
Dual Antiplatelet Therapy with Parenteral P2Y12 Inhibitors: Rationale, Evidence, and Future Directions




Abstract
:1. Introduction
2. P2Y12 Inhibitor Antiplatelet Agents
2.1. Oral P2Y12 Inhibitors
2.2. Drawbacks of Oral P2Y12 Inhibitors
2.3. Parenteral P2Y12 Inhibitors
3. Efficacy and Safety of Cangrelor: Main Evidence Available
3.1. The CHAMPION Program
3.2. Use of Cangrelor in Combination with Potent Oral P2Y12 Inhibitors
4. Current Recommendations for the Transition from Cangrelor to Oral P2Y12 Inhibitors
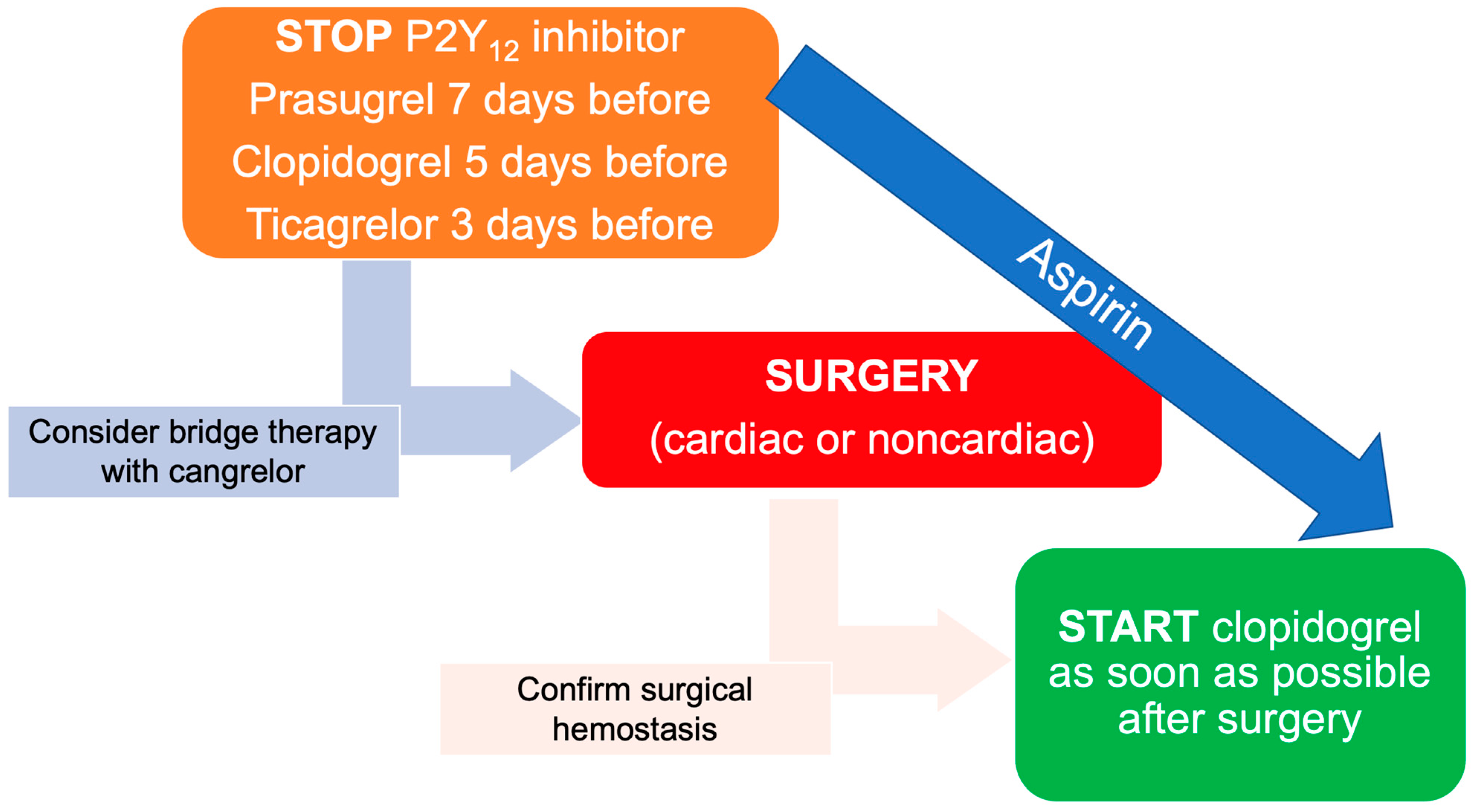
5. Antiplatelet Bridging for CABG and Non-Cardiac Surgery
6. Future Directions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leon, M.B.; Baim, D.S.; Popma, J.J.; Gordon, P.C.; Cutlip, D.E.; Ho, K.K.; Giambartolomei, A.; Diver, D.J.; Lasorda, D.M.; Williams, D.O.; et al. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. Stent Anticoagulation Restenosis Study Investigators. N. Engl. J. Med. 1998, 339, 1665–1671. [Google Scholar] [CrossRef] [PubMed]
- Schömig, A.; Neumann, F.J.; Kastrati, A.; Schühlen, H.; Blasini, R.; Hadamitzky, M.; Walter, H.; Zitzmann-Roth, E.M.; Richardt, G.; Alt, E.; et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N. Engl. J. Med. 1996, 334, 1084–1089. [Google Scholar] [CrossRef]
- McFadden, E.P.; Stabile, E.; Regar, E.; Cheneau, E.; Ong, A.T.; Kinnaird, T.; Suddath, W.O.; Weissman, N.J.; Torguson, R.; Kent, K.M.; et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet 2004, 364, 1519–1521. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [Green Version]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Bhatt, D.L.; Cohen, M.; Steg, P.G.; Storey, R.F.; Jensen, E.C.; Magnani, G.; Bansilal, S.; Fish, M.P.; Im, K.; et al. Long-term use of ticagrelor in patients with prior myocardial infarction. N. Engl. J. Med. 2015, 372, 1791–1800. [Google Scholar] [CrossRef] [Green Version]
- Yeh, R.W.; Kereiakes, D.J.; Steg, P.G.; Windecker, S.; Rinaldi, M.J.; Gershlick, A.H.; Cutlip, D.E.; Cohen, D.J.; Tanguay, J.F.; Jacobs, A.; et al. Benefits and Risks of Extended Duration Dual Antiplatelet Therapy After PCI in Patients With and Without Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2015, 65, 2211–2221. [Google Scholar] [CrossRef] [Green Version]
- Ando, G.; De Santis, G.A.; Greco, A.; Pistelli, L.; Francaviglia, B.; Capodanno, D.; De Caterina, R.; Capranzano, P. P2Y(12) Inhibitor or Aspirin Following Dual Antiplatelet Therapy After Percutaneous Coronary Intervention: A Network Meta-Analysis. JACC Cardiovasc. Interv. 2022, 15, 2239–2249. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Maehara, A.; Kwong, R.Y.; Sedlak, T.; Saw, J.; Smilowitz, N.R.; Mahmud, E.; Wei, J.; Marzo, K.; Matsumura, M.; et al. Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction With Nonobstructive Coronary Arteries in Women. Circulation 2021, 143, 624–640. [Google Scholar] [CrossRef] [PubMed]
- Waterbury, T.M.; Tarantini, G.; Vogel, B.; Mehran, R.; Gersh, B.J.; Gulati, R. Non-atherosclerotic causes of acute coronary syndromes. Nat. Rev. Cardiol. 2020, 17, 229–241. [Google Scholar] [CrossRef]
- Ando, G.; Trio, O.; de Gregorio, C. Transient left ventricular dysfunction in patients with neurovascular events. Acute Card Care 2010, 12, 70–74. [Google Scholar] [CrossRef]
- Tarantini, G.; Mojoli, M.; Varbella, F.; Caporale, R.; Rigattieri, S.; Ando, G.; Cirillo, P.; Pierini, S.; Santarelli, A.; Sganzerla, P.; et al. Timing of Oral P2Y(12) Inhibitor Administration in Patients With Non-ST-Segment Elevation Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2020, 76, 2450–2459. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Zhao, F.; Mehta, S.R.; Chrolavicius, S.; Tognoni, G.; Fox, K.K. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N. Engl. J. Med. 2001, 345, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurbel, P.A.; Tantry, U.S. Drug insight: Clopidogrel nonresponsiveness. Nat. Clin. Pract. Cardiovasc. Med. 2006, 3, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.L.; Samant, S.; Lesko, L.J.; Schmidt, S. Clinical pharmacokinetics and pharmacodynamics of clopidogrel. Clin Pharmacokinet 2015, 54, 147–166. [Google Scholar] [CrossRef] [Green Version]
- Brandt, J.T.; Payne, C.D.; Wiviott, S.D.; Weerakkody, G.; Farid, N.A.; Small, D.S.; Jakubowski, J.A.; Naganuma, H.; Winters, K.J. A comparison of prasugrel and clopidogrel loading doses on platelet function: Magnitude of platelet inhibition is related to active metabolite formation. Am. Heart J. 2007, 153, 66.e9–66.e16. [Google Scholar] [CrossRef]
- Schüpke, S.; Neumann, F.J.; Menichelli, M.; Mayer, K.; Bernlochner, I.; Wöhrle, J.; Richardt, G.; Liebetrau, C.; Witzenbichler, B.; Antoniucci, D.; et al. Ticagrelor or Prasugrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2019, 381, 1524–1534. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Cattaneo, M.; Faioni, E.M. Why does ticagrelor induce dyspnea? Thromb. Haemost. 2012, 108, 1031–1036. [Google Scholar] [CrossRef]
- Alexopoulos, D.; Xanthopoulou, I.; Gkizas, V.; Kassimis, G.; Theodoropoulos, K.C.; Makris, G.; Koutsogiannis, N.; Damelou, A.; Tsigkas, G.; Davlouros, P.; et al. Randomized assessment of ticagrelor versus prasugrel antiplatelet effects in patients with ST-segment-elevation myocardial infarction. Circ. Cardiovasc. Interv. 2012, 5, 797–804. [Google Scholar] [CrossRef] [Green Version]
- Valgimigli, M.; Tebaldi, M.; Campo, G.; Gambetti, S.; Bristot, L.; Monti, M.; Parrinello, G.; Ferrari, R. Prasugrel versus tirofiban bolus with or without short post-bolus infusion with or without concomitant prasugrel administration in patients with myocardial infarction undergoing coronary stenting: The FABOLUS PRO (Facilitation through Aggrastat By drOpping or shortening Infusion Line in patients with ST-segment elevation myocardial infarction compared to or on top of PRasugrel given at loading dOse) trial. JACC Cardiovasc. Interv. 2012, 5, 268–277. [Google Scholar] [CrossRef] [Green Version]
- Parodi, G.; Valenti, R.; Bellandi, B.; Migliorini, A.; Marcucci, R.; Comito, V.; Carrabba, N.; Santini, A.; Gensini, G.F.; Abbate, R.; et al. Comparison of prasugrel and ticagrelor loading doses in ST-segment elevation myocardial infarction patients: RAPID (Rapid Activity of Platelet Inhibitor Drugs) primary PCI study. J. Am. Coll. Cardiol. 2013, 61, 1601–1606. [Google Scholar] [CrossRef] [Green Version]
- Parodi, G.; Xanthopoulou, I.; Bellandi, B.; Gkizas, V.; Valenti, R.; Karanikas, S.; Migliorini, A.; Angelidis, C.; Abbate, R.; Patsilinakos, S.; et al. Ticagrelor crushed tablets administration in STEMI patients: The MOJITO study. J. Am. Coll. Cardiol. 2015, 65, 511–512. [Google Scholar] [CrossRef] [Green Version]
- Rollini, F.; Franchi, F.; Hu, J.; Kureti, M.; Aggarwal, N.; Durairaj, A.; Park, Y.; Seawell, M.; Cox-Alomar, P.; Zenni, M.M.; et al. Crushed Prasugrel Tablets in Patients With STEMI Undergoing Primary Percutaneous Coronary Intervention: The CRUSH Study. J. Am. Coll. Cardiol. 2016, 67, 1994–2004. [Google Scholar] [CrossRef] [PubMed]
- Venetsanos, D.; Sederholm Lawesson, S.; Swahn, E.; Alfredsson, J. Chewed ticagrelor tablets provide faster platelet inhibition compared to integral tablets: The inhibition of platelet aggregation after administration of three different ticagrelor formulations (IPAAD-Tica) study, a randomised controlled trial. Thromb. Res. 2017, 149, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orme, R.C.; Parker, W.A.E.; Thomas, M.R.; Judge, H.M.; Baster, K.; Sumaya, W.; Morgan, K.P.; McMellon, H.C.; Richardson, J.D.; Grech, E.D.; et al. Study of Two Dose Regimens of Ticagrelor Compared with Clopidogrel in Patients Undergoing Percutaneous Coronary Intervention for Stable Coronary Artery Disease (STEEL-PCI). Circulation 2018, 138, 1290–1300. [Google Scholar] [CrossRef]
- Serenelli, M.; Pavasini, R.; Vitali, F.; Tonet, E.; Bilotta, F.; Parodi, G.; Campo, G. Efficacy and safety of alternative oral administrations of P2Y12-receptor inhibitors: Systematic review and meta-analysis. J. Thromb. Haemost. 2019, 17, 944–950. [Google Scholar] [CrossRef]
- Capranzano, P.; Angiolillo, D.J. Tackling the gap in platelet inhibition with oral antiplatelet agents in high-risk patients undergoing percutaneous coronary intervention. Expert. Rev. Cardiovasc. Ther. 2021, 19, 519–535. [Google Scholar] [CrossRef]
- Reilly, P.M.; Wilkins, K.B.; Fuh, K.C.; Haglund, U.; Bulkley, G.B. The mesenteric hemodynamic response to circulatory shock: An overview. Shock 2001, 15, 329–343. [Google Scholar] [CrossRef]
- Wakabayashi, S.; Kitahara, H.; Nishi, T.; Sugimoto, K.; Nakayama, T.; Fujimoto, Y.; Ariyoshi, N.; Kobayashi, Y. Platelet inhibition after loading dose of prasugrel in patients with ST-elevation and non-ST-elevation acute coronary syndrome. Cardiovasc. Interv. Ther. 2018, 33, 239–246. [Google Scholar] [CrossRef]
- Parodi, G.; Talanas, G.; Mura, E.; Canonico, M.E.; Siciliano, R.; Guarino, S.; Marini, A.; Dossi, F.; Franca, P.; Raccis, M.; et al. Orodispersible Ticagrelor in Acute Coronary Syndromes: The TASTER Study. J. Am. Coll. Cardiol. 2021, 78, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Schilling, U.; Dingemanse, J.; Ufer, M. Pharmacokinetics and Pharmacodynamics of Approved and Investigational P2Y12 Receptor Antagonists. Clin. Pharmacokinet. 2020, 59, 545–566. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Stone, G.W.; Mahaffey, K.W.; Gibson, C.M.; Steg, P.G.; Hamm, C.W.; Price, M.J.; Leonardi, S.; Gallup, D.; Bramucci, E.; et al. Effect of platelet inhibition with cangrelor during PCI on ischemic events. N. Engl. J. Med. 2013, 368, 1303–1313. [Google Scholar] [CrossRef] [Green Version]
- Zwart, B.; Parker, W.A.E.; Storey, R.F. New Antithrombotic Drugs in Acute Coronary Syndrome. J. Clin. Med. 2020, 9, 2059. [Google Scholar] [CrossRef]
- Caroff, E.; Meyer, E.; Treiber, A.; Hilpert, K.; Riederer, M.A. Optimization of 2-phenyl-pyrimidine-4-carboxamides towards potent, orally bioavailable and selective P2Y(12) antagonists for inhibition of platelet aggregation. Bioorg. Med. Chem. Lett. 2014, 24, 4323–4331. [Google Scholar] [CrossRef]
- Parker, W.A.E.; Storey, R.F. Novel approaches to P2Y(12) inhibition and aspirin dosing. Platelets 2021, 32, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Rey, M.; Kramberg, M.; Hess, P.; Morrison, K.; Ernst, R.; Haag, F.; Weber, E.; Clozel, M.; Baumann, M.; Caroff, E.; et al. The reversible P2Y(12) antagonist ACT-246475 causes significantly less blood loss than ticagrelor at equivalent antithrombotic efficacy in rat. Pharmacol. Res. Perspect. 2017, 5, e00338. [Google Scholar] [CrossRef] [Green Version]
- Ufer, M.; Huynh, C.; van Lier, J.J.; Caroff, E.; Fischer, H.; Dingemanse, J. Absorption, distribution, metabolism and excretion of the P2Y12 receptor antagonist selatogrel after subcutaneous administration in healthy subjects. Xenobiotica 2020, 50, 427–434. [Google Scholar] [CrossRef]
- Storey, R.F.; Gurbel, P.A.; Ten Berg, J.; Bernaud, C.; Dangas, G.D.; Frenoux, J.M.; Gorog, D.A.; Hmissi, A.; Kunadian, V.; James, S.K.; et al. Pharmacodynamics, pharmacokinetics, and safety of single-dose subcutaneous administration of selatogrel, a novel P2Y12 receptor antagonist, in patients with chronic coronary syndromes. Eur. Heart J. 2020, 41, 3132–3140. [Google Scholar] [CrossRef] [Green Version]
- Sinnaeve, P.; Fahrni, G.; Schelfaut, D.; Spirito, A.; Mueller, C.; Frenoux, J.M.; Hmissi, A.; Bernaud, C.; Ufer, M.; Moccetti, T.; et al. Subcutaneous Selatogrel Inhibits Platelet Aggregation in Patients With Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2020, 75, 2588–2597. [Google Scholar] [CrossRef]
- Valgimigli, M.; Landi, A. Subcutaneous RUC-4 for acute myocardial infarction: A new treatment on the horizon for pre-hospital care? EuroIntervention 2021, 17, e362–e363. [Google Scholar] [CrossRef]
- Kereiakes, D.J.; Henry, T.D.; DeMaria, A.N.; Bentur, O.; Carlson, M.; Seng Yue, C.; Martin, L.H.; Midkiff, J.; Mueller, M.; Meek, T.; et al. First Human Use of RUC-4: A Nonactivating Second-Generation Small-Molecule Platelet Glycoprotein IIb/IIIa (Integrin alphaIIbbeta3) Inhibitor Designed for Subcutaneous Point-of-Care Treatment of ST-Segment-Elevation Myocardial Infarction. J. Am. Heart Assoc. 2020, 9, e016552. [Google Scholar] [CrossRef]
- Bor, W.L.; Zheng, K.L.; Tavenier, A.H.; Gibson, C.M.; Granger, C.B.; Bentur, O.; Lobatto, R.; Postma, S.; Coller, B.S.; van ’t Hof, A.W.J.; et al. Pharmacokinetics, pharmacodynamics, and tolerability of subcutaneous administration of a novel glycoprotein IIb/IIIa inhibitor, RUC-4, in patients with ST-segment elevation myocardial infarction. EuroIntervention 2021, 17, e401–e410. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J.; Bhatt, D.L.; Steg, P.G.; Stone, G.W.; White, H.D.; Gibson, C.M.; Hamm, C.W.; Price, M.J.; Prats, J.; Liu, T.; et al. Impact of cangrelor overdosing on bleeding complications in patients undergoing percutaneous coronary intervention: Insights from the CHAMPION trials. J. Thromb. Thrombolysis 2015, 40, 317–322. [Google Scholar] [CrossRef]
- Franchi, F.; Rollini, F.; Park, Y.; Angiolillo, D.J. A Safety Evaluation of Cangrelor in Patients Undergoing PCI. Expert Opin. Drug Saf. 2016, 15, 275–285. [Google Scholar] [CrossRef]
- Leonardi, S.; Bhatt, D.L. Practical considerations for cangrelor use in patients with acute coronary syndromes. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 39–44. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Lincoff, A.M.; Gibson, C.M.; Stone, G.W.; McNulty, S.; Montalescot, G.; Kleiman, N.S.; Goodman, S.G.; White, H.D.; Mahaffey, K.W.; et al. Intravenous platelet blockade with cangrelor during PCI. N. Engl. J. Med. 2009, 361, 2330–2341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [Green Version]
- Harrington, R.A.; Stone, G.W.; McNulty, S.; White, H.D.; Lincoff, A.M.; Gibson, C.M.; Pollack, C.V., Jr.; Montalescot, G.; Mahaffey, K.W.; Kleiman, N.S.; et al. Platelet inhibition with cangrelor in patients undergoing PCI. N. Engl. J. Med. 2009, 361, 2318–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, K.Y.; Mahaffey, K.W. Cangrelor in clinical use. Future Cardiol. 2020, 16, 89–102. [Google Scholar] [CrossRef]
- White, H.D.; Chew, D.P.; Dauerman, H.L.; Mahaffey, K.W.; Gibson, C.M.; Stone, G.W.; Gruberg, L.; Harrington, R.A.; Bhatt, D.L. Reduced immediate ischemic events with cangrelor in PCI: A pooled analysis of the CHAMPION trials using the universal definition of myocardial infarction. Am. Heart J. 2012, 163, 182–190.e184. [Google Scholar] [CrossRef]
- Abtan, J.; Steg, P.G.; Stone, G.W.; Mahaffey, K.W.; Gibson, C.M.; Hamm, C.W.; Price, M.J.; Abnousi, F.; Prats, J.; Deliargyris, E.N.; et al. Efficacy and Safety of Cangrelor in Preventing Periprocedural Complications in Patients With Stable Angina and Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention: The CHAMPION PHOENIX Trial. JACC Cardiovasc. Interv. 2016, 9, 1905–1913. [Google Scholar] [CrossRef] [PubMed]
- Steg, P.G.; Bhatt, D.L.; Hamm, C.W.; Stone, G.W.; Gibson, C.M.; Mahaffey, K.W.; Leonardi, S.; Liu, T.; Skerjanec, S.; Day, J.R.; et al. Effect of cangrelor on periprocedural outcomes in percutaneous coronary interventions: A pooled analysis of patient-level data. Lancet 2013, 382, 1981–1992. [Google Scholar] [CrossRef]
- Franchi, F.; Rollini, F.; Rivas, A.; Wali, M.; Briceno, M.; Agarwal, M.; Shaikh, Z.; Nawaz, A.; Silva, G.; Been, L.; et al. Platelet Inhibition With Cangrelor and Crushed Ticagrelor in Patients With ST-Segment-Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention. Circulation 2019, 139, 1661–1670. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, M.A.; Andell, P.; Koul, S.; James, S.; Scherstén, F.; Götberg, M.; Erlinge, D. Cangrelor in combination with ticagrelor provides consistent and potent P2Y12-inhibition during and after primary percutaneous coronary intervention in real-world patients with ST-segment-elevation myocardial infarction. Platelets 2017, 28, 414–416. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, D.; Pappas, C.; Sfantou, D.; Xanthopoulou, I.; Didagelos, M.; Kikas, P.; Ziakas, A.; Tziakas, D.; Karvounis, H.; Iliodromitis, E. Cangrelor in Ticagrelor-Loaded STEMI Patients Undergoing Primary Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2018, 72, 1750–1751. [Google Scholar] [CrossRef]
- Franchi, F.; Ortega-Paz, L.; Rollini, F.; Galli, M.; Been, L.; Ghanem, G.; Shalhoub, A.; Ossi, T.; Rivas, A.; Zhou, X.; et al. Cangrelor in Patients With Coronary Artery Disease Pretreated With Ticagrelor: The Switching Antiplatelet (SWAP)-5 Study. JACC Cardiovasc. Interv. 2023, 16, 36–46. [Google Scholar] [CrossRef]
- Grimfjärd, P.; Lagerqvist, B.; Erlinge, D.; Varenhorst, C.; James, S. Clinical use of cangrelor: Nationwide experience from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). Eur. Heart J. Cardiovasc. Pharmacother. 2019, 5, 151–157. [Google Scholar] [CrossRef]
- Franchi, F.; Rollini, F.; Angiolillo, D.J. Antithrombotic therapy for patients with STEMI undergoing primary PCI. Nat. Rev. Cardiol. 2017, 14, 361–379. [Google Scholar] [CrossRef]
- Franchi, F.; Rollini, F.; Park, Y.; Hu, J.; Kureti, M.; Rivas Rios, J.; Faz, G.; Yaranov, D.; Been, L.; Pineda, A.M.; et al. Effects of Methylnaltrexone on Ticagrelor-Induced Antiplatelet Effects in Coronary Artery Disease Patients Treated With Morphine. JACC Cardiovasc. Interv. 2019, 12, 1538–1549. [Google Scholar] [CrossRef] [PubMed]
- Rymer, J.A.; Bhatt, D.L.; Angiolillo, D.J.; Diaz, M.; Garratt, K.N.; Waksman, R.; Edwards, L.; Tasissa, G.; Salahuddin, K.; El-Sabae, H.; et al. Cangrelor Use Patterns and Transition to Oral P2Y(12) Inhibitors Among Patients With Myocardial Infarction: Initial Results From the CAMEO Registry. J. Am. Heart Assoc. 2022, 11, e024513. [Google Scholar] [CrossRef] [PubMed]
- Kordis, P.; Bozic Mijovski, M.; Berden, J.; Steblovnik, K.; Blinc, A.; Noc, M. Cangrelor for comatose survivors of out-of-hospital cardiac arrest undergoing percutaneous coronary intervention: The CANGRELOR-OHCA study. EuroIntervention 2023, 18, 1269–1271. [Google Scholar] [CrossRef] [PubMed]
- De Luca, L.; Calabrò, P.; Chirillo, F.; Rolfo, C.; Menozzi, A.; Capranzano, P.; Menichelli, M.; Nicolini, E.; Mauro, C.; Trani, C.; et al. Use of cangrelor in patients with acute coronary syndromes undergoing percutaneous coronary intervention: Study design and interim analysis of the ARCANGELO study. Clin. Cardiol. 2022, 45, 913–920. [Google Scholar] [CrossRef]
- Hochholzer, W.; Kleiner, P.; Younas, I.; Valina, C.M.; Loffelhardt, N.; Amann, M.; Bomicke, T.; Ferenc, M.; Hauschke, D.; Trenk, D.; et al. Randomized Comparison of Oral P2Y(12)-Receptor Inhibitor Loading Strategies for Transitioning From Cangrelor: The ExcelsiorLOAD2 Trial. JACC Cardiovasc. Interv. 2017, 10, 121–129. [Google Scholar] [CrossRef]
- Rollini, F.; Franchi, F.; Angiolillo, D.J. Drug-Drug Interactions When Switching Between Intravenous and Oral P2Y(12) Receptor Inhibitors: How Real Is It? JACC Cardiovasc. Interv. 2017, 10, 130–132. [Google Scholar] [CrossRef]
- Gargiulo, G.; Esposito, G.; Avvedimento, M.; Nagler, M.; Minuz, P.; Campo, G.; Gragnano, F.; Manavifar, N.; Piccolo, R.; Tebaldi, M.; et al. Cangrelor, Tirofiban, and Chewed or Standard Prasugrel Regimens in Patients With ST-Segment-Elevation Myocardial Infarction: Primary Results of the FABOLUS-FASTER Trial. Circulation 2020, 142, 441–454. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Schneider, D.J.; Bhatt, D.L.; French, W.J.; Price, M.J.; Saucedo, J.F.; Shaburishvili, T.; Huber, K.; Prats, J.; Liu, T.; et al. Pharmacodynamic effects of cangrelor and clopidogrel: The platelet function substudy from the cangrelor versus standard therapy to achieve optimal management of platelet inhibition (CHAMPION) trials. J. Thromb. Thrombolysis 2012, 34, 44–55. [Google Scholar] [CrossRef]
- Schneider, D.J.; Seecheran, N.; Raza, S.S.; Keating, F.K.; Gogo, P. Pharmacodynamic effects during the transition between cangrelor and prasugrel. Coron Artery Dis. 2015, 26, 42–48. [Google Scholar] [CrossRef]
- Schneider, D.J.; Agarwal, Z.; Seecheran, N.; Keating, F.K.; Gogo, P. Pharmacodynamic effects during the transition between cangrelor and ticagrelor. JACC Cardiovasc. Interv. 2014, 7, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, G.; Marenna, A.; Sperandeo, L.; Manzi, L.; Avvedimento, M.; Simonetti, F.; Canonico, M.E.; Paolillo, R.; Spinelli, A.; Borgia, F.; et al. Pharmacodynamic effects of cangrelor in elective complex PCI: Insights from the POMPEII Registry. EuroIntervention 2023, 18, 1266–1268. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Firstenberg, M.S.; Price, M.J.; Tummala, P.E.; Hutyra, M.; Welsby, I.J.; Voeltz, M.D.; Chandna, H.; Ramaiah, C.; Brtko, M.; et al. Bridging antiplatelet therapy with cangrelor in patients undergoing cardiac surgery: A randomized controlled trial. JAMA 2012, 307, 265–274. [Google Scholar] [CrossRef]
- Rossini, R.; Tarantini, G.; Musumeci, G.; Masiero, G.; Barbato, E.; Calabrò, P.; Capodanno, D.; Leonardi, S.; Lettino, M.; Limbruno, U.; et al. A Multidisciplinary Approach on the Perioperative Antithrombotic Management of Patients With Coronary Stents Undergoing Surgery: Surgery After Stenting 2. JACC Cardiovasc. Interv. 2018, 11, 417–434. [Google Scholar] [CrossRef]
- Rossini, R.; Masiero, G.; Fruttero, C.; Passamonti, E.; Calvaruso, E.; Cecconi, M.; Carlucci, C.; Mojoli, M.; Guido, P.; Talanas, G.; et al. Antiplatelet Therapy with Cangrelor in Patients Undergoing Surgery after Coronary Stent Implantation: A Real-World Bridging Protocol Experience. TH Open 2020, 4, e437–e445. [Google Scholar] [CrossRef]


{kind=link}
| CHAMPION PLATFORM | CHAMPION PCI | CHAMPION PHOENIX | |
|---|---|---|---|
| Years | 2007–2009 | 2007–2009 | 2010–2012 |
| Patients (n) | 5362 | 8877 | 11,145 |
| Diagnosis | NSTE-ACS (94.8%); stable angina (5.2%) | STEMI (11.2%); NSTE-ACS (73.8%); stable angina (1.5%) | STEMI (18%); NSTE-ACS (25.7%); stable angina (62.3%) |
| Antiplatelet therapy | Clopidogrel naïve | Clopidogrel | Clopidogrel naïve |
| Treatment | Cangrelor: 30 μg/kg bolus, 4 μg/kg/min infusion | Cangrelor: 30 μg/kg bolus, 4 μg/kg/min infusion | Cangrelor: 30 μg/kg bolus, 4 μg/kg/min infusion |
| Transition to clopidogrel | Clopidogrel 600 mg at the end of cangrelor infusion | Clopidogrel 600 mg at the end of cangrelor infusion | Clopidogrel 600 mg at the end of cangrelor infusion |
| Control arm | Placebo | Clopidogrel 600 mg | Clopidogrel 600 mg or 300 mg |
| Definition of myocardial infarction | Clinical | Clinical | Universal definition |
| Primary composite endpoint | Death, MI, IDR at 48 h | Death, MI, IDR at 48 h | Death, MI, IDR at 48 h |
| Results | OR 0.87 (95% CI 0.71–1.07; p = 0.17) | OR 1.05 (95% CI 0.88–1.24; p = 0.59) | OR 0.78 (95% CI 0.66–0.93; p = 0.005) |
| Cangrelor Group | Placebo Group | p-Value | |
|---|---|---|---|
| Patients, n | 22 | 22 | |
| Diagnosis | STEMI | STEMI | |
| Treatment | Cangrelor: 30 μg/kg 2 h bolus, 4 μg/kg/min infusion | Placebo | |
|
Time from bolus to end of PCI, min (SD) | 39 (18–51) | 33 (26–60) | |
| Transition to ticagrelor | Crushed ticagrelor 180 mg | Crushed ticagrelor 180 mg | |
| HPR at baseline, n HPR during cangrelor 5 min, n (%) 30 min, n (%) End of PCI, n (%) 1 h, n (%) 2 h, n (%) HPR post cangrelor 1 h, n (%) 2 h, n (%) | 15 (68%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 2 (10%) 1 (5%) | 15 (68%) 15 (71%) 12 (57%) 13 (62%) 8 (38%) 6 (33%) 2 (12%) 1 (6%) | NS <0.001 <0.001 <0.001 0.003 0.007 NS NS |
| Rates | p-Values | |||||||
|---|---|---|---|---|---|---|---|---|
| Tirofiban | Cangrelor | Chewed Prasugrel | Integral Prasugrel | Tirofiban vs. Cangrelor | Tirofiban vs. Chewed Prasugrel | Cangrelor vs. Chewed Prasugrel | Chewed Prasugrel vs. Integral Prasugrel | |
|
>59% LTA with ADP 20 µmol/L 15 min 30 min 1 h 2 h 3 h 4 to 6 h | 0.0% 0.0% 0.0% 0.0% 7.5% 7.5% | 57.5% 55.0% 55.0% 50.0% 81.6% 68.4% | 100.0% 90.5% 66.7% 38.1% 28.6% 33.3% | 95.2% 95.2% 81.0% 52.4% 19.0% 19.0% | <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 | <0.001 <0.001 <0.001 <0.001 0.030 0.014 | <0.001 0.012 NS NS <0.001 0.009 | NS NS NS NS NS NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alagna, G.; Mazzone, P.; Contarini, M.; Andò, G. Dual Antiplatelet Therapy with Parenteral P2Y12 Inhibitors: Rationale, Evidence, and Future Directions. J. Cardiovasc. Dev. Dis. 2023, 10, 163. https://doi.org/10.3390/jcdd10040163
Alagna G, Mazzone P, Contarini M, Andò G. Dual Antiplatelet Therapy with Parenteral P2Y12 Inhibitors: Rationale, Evidence, and Future Directions. Journal of Cardiovascular Development and Disease. 2023; 10(4):163. https://doi.org/10.3390/jcdd10040163
Chicago/Turabian StyleAlagna, Giulia, Paolo Mazzone, Marco Contarini, and Giuseppe Andò. 2023. "Dual Antiplatelet Therapy with Parenteral P2Y12 Inhibitors: Rationale, Evidence, and Future Directions" Journal of Cardiovascular Development and Disease 10, no. 4: 163. https://doi.org/10.3390/jcdd10040163
APA StyleAlagna, G., Mazzone, P., Contarini, M., & Andò, G. (2023). Dual Antiplatelet Therapy with Parenteral P2Y12 Inhibitors: Rationale, Evidence, and Future Directions. Journal of Cardiovascular Development and Disease, 10(4), 163. https://doi.org/10.3390/jcdd10040163