
Fluid Overload in Pediatric Univentricular Patients Undergoing Fontan Completion

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Intra-Operative Variables
3.2. Postoperative PICU Variables
3.3. Regression Analysis
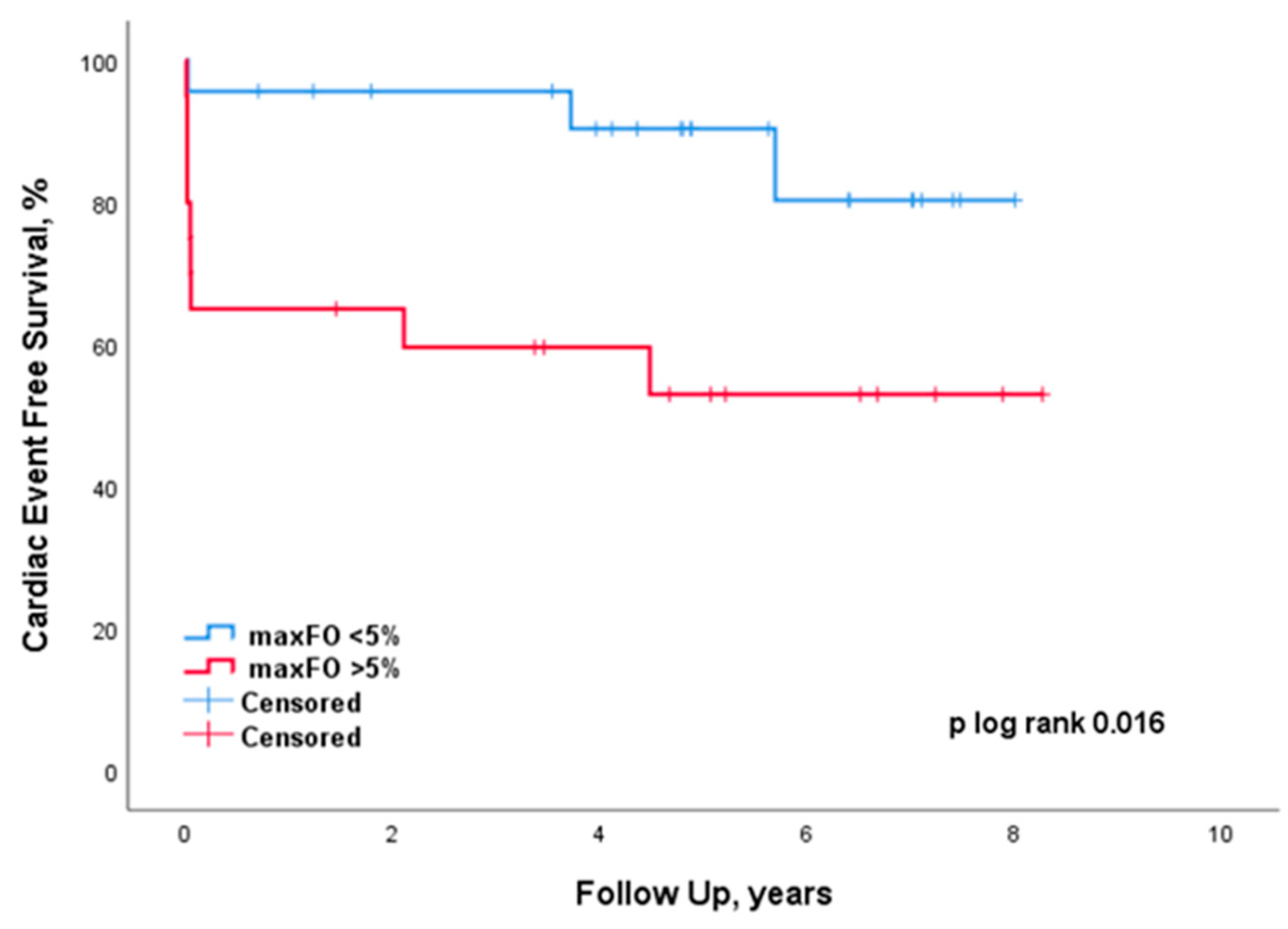
3.4. Follow-Up
3.5. Preoperative Cardiac Catheterizations, Ultrasounds and Interventions
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bellomo, R.; Raman, J.; Ronco, C. Intensive care unit management of the critically ill patient with fluid overload after open heart surgery. Cardiology 2001, 96, 169–176. [Google Scholar] [CrossRef]
- Lex, D.J.; Tóth, R.; Czobor, N.R.; Alexander, S.I.; Breuer, T.; Sápi, E.; Szatmári, A.; Székely, E.; Gál, J.; Székely, A. Fluid Overload Is Associated With Higher Mortality and Morbidity in Pediatric Patients Undergoing Cardiac Surgery. Pediatr. Crit. Care Med. 2016, 17, 307–314. [Google Scholar] [CrossRef]
- Seguin, J.; Albright, B.; Vertullo, L.; Lai, P.; Dancea, A.; Bernier, P.-L.; Tchervenkov, C.I.; Calaritis, C.; Drullinsky, D.; Gottesman, R.; et al. Extent, risk factors, and outcome of fluid overload after pediatric heart surgery*. Crit. Care Med. 2014, 42, 2591–2599. [Google Scholar] [CrossRef] [PubMed]
- Hazle, M.A.; Gajarski, R.J.; Yu, S.; Donohue, J.; Blatt, N.B. Fluid overload in infants following congenital heart surgery. Pediatr. Crit. Care Med. 2013, 14, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, T.Z.A.L.; O’Hearn, K.; Reddy, D.; Menon, K. The Influence of Fluid Overload on the Length of Mechanical Ventilation in Pediatric Congenital Heart Surgery. Pediatr. Cardiol. 2015, 36, 1692–1699. [Google Scholar] [CrossRef]
- Bellos, I.; Iliopoulos, D.; Perrea, D. Association of postoperative fluid overload with adverse outcomes after congenital heart surgery: A systematic review and dose-response meta-analysis. Pediatr. Nephrol. 2020, 35, 1109–1119. [Google Scholar] [CrossRef]
- Hassinger, A.B.; Wald, E.; Goodman, D. Early postoperative fluid overload precedes acute kidney injury and is associated with higher morbidity in pediatric cardiac surgery patients. Pediatr. Crit. Care Med. 2014, 15, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Wilder, N.S.; Yu, S.; Donohue, J.E.; Goldberg, C.S.; Blatt, N.B. Fluid Overload Is Associated With Late Poor Outcomes in Neonates Following Cardiac Surgery. Pediatr. Crit. Care Med. 2016, 17, 420–427. [Google Scholar] [CrossRef]
- Pundi, K.N.; Johnson, J.N.; Dearani, J.A.; Pundi, K.N.; Li, Z.; Hinck, C.A.; Dahl, S.H.; Cannon, B.C.; O’Leary, P.W.; Driscoll, D.J.; et al. 40-Year Follow-Up After the Fontan Operation: Long-Term Outcomes of 1052 Patients. J. Am. Coll. Cardiol. 2015, 66, 1700–1710. [Google Scholar] [CrossRef]
- Gaies, M.G.; Jeffries, H.E.; Niebler, R.A.; Pasquali, S.K.; Donohue, J.E.; Yu, S.; Gall, C.; Rice, T.B.; Thiagarajan, R.R. Vasoactive-inotropic score is associated with outcome after infant cardiac surgery: An analysis from the Pediatric Cardiac Critical Care Consortium and Virtual PICU System Registries. Pediatr. Crit. Care Med. 2014, 15, 529–537. [Google Scholar] [CrossRef]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Blinder, J.J.; Goldstein, S.L.; Lee, V.-V.; Baycroft, A.; Fraser, C.D.; Nelson, D.; Jefferies, J.L. Congenital heart surgery in infants: Effects of acute kidney injury on outcomes. J. Thorac. Cardiovasc. Surg. 2012, 143, 368–374. [Google Scholar] [CrossRef]
- Claure-Del Granado, R.; Mehta, R. Fluid overload in the ICU: Evaluation and management. BMC Nephrol. 2016, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- Boyle, A.; Maurer, M.; Sobotka, P. Myocellular and interstitial edema and circulating volume expansion as a cause of morbidity and mortality in heart failure. J. Card. Fail. 2007, 13, 133–136. [Google Scholar] [CrossRef]
- Echten, J.E.K.-V.H.T.; Goedvolk, C.A.; Doornaar, M.; Van Der Vorst, M.; Bosman-Vermeeren, J.M.; Brand, R.; Van Der Heijden, A.J.; Schoof, P.H.; Hazekamp, M.G. Acute renal insufficiency and renal replacement therapy after pediatric cardiopulmonary bypass surgery. Pediatr. Cardiol. 2001, 22, 321–326. [Google Scholar] [CrossRef]
- Licker, M.; Hagerman, A.; Bedat, B.; Ellenberger, C.; Triponez, F.; Schorer, R.; Karenovics, W. Restricted, optimized or liberal fluid strategy in thoracic surgery: A narrative review. Saudi J. Anaesth. 2021, 15, 324–334. [Google Scholar] [CrossRef]
- Arrahmani, I.; Ingelse, S.A.; van Woensel, J.B.M.; Bem, R.A.; Lemson, J. Current Practice of Fluid Maintenance and Replacement Therapy in Mechanically Ventilated Critically Ill Children: A European Survey. Front. Pediatr. 2022, 10, 828637. [Google Scholar] [CrossRef] [PubMed]
- Malbrain, M.L.N.G.; Van Regenmortel, N.; Saugel, B.; De Tavernier, B.; Van Gaal, P.-J.; Joannes-Boyau, O.; Teboul, J.-L.; Rice, T.W.; Mythen, M.; Monnet, X. Principles of fluid management and stewardship in septic shock: It is time to consider the four D’s and the four phases of fluid therapy. Ann. Intensive Care 2018, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Malbrain, M.L.N.G.; Langer, T.; Annane, D.; Gattinoni, L.; Elbers, P.; Hahn, R.G.; De Laet, I.; Minini, A.; Wong, A.; Ince, C.; et al. Intravenous fluid therapy in the perioperative and critical care setting: Executive summary of the International Fluid Academy (IFA). Ann. Intensive Care 2020, 10, 64. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, R.S.; Seidel, K.; Symons, J. Effect of fluid overload and dose of replacement fluid on survival in hemofiltration. Pediatr. Nephrol. 2004, 19, 1394–1399. [Google Scholar] [CrossRef]
- Sutherland, S.M.; Zappitelli, M.; Alexander, S.R.; Chua, A.N.; Brophy, P.D.; Bunchman, T.E.; Hackbarth, R.; Somers, M.J.; Baum, M.; Symons, J.M.; et al. Fluid overload and mortality in children receiving continuous renal replacement therapy: The prospective pediatric continuous renal replacement therapy registry. Am. J. Kidney Dis. 2010, 55, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Foland, J.A.; Fortenberry, J.D.; Warshaw, B.L.; Pettignano, R.; Merritt, R.K.; Heard, M.L.; Rogers, K.; Reid, C.; Tanner, A.J.; Easley, K.A. Fluid overload before continuous hemofiltration and survival in critically ill children: A retrospective analysis. Crit. Care Med. 2004, 32, 1771–1776. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.; Carcillo, J.A.; Choong, K.; Cornell, T.; DeCaen, A.; Deymann, A.; Doctor, A.; Davis, A.; Duff, J.; Dugas, M.-A.; et al. Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine. Crit. Care Med. 2009, 37, 666–688. [Google Scholar] [CrossRef]
- Goldstein, S.L.; Currier, H.; Graf, J.M.; Cosio, C.C.; Brewer, E.D.; Sachdeva, R. Outcome in children receiving continuous venovenous hemofiltration. Pediatrics 2001, 107, 1309–1312. [Google Scholar] [CrossRef]
- Selewski, D.T.; Cornell, T.T.; Lombel, R.M.; Blatt, N.B.; Han, Y.Y.; Mottes, T.; Kommareddi, M.; Kershaw, D.B.; Shanley, T.P.; Heung, M. Weight-based determination of fluid overload status and mortality in pediatric intensive care unit patients requiring continuous renal replacement therapy. Intensive Care Med. 2011, 37, 1166–1173. [Google Scholar] [CrossRef] [PubMed]
- Gewillig, M.; Brown, S. The Fontan circulation after 45 years: Update in physiology. Heart 2016, 102, 1081–1086. [Google Scholar] [CrossRef]


{kind=link}
| Variables | All (N = 43) | maxFO < 5% (N = 23) | maxFO > 5% (N = 20) | p-Value |
|---|---|---|---|---|
| Demographics and Preoperative | ||||
| Male, N(%) | 28 (65) | 15 (65) | 13 (65) | 1.000 |
| Age, years | 4.1 [3.5–4.7] | 4.1 [3.5–5.0] | 4.0 [3.6–4.6] | 0.805 |
| Weight, kg | 15.6 [15.0–16.6] | 15.7 [15.0–18.9] | 15.6 [15.0–16.6] | 0.608 |
| Length, cm | 102 [98–107] | 102 [100–110] | 101 [98–105] | 0.336 |
| Hemoglobin, mmol/L | 10.3 (1.1) | 10.3 (1.0) | 10.4 (1.2) | 0.716 |
| Creatinine, µmol/L | 31 [28–39] | 29 [27–38] | 32 [29–40] | 0.369 |
| Prematurity, N(%) | 1 (2) | 1 (4) | 0 (0) | 1.000 |
| Chromosomal abnormalities, N(%) | 1 (2) | 1 (4) | 0 (0) | 1.000 |
| Hypoplastic left ventricle, N(%) | 9 (21) | 3 (13) | 6 (30) | 0.263 |
| Intra-Operative | ||||
| CPB, min | 126 [105–185] | 125 [92–173] | 140 [109–206] | 0.337 |
| AOX, min | 75 [24–100] | 53 [0–88] | 79 [69–107] | 0.019 |
| Minimum temperature, °C | 26.4 (4.1) | 26.4 (4.9) | 26.4 (3.5) | 0.990 |
| Ultrafiltration, mL | 600 [323–840] | 480 [248–800] | 710 [500–1120] | 0.041 |
| Administered erythrocytes, mL | 100 [0–250] | 50 [0–213] | 150 [0–275] | 0.145 |
| Administered FFP, mL | 160 [68–255] | 170 [15–300] | 160 [75–220] | 0.995 |
| Postoperative | ||||
| PICU LOS, days | 2.6 [1.8–4.0] | 1.9 [1.0–2.6] | 3.9 [2.9–6.9] | <0.001 |
| Invasive ventilation, hours | 9 [6–22] | 6 [5–10] | 21 [9–21] | 0.001 |
| Prolonged ventilation > 48 h, N(%) | 10 (23) | 1 (4) | 9 (45) | 0.003 |
| Maximum lactate, mmol/L | 2.8 [2.4–3.6] | 2.5 [2.3–3.4] | 3.2 [2.6–3.7] | 0.047 |
| Lowest hemoglobin, mmol/L | 7.1 (0.9) | 7.2 (0.8) | 7.0 (1.0) | 0.551 |
| Highest hemoglobin, mmol/L | 8.7 (1.1) | 8.2 (1.0) | 9.2 (1.0) | 0.003 |
| Lowest serum albumin, g/L | 29 (5) | 32 (4) | 25 (5) | <0.001 |
| Highest creatinine, µmol/L | 41 [33–48] | 38 [33–43] | 44 [37–70] | 0.028 |
| Abdominal catheter, N(%) | 6 (14) | 0 (0) | 5 (30) | 0.006 |
| AKIN | 0.036 | |||
| Stage 1, N(%) | 6 (14) | 3 (13) | 3 (15) | |
| Stage 2, N(%) | 2 (5) | 0 (0) | 2 (10) | |
| Stage 3, N(%) | 3 (7) | 0 (0) | 3 (15) | |
| VIS score | 26 [15–45] | 16 [12–31] | 44 [23–58] | 0.001 |
| Drain duration, days | 4 [3–5] | 3 [2–4] | 4 [4–7] | <0.001 |
| Total drain volume, mL | 1027 [550–1886] | 610 [400–1027] | 1918 [1218–5235] | <0.001 |
| Intake fluids DOS and POD1, mL | 2359 [1956–3186] | 1976 [1711–2353] | 3140 [2604–3803] | <0.001 |
| Predictors | Unstandardized β | 95% CI | p-Value |
|---|---|---|---|
| AOX | 1.007 | 1.002–1.014 | 0.015 |
| Administered Erythrocytes | 1.002 | 1.000–1.005 | 0.017 |
| Highest creatinine | 1.023 | 1.012–1.035 | 0.000 |
| Maximum lactate | 1.358 | 1.164–1.585 | 0.000 |
| Lowest hemoglobin | 0.721 | 0.532–0.977 | 0.036 |
| Lowest serum albumin | 0.883 | 0.853–0.916 | 0.000 |
| Abdominal catheter | 4.487 | 2.286–8.810 | 0.000 |
| FO DOS (%) | 1.122 | 1.014–1.239 | 0.026 |
| FO POD1 (%) | 1.114 | 1.035–1.202 | 0.006 |
| MaxFO (%) | 1.178 | 1.079–1.282 | 0.000 |
| cFO POD1 (%) | 1.096 | 1.040–1.156 | 0.001 |
| cFO POD2 (%) | 1.059 | 1.021–1.099 | 0.004 |
| VIS score | 1.014 | 1.005–1.021 | 0.002 |
| Predictors | Unstandardized β | 95% CI | p-Value |
|---|---|---|---|
| MaxFO (%) | 1.132 | 1.042–1.227 | 0.004 |
| Maximum lactate | 1.271 | 1.096–1.472 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luppes, V.A.C.; Willems, A.; Hazekamp, M.G.; Blom, N.A.; Ten Harkel, A.D.J. Fluid Overload in Pediatric Univentricular Patients Undergoing Fontan Completion. J. Cardiovasc. Dev. Dis. 2023, 10, 156. https://doi.org/10.3390/jcdd10040156
Luppes VAC, Willems A, Hazekamp MG, Blom NA, Ten Harkel ADJ. Fluid Overload in Pediatric Univentricular Patients Undergoing Fontan Completion. Journal of Cardiovascular Development and Disease. 2023; 10(4):156. https://doi.org/10.3390/jcdd10040156
Chicago/Turabian StyleLuppes, Victorien A. C., Ariane Willems, Mark G. Hazekamp, Nico A. Blom, and Arend D. J. Ten Harkel. 2023. "Fluid Overload in Pediatric Univentricular Patients Undergoing Fontan Completion" Journal of Cardiovascular Development and Disease 10, no. 4: 156. https://doi.org/10.3390/jcdd10040156
APA StyleLuppes, V. A. C., Willems, A., Hazekamp, M. G., Blom, N. A., & Ten Harkel, A. D. J. (2023). Fluid Overload in Pediatric Univentricular Patients Undergoing Fontan Completion. Journal of Cardiovascular Development and Disease, 10(4), 156. https://doi.org/10.3390/jcdd10040156