
Early and Long-Term Clinical and Echocardiographic Outcomes of Sutureless vs. Sutured Bioprosthesis for Aortic Valve Replacement





Abstract
:1. Introduction
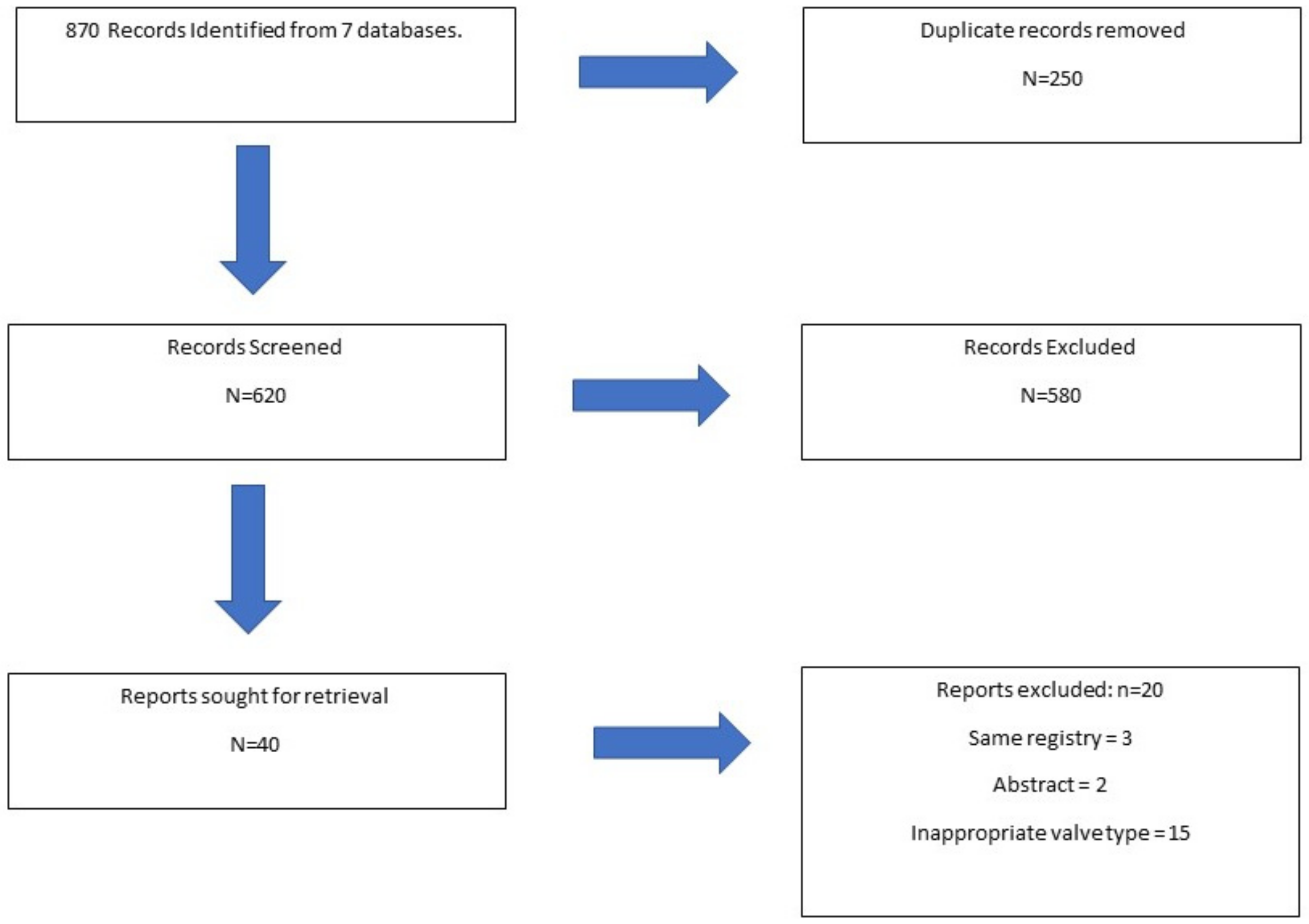
2. Material and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Data Collection
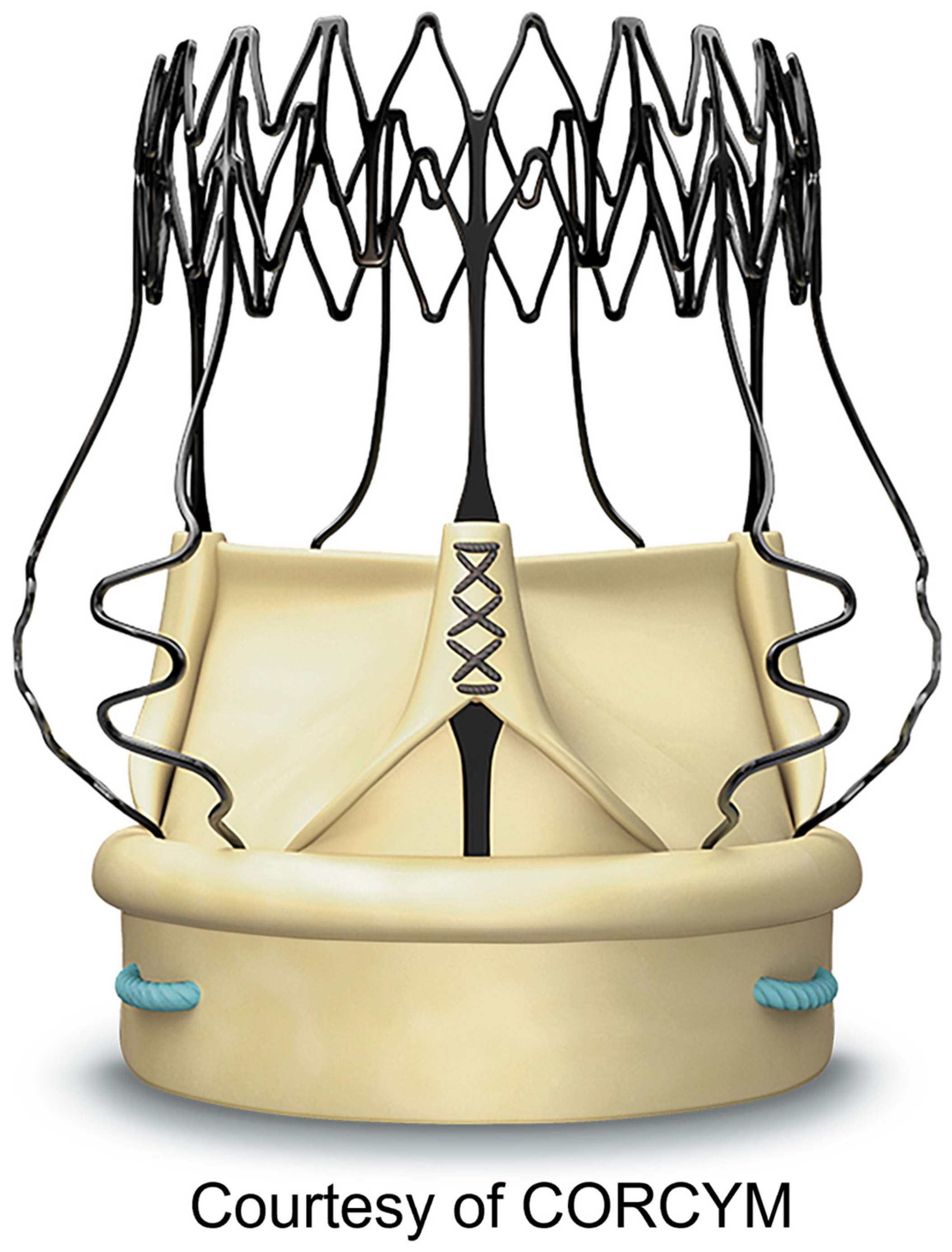
2.4. Surgical Technique for Perceval Sutureless Valve Implantation
3. Results
3.1. Sutureless vs. Sutured Bioprosthesis
3.2. Perceval in Bicuspid Native Aortic Valves
3.3. Echocardiographic Outcomes
3.4. Hospital Costs Outcomes
4. Discussion
Summary of Findings
- (1)
- SU-AVR had a lower incidence of in-hospital complications and overall mortality when compared to SB.
- (2)
- SU-AVR had the lowest hospital costs when compared to SB bioprosthesis.
5. Comments
5.1. Outcomes of Sutureless Valves
5.2. Long-Term Clinical Outcomes
5.3. Long-Term Echocardiographic Outcomes
5.4. Reported Cost Outcomes
5.5. Comparison with Other Literature Reviews
5.6. Comparison with Our Previous Study
5.7. Future Perspectives
6. Conclusions
7. Learning Objectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Glossary of Abbreviations
| TAVR | transcatheter aortic valve replacement |
| CPB | cardiopulmonary bypass |
| PPI | permanent pacemaker implantation |
| BAV | bicuspid aortic valve |
| MI | myocardial infarction |
| PVL | paravalvular leak |
| SAVR | surgical aortic valve replacement |
| SU-AVR | sutureless aortic valve replacement |
| SB | sutured bioprosthesis. |
References
- Santarpino, G.; Pfeiffer, S.; Concistre, G.; Grossmann, I.; Hinzmann, M.; Fischlein, T. The Perceval S aortic valve has the potential of shortening surgical time: Does it also result in improved outcome? Ann. Thorac. Surg. 2013, 96, 77–81. [Google Scholar] [CrossRef]
- Dokollari, A.; Ramlawi, B.; Torregrossa, G.; Sá, M.P.; Sicouri, S.; Prifti, E.; Gelsomino, S.; Bonacchi, M. Benefits and Pitfalls of the Perceval Sutureless Bioprosthesis. Front. Cardiovasc. Med. 2022, 8, 789392. [Google Scholar] [CrossRef]
- Dokollari, A.; Torregrossa, G.; Sicouri, S.; Veshti, A.; Margaryan, R.; Cameli, M.; Mandoli, G.E.; Maccherini, M.; Montesi, G.; Cabrucci, F.; et al. Pearls, pitfalls, and surgical indications of the Intuity TM heart valve: A rapid deployment bioprosthesis. A systematic review of the literature. J. Card. Surg. 2022, 37, 5411–5417. [Google Scholar] [CrossRef] [PubMed]
- Sá, M.P.; Jabagi, H.; Dokollari, A.; Awad, A.K.; Van den Eynde, J.; Malin, J.H.; Sicouri, S.; Torregrossa, G.; Ruhparwar, A.; Weymann, A.; et al. Early and late outcomes of surgical aortic valve replacement with sutureless and rapid-deployment valves versus transcatheter aortic valve implantation: Meta-analysis with reconstructed time-to-event data of matched studies. Catheter. Cardiovasc. Interv. 2022, 99, 1886–1896. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Reardon, M.R.; Mieghem, N.M.V.; Pompa, J.J.; Kleiman, N.S.; Sondergaard, L.; Mumtaz, M.; Adams, D.H.; Deeb, G.M.; Maini, B.; Gada, H.; et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2017, 376, 1321–1331. [Google Scholar] [CrossRef]
- Powell, R.; Pelletier, M.P.; Chu, M.W.A.; Bouchard, D.; Melvin, K.N.; Adams, C. The Perceval Sutureless Aortic Valve: Review of Outcomes, Complications, and Future Direction. Innovations 2017, 12, 155–173. [Google Scholar] [CrossRef]
- Dokollari, A.; Cameli, M.; Mandoli, G.E.; Kalra, D.S.; Poston, R.; Coku, L.; Pernoci, M.; Miri, M.; Bonacchi, M.; Gelsomino, S. Early and Midterm Clinical Outcomes of Transcatheter Valve-in-Valve Implantation Versus Redo Surgical Aortic Valve Replacement for Aortic Bioprosthetic Valve Degeneration: Two Faces of the Same Medal. J. Cardiothorac. Vasc. Anesth. 2021, 24, 3223–3231. [Google Scholar] [CrossRef]
- Sá, M.P.; Van den Eynde, J.; Simonato, M.; Hirji, S.; Erten, O.; Jacquemyn, X.; Tasoudis, P.; Dokollari, A.; Sicouri, S.; Weymann, A.; et al. Late outcomes of valve-in-valve transcatheter aortic valve implantation versus re-replacement: Meta-analysis of reconstructed time-to-event data. Int. J. Cardiol. 2023, 370, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Biancari, F.; Barbanti, M.; Santarpino, G.; Deste, W.; Tamburrino, C.; Gulino, S.; Immè, S.; Di Simone, E.; Todaro, D.; Pollari, F.; et al. Immediate outcome after sutureless versus transcatheter aortic valve replacement. Heart Vessels 2016, 31, 427–433. [Google Scholar] [CrossRef]
- Muneretto, C.; Solinas, M.; Folliguet, T.; Di Bartolomeo, R.; Repossini, A.; Laborde, F.; Rambaldini, M.; Santarpino, G.; Di Bacco, L.; Fischlein, T. Sutureless versus transcatheter aortic valves in elderly patients with aortic stenosis at intermediate risk: A multi-institutional study. J. Thorac. Cardiovasc. Surg. 2020, 163, 925–935.e5. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, A.; Rizzoli, G.; Messina, A.; Alfieri, O.; Lorusso, R.; Salizzoni, S.; Glauber, M.; Di Bartolomeo, R.; Besola, L.; Rinaldi, M.; et al. Conventional surgery, sutureless valves, and transapical aortic valve replacement: What is the best option for patients with aortic valve stenosis? A multicenter, propensity-matched analysis. J. Thorac. Cardiovasc. Surg. 2013, 146, 1065–1070. [Google Scholar] [CrossRef]
- Santarpino, G.; Pfeiffer, S.; Jessl, J.; Dell’Aquila, A.M.; Pollari, F.; Pauschinger, M.; Fischlein, T. Sutureless replacement versus transcatheter valve implantation in aortic valve stenosis: A propensity matched analysis of 2 strategies in high-risk patients. J. Thorac. Cardiovasc. Surg. 2014, 147, 561–567. [Google Scholar] [CrossRef]
- Miceli, A.; Gilmanov, D.; Murzi, M.; Marchi, F.; Ferrarini, M.; Cerillo, A.G.; Quaini, E.; Solinas, M.; Berti, S.; Glauber, M. Minimally invasive aortic valve replacement with a sutureless valve through a right anterior mini-thoracotomy versus transcatheter aortic valve implantation in high-risk patients. Eur. J. Cardiothorac. Surg. 2016, 49, 960–965. [Google Scholar] [CrossRef]
- Muneretto, C.; Bisleri, G.; Moggi, A.; Di Bacco, L.; Tespili, M.; Repossini, A.; Rambaldini, M. Interact Cardiovasc Thorac Surg. Treating the patients in the ‘grey-zone’ with aortic valve disease: A comparison among conventional surgery, sutureless valves and transcatheter aortic valve replacement. Interact. Cardiovasc. Thorac. Surg. 2014, 20, 90–95. [Google Scholar] [CrossRef]
- Repossini, A.; Fischlein, T.; Solinas, M.; Di Bacco, L.; Passaretti, B.; Grubitzsch, H.; Folliguet, T.; Santarpino, G.; Laborde, F.; Muneretto, C. Stentless sutureless and transcatheter valves: A comparison of the hemodynamic performance of different prostheses concept. Minerva Cardioangiol. 2018, 66, 180–190. [Google Scholar] [CrossRef]
- Gerfer, S.; Mauri, V.; Kuhn, E.; Adam, M.; Djordevic, I.; Ivanov, B.; Gaisendrees, C.; Frerker, C.; Schmidt, T.; Mader, N.; et al. Comparison of Self-Expanding RDV Perceval S versus TAVI ACURATE neo/TF. Thorac. Cardiovasc. Surg. 2021, 69, 420–427. [Google Scholar] [CrossRef]
- Zubarevich, A.; Szczechowicz, M.; Amanov, L.; Arjomandi Rad, A.; Osswald, A.; Torabi, S.; Ruhparwar, A.; Weymann, A. Non-Inferiority of Sutureless Aortic Valve Replacement in the TAVR Era: David versus Goliath. Life 2022, 12, 979. [Google Scholar] [CrossRef] [PubMed]
- Vilalta, V.; Alperi, A.; Cediel, G.; Mohammadi, S.; Fernández-Nofrerias, E.; Kalvrouziotis, D.; Delarochellière, R.; Paradis, J.M.; González-Lopera, M.; Fadeuilhe, E.; et al. Midterm Outcomes Following Sutureless and Transcatheter Aortic Valve Replacement in Low-Risk Patients With Aortic Stenosis. Circ. Cardiovasc. Interv. 2021, 14, e011120. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.H.; Lee, S.H.; Ko, Y.G.; Lee, S.; Shim, C.Y.; Ahn, C.M.; Hong, G.R.; Shim, J.K.; Kwak, Y.L.; Hong, M.K. Transcatheter Aortic Valve Replacement versus Sutureless Aortic Valve Replacement: A Single Center Retrospective Cohort Study. Yonsei Med. J. 2021, 62, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Santarpino, G.; Lorusso, R.; Moscarelli, M.; Mikus, E.; Wisniewski, K.; Dell’Aquila, A.M.; Margari, V.; Carrozzo, A.; Barbato, L.; Fiorani, V.; et al. Sutureless versus transcatheter aortic valve replacement: A multicenter analysis of “real-world” data. J. Cardiol. 2022, 79, 121–126. [Google Scholar] [CrossRef]
- Muneretto, C.; Alfieri, O.; Cesana, B.M.; De Bonis, M.; Di Bartolomeo, R.; Savini, C.; Folesani, G.; Di Bacco, L.; Rambaldini, M.; Maureira, J.P.; et al. A comparison of conventional surgery, transcatheter aortic valve replacement, and sutureless valves in “real-world” patients with aortic stenosis and intermediate- to high-risk profile. J. Thorac. Cardiovasc. Surg. 2015, 150, 1570–1577; discussion 1577–1579. [Google Scholar] [CrossRef]
- Gilmanov, D.; Miceli, A.; Ferrarini, M.; Farneti, P.; Murzi, M.; Solinas, M.; Glauber, M. Aortic valve replacement through right anterior minithoracotomy: Can sutureless technology improve clinical outcomes? Ann. Thorac. Surg. 2014, 98, 1585–1592. [Google Scholar] [CrossRef]
- Pollari, F.; Santarpino, G.; Dell’Aquila, A.M.; Gazdag, L.; Alnahas, H.; Vogt, F.; Pfeiffer, S.; Fischlein, T. Better short-term outcome by using sutureless valves: A propensity-matched score analysis. Ann. Thorac. Surg. 2014, 98, 611–616; discussion 616–617. [Google Scholar] [CrossRef]
- D’Onofrio, A.; Messina, A.; Lorusso, R.; Alfieri, O.; Fusari, M.; Rubino, P.; Rinaldi, M.; Di Bartolomeo, R.; Glauber, M.; Troise, G.; et al. Sutureless aortic valve replacement as an alternative treatment for patients belonging to the “gray zone” between transcatheter aortic valve implantation and conventional surgery: A propensity-matched, multicenter analysis. J. Thorac. Cardiovasc. Surg. 2012, 144, 1010–1018. [Google Scholar] [CrossRef]
- Fischlein, T.; Folliguet, T.; Meuris, B.; Shrestha, M.L.; Roselli, E.E.; McGlothlin, A.; Kappert, U.; Pfeiffer, S.; Corbi, P.; Lorusso, R.; et al. Sutureless versus conventional bioprostheses for aortic valve replacement in severe symptomatic aortic valve stenosis. J. Thorac. Cardiovasc. Surg. 2021, 161, 920–932. [Google Scholar] [CrossRef]
- Dalen, M.; Biancari, F.; Rubino, A.S.; Santarpino, G.; Glaser, N.; Praetere, H.D.; Kasama, K.; Juvonen, T.; Deste, W.; Pollari, F.; et al. Aortic valve replacement through full sternotomy with a stented bioprosthesis versus minimally invasive sternotomy with a sutureless bioprosthesis. Eur. J. Cardithorac. Surg. 2016, 49, 220–227. [Google Scholar] [CrossRef]
- Forcillo, J.; Bouchard, D.; Nguyen, A.; Perrault, L.; Cartier, R.; Pellerin, M.; Demers, P.; Stevens, L.M.; Carrier, M. Perioperative outcomes with sutureless versus stented biological aortic valves in elderly persons. J. Thorac. Cardiovasc. Surg. 2016, 151, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Dokollari, A.; Margaryan, R.; Torregrossa, G.; Sicouri, S.; Cameli, M.; Mandoli, G.E.; Prifti, E.; Veshti, A.; Bonacchi, M.; Gelsomino, S. Risk predictors that impact long-term prognosis in patients undergoing aortic valve replacement with the Perceval sutureless bioprosthesis. Cardiovasc. Revasc. Med. 2023, 11, S1553-8389(23)00129-X. [Google Scholar] [CrossRef]
- Durdu, M.S.; Gumus, F.; Ozcinar, E.; Cakici, M.; Bermede, O.; Dincer, I.; Kılıckap, M.; Sirlak, M.; Ucanok, K.; Akar, A.R. Sutureless Valve Replacement Through a Right Anterior Mini-thoracotomy in Elderly Patients With Stenotic Bicuspid Aortic Valve. Semin. Thorac. Cardiovasc. Surg. 2019, 31, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.; Fortin, W.; Mazine, A.; Bouchard, D.; Carrier, M.; El-Hamamsy, I.; Lamarche, Y.; Demers, P. Sutureless aortic valve replacement in patients who have bicuspid aortic valve. J. Thorac. Cardiovasc. Surg. 2015, 150, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Szecel, D.; Eurlings, R.; Rega, F.; Verbrugghe, P.; Meuris, B. Perceval sutureless aortic valve implantation: Mid-term outcomes. Ann. Thorac. Surg. 2020, 111, 1331–1337. [Google Scholar] [CrossRef]
- Miceli, A.; Berretta, P.; Fiore, A.; Andreas, M.; Solinas, M.; Santarpino, G.; Kappert, U.; Misfeld, M.; Savini, C.; Albertini, A.; et al. Sutureless and rapid deployment implantation in bicuspid aortic valve: Results from the sutureless and rapid-deployment aortic valve replacement international registry. Ann. Cardiothorac. Surg. 2020, 9, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Suri, R.M.; Javadikasgari, H.; Heimansohn, D.A.; Weissman, N.J.; Ailawadi, G.; Ad, N.; Aldea, G.S.; Thourani, V.H.; Szeto, W.Y.; Michler, R.E.; et al. Prospective USinvestigational device exemption trial of a sutureless aorticbioprosthesis: One-year outcomes. J. Thorac. Cardiovasc. Surg. 2019, 157, 1773–1782. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, M.; Fischlein, T.; Meuris, B.; Flameng, W.; Carrel, T.; Madonna, F.; Misfeld, M.; Folliguet, T.; Haverich, A.; Laborde, F. European multicentre experience with the sutureless Perceval valve: Clinical and haemodynamic outcomes up to 5 years in over 700 patients. Eur. J. Cardiothorac. Surg. 2016, 49, 234–241. [Google Scholar] [CrossRef]
- Meuris, B.; Flameng, W.J.; Laborde, F.; Folliguet, T.A.; Haverich, A.; Shrestha, M. Five-year results of the pilot trial of a sutureless valve. J. Thorac. Cardiovasc. Surg. 2015, 150, 84–88. [Google Scholar] [CrossRef]
- Pollari, F.; Mamdooh, H.; Hitzl, W.; Grossmann, I.; Vogt, F.; Fischlein, T. Ten years’ experience with the sutureless aortic valve replacement: Incidence and predictors for survival and valve durability at follow-up. Eur. J. Cardiothorac. Surg. 2023, 63, ezac572. [Google Scholar] [CrossRef]
- Rubino, A.S.; Mignosa, C. Sutureless valves and the quality of perfusion: Towards a goal directed aortic valve replacement. Minerva. Cardioangiol. 2018, 66, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Mazine, A.; Teoh, K.; Bouhout, I.; Bhatnagar, G.; Pelletier, M.; Voisine, P.; Demers, P.; Carrier, M.; Bouchard, D. Sutureless aortic valve replacement: A Canadian multicentre study. Can. J. Cardiol. 2015, 31, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, M.; Folliguet, T.; Meuris, B.; Dibie, A.; Bara, C.; Herregods, M.C.; Khaladj, N.; Hagl, C.; Flameng, W.; Laborde, F.; et al. Sutureless Perceval S aortic valve replacement: A multicenter, prospective pilot trial. J. Heart Valve Dis. 2009, 18, 698–702. [Google Scholar]
- Shrestha, M.; Maeding, I.; Höffler, K.; Koigeldiyev, N.; Marsch, G.; Siemeni, T.; Fleissner, F.; Haverich, A. Aortic valve replacement in geriatric patients with small aortic roots: Are sutureless valves the future? Interact. Cardiovasc. Thorac. Surg. 2013, 17, 778–782; discussion 782. [Google Scholar] [CrossRef] [PubMed]
- Villa, E.; Dalla Tomba, M.; Messina, A.; Trenta, A.; Brunelli, F.; Cirillo, M.; Mhagna, Z.; Chiariello, G.A.; Troise, G. Sutureless aortic valve replacement in high risk patients neutralizes expected worse hospital outcome: A clinical and economic analysis. Cardiol. J. 2019, 26, 56–65. [Google Scholar] [CrossRef]
- Sá, M.P.; Sun, T.; Fatehi Hassanabad, A.; Awad, A.K.; Van den Eynde, J.; Malin, J.H.; Sicouri, S.; Torregrossa, G.; Ruhparwar, A.; Weymann, A.; et al. Complete transcatheter versus complete surgical treatment in patients with aortic valve stenosis and concomitant coronary artery disease: Study-level meta-analysis with reconstructed time-to-event data. J. Card. Surg. 2022, 37, 2072–2083. [Google Scholar] [CrossRef]
- Povero, M.; Miceli, A.; Pradelli, L.; Ferrarini, M.; Pinciroli, M.; Glauber, M. Cost-utility of surgical sutureless bioprostheses vs TAVI in aortic valve replacement for patients at intermediate and high surgical risk. Clin. Outcomes Res. 2018, 10, 733–745. [Google Scholar] [CrossRef] [PubMed]
- Sá, M.P.; Jacquemyn, X.; Van den Eynde, J.; Tasoudis, P.; Dokollari, A.; Torregrossa, G.; Sicouri, S.; Clavel, M.A.; Pibarot, P.; Ramlawi, B. Impact of Prosthesis-Patient Mismatch After Transcatheter Aortic Valve Replacement: Meta-Analysis of Kaplan-Meier-Derived Individual Patient Data. JACC Cardiovasc. Imaging 2023, 16, 298–310. [Google Scholar] [CrossRef]
- Deeb, G.M.; Reardon, M.J.; Ramlawi, B.; Yakubov, S.J.; Chetcuti, S.J.; Kleiman, N.S.; Mangi, A.A.; Zahr, F.; Song, H.K.; Gada, H.; et al. Propensity-Matched 1-Year Outcomes Following Transcatheter Aortic Valve Replacement in Low-Risk Bicuspid and Tricuspid Patients. JACC Cardiovasc. Interv. 2022, 15, 511–522. [Google Scholar] [CrossRef]
- Bedeir, K.; Reardon, M.; Cohn, L.H.; Ramlawi, B. Sutureless Aortic Valves: Combining the Best or the Worst? Semin. Thorac. Cardiovasc. Surg. 2016, 28, 341–352. [Google Scholar] [CrossRef]
- Dokollari, A.; Sá, M.P.; Sicouri, S.; Ramlawi, B.; Torregrossa, G.; Bonacchi, M. Commentary: Osteogenic Metaplasia of the Aortic Valve. Do Bacteria, Diabetes, and Dyslipidemia Play a Role? Semin. Thorac. Cardiovasc. Surg. 2022, 34, 1178–1179. [Google Scholar] [CrossRef] [PubMed]
- Bonacchi, M.; Dokollari, A.; Parise, O.; Sani, G.; Prifti, E.; Bisleri, G.; Gelsomino, S. Ministernotomy compared with right anterior minithoracotomy for aortic valve surgery. J. Thorac. Cardiovasc. Surg. 2021, 23, S0022–S5223. [Google Scholar] [CrossRef] [PubMed]
- Prifti, E.; Bonacchi, M.; Minardi, G.; Krakulli, K.; Baboci, A.; Esposito, G.; Demiraj, A.; Zeka, M.; Rruci, E. Early and Mid-term Outcome of the St. Jude Medical Regent 19-mm Aortic Valve Mechanical Prosthesis. Functional and Haemodynamic Evaluation. Heart Lung Circ. 2018, 27, 235–247. [Google Scholar] [CrossRef]
- Bach, D.S.; Kon, N.D. Long-term clinical outcomes 15 years after aortic valve replacement with the Freestyle stentless aortic bioprosthesis. Ann. Thorac. Surg. 2014, 97, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Kim, J.H.; Joo, H.C.; Lee, S.; Youn, Y.N.; Lee, S.H. Prognostic Markers and Long-Term Outcomes After Aortic Valve Replacement in Patients with Chronic Aortic Regurgitation. J. Am. Heart Assoc. 2020, 9, e018292. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Author | Muneretto et al. [24] | Gilmanov et al. [25] | Pollari et al. [26] | D’Onofrio et al. [27] | Vaquero et al. [28] | Fischlein et al. [29] | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type of Clinical Study | Prospective | Retrospective | Prospective | Retrospective | Prospective | Prospective | ||||||
| Valves and patients | Perceval N = 53 | Stented N = 55 | Perceval N = 133 | Stented N = 133 | Perceval N = 88 | Stented N = 88 | Perceval N = 31 | Stented N = 112 | Perceval N = 140 | Stented N = 409 | Perceval N = 447 | Stented N = 449 |
| 30-day Mortality (%) | 0 | 0 | 0.8 | 1.5 | 2.4 | 3.7 | 0 | 1.8 | 6.4 | 5.9 | 1 | 1 |
| Bleeding requiring surgery (%) | 7.5 | 10.5 | 6.8 | 3.8 | 2.4 | 6.1 | NR | NR | NR | NR | 4.4 | 6.3 |
| Paravalvular leak (%) | 1.9 | 0 | NR | NR | NR | NR | 19.4 | 1 | 3.6 | 0.5 | 1 | 0 |
| Stroke (%) | 0 | 1.8 | NR | NR | 3.7 | 7.3 | 0 | 0 | 2.9 | 2.7 | 1.5 | 1.9 |
| Myocardial infarction (%) | 0 | 0 | 1.5 | 0 | NR | NR | 0 | 0.9 | 7.8 | 4.3 | 1 | 1.5 |
| Permanent pacemaker implantation (%) | 2 | 1.8 | NR | NR | 6.1 | 8.5 | 3.2 | 0.9 | 10.7 | 2 | 10.6 | 3.2 |
| Aortic cross-clamp time in minutes/SD | 30.8 ± 13.6 | 65.3 ± 27.7 | 56 | 90 | 47 ± 16 | 59 ± 23 | NR | NR | 65.3 ± 29.1 | 77.2 ± 30.3 | 48.5 ± 24.7 | 65.2 ± 23.6 |
| Cardiopulmonary bypass time in minutes/SD | 47 ± 18.5 | 89.4 ± 20.4 | 88 | 120 | 71 ± 11 | 92 ± 33 | NR | NR | 81.3 ± 34.9 | 95.7 ± 37.9 | 71.0 ± 34.1 | 87.8 ± 33.9 |
| Type of stented valves | NA | Perimount, Edwards | NA | CE Edwards, Medtronic, CE standard | NA | NR | NA | NR | NA | Triflecta | NA | NR |
| Study author | Dalen et al. [30] | Forcillo et al. [31] | Dokollari et al. [32] | |||||||||
| Type of Clinical Study | Retrospective | Retrospective | Retrospective | |||||||||
| Valves and patients | Perceval = 171 | Stented = 171 | Perceval = 76 | Stented = 319 | Perceval = 25 | Stented = 57 | ||||||
| 30-day Mortality (%) | 1.8 | 2.3 | 5 | 6 | 4 | 7 | ||||||
| Bleeding requiring surgery (%) | 4.1 | 6.4 | 8 | 8 | 16 | 15.8 | ||||||
| Paravalvular leak (%) | 0 | 1.2 | 0 | 0 | NA | NA | ||||||
| Stroke (%) | 2.3 | 1.2 | 0 | 5 | 7 | 4 | ||||||
| Myocardial infarction (%) | NR | NR | 0 | 0 | 10.5 | 4 | ||||||
| Permanent pacemaker implantation (%) | 9.9 | 2.9 | 17 | 8 | 8.8 | 4 | ||||||
| Aortic cross-clamp time in minutes/SD | 40 ± 15 | 65 ± 15 | 46 | 68 | NR | NR | ||||||
| Cardiopulmonary bypass time in minutes/SD | 69 ± 20 | 87 ± 20 | 60 | 85 | NR | NR | ||||||
| Type of stented valves | NA | CE Perimount | NA | CE, Medtronic, Mitroflow, St. Jude epic, St. Jude Biocor | NR | NR | ||||||
| Study Author | Durdu et al. [33] (Mean ± SD) | Nguyen et al. [34] (Mean ± SD) | Szecel et al. [35] (Mean ± SD) | Miceli et al. [36] (Mean ± SD) | Suri et al. [37] (Mean ± SD) | Dokollari et al. [32] |
|---|---|---|---|---|---|---|
| Number of patients | N = 13 patients | N = 25 patients | N = 11 patients | N = 88 patients | N = 20 patients | N = 25 patients |
| Type of clinical study | Retrospective | Retrospective | Retrospective | Retrospective | Retrospective | Retrospective |
| 30-day Mortality (%) | 0 | 4 | 0 | 1.6 | 2 | 0 |
| Bleeding requiring surgery (%) | 7.6 | 1 | NR | 3.1 | 4 | 1 |
| Paravalvular leak (%) | 0 | 0 | 0 | 2.3 | NR | NR |
| Stroke (%) | 7.6 | 8 | 0 | 4.2 | NR | 1 |
| Myocardial infarction (%) | 0 | 0 | 0 | NR | NR | 0 |
| Permanent pacemaker implantation (%) | 7.6 | 20 | 0 | 5.7 | NR | 2 |
| Aortic cross-clamping time in minutes/SD | 40.3 ± 3.1 | 45.9 ± 14.0 | 39 ± 13 | 55 | 52.3 ± 19.6 | NR |
| Cardiopulmonary bypass time in minutes/SD | 54.5 ± 4.4 | 56.1 ± 14.9 | 66 ± 22 | 80 | 70.2 ± 27.8 | NR |
| Late Events > 30 Days | Shrestha et al. [38] | Meuris et al. [39] | Pollari et al. [40] | Dokollari [32] |
|---|---|---|---|---|
| Studies | N = 729 Patients | N = 30 Patients | N = 547 Patients | N = 101 |
| Type of study | Retrospective | Prospective clinical trial | Retrospective | Retrospective |
| Follow-up duration | 5 years | 5 years | 8 years | 7 years |
| Deaths (%) | 7 | 28.7 | 22.5 | 12.1 |
| Cardiac Deaths (%) | 1.4 | 3.3 | NR | 5 |
| Valve Explants (%) | 1.5 | 0 | NR | NR |
| Major Paravalvular leak (%) | 1 | 0 | NR | 1 |
| Endocarditis (%) | 1.6 | 6.6 | NR | 0 |
| Structural valve deterioration (%) | 0 | 0 | 4.2 | NR |
| Valve thrombosis (%) | 0 | 0 | NR | NR |
| AV block III (%) | 1.4 | 3.3 | NR | 3 |
| Stroke | 0.8 | 0 |
| Endpoints | Santarpino et al. [1] N = 658 (Mean ± SD) | Rubino et al. [41] N = 314 (Mean ± SD) | Mazine et al. [42] N = 215 (Mean ± SD) | Folliguet et al. [39] N = 208 (Mean ± SD) | Shrestha et al. [43] N = 30 (Mean ± SD) | Shrestha et al. [44] N = 243 (Mean ± SD) | Miceli et al. [36] N = 37 (Mean ± SD) | Repossini et al. [19] N = 158 (Mean ± SD) |
|---|---|---|---|---|---|---|---|---|
| Type of clinical study | Prospective | Retrospective | Retrospective | Retrospective | Prospective | Retrospective | Retrospective | Retrospective |
| EOA (cm2) at discharge | 1.5 ± 0.4 | NR | 1.56 ± 0.37 | 1.4 ± 0.4 | NR | 1.5 ± 0.4 | NR | NR |
| EOA (cm2) at 6 months | 1.5 ± 0.3 | NR | NR | 1.5 ± 0.4 | NR | 1.5 ± 0.4 | NR | NR |
| EOA (cm2) at 1 year | 1.5 ± 0.4 | NR | NR | 1.5 ± 0.3 | 1.55 ± 0.35 | 1.6 ± 0.4 | NR | NR |
| EOA (cm2) at 2 years | NR | NR | NR | NR | 1.51 ± 0.26 | 1.7 ± 0.5 | NR | NR |
| Mean gradient (mmHg) at discharge | 10.3 ± 4.5 | 14 ± 6 | 13.3 ± 6.4 | 10.4 ± 4.3 | NR | 10.1 ± 4.7 | 11.4 ± 3.7 | 10.9 ± 5.4 |
| Mean gradient (mmHg) at 6 months | 8.9 ± 4.1 | NR | NR | 8.9 ± 3.2 | NR | 8.9 ± 4.2 | NR | NR |
| Mean gradient (mmHg) at 1 year | 9.2 ± 5 | NR | NR | 8.7 ± 3.7 | 9.9 ± 4.6 | 8.9 ± 4.6 | NR | NR |
| Mean gradient (mmHg) at 2 years | NR | NR | NR | NR | 8 ± 4.1 | 9 ± 3.4 | NR | NR |
| Peak gradient (mmHg) at discharge | 19.4 ± 8.1 | 27 ± 11 | 24.5 ± 10.8 | 21.3 ± 8.6 | NR | 20.3 ± 9.9 | 19.2 ± 6.9 | 18.7 ± 9.1 |
| Peak gradient (mmHg) at 6 months | 16.8 ± 7 | NR | NR | 19.6 ± 6.7 | NR | 18 ± 7.6 | NR | NR |
| Peak gradient (mmHg) at 1 year | 17.1 ± 8.7 | NR | NR | 18.8 ± 7.6 | 20.9 ± 9.2 | 17.5 ± 8.2 | NR | NR |
| Peak gradient (mmHg) at 2 years | NR | NR | NR | NR | 16.6 ± 7.2 | 18.3 ± 5.6 | NR | NR |
| Endpoints | Chung et al. [23] | Suri et al. [37] | Durdu et al. [33] | Miceli et al. [17] | Nguyen et al. [34] | |||
| Type of clinical study | Retrospective | Retrospective | Retrospective | Retrospective | Retrospective | |||
| EOA (cm2) at discharge | 1.6 ± 0.4 | 1.4 ± 0.3 | 1.81 ± 0.38 | NR | 1.86 ± 0.6 | |||
| EOA (cm2) at 6 months | NR | NR | NR | NR | NR | |||
| EOA (cm2) at 1 year | 1.5 ± 0.3 | NR | NR | NR | NR | |||
| EOA (cm2) at 2 years | NR | NR | NR | NR | NR | |||
| Mean gradient (mmHg) at discharge | 14.7 ± 3.8 | 10.3 ± 3.7 | 13.6 ± 4.4 | 14.8 ± 5.8 | 12.7 ± 6.4 | |||
| Mean gradient (mmHg) at 6 months | NR | NR | NR | NR | NR | |||
| Mean gradient (mmHg) at 1 year | 12.4 ± 5.3 | NR | NR | NR | NR | |||
| Mean gradient (mmHg) at 2 years | NR | NR | NR | NR | NR | |||
| Peak gradient (mmHg) at discharge | 27.5 ± 7.0 | NR | NR | 28.3 ± 10.9 | NR | |||
| Peak gradient (mmHg) at 6 months | NR | NR | NR | NR | NR | |||
| Peak gradient (mmHg) at 1 year | 23.8 ± 8.8 | NR | NR | NR | NR | |||
| Peak gradient (mmHg) at 2 years | NR | NR | NR | NR | NR | |||
| Study | Shrestha et al. [45] N = 729 Patients (Mean ± SD) | Meuris et al. [39] N = 30 Patients (Mean ± SD) |
|---|---|---|
| LVEF at 3 years (%) | 67 ± 9 | NR |
| LVEF at 4 years (%) | 66.1 ± 9.1 | NR |
| LVEF at 5 years (%) | 65.8 ± 7.7 | NR |
| Mean transvalvular gradient at 3 years mmHg | 7.7 ± 2.8 | 8.3 ± 2.5 |
| Mean transvalvular gradient at 4 years mmHg | 7.8 ± 3.8 | 7.6 ± 3.6 |
| Mean transvalvular gradient at 5 years mmHg | 8.8 ± 4.6 | 9.3 ± 5.5 |
| Peak transvalvular gradient at 3 years mmHg | 16 ± 5.2 | 16.6 ± 6.2 |
| Peak transvalvular gradient at 4 years mmHg | 17.8 ± 8.1 | 17.5 ± 7.8 |
| Peak transvalvular gradients at 5 years mmHg | 21.1 ± 9.7 | 21.4 ± 11.5 |
| EOA at 3 years (cm2) | 1.64 ± 0.42 | 1.68 ± 0.4 |
| EOA at 4 years (cm2) | 1.68 ± 0.43 | 1.68 ± 0.43 |
| EOA at 5 years (cm2) | 1.8 ± 0.3 | 1.69 ± 0.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dokollari, A.; Torregrossa, G.; Bisleri, G.; Hassanabad, A.F.; Sa, M.P.; Sicouri, S.; Veshti, A.; Prifti, E.; Bacchi, B.; Cabrucci, F.; et al. Early and Long-Term Clinical and Echocardiographic Outcomes of Sutureless vs. Sutured Bioprosthesis for Aortic Valve Replacement. J. Cardiovasc. Dev. Dis. 2023, 10, 224. https://doi.org/10.3390/jcdd10050224
Dokollari A, Torregrossa G, Bisleri G, Hassanabad AF, Sa MP, Sicouri S, Veshti A, Prifti E, Bacchi B, Cabrucci F, et al. Early and Long-Term Clinical and Echocardiographic Outcomes of Sutureless vs. Sutured Bioprosthesis for Aortic Valve Replacement. Journal of Cardiovascular Development and Disease. 2023; 10(5):224. https://doi.org/10.3390/jcdd10050224
Chicago/Turabian StyleDokollari, Aleksander, Gianluca Torregrossa, Gianluigi Bisleri, Ali Fatehi Hassanabad, Michel Pompeu Sa, Serge Sicouri, Altin Veshti, Edvin Prifti, Beatrice Bacchi, Francesco Cabrucci, and et al. 2023. "Early and Long-Term Clinical and Echocardiographic Outcomes of Sutureless vs. Sutured Bioprosthesis for Aortic Valve Replacement" Journal of Cardiovascular Development and Disease 10, no. 5: 224. https://doi.org/10.3390/jcdd10050224
APA StyleDokollari, A., Torregrossa, G., Bisleri, G., Hassanabad, A. F., Sa, M. P., Sicouri, S., Veshti, A., Prifti, E., Bacchi, B., Cabrucci, F., Ramlawi, B., & Bonacchi, M. (2023). Early and Long-Term Clinical and Echocardiographic Outcomes of Sutureless vs. Sutured Bioprosthesis for Aortic Valve Replacement. Journal of Cardiovascular Development and Disease, 10(5), 224. https://doi.org/10.3390/jcdd10050224