
Growing Heart Valve Implants for Children

 ,
,
Abstract
:1. Introduction
2. Current Standard of Care
3. Strategies for Delivering Growing Heart Valves
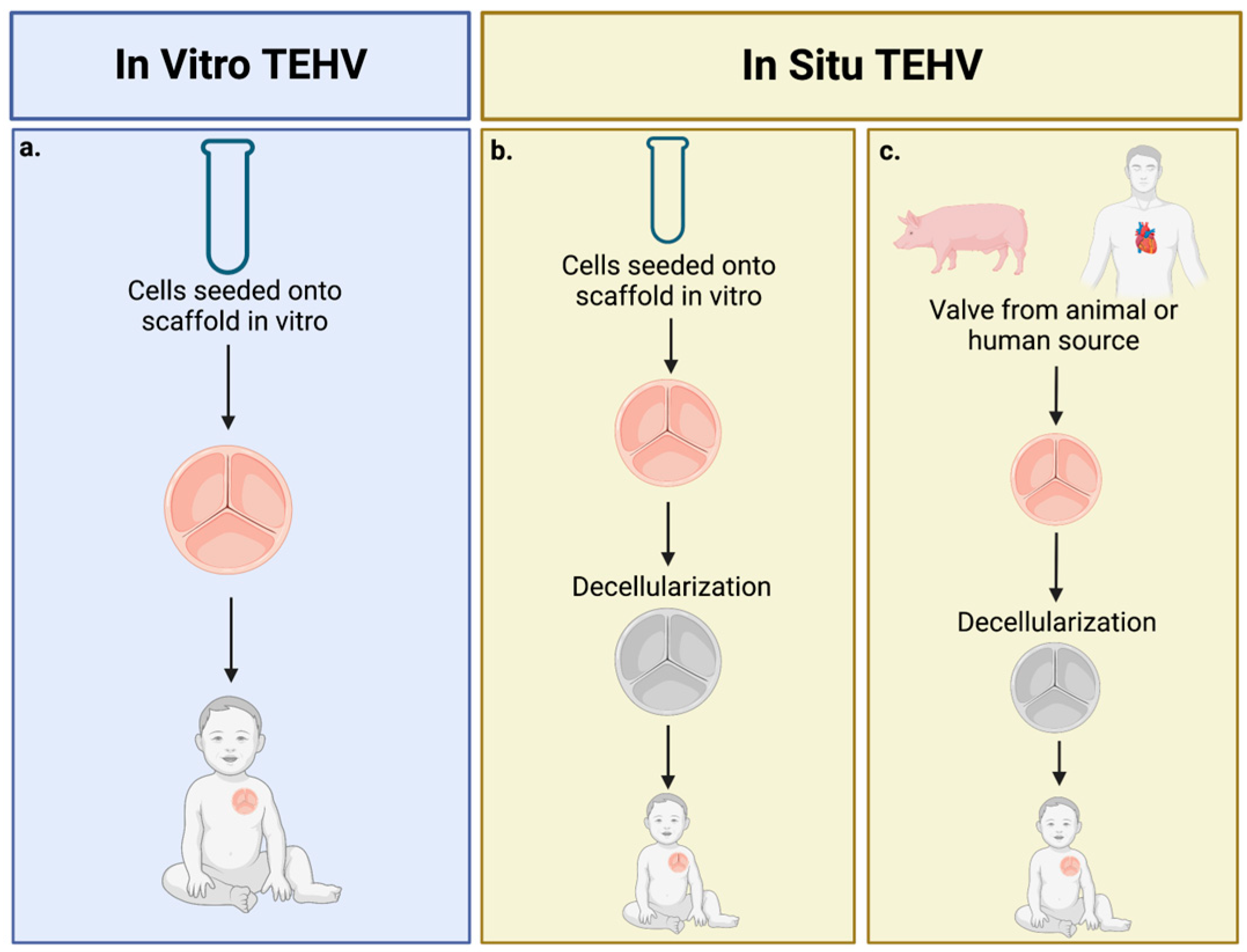
3.1. Tissue-Engineered Heart Valves
3.1.1. Design—Cell Sources and Scaffolds
3.1.2. In Vitro Heart Valve Tissue Engineering
3.1.3. In Situ Heart Valve Tissue Engineering
3.1.4. TEHVs in Clinical Studies with Pediatric Patients
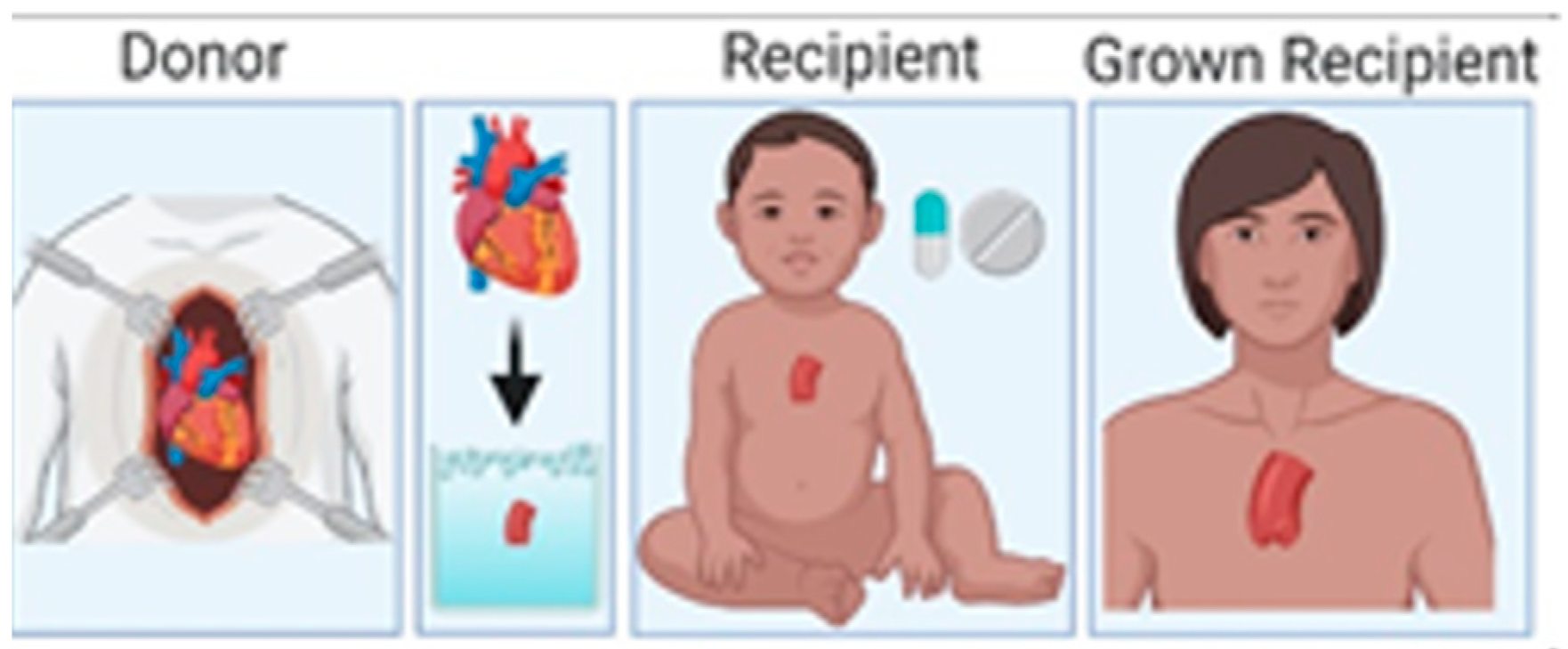
3.2. Partial Heart Transplant
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, W.; He, J.; Shao, X. Incidence and mortality trend of congenital heart disease at the global, regional, and national level, 1990–2017. Medicine 2020, 99, e20593. [Google Scholar] [CrossRef] [PubMed]
- Gilboa, S.M.; Devine, O.J.; Kucik, J.E.; Oster, M.E.; Riehle-Colarusso, T.; Nembhard, W.N.; Xu, P.; Correa, A.; Jenkins, K.; Marelli, A.J. Congenital Heart Defects in the United States: Estimating the Magnitude of the Affected Population in 2010. Circulation 2016, 134, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Applegate, P.M.; Boyd, W.D.; Applegate, R.L., II; Liu, H. Is it the time to reconsider the choice of valves for cardiac surgery: Mechanical or bioprosthetic? J. Biomed. Res. 2017, 31, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.I. The global burden of congenital heart disease: Review article. Cardiovasc. J. Afr. 2013, 24, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triedman, J.K.; Newburger, J.W. Trends in Congenital Heart Disease. Circulation 2016, 133, 2716–2733. [Google Scholar] [CrossRef]
- Shinoka, T.; Miyachi, H. Current Status of Tissue Engineering Heart Valve. World J. Pediatr. Congenit. Heart Surg. 2016, 7, 677–684. [Google Scholar] [CrossRef]
- Etnel, J.R.; Elmont, L.C.; Ertekin, E.; Mokhles, M.M.; Heuvelman, H.J.; Roos-Hesselink, J.W.; de Jong, P.L.; Helbing, W.A.; Bogers, A.J.; Takkenberg, J.J. Outcome after aortic valve replacement in children: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2015, 151, 143–152.e3. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.S.; Trento, A.; DeRobertis, M.; Kass, R.M.; Sandhu, M.; Czer, L.S.; Blanche, C.; Raissi, S.; Fontana, G.P.; Cheng, W.; et al. Twenty-year comparison of tissue and mechanical valve replacement. J. Thorac. Cardiovasc. Surg. 2001, 122, 257–269. [Google Scholar] [CrossRef] [Green Version]
- Kostyunin, A.E.; Yuzhalin, A.E.; Rezvova, M.A.; Ovcharenko, E.; Glushkova, T.V.; Kutikhin, A.G. Degeneration of Bioprosthetic Heart Valves: Update 2020. J. Am. Heart Assoc. 2020, 9, e018506. [Google Scholar] [CrossRef]
- Hawkins, J.A.; Hillman, N.D.; Lambert, L.M.; Jones, J.; Di Russo, G.B.; Profaizer, T.; Fuller, T.C.; Minich, L.; Williams, R.V.; Shaddy, R.E. Immunogenicity of decellularized cryopreserved allografts in pediatric cardiac surgery: Comparison with standard cryopreserved allografts. J. Thorac. Cardiovasc. Surg. 2003, 126, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Henaine, R.; Roubertie, F.; Vergnat, M.; Ninet, J. Valve replacement in children: A challenge for a whole life. Arch. Cardiovasc. Dis. 2012, 105, 517–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, J.H.; Hill, M.; Gerry, B.; Kubalak, S.W.; Mohiuddin, M.; Kavarana, M.N.; Rajab, T.K. Surgical techniques for aortic valve xenotransplantation. J. Cardiothorac. Surg. 2021, 16, 358. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.P.; Mavroudis, C.; Quintessenza, J.A.; Chai, P.J.; Pasquali, S.K.; Hill, K.D.; Vricella, L.A.; Jacobs, M.L.; Dearani, J.A.; Cameron, D. Reoperations for pediatric and congenital heart disease: An analysis of the Society of Thoracic Surgeons (STS) congenital heart surgery database. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 2014, 17, 2–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacks, M.S.; Schoen, F.J.; Mayer, J.E. Bioengineering Challenges for Heart Valve Tissue Engineering. Annu. Rev. Biomed. Eng. 2009, 11, 289–313. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef] [Green Version]
- Gottlieb, D.; Kunal, T.; Emani, S.; Aikawa, E.; Brown, D.W.; Powell, A.J.; Nedder, A.; Engelmayr, G.C., Jr.; Melero-Martin, J.M.; Sacks, M.S.; et al. In vivo monitoring of function of autologous engineered pulmonary valve. J. Thorac. Cardiovasc. Surg. 2010, 139, 723–731. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, T.C.; Sachweh, J.S.; Frese, J.; Schnöring, H.; Gronloh, N.; Koch, S.; Tolba, R.H.; Schmitz-Rode, T.; Jockenhoevel, S. In Vivo Remodeling and Structural Characterization of Fibrin-Based Tissue-Engineered Heart Valves in the Adult Sheep Model. Tissue Eng. Part A 2009, 15, 2965–2976. [Google Scholar] [CrossRef]
- Schmidt, D.; Dijkman, P.E.; Driessen-Mol, A.; Stenger, R.; Mariani, C.; Puolakka, A.; Rissanen, M.; Deichmann, T.; Odermatt, B.; Weber, B.; et al. Minimally-Invasive Implantation of Living Tissue Engineered Heart Valves: A Comprehensive Approach From Autologous Vascular Cells to Stem Cells. J. Am. Coll. Cardiol. 2010, 56, 510–520. [Google Scholar] [CrossRef] [Green Version]
- Weber, B.; Emmert, M.; Hoerstrup, S. Stem cells for heart valve regeneration. Swiss Med. Wkly. 2012, 142, w13622. [Google Scholar] [CrossRef] [Green Version]
- Weber, B.; Dijkman, P.E.; Scherman, J.; Sanders, B.; Emmert, M.Y.; Grünenfelder, J.; Verbeek, R.; Bracher, M.; Black, M.; Franz, T.; et al. Off-the-shelf human decellularized tissue-engineered heart valves in a non-human primate model. Biomaterials 2013, 34, 7269–7280. [Google Scholar] [CrossRef]
- Driessen-Mol, A.; Emmert, M.Y.; Dijkman, P.E.; Frese, L.; Sanders, B.; Weber, B.; Cesarovic, N.; Sidler, M.; Leenders, J.; Jenni, R.; et al. Transcatheter Implantation of Homologous “Off-the-Shelf” Tissue-Engineered Heart Valves With Self-Repair Capacity. J. Am. Coll. Cardiol. 2014, 63, 1320–1329. [Google Scholar] [CrossRef] [PubMed]
- Motta, S.E.; Lintas, V.; Fioretta, E.S.; Dijkman, P.E.; Putti, M.; Caliskan, E.; Biefer, H.R.C.; Lipiski, M.; Sauer, M.; Cesarovic, N.; et al. Human cell-derived tissue-engineered heart valve with integrated Valsalva sinuses: Towards native-like transcatheter pulmonary valve replacements. NPJ Regen. Med. 2019, 4, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reimer, J.; Syedain, Z.; Haynie, B.; Lahti, M.; Berry, J.; Tranquillo, R. Implantation of a Tissue-Engineered Tubular Heart Valve in Growing Lambs. Ann. Biomed. Eng. 2017, 45, 439–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syedain, Z.; Reimer, J.; Schmidt, J.; Lahti, M.; Berry, J.; Bianco, R.; Tranquillo, R.T. 6-Month aortic valve implantation of an off-the-shelf tissue-engineered valve in sheep. Biomaterials 2015, 73, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Emmert, M.Y.; Schmitt, B.A.; Loerakker, S.; Sanders, B.; Spriestersbach, H.; Fioretta, E.S.; Bruder, L.; Brakmann, K.; Motta, S.E.; Lintas, V.; et al. Computational modeling guides tissue-engineered heart valve design for long-term in vivo performance in a translational sheep model. Sci. Transl. Med. 2018, 10, eaan4587. [Google Scholar] [CrossRef] [Green Version]
- Kluin, J.; Talacua, H.; Smits, A.I.; Emmert, M.Y.; Brugmans, M.C.; Fioretta, E.S.; Dijkman, P.E.; Söntjens, S.H.; Duijvelshoff, R.; Dekker, S.; et al. In situ heart valve tissue engineering using a bioresorbable elastomeric implant—From material design to 12 months follow-up in sheep. Biomaterials 2017, 125, 101–117. [Google Scholar] [CrossRef]
- Cebotari, S.; Lichtenberg, A.; Tudorache, I.; Hilfiker, A.; Mertsching, H.; Leyh, R.; Breymann, T.; Kallenbach, K.; Maniuc, L.; Batrinac, A.; et al. Clinical Application of Tissue Engineered Human Heart Valves Using Autologous Progenitor Cells. Circulation 2006, 114 (Suppl. S1), I-132–I-137. [Google Scholar] [CrossRef] [Green Version]
- Simon, P. Early failure of the tissue engineered porcine heart valve SYNERGRAFT™ in pediatric patients. Eur. J. Cardio-Thorac. Surg. 2003, 23, 1002–1006. [Google Scholar] [CrossRef] [Green Version]
- Rüffer, A.; Purbojo, A.; Cicha, I.; Glöckler, M.; Potapov, S.; Dittrich, S.; Cesnjevar, R.A. Early failure of xenogenous de-cellularised pulmonary valve conduits—A word of caution!☆. Eur. J. Cardio-Thorac. Surg. 2010, 38, 78–85. [Google Scholar] [CrossRef]
- Voges, I.; Bräsen, J.H.; Entenmann, A.; Scheid, M.; Scheewe, J.; Fischer, G.; Hart, C.; Andrade, A.; Pham, H.M.; Kramer, H.-H.; et al. Adverse results of a decellularized tissue-engineered pulmonary valve in humans assessed with magnetic resonance imaging. Eur. J. Cardio-Thorac. Surg. 2013, 44, e272–e279. [Google Scholar] [CrossRef] [Green Version]
- Sarikouch, S.; Horke, A.; Tudorache, I.; Beerbaum, P.; Westhoff-Bleck, M.; Boethig, D.; Repin, O.; Maniuc, L.; Ciubotaru, A.; Haverich, A.; et al. Decellularized fresh homografts for pulmonary valve replacement: A decade of clinical experience. Eur. J. Cardio-Thorac. Surg. 2016, 50, 281–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tudorache, I.; Horke, A.; Cebotari, S.; Sarikouch, S.; Boethig, D.; Breymann, T.; Beerbaum, P.; Bertram, H.; Westhoff-Bleck, M.; Theodoridis, K.; et al. Decellularized aortic homografts for aortic valve and aorta ascendens replacement. Eur. J. Cardio-Thorac. Surg. 2016, 50, 89–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horke, A.; Tudorache, I.; Laufer, G.; Andreas, M.; Pomar, J.L.; Pereda, D.; Quintana, E.; Sitges, M.; Meyns, B.; Rega, F.; et al. Early results from a prospective, single-arm European trial on decellularized allografts for aortic valve replacement: The ARISE study and ARISE Registry data. Eur. J. Cardio-Thorac. Surg. 2020, 58, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Prodan, Z.; Mroczek, T.; Sivalingam, S.; Bennink, G.; Asch, F.M.; Cox, M.; Carrel, T.; Yakub, M.A.; Nagy, Z.; Skalski, J.; et al. Initial Clinical Trial of a Novel Pulmonary Valved Conduit. Semin. Thorac. Cardiovasc. Surg. 2022, 34, 985–991. [Google Scholar] [CrossRef]
- Rajab, T.K. Evidence-based surgical hypothesis: Partial heart transplantation can deliver growing valve implants for congenital cardiac surgery. Surgery 2021, 169, 983–985. [Google Scholar] [CrossRef]
- Rajab, T.K.; Ochoa, B.; Zilinskas, K.; Kwon, J.; Taylor, C.L.; Henderson, H.T.; Savage, A.J.; Kavarana, M.; Turek, J.W.; Costello, J.M. Partial heart transplantation for pediatric heart valve dysfunction: A clinical trial protocol. PLoS ONE 2023, 18, e0280163. [Google Scholar] [CrossRef]
- Nomoto, R.; Sleeper, L.A.; Borisuk, M.J.; Bergerson, L.; Pigula, F.A.; Emani, S.; Fynn-Thompson, F.; Mayer, J.E.; del Nido, P.J.; Baird, C.W. Outcome and performance of bioprosthetic pulmonary valve replacement in patients with congenital heart disease. J. Thorac. Cardiovasc. Surg. 2016, 152, 1333–1342.e3. [Google Scholar] [CrossRef] [Green Version]
- Lisy, M.; Kalender, G.; Schenke-Layland, K.; Brockbank, K.G.M.; Biermann, A.; Stock, U.A. Allograft Heart Valves: Current Aspects and Future Applications. Biopreserv. Biobank. 2017, 15, 148–157. [Google Scholar] [CrossRef]
- Ross, D.N. Evolution of the homograft valve. Ann. Thorac. Surg. 1995, 59, 565–567. [Google Scholar] [CrossRef]
- O’Brien, M.F.; Stafford, E.G.; Gardner, M.A.; Pohlner, P.G.; McGiffin, D.C.; Kirklin, J.W. A comparison of aortic valve replacement with viable cryopreserved and fresh allograft valves, with a note on chromosomal studies. J. Thorac. Cardiovasc. Surg. 1987, 94, 812–823. [Google Scholar] [CrossRef]
- Allen, M.D.; Shoji, Y.; Fujimura, Y.; Gordon, D.; Thomas, R.; Brockbank, K.G.; Disteche, C.M. Growth and cell viability of aortic versus pulmonic homografts in the systemic circulation. Circulation 1991, 84 (Suppl. S5), III94-9. [Google Scholar] [PubMed]
- Bibevski, S.; Ruzmetov, M.; Fortuna, R.S.; Turrentine, M.W.; Brown, J.W.; Ohye, R.G. Performance of SynerGraft Decellularized Pulmonary Allografts Compared With Standard Cryopreserved Allografts: Results From Multiinstitutional Data. Ann. Thorac. Surg. 2017, 103, 869–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, A.; Ahmed, S.; Varghese, K.S.; Mathew, D.M.; Pandey, R.; Rogando, D.O.; Salazar, S.A.; Fusco, P.J.; Levy, K.H. Decellularized versus cryopreserved pulmonary allografts for right ventricular outflow tract reconstruction during the Ross procedure: A meta-analysis of short- and long-term outcomes. Egypt. Heart J. 2021, 73, 100. [Google Scholar] [CrossRef]
- Woods, R.K.; Pasquali, S.K.; Jacobs, M.L.; Austin, E.H.; Jacobs, J.P.; Krolikowski, M.; Mitchell, M.E.; Pizarro, C.; Tweddell, J.S. Aortic valve replacement in neonates and infants: An analysis of the Society of Thoracic Surgeons Congenital Heart Surgery Database. J. Thorac. Cardiovasc. Surg. 2012, 144, 1084–1090. [Google Scholar] [CrossRef] [Green Version]
- McElhinney, D.B.; Reddy, V.M.; Rajasinghe, H.A.; Mora, B.N.; Silverman, N.H.; Hanley, F.L. Trends in the Management of Truncal Valve Insufficiency. Ann. Thorac. Surg. 1998, 65, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, D.; Kolla, S.; Miner, M.; Pitlick, P.; Griffin, M.; Starnes, V.; Rowan, R.; Billingham, M.; Baum, D. Cardiac growth after pediatric heart transplantation. Circulation 1992, 85, 1433–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delmo Walter, E.M.; Huebler, M.; Stamm, C.; Alexi-Meskishvili, V.; Weng, Y.; Berger, F.; Hetzer, R. Adaptive growth and remodeling of transplanted hearts in children. Eur. J. Cardio-Thorac. Surg. 2011, 40, 1374–1382; discussion 1382–1383. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, R.N.; Jonas, R.A.; Schoen, F.J. Pathology Of Explanted Cryopreserved Allograft Heart Valves: Comparison With Aortic Valves From Orthotopic Heart Transplants. J. Thorac. Cardiovasc. Surg. 1998, 115, 118–127. [Google Scholar] [CrossRef] [Green Version]
- Valante, M.; Faggian, G.; Billingham, M.E.; Talenti, E.; Calabrese, F.; Casula, R.; Shumway, N.E.; Thiene, G. The aortic valve after heart transplantation. Ann. Thorac. Surg. 1995, 60, S135–S140. [Google Scholar] [CrossRef]
- John, M.M.; Razzouk, A.J.; Chinnock, R.E.; Bock, M.J.; Kuhn, M.A.; Martens, T.; Bailey, L.L. Primary Transplantation for Congenital Heart Disease in the Neonatal Period: Long-term Outcomes. Ann. Thorac. Surg. 2019, 108, 1857–1864. [Google Scholar] [CrossRef]
- Lin, Y.; Davis, T.J.; Zorrilla-Vaca, A.; Wojcik, B.M.; Miyamoto, S.D.; Everitt, M.D.; Campbell, D.N.; Jaggers, J.J.; Rajab, T.K. Neonatal heart transplant outcomes: A single institutional experience. J. Thorac. Cardiovasc. Surg. 2021, 162, 1361–1368. [Google Scholar] [CrossRef] [PubMed]
- Rippel, R.A.; Ghanbari, H.; Seifalian, A.M. Tissue-Engineered Heart Valve: Future of Cardiac Surgery. World J. Surg. 2012, 36, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Nachlas, A.L.Y.; Li, S.; Davis, M.E. Developing a Clinically Relevant Tissue Engineered Heart Valve—A Review of Current Approaches. Adv. Healthc. Mater. 2017, 6, 1700918. [Google Scholar] [CrossRef]
- Taghizadeh, B.; Ghavami, L.; Derakhshankhah, H.; Zangene, E.; Razmi, M.; Jaymand, M.; Zarrintaj, P.; Zarghami, N.; Jaafari, M.R.; Shahri, M.M.; et al. Biomaterials in Valvular Heart Diseases. Front. Bioeng. Biotechnol. 2020, 8, 529244. [Google Scholar] [CrossRef] [PubMed]
- Vander Roest, M.J.; Merryman, W.D. A developmental approach to induced pluripotent stem cells-based tissue engineered heart valves. Future Cardiol. 2017, 13, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dijkman, P.E.; Fioretta, E.S.; Frese, L.; Pasqualini, F.S.; Hoerstrup, S.P. Heart Valve Replacements with Regenerative Capacity. Transfus. Med. Hemother. 2016, 43, 282–290. [Google Scholar] [CrossRef] [Green Version]
- Snyder, Y.; Jana, S. Strategies for development of decellularized heart valve scaffolds for tissue engineering. Biomaterials 2022, 288, 121675. [Google Scholar] [CrossRef]
- Sodian, R.; Hoerstrup, S.P.; Sperling, J.S.; Daebritz, S.; Martin, D.P.; Moran, A.M.; Kim, B.S.; Schoen, F.J.; Vacanti, J.P.; Mayer, J.E., Jr. Early in vivo experience with tissue-engineered trileaflet heart valves. Circulation 2000, 102 (Suppl. S3), III22–III29. [Google Scholar] [CrossRef]
- Ciolacu, D.E.; Nicu, R.; Ciolacu, F. Natural Polymers in Heart Valve Tissue Engineering: Strategies, Advances and Challenges. Biomedicines 2022, 10, 1095. [Google Scholar] [CrossRef]
- Mirani, B.; Nejad, S.P.; Simmons, C.A. Recent Progress Toward Clinical Translation of Tissue-Engineered Heart Valves. Can. J. Cardiol. 2021, 37, 1064–1077. [Google Scholar] [CrossRef]
- Zhang, B.; Chen, X.; Xu, T.-Y.; Zhang, Z.-G.; Li, X.; Han, L.; Xu, Z.-Y. Transcatheter Pulmonary Valve Replacement by Hybrid Approach Using a Novel Polymeric Prosthetic Heart Valve: Proof of Concept in Sheep. PLoS ONE 2014, 9, e100065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, J.H.; Hill, M.A.; Gerry, B.; Morningstar, J.; Kavarana, M.N.; Nadig, S.N.; Rajab, T.K. Cellular Viability of Partial Heart Transplant Grafts in Cold Storage. Front. Surg. 2021, 8, 676739. [Google Scholar] [CrossRef] [PubMed]
- Sherard, C.; Atteya, M.; Vogel, A.D.; Bisbee, C.; Kang, L.; Turek, J.W.; Rajab, T.K. Partial heart transplantation can ameliorate donor organ utilization. J. Card. Surg. 2022, 37, 5307–5312. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Stage of Development | Approach | Progress | Reference |
|---|---|---|---|
| In vivo | Autologous ovine bone marrow-derived mesenchymal cells seeded onto a bioresorbable scaffold | Acceptable initial valve function in sheep with increasing regurgitation and decreasing cusp length after 12–20 weeks | [16] |
| In vivo | Autologous vascular cells seeded on a biopolyester scaffold in vitro | Large animal studies in sheep revealed normal function after 17 weeks with mild stenosis and incomplete endothelial cell seeding | [17] |
| In vivo | Autologous endothelial, smooth muscle, and fibroblast cells seeded on patient-derived fibrin scaffold in vitro | Sheep studies revealed successful remodeling after 3 months; however, all valved failed due to valvular insufficiency | [18] |
| In vivo | Autologous ovine bone-marrow-derived stem cells seeded onto a bioresorbable scaffold integrated into a self-expanding stent | Minimally invasive implantation in sheep was successful. After 8 weeks, valves showed normal functionality with leaflet thickening present | [19] |
| In vivo | Decellularized heart valve fabricated on a bioresorbable nitinol stent scaffold with human vascular-derived fibroblasts | Prior to implantation, valves demonstrated reduced coaptation leading to leaflet shortening after implantation in non-human primates (chacma baboons) | [20] |
| In vivo | Decellularized heart valve engineered on a rapidly degrading synthetic scaffold with autologous vascular-derived cells | By 24 weeks post-implantation, moderate regurgitation was observed in sheep models with a significant reduction in coaptation leading to non-physiological loading and insufficient washout during diastole | [21] |
| In vivo | Decellularized valve engineered in vitro from human neonatal dermal fibroblasts on a bioresorbable PGA scaffold with integrated Valsalva sinuses | 4 h after implantation in sheep, valves demonstrated normal function | [22] |
| In vivo | Decellularized tubular valve engineered in vitro from autologous ovine dermal fibroblasts with degradable sutures | Valve integration and normal function of implanted valves in sheep for 8 weeks with leaflet shortening, loss of functional ability and ultimately valve failure by 22 weeks | [23] |
| In vivo | Decellularized tubular valve engineered on a collagen scaffold with ovine dermal fibroblasts | 24 weeks after implantation in the aortic position in sheep, valves showed normal function and recellularization | [24] |
| In vivo | Computationally inspired in vitro design of decellularized TEHV seeded with myofibroblasts | After 1 year of implantation in sheep, valves showed normal function, ECM remodeling, and mild regurgitation | [25] |
| In vivo | Trileaflet polymeric pulmonary valve with leaflets made of 0.1 mm expanded polytetrafluoroethylene coated with phosphorylcholine and balloon-expandable stent | Polymeric valves implanted in sheep exhibited normal function, and no evidence of insufficiency or thrombosis; however, mild fibrous overgrowth was revealed with no evidence of tissue infiltration | [26] |
| In vivo | Pulmonary valve with scaffold created from a bioresorbable novel supramolecular elastomer based on bis-urea-modified polycarbonate | Twelve months after implantation, valves demonstrated normal functionality with evidence of host cell colonization and formation of neo-tissue. However, scaffold resorption was incomplete, indicating longer follow-up studies for long-term durability | [27] |
| Clinical | Decellularized human pulmonary valve allograft reseeded with autologous endothelial progenitor cells | The valves were implanted in two pediatric patients. At 3.5 years follow-up, the valves demonstrated trivial regurgitation, increased valve annulus diameter, and no evidence of valve degeneration | [28] |
| Clinical | SynergraftTM valve: Decellularized porcine heart valve | Hyperacute and acute rejection of valves, resulting in the deaths of 3 of the 4 children | [29] |
| Clinical | Decellularized xenograft using Matrix P plus (decellularized porcine pulmonary valve) | Six of the 16 pediatric patients required reoperation after 10 months due to graft obstruction secondary to inflammatory infiltration | [30] |
| Clinical | Decellularized xenograft using Matrix P and Matrix P plus pulmonary valves | Reoperation was required in 14 of 26 patients due to graft failure secondary to inflammation and fibrosis | [31] |
| Clinical | Decellularized pulmonary valve homograft | Ten year follow-up in pediatric patients revealed less degeneration than the current standard of care, but some implants developed stenosis and regurgitation; evidence of growth was present after 5 years | [32] |
| Clinical | Decellularized aortic allograft | Average 2–3 year follow-up in 16 pediatric patients revealed normal valve function but no evidence of annulus diameter growth | [33] |
| Clinical | ARISE trial: Decellularized aortic allograft | Early results in pediatric patients demonstrated comparable results to the Ross procedure, pending 10 year follow-up results | [34] |
| Clinical | Xeltis pulmonary valve made of bioresorbable supramolecular 2-ureido-4[1H]-pyrimidone | The Xeltis valve was transplanted into 12 human pediatric patients. After 24 months, the valves showed no evidence of degeneration or stenosis. However, 5 patients developed severe insufficiency due to leaflet prolapse | [35] |
| Clinical | Partial heart transplantation | Prospective, non-randomized, single-center, single-arm pilot trial to be performed on children less than 2 years of age. Awaiting trial results | [36] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konsek, H.; Sherard, C.; Bisbee, C.; Kang, L.; Turek, J.W.; Rajab, T.K. Growing Heart Valve Implants for Children. J. Cardiovasc. Dev. Dis. 2023, 10, 148. https://doi.org/10.3390/jcdd10040148
Konsek H, Sherard C, Bisbee C, Kang L, Turek JW, Rajab TK. Growing Heart Valve Implants for Children. Journal of Cardiovascular Development and Disease. 2023; 10(4):148. https://doi.org/10.3390/jcdd10040148
Chicago/Turabian StyleKonsek, Haley, Curry Sherard, Cora Bisbee, Lillian Kang, Joseph W. Turek, and Taufiek K. Rajab. 2023. "Growing Heart Valve Implants for Children" Journal of Cardiovascular Development and Disease 10, no. 4: 148. https://doi.org/10.3390/jcdd10040148
APA StyleKonsek, H., Sherard, C., Bisbee, C., Kang, L., Turek, J. W., & Rajab, T. K. (2023). Growing Heart Valve Implants for Children. Journal of Cardiovascular Development and Disease, 10(4), 148. https://doi.org/10.3390/jcdd10040148