
The Impact of Polymorphisms in ATP-Binding Cassette Transporter Genes on Anthracycline-Induced Early Cardiotoxicity in Patients with Breast Cancer

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
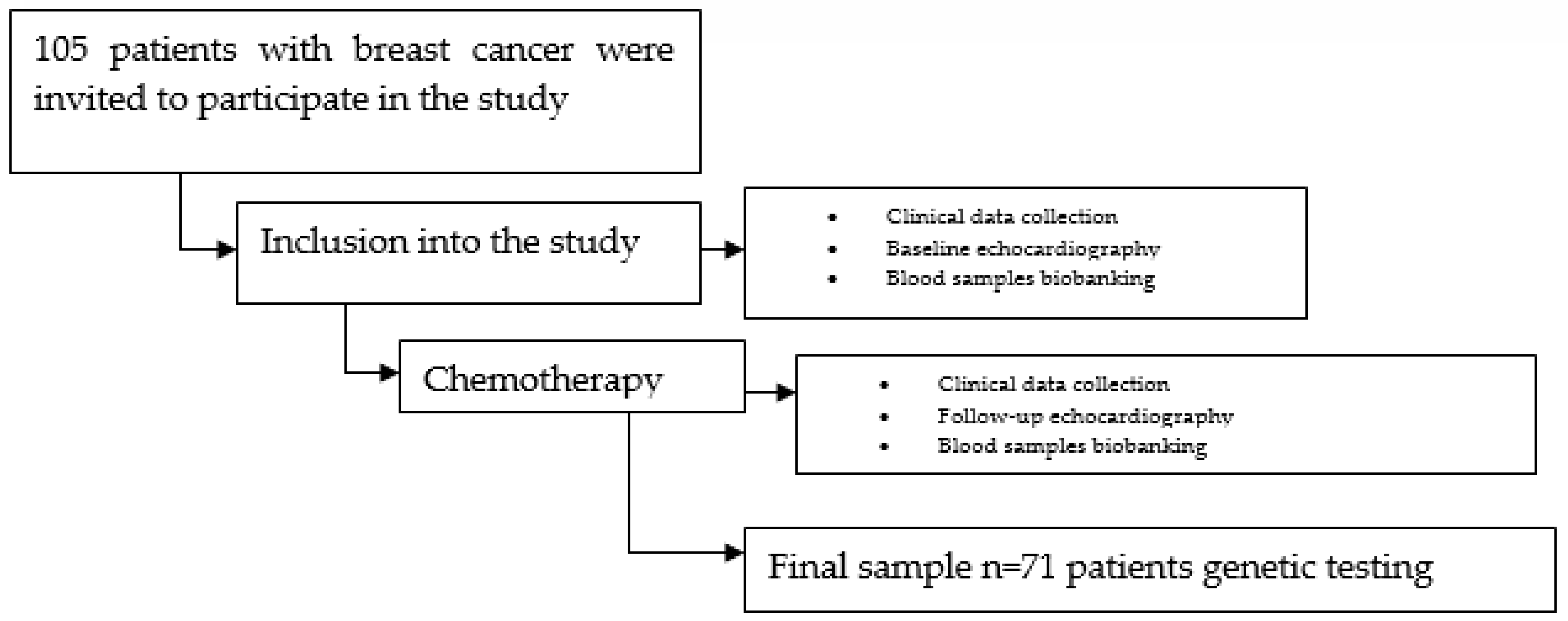
2.1. Study Population
- AC (doxorubicin 60 mg/m2 + cyclophosphamide 600 mg/m2 every 3 weeks for four cycles);
- AC-P (doxorubicin 60 mg/m2 + cyclophosphamide 600 mg/m2 every 3 weeks for four cycles, followed by paclitaxel 80 mg/m2 weekly for 12 times or paclitaxel 175 mg/m2 every 21 days for four cycles);
- AC + D (doxorubicin 60 mg/m2 + cyclophosphamide 600 mg/m2 every 3 weeks for four cycles, followed by docetaxel 100 mg/m2 every 3 weeks for four cycles);
- FAC + D (5-FU 500 mg/m2 on days 1 and 8 + doxorubicin 50 mg/m2 on day 1 + cyclophosphamide 500 mg/m2 on day 1 every 3 weeks for three cycles, followed by docetaxel 100 mg/m2 every 3 weeks for three cycles);
- TAC (docetaxel 75 mg/m2 + doxorubicin 50 mg/m2 + cyclophosphamide 500 mg/m2 IV every 3 weeks for six cycles);
- FAC (5-FU 500 mg/m2 on days 1 and 8 + doxorubicin 50 mg/m2 on day 1 + cyclophosphamide 500 mg/m2 on day 1 every 3 weeks for six cycles).
2.2. Echocardiography
2.3. Genotyping Methods
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef]
- Siegel, R.; DeSantis, C.; Virgo, K.; Stein, K.; Mariotto, A.; Smith, T.; Cooper, D.; Gansler, T.; Lerro, C.; Fedewa, S.; et al. Cancer treatment and survivorship statistics. CA Cancer J. Clin. 2012, 62, 220–241. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Herman, E.H.; Lipshultz, S.E.; Minotti, G.; Sarvazyan, N.; Sawyer, D.B. Anthracycline Cardiotoxicity: From Bench to Bedside. J. Clin. Oncol. 2008, 26, 3777–3784. [Google Scholar] [CrossRef] [PubMed]
- Bober, P.; Alexovič, M.; Tomková, Z.; Kilík, R.; Sabo, J. RHOA and mDia1 promotes apoptosis of breast cancer cells via a high dose of doxorubicin treatment. Open Life Sci. 2019, 14, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Pilco-Ferreto, N.; Calaf, G.M. Influence of doxorubicin on apoptosis and oxidative stress in breast cancer cell lines. Int. J. Oncol. 2016, 49, 753–762. [Google Scholar] [CrossRef]
- Lovitt, C.J.; Shelper, T.B.; Avery, V.M. Doxorubicin resistance in breast cancer cells is mediated by extracellular matrix proteins. BMC Cancer 2018, 18, 41. [Google Scholar] [CrossRef]
- Jamialahmadi, K.; Zahedipour, F.; Karimi, G. The role of microRNAs on doxorubicin drug resistance in breast cancer. J. Pharm. Pharmacol. 2021, 73, 997–1006. [Google Scholar] [CrossRef]
- Shafei, A.; El-Bakly, W.; Sobhy, A.; Wagdy, O.; Reda, A.; Aboelenin, O.; Marzouk, A.; El Habak, K.; Mostafa, R.; Ali, M.A.; et al. A review on the efficacy and toxicity of different doxorubicin nanoparticles for targeted therapy in metastatic breast cancer. Biomed. Pharmacother. 2017, 95, 1209–1218. [Google Scholar] [CrossRef]
- Hadla, M.; Palazzolo, S.; Corona, G.; Caligiuri, I.; Canzonieri, V.; Toffoli, G.; Rizzolio, F. Exosomes increase the therapeutic index of doxorubicin in breast and ovarian cancer mouse models. Nanomedicine 2016, 11, 2431–2441. [Google Scholar] [CrossRef]
- Armenian, S.H.; Lacchetti, C.; Barac, A.; Carver, J.; Constine, L.S.; Denduluri, N.; Dent, S.; Douglas, P.S.; Durand, J.-B.; Ewer, M.; et al. Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2017, 35, 893–911. [Google Scholar] [CrossRef]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert Consensus for Multimodality Imaging Evaluation of Adult Patients during and after Cancer Therapy: A Report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2014, 27, 911–939. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801, Corrigendum in: Eur. Heart J. 2018, 39, 839. [Google Scholar] [CrossRef] [PubMed]
- Kremer, L.C.M.; van der Pal, H.J.H.; Offringa, M.; van Dalen, E.C.; Voûte, P.A. Frequency and risk factors of subclinical cardiotoxicity after anthracycline therapy in children: A systematic review. Ann. Oncol. 2002, 13, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D.; Layard, M.W.; Basa, P.; Davis, H.L., Jr.; Von Hoff, A.L.; Rozencweig, M.; Muggia, F.M. Risk Factors for Doxorubicin-lnduced Congestive Heart Failure. Ann. Intern. Med. 1979, 91, 710–717. [Google Scholar] [CrossRef]
- Lipshultz, S.E.; Lipsitz, S.R.; Mone, S.M.; Goorin, A.M.; Sallan, S.E.; Sanders, S.P.; Orav, E.J.; Gelber, R.D.; Colan, S.D. Female Sex and Higher Drug Dose as Risk Factors for Late Cardiotoxic Effects of Doxorubicin Therapy for Childhood Cancer. N. Engl. J. Med. 1995, 332, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Shao, T. Anthracycline cardiotoxicity after breast cancer treatment. Oncology 2009, 23, 227. [Google Scholar] [PubMed]
- Menna, P.; Paz, O.G.; Chello, M.; Covino, E.; Salvatorelli, E.; Minotti, G. Anthracycline cardiotoxicity. Expert Opin. Drug Saf. 2011, 11, S21–S36. [Google Scholar] [CrossRef]
- Aminkeng, F.; Ross, C.J.D.; Rassekh, S.R.; Hwang, S.; Rieder, M.J.; Bhavsar, A.P.; Smith, A.; Sanatani, S.; Gelmon, K.A.; Bernstein, D.; et al. Recommendations for genetic testing to reduce the incidence of anthracycline-induced cardiotoxicity. Br. J. Clin. Pharmacol. 2016, 82, 683–695. [Google Scholar] [CrossRef]
- Jones, P.M.; George, A.M. The ABC transporter structure and mechanism: Perspectives on recent research. Cell. Mol. Life Sci. 2004, 61, 682–699. [Google Scholar] [CrossRef]
- Cascorbi, I. Role of pharmacogenetics of ATP-binding cassette transporters in the pharmacokinetics of drugs. Pharmacol. Ther. 2006, 112, 457–473. [Google Scholar] [CrossRef]
- Wang, Y.-J.; Zhang, Y.-K.; Kathawala, R.J.; Chen, Z.-S. Repositioning of Tyrosine Kinase Inhibitors as Antagonists of ATP-Binding Cassette Transporters in Anticancer Drug Resistance. Cancers 2014, 6, 1925–1952. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.; Fu, L.; Huang, J.; Dai, Y.; Wang, B.; Xu, G.; Wu, L.; Zhou, H. Curcumin reverses doxorubicin resistance via inhibition the efflux function of ABCB4 in doxorubicin-resistant breast cancer cells. Mol. Med. Rep. 2019, 19, 5162–5168. [Google Scholar] [CrossRef] [PubMed]
- Wen, S.-H.; Su, S.-C.; Liou, B.-H.; Lin, C.-H.; Lee, K.-R. Sulbactam-enhanced cytotoxicity of doxorubicin in breast cancer cells. Cancer Cell Int. 2018, 18, 128. [Google Scholar] [CrossRef] [PubMed]
- Gatta, A.K.; Chandrashekhar, R.; Udupa, N.; Reddy, M.S.; Mutalik, S.; Josyula, V.R. Strategic Design of Dicer Substrate siRNA to Mitigate the Resistance Mediated by ABCC1 in Doxorubicin-resistant Breast Cancer. Indian J. Pharm. Sci. 2020, 82, 329–340. [Google Scholar] [CrossRef]
- Adorni, M.P.; Galetti, M.; La Monica, S.; Incerti, M.; Ruffoni, A.; Elviri, L.; Zanotti, I.; Papotti, B.; Cavallo, D.; Alfieri, R.; et al. A New ABCB1 Inhibitor Enhances the Anticancer Effect of Doxorubicin in both In Vitro and In Vivo Models of NSCLC. Int. J. Mol. Sci. 2023, 24, 989. [Google Scholar] [CrossRef]
- Zalcberg, J.; Hu, X.; Slater, A.; Parisot, J.; El-Osta, S.; Kantharidis, P.; Chou, S.; Parkin, J. MRP1 not MDR1 gene expression is the predominant mechanism of acquired multidrug resistance in two prostate carcinoma cell lines. Prostate Cancer Prostatic Dis. 2000, 3, 66–75. [Google Scholar] [CrossRef]
- Liu, Z.; Duan, Z.-J.; Chang, J.-Y.; Zhang, Z.-F.; Chu, R.; Li, Y.-L.; Dai, K.-H.; Mo, G.-Q.; Chang, Q.-Y. Sinomenine Sensitizes Multidrug-Resistant Colon Cancer Cells (Caco-2) to Doxorubicin by Downregulation of MDR-1 Expression. PLoS ONE 2014, 9, e98560. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Marwick, T.H.; Leano, R.L.; Brown, J.; Sun, J.-P.; Hoffmann, R.; Lysyansky, P.; Becker, M.; Thomas, J.D. Myocardial Strain Measurement with 2-Dimensional Speckle-Tracking Echocardiography: Definition of normal range. JACC Cardiovasc. Imaging 2009, 2, 80–84. [Google Scholar] [CrossRef]
- Octavia, Y.; Tocchetti, C.G.; Gabrielson, K.L.; Janssens, S.; Crijns, H.J.; Moens, A.L. Doxorubicin-induced cardiomyopathy: From molecular mechanisms to therapeutic strategies. J. Mol. Cell. Cardiol. 2012, 52, 1213–1225. [Google Scholar] [CrossRef]
- Albini, A.; Pennesi, G.; Donatelli, F.; Cammarota, R.; De Flora, S.; Noonan, D.M. Cardiotoxicity of Anticancer Drugs: The Need for Cardio-Oncology and Cardio-Oncological Prevention. Gynecol. Oncol. 2010, 102, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Hamo, C.E.; Bloom, M.W. Cancer and Heart Failure: Understanding the Intersection. Card. Fail. Rev. 2017, 3, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Mitry, M.A.; Edwards, J.G. Doxorubicin induced heart failure: Phenotype and molecular mechanisms. IJC Hear. Vasc. 2015, 10, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Kalivendi, S.V.; Kotamraju, S.; Zhao, H.; Joseph, J.; Kalyanaraman, B. Doxorubicin-induced Apoptosis Is Associated with Increased Transcription of Endothelial Nitric-oxide Synthase. J. Biol. Chem. 2001, 276, 47266–47276. [Google Scholar] [CrossRef]
- Simunek, T.; Sterba, M. Anthracycline-induced cardiotoxicity: Overview of studies examining the roles of oxidative stress and free cellular iron. Pharmacol. Rep. 2009, 61, 154–171. [Google Scholar] [CrossRef]
- Floyd, J.D.; Nguyen, D.T. Cardiotoxicity of cancer therapy. J. Clin. Oncol. 2005, 23, 7685–7696. [Google Scholar] [CrossRef]
- Thorn, C.F.; Oshiro, C. Altman Doxorubicin pathways: Pharmacodynamics and adverse effects. Pharmacogenet. Genomics 2011, 21, 440–446. [Google Scholar] [CrossRef]
- Billingham, M.E.; Mason, J.W.; Bristow, M.R.; Daniels, J.R. Anthracycline cardiomyopathy monitored by morphologic changes. Cancer Treat. Rep. 1978, 62, 865–872. [Google Scholar]
- Kim, Y.; Seidman, J.G.; Seidman, C.E. Genetics of cancer therapy-associated cardiotoxicity. J. Mol. Cell. Cardiol. 2022, 167, 85–91. [Google Scholar] [CrossRef]
- Barrett-Lee, P.J.; Dixon, J.M.; Farrell, C.; Jones, A.; Leonard, R.; Murray, N.; Palmieri, C.; Plummer, C.J.; Stanley, A.; Verrill, M.W. Expert opinion on the use of anthracyclines in patients with advanced breast cancer at cardiac risk. Ann. Oncol. 2009, 20, 816–827. [Google Scholar] [CrossRef]
- Feola, M.; Garrone, O.; Occelli, M.; Francini, A.; Biggi, A.; Visconti, G.; Albrile, F.; Bobbio, M.; Merlano, M. Cardiotoxicity after anthracycline chemotherapy in breast carcinoma: Effects on left ventricular ejection fraction, troponin I and brain natriuretic peptide. Int. J. Cardiol. 2011, 148, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Gimeno, E.; Gomez, M. NT-proBNP: A cardiac biomarker to assess prognosis in non-Hodgkin lymphoma. Leuk Res. 2011, 35, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Dean, M.; Rzhetsky, A.; Allikmets, R. The Human ATP-Binding Cassette (ABC) Transporter Superfamily. Genome Res. 2001, 11, 1156–1166. [Google Scholar] [CrossRef] [PubMed]
- Gillet, J.-P.; Efferth, T.; Remacle, J. Chemotherapy-induced resistance by ATP-binding cassette transporter genes. Biochim. Biophys. Acta-Rev. Cancer 2007, 1775, 237–262. [Google Scholar] [CrossRef]
- Dean, M.; Moitra, K.; Allikmets, R. The human ATP-binding cassette (ABC) transporter superfamily. Hum. Mutat. 2022, 43, 1162–1182. [Google Scholar] [CrossRef]
- Wang, J.; Wu, Z.; Yang, Y.; Teng, Q.; Li, Y.; Lei, Z.; Jani, K.A.; Kaushal, N.; Chen, Z. ATP-binding cassette (ABC) transporters in cancer: A review of recent updates. J. Evid.-Based Med. 2021, 14, 232–256. [Google Scholar] [CrossRef]
- Leong, S.L.; Chaiyakunapruk, N.; Lee, S.W.H. Candidate Gene Association Studies of Anthracycline-induced Cardiotoxicity: A Systematic Review and Meta-analysis. Sci. Rep. 2017, 7, 39. [Google Scholar] [CrossRef]
- Hertz, D.L.; Caram, M.V.; Kidwell, K.M.; Thibert, J.N.; Gersch, C.; Seewald, N.J.; Smerage, J.; Rubenfire, M.; Henry, N.L.; A Cooney, K.; et al. Evidence for association of SNPs in ABCB1 and CBR3, but not RAC2, NCF4, SLC28A3 or TOP2B, with chronic cardiotoxicity in a cohort of breast cancer patients treated with anthracyclines. Pharmacogenomics 2016, 17, 231–240. [Google Scholar] [CrossRef]
- Rossi, D.; Rasi, S.; Franceschetti, S.; Capello, D.; Castelli, A.; De Paoli, L.; Ramponi, A.; Chiappella, A.; Pogliani, E.M.; Vitolo, U.; et al. Analysis of the host pharmacogenetic background for prediction of outcome and toxicity in diffuse large B-cell lymphoma treated with R-CHOP21. Leukemia 2009, 23, 1118–1126. [Google Scholar] [CrossRef]
- Visscher, H.; Ross, C.J.; Rassekh, S.R.; Barhdadi, A.; Dubé, M.-P.; Al-Saloos, H.; Sandor, G.S.; Caron, H.N.; van Dalen, E.C.; Kremer, L.C.; et al. Pharmacogenomic Prediction of Anthracycline-Induced Cardiotoxicity in Children. J. Clin. Oncol. 2012, 30, 1422–1428. [Google Scholar] [CrossRef]
- Liu, B.; Guan, X. The Incidence of Adjuvant Chemotherapy-Related Early-Onset Cardiac Events in Breast Cancer Patients and Its Relationship with Genetic Susceptibility: A Prospective Cohort Study. 2020. Available online: https://www.researchsquare.com/article/rs-18261/v1.pdf (accessed on 27 March 2020).
- Semsei, A.F.; Erdelyi, D.J.; Ungvari, I.; Csagoly, E.; Hegyi, M.Z.; Kiszel, P.S.; Lautner-Csorba, O.; Szabolcs, J.; Masat, P.; Fekete, G.; et al. ABCC1 polymorphisms in anthracycline-induced cardiotoxicity in childhood acute lymphoblastic leukaemia. Cell Biol. Int. 2011, 36, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Gándara-Mireles, J.A.; Lares-Asseff, I.; Espinoza, E.A.R.; Blanco, J.G.; Font, A.E.G.; Hurtado, L.P.C.; Castañeda, V.L.; Fierro, I.V.; Romero, L.P.; Reyes, H.A. Association of genetic polymorphisms NCF4 rs1883112, CBR3 rs1056892, and ABCC1 rs3743527 with the cardiotoxic effects of doxorubicin in children with acute lymphoblastic leukemia. Pharmacogenetics Genom. 2021, 31, 108–115. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Patients (n = 71) | Noncardiotoxicity (n = 51, 71.8%) | Cardiotoxicity (n = 20, 28.2%) | p-Value | |
|---|---|---|---|---|
| Age (years) | 53.76 ± 9.23 | 53.94 ± 8.42 | 53.30 ± 11.25 | 0.868 |
| BMI (kg/m2) | 28.44 ± 6.04 | 28.39 ± 6.09 | 28.55 ± 6.08 | 0.928 |
| CVD risk factors | ||||
| AH, n (%) | 31 (43.7) | 16 (31.4) | 15 (75.0) | 0.001 |
| Diabetes mellitus, n (%) | 11 (15.5) | 8 (15.7) | 3 (15.0) | 1.000 |
| Smoking, n (%) | 16 (22.5) | 10 (19.6) | 6 (30.0) | 0.360 |
| Family history of CVD, n (%) | 17 (23.9) | 8 (15.7) | 9 (45.0) | 0.014 |
| Dyslipidemia, n (%) | 18 (25.4) | 12 (23.5) | 6 (30.0) | 0.561 |
| Medications | ||||
| ACE inhibitors/ARBs | 19 (26.8) | 11 (21.6) | 8 (40.0) | 0.141 |
| β-Blockers | 25 (35.2) | 12 (23.5) | 13 (65.0) | 0.002 |
| Diuretics | 6 (8.5) | 2 (3.9) | 4 (20.0) | 0.049 |
| Calcium channel blockers | 6 (8.5) | 3 (5.9) | 3 (15.0) | 0.340 |
| NT pro-BNP (ng/L) | 91.96 ± 42.64 | 84.83 ± 43.21 | 109.01 ± 36.97 | 0.042 |
| Pathological stage (pTNM) | 0.0901 | |||
| 0 | 3 (4.2) | 3 (5.9) | 0 (0.0) | |
| IA | 21 (29.6) | 14 (27.5) | 7 (35.0) | |
| IB | 11 (15.5) | 7 (13.7) | 4 (20.0) | |
| IIA | 24 (33.8) | 18 (35.3) | 6 (30.0) | |
| IIB | 6 (8.5) | 4 (7.8) | 2 (10.0) | |
| IIIA | 5 (7.0) | 4 (7.8) | 1 (5.0) | |
| IIIB | 1 (1.4) | 1 (2.0) | 0 (0.0) |
| Regimen | All Patients (n = 71) | Noncardiotoxicity (n = 51, 71.8%) | Cardiotoxicity (n = 20, 28.2%) | p-Value |
|---|---|---|---|---|
| AC | 7 (9.9) | 5 (9.8) | 2 (10.0) | 1.000 |
| AC-paclitaxel | 47 (66.2) | 34 (66.7) | 13 (65.0) | 1.000 |
| AC-docetaxel | 6 (8.5) | 5 (9.8) | 1 (5.0) | 0.668 |
| FAC-docetaxel | 4 (5.6) | 3 (5.9) | 1 (5.0) | 1.000 |
| TAC | 4 (5.6) | 1 (2.0) | 3 (15.0) | 0.065 |
| FAC | 3 (4.2) | 3 (5.9) | 0 (0.0) | 0.554 |
| Doxorubicin cumulative dose (mg/m2) | 231.74 ± 29.03 | 231.81 ± 30.04 | 231.57 ± 27.01 | 0.505 |
| Baseline (n = 71) | Follow-up (n = 71) | p-Value | |
|---|---|---|---|
| LVEF (%) | 60.51 ± 1.89 | 53.94 ± 2.83 | <0.001 |
| GLS (%) | −20.96 ± 0.51 | −18.02 ± 1.01 | <0.001 |
| LVEDD (mm) | 46.25 ± 3.85 | 47.11 ± 3.76 | 0.157 |
| LVEDD index (mm/m2) | 24.94 ± 2.82 | 25.64 ± 3.69 | 0.204 |
| MAPSE (mm) | 14.96 ± 1.89 | 13.32 ± 1.74 | <0.001 |
| S′ mean (cm/s) | 9.17 ± 1.35 | 8.07 ± 1.21 | <0.001 |
| E (cm/s) | 73.38 ± 15.15 | 67.0 ± 13.14 | <0.022 |
| A (cm/s) | 72.49 ± 17.52 | 77.49 ± 18.07 | 0.126 |
| E/A ratio | 1.08 ± 0.36 | 0.91 ± 0.28 | 0.003 |
| E′ mean (cm/s) | 11.58 ± 2.83 | 9.94 ± 2.27 | <0.001 |
| E/e′ | 6.65 ± 1.39 | 7.17 ± 1.53 | 0.037 |
| Variables | Cardiotoxicity (n = 20, 28.2%) | No Cardiotoxicity (n = 51, 71.8%) | ||||
|---|---|---|---|---|---|---|
| Baseline | Follow-Up | p-Value | Baseline | Follow-Up | p-Value | |
| LVEF (%) | 62.20 ± 1.88 | 50.20 ± 2.38 | <0.001 | 59.84 ± 1.43 | 55.41 ± 1.13 | <0.001 |
| GLS (%) | −20.85 ± 0.35 | −17.03 ± 0.52 | <0.001 | −21.00 ± 0.55 | −18.40 ± 0.88 | <0.001 |
| LVEDD (mm) | 46.75 ± 2.45 | 47.50 ± 3.25 | 0.413 | 46.06 ± 4.28 | 46.95 ± 3.96 | 0.215 |
| LVEDD index (mm/m2) | 25.28 ± 3.10 | 25.75 ± 2.95 | 0.623 | 24.81 ± 2.72 | 25.60 ± 3.97 | 0.242 |
| MAPSE (mm) | 14.99 ± 1.69 | 13.01 ± 1.84 | <0.001 | 14.95 ± 1.99 | 13.44 ± 1.70 | <0.001 |
| S′ mean (cm/s) | 9.02 ± 1.18 | 7.62 ± 1.17 | <0.001 | 9.23 ± 1.42 | 8.24 ± 1.19 | <0.001 |
| E (cm/s) | 73.70 ± 15.18 | 65.85 ± 11.74 | 0.107 | 73.25 ± 15.28 | 67.45 ± 13.73 | 0.079 |
| A (cm/s) | 70.15 ± 17.35 | 76.95 ± 19.16 | 0.247 | 73.41 ± 17.66 | 77.71 ± 17.82 | 0.225 |
| E/A ratio | 1.12 ± 0.37 | 0.91 ± 0.32 | 0.022 | 1.07 ± 0.36 | 0.90 ± 0.26 | 0.019 |
| E′ mean (cm/s) | 11.41 ± 2.38 | 9.99 ± 2.61 | 0.082 | 11.64 ± 2.40 | 9.92 ± 2.15 | <0.001 |
| E/E′ ratio | 6.77 ± 1.24 | 7.20 ± 1.32 | 0.291 | 6.60 ± 1.46 | 7.15 ± 1.62 | 0.066 |
| Polymorphism | Cardiotoxicity | p-Value * | OR (95% CI) | p-Value | Adjusted OR a (95% CI) | p-Value | Adjusted OR b (95% CI) | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| No (n = 51, 71.8%) | Yes (n = 20, 28.2%) | ||||||||
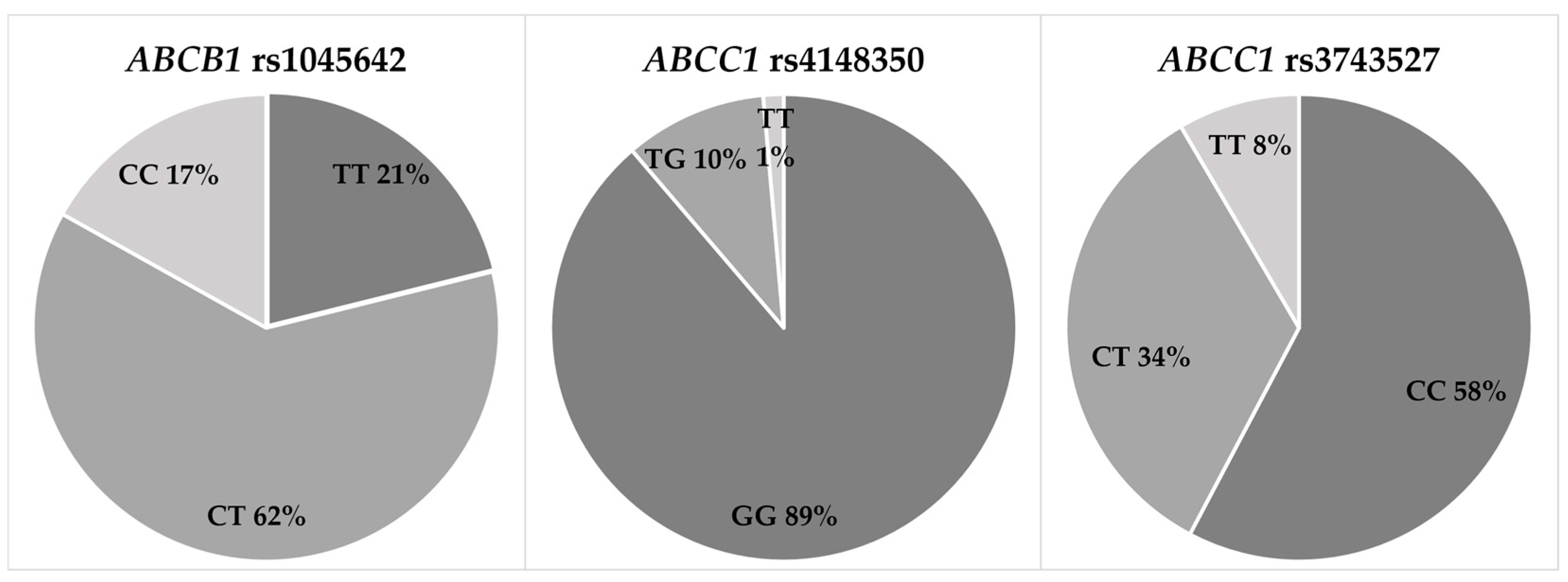
| ABCB1 rs1045642 | |||||||||
| TT | 10 (19.6) | 5 (25.0) | 0.806 | 1 (reference) | 1 (reference) | 1 (reference) | |||
| CT | 33 (64.7) | 11 (55.0) | 0.667 (0.187–2.379) | 0.532 | 0.640 (0.146–2.806) | 0.554 | 0.603 (0.136–2.672) | 0.505 | |
| CC | 8 (15.7) | 4 (20.0) | 1.000 (0.200–5.004) | 1.000 | 1.235 (0.199–7.665) | 0.821 | 1.319 (0.209–8.310) | 0.768 | |
| CC, CT vs. TT | 0.732 (0.215–2.492) | 0.617 | 0.752 (0.182–3.102) | 0.693 | 0.737 (0.178–3.047) | 0.673 | |||
| CC vs. CT, TT | 1.344 (0.355–5.083) | 0.663 | 1.704 (0.383–7.589) | 0.484 | 1.870 (0.401–8.725) | 0.426 | |||
| ABCC1 rs4148350 | |||||||||
| GG | 48 (94.1) | 15 (75.0) | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| TG | 2 (3.9) | 5 (25.0) | 0.016 | 8.000 (1.405–45.547) | 0.019 | 9.258 (1.364–62.846) | 0.023 | 9.661 (1.418–65.824) | 0.021 |
| TT | 1 (2.0) | 0 (0.0) | x | x | x | ||||
| TT, TG vs. GG | 5.333 (1.138–24.985) | 0.034 | 6.370 (1.171–34.642) | 0.032 | 6.544 (1.202–35.615) | 0.030 | |||
| TT vs. TG, GG | x | x | x | ||||||
| ABCC1 rs3743527 | |||||||||
| CC | 29 (56.9) | 12 (60.0) | 0.856 | 1 (reference) | 1 (reference) | 1 (reference) | |||
| CT | 17 (33.3) | 7 (35.0) | 0.995 (0.329–3.013) | 0.993 | 0.846 (0.224–3.196) | 0.805 | 0.834 (0.220–3.169) | 0.790 | |
| TT | 5 (9.8) | 1 (5.0) | 0.483 (0.051–4.586) | 0.527 | 0.638 (0.061–6.707) | 0.708 | 0.626 (0.060–6.582) | 0.697 | |
| TT, CT vs. CC | 0.879 (0.307–2.517) | 0.810 | 0.797 (0.234–2.709) | 0.716 | 0.784 (0.229–2.680) | 0.698 | |||
| TT vs. CT, CC | 0.484 (0.053–4.425) | 0.521 | 0.669 (0.066–6.796) | 0.734 | 0.660 (0.065–6.696) | 0.725 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muckiene, G.; Vaitiekus, D.; Zaliaduonyte, D.; Bartnykaite, A.; Plisiene, J.; Zabiela, V.; Juozaityte, E.; Jurkevicius, R. The Impact of Polymorphisms in ATP-Binding Cassette Transporter Genes on Anthracycline-Induced Early Cardiotoxicity in Patients with Breast Cancer. J. Cardiovasc. Dev. Dis. 2023, 10, 232. https://doi.org/10.3390/jcdd10060232
Muckiene G, Vaitiekus D, Zaliaduonyte D, Bartnykaite A, Plisiene J, Zabiela V, Juozaityte E, Jurkevicius R. The Impact of Polymorphisms in ATP-Binding Cassette Transporter Genes on Anthracycline-Induced Early Cardiotoxicity in Patients with Breast Cancer. Journal of Cardiovascular Development and Disease. 2023; 10(6):232. https://doi.org/10.3390/jcdd10060232
Chicago/Turabian StyleMuckiene, Gintare, Domas Vaitiekus, Diana Zaliaduonyte, Agne Bartnykaite, Jurgita Plisiene, Vytautas Zabiela, Elona Juozaityte, and Renaldas Jurkevicius. 2023. "The Impact of Polymorphisms in ATP-Binding Cassette Transporter Genes on Anthracycline-Induced Early Cardiotoxicity in Patients with Breast Cancer" Journal of Cardiovascular Development and Disease 10, no. 6: 232. https://doi.org/10.3390/jcdd10060232
APA StyleMuckiene, G., Vaitiekus, D., Zaliaduonyte, D., Bartnykaite, A., Plisiene, J., Zabiela, V., Juozaityte, E., & Jurkevicius, R. (2023). The Impact of Polymorphisms in ATP-Binding Cassette Transporter Genes on Anthracycline-Induced Early Cardiotoxicity in Patients with Breast Cancer. Journal of Cardiovascular Development and Disease, 10(6), 232. https://doi.org/10.3390/jcdd10060232