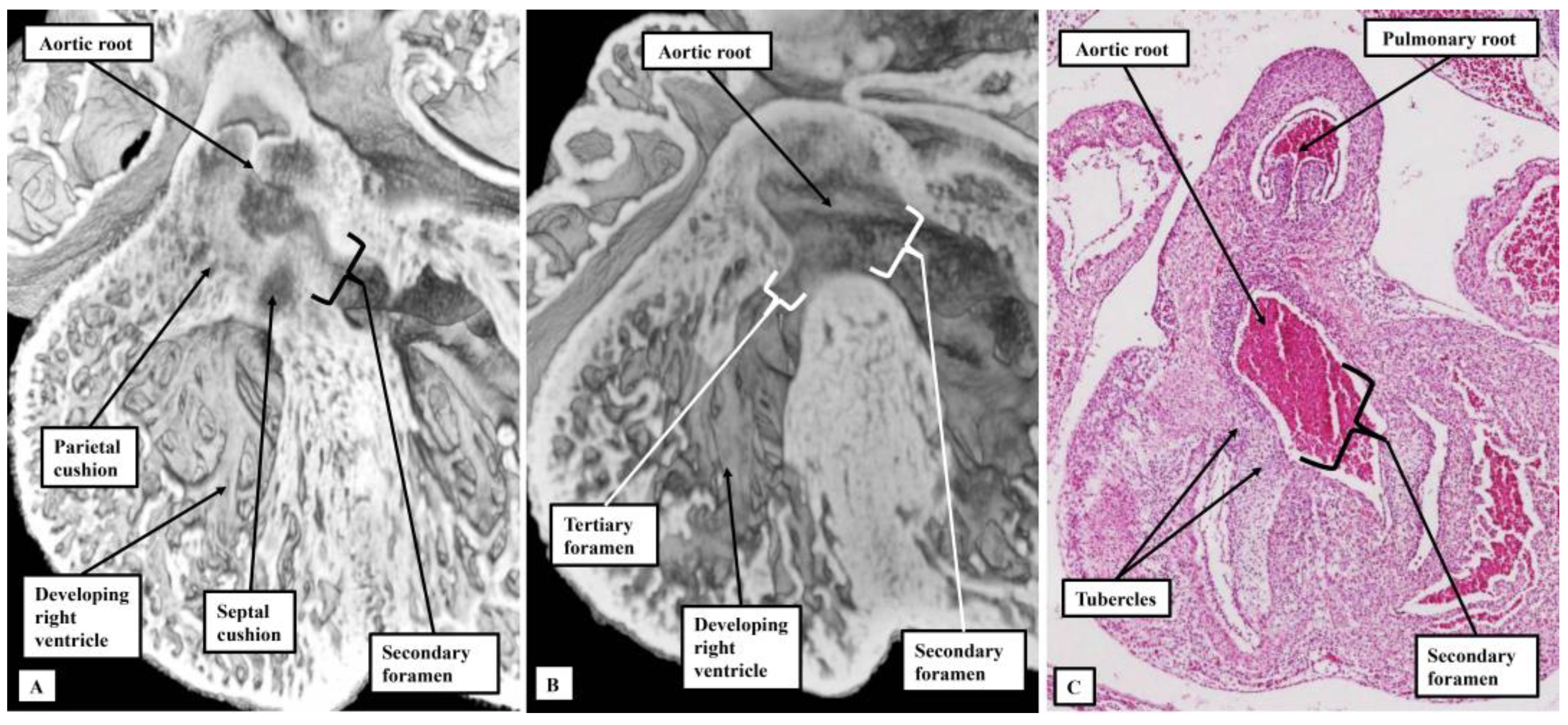
3.1. Evidence from Development
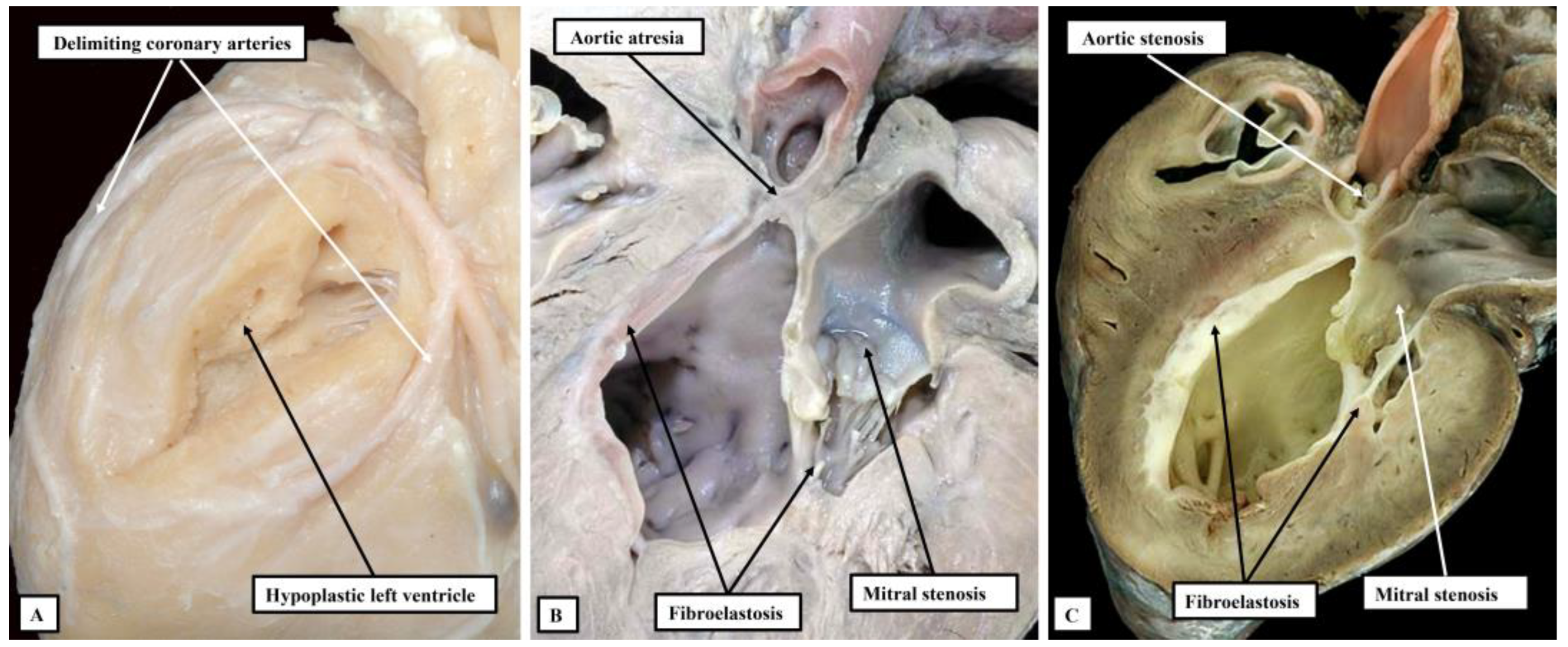
3.2. Morphological Findings in Postnatal Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tchervenkov, C.I.; Jacobs, J.P.; Weinberg, P.M.; Aiello, V.D.; Béland, M.J.; Colan, S.D.; Elliott, M.J.; Franklin, R.C.; Gaynor, J.W.; Krogmann, O.N.; et al. The nomenclature, definition and classification of hypoplastic left heart syndrome. Cardiol. Young 2006, 16, 339–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Yagi, H.; Saeed, S.; Bais, A.S.; Gabriel, G.C.; Chen, Z.; Peterson, K.A.; Li, Y.; Schwartz, M.C.; Reynolds, W.T.; et al. The complex genetics of hypoplastic left heart syndrome. Nat. Gene 2017, 49, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.H.; Spicer, D.E.; Crucean, A. Clarification of the definition of hypoplastic left heart syndrome. Nat. Rev. Cardiol. 2021, 18, 147–148. [Google Scholar] [CrossRef] [PubMed]
- Stephens, E.H.; Gupta, D.; Bleiweis, M.; Backer, C.L.; Anderson, R.H.; Spicer, D.E. Pathologic characteristics of 119 archived specimens showing the phenotypic features of hypoplastic left heart syndrome. Sem. Thorac. Cardiovasc. Surg. 2020, 32, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Noonan, J.A.; Nadas, A.S. The hypoplastic left heart syndrome: An analysis of 101 cases. Pediat. Clin. N. Am. 1958, 5, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Lev, M. Pathologic anatomy and interrelationship of hypoplasia of the aortic tract complexes. Lab. Investig. 1952, 1, 61–70. [Google Scholar] [PubMed]
- Lev, M. Some newer concepts of the pathology of congenital heart disease. Med. Clin. N. Am. 1966, 50, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Alphonso, N.; Angelini, A.; Barron, D.J.; Bellsham-Revell, H.; Blom, N.A.; Brown, K.; Davis, D.; Duncan, D.; Fedrigo, M.; Galletti, L.; et al. Guidelines for the management of neonates and infants with hypoplastic left heart syndrome: The European Association for Cardio-Thoracic Surgery (EACTS) and the Association for European Paediatric and Congenital Cardiology (AEPC) Hypoplastic Left Heart Syndrome Guidelines Task Force. Eur. J. Cardio-Thorac. Surg. 2020, 58, 416–499. [Google Scholar]
- Mickell, J.J.; Mathews, R.A.; Anderson, R.H.; Zuberbuhler, J.R.; Lenox, C.C.; Neches, W.H.; Park, S.C.; Fricker, F.J. The anatomical heterogeneity of hearts lacking a patent communication between the left atrium and the ventricular mass (‘mitral atresia’) in presence of a patent aortic valve. Eur. Heart J. 1983, 4, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Norwood, W.I.; Lang, P.; Hansen, D.D. Physiologic repair of aortic atresia–hypoplastic left heart syndrome. N. Engl. J. Med. 1983, 308, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Gittenberger-de Groot, A.C.; Wenink, A.C. Mitral atresia. Morphological details. Br. Heart J. 1984, 51, 252–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchervenkov, C.I.; Tahta, S.A.; Jutras, L.C.; Béland, M.J. Biventricular repair in neonates with hypoplastic left heart complex. Ann. Thor. Surg. 1998, 66, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Pesevski, Z.; Kvasilova, A.; Stopkova, T.; Nanka, O.; Drobna Krejci, E.; Buffinton, C.; Kockova, R.; Eckhardt, A.; Sedmera, D. Endocardial fibroelastosis is secondary to hemodynamic alterations in the chick embryonic model of hypoplastic left heart syndrome. Dev. Dyn. 2018, 247, 509–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weixler, V.; Marx, G.R.; Hammer, P.E.; Emani, S.M.; Pedro, J.; Friehs, I. Flow disturbances and the development of endocardial fibroelastosis. J. Thorac. Cardiovasc. Surg. 2020, 159, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Crucean, A.; Alqahtani, A.; Barron, D.J.; Brawn, W.J.; Richardson, R.V.; O’Sullivan, J.; Anderson, R.H.; Henderson, D.J.; Chaudhry, B. Re-evaluation of hypoplastic left heart syndrome from a developmental and morphological perspective. Orphanet J. Rare Dis. 2017, 12, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, A.; DeYoung, T.; Cahill, L.S.; Yee, Y.; Debebe, S.K.; Botelho, O.; Seed, M.; Chaturvedi, R.R.; Sled, J.G. A mouse model of hypoplastic left heart syndrome demonstrating left heart hypoplasia and retrograde aortic arch flow. Dis. Models Mech. 2021, 14, dmm049077. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anderson, R.H.; Crucean, A.; Spicer, D.E. What Is the Hypoplastic Left Heart Syndrome? J. Cardiovasc. Dev. Dis. 2023, 10, 133. https://doi.org/10.3390/jcdd10040133
Anderson RH, Crucean A, Spicer DE. What Is the Hypoplastic Left Heart Syndrome? Journal of Cardiovascular Development and Disease. 2023; 10(4):133. https://doi.org/10.3390/jcdd10040133
Chicago/Turabian StyleAnderson, Robert H., Adrian Crucean, and Diane E. Spicer. 2023. "What Is the Hypoplastic Left Heart Syndrome?" Journal of Cardiovascular Development and Disease 10, no. 4: 133. https://doi.org/10.3390/jcdd10040133
APA StyleAnderson, R. H., Crucean, A., & Spicer, D. E. (2023). What Is the Hypoplastic Left Heart Syndrome? Journal of Cardiovascular Development and Disease, 10(4), 133. https://doi.org/10.3390/jcdd10040133