
Outcomes of the Valve-Sparing Root Replacement Procedure with Partial Upper Sternotomy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Follow Up
2.2. Surgical Technique
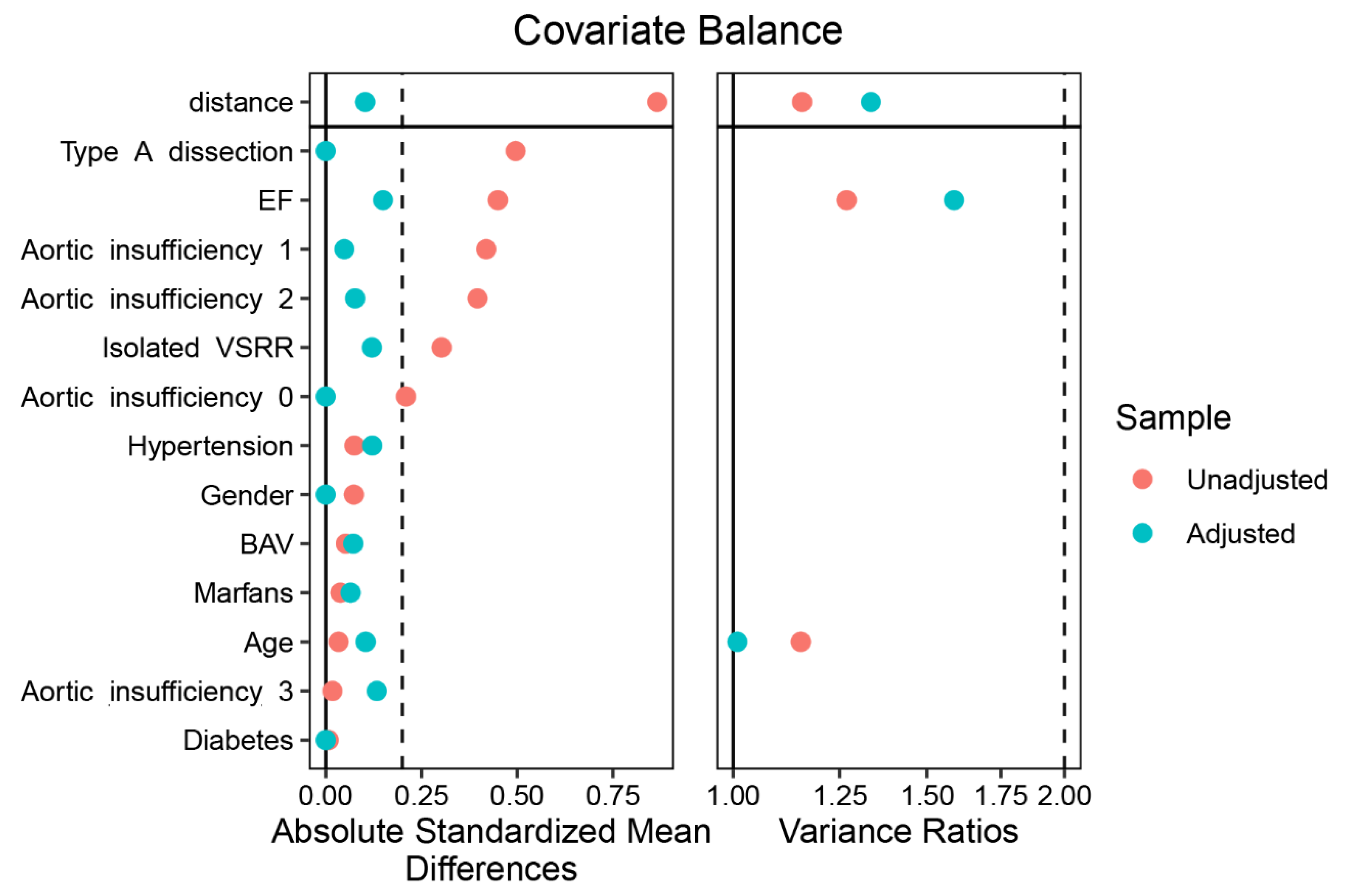
2.3. Statistical Analysis
3. Results
3.1. Patient Baseline Characteristics
3.2. Perioperative Data
3.3. Postoperative Mortality, Morbidity, and Hospitalization Expenses
3.4. Follow-Up and Characteristics of Echocardiography
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- David, T.E.; Feindel, C.M. An aortic valve-sparing operation for patients with aortic incompetence and aneurysm of the ascending aorta. J. Thorac. Cardiovasc. Surg. 1992, 103, 617–621. [Google Scholar] [CrossRef]
- David, T.E.; Armstrong, S.; Manlhiot, C.; McCrindle, B.W.; Feindel, C.M. Long-term results of aortic root repair using the reimplantation technique. J. Thorac. Cardiovasc. Surg. 2013, 145, S22–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Huang, Y.; Qiu, J.; Saeed, B.; Yu, C. Is valve-sparing root replacement a safe option in acute type A aortic dissection? A systematic review and meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 766–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneko, T.; Couper, G.S.; Borstlap, W.A.A.; Nauta, F.J.H.; Wollersheim, L.; McGurk, S.; Cohn, L.H. Minimal-access aortic valve replacement with concomitant aortic procedure: A 9-year experience. Innovations 2012, 7, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, M.L.; Junge, A.; Haverich, A.; Martens, A. David procedure through an upper partial sternotomy. Ann. Cardiothorac. Surg. 2015, 4, 212–213. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, E.; Martens, A.; Krüger, H.; Korte, W.; Kaufeld, T.; Stettinger, A.; Haverich, A.; Shrestha, M.L. Aortic valve-sparing root replacement in patients with bicuspid aortic valve: Long-term outcome with the David I procedure over 20 years. Eur. J. Cardiothorac. Surg. 2020, 58, 86–93. [Google Scholar] [CrossRef] [PubMed]
- De Paulis, R.; Scaffa, R.; Chirichilli, I. Valve sparing root replacement: An update. Curr. Opin. Cardiol. 2020, 35, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Svensson, L.G. Minimal-access “J” or “j” sternotomy for valvular, aortic, and coronary operations or reoperations. Ann. Thorac. Surg. 1997, 64, 1501–1503. [Google Scholar] [CrossRef]
- Shrestha, M.; Krueger, H.; Umminger, J.; Koigeldiyev, N.; Beckmann, E.; Haverich, A.; Martens, A. Minimally invasive valve sparing aortic root replacement (David procedure) is safe. Ann. Cardiothorac. Surg. 2015, 4, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Monsefi, N.; Risteski, P.; Miskovic, A.; Moritz, A.; Zierer, A. Midterm Results of a Minimally Invasive Approach in David Procedure. Thorac. Cardiovasc. Surg. 2018, 66, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Elghannam, M.; Aljabery, Y.; Naraghi, H.; Moustafine, V.; Bechte, M.; Strauch, J.; Haldenwang, P. Minimally invasive aortic root surgery: Midterm results in a 2-year follow-up. J. Card. Surg. 2020, 35, 1484–1491. [Google Scholar] [CrossRef] [PubMed]
- Wachter, K.; Franke, U.F.W.; Yadav, R.; Nagib, R.; Ursulescu, A.; Ahad, S.; Baumbach, H. Feasibility and clinical outcome after minimally invasive valve-sparing aortic root replacement. Interact. Cardiovasc. Thorac. Surg. 2017, 24, 377–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayner, T.A.; Harrison, S.; Rival, P.; Mahoney, D.E.; Caputo, M.; Angelini, G.D.; Savović, J.; Vohra, H.A. Minimally invasive versus conventional surgery of the ascending aorta and root: A systematic review and meta-analysis. Eur. J. Cardiothorac. Surg. 2020, 57, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Dieberg, G.; Smart, N.A.; King, N. Minimally invasive cardiac surgery: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 223, 554–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, C.; Gupta, S.; Chandrakumar, D.; Nienaber, T.A.; Indraratna, P.; Ang, S.C.; Phan, K.; Yan, T.D. A meta-analysis of minimally invasive versus conventional mitral valve repair for patients with degenerative mitral disease. Ann. Cardiothorac. Surg. 2013, 2, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Hastaoglu, İ.O.; Tokoz, H.; Ozgen, A.; Bilgen, F. Proximal Aortic Surgery: Upper “J” or Conventional Sternotomy? Heart Surg. Forum 2018, 21, E004–E008. [Google Scholar] [CrossRef] [PubMed]
- Augustin, P.; Tanaka, S.; Chhor, V.; Provenchère, S.; Arnaudovski, D.; Ibrahim, H.; Dilly, M.-P.; Allou, N.; Montravers, P.; Philip, I. Prognosis of Prolonged Intensive Care Unit Stay After Aortic Valve Replacement for Severe Aortic Stenosis in Octogenarians. J. Cardiothorac. Vasc. Anesth. 2016, 30, 1555–1561. [Google Scholar] [CrossRef] [PubMed]
- Augoustides, J.G.; Pochettino, A.; Ochroch, E.A.; Cowie, D.; McGarvey, M.L.; Weiner, J.; Gambone, A.J.; Pinchasik, D.; Cheung, A.T.; Bavaria, J.E. Clinical predictors for prolonged intensive care unit stay in adults undergoing thoracic aortic surgery requiring deep hypothermic circulatory arrest. J. Cardiothorac. Vasc. Anesth. 2006, 20, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, M.E.; Vaughan, K.; Chong, C.A.K.Y.; Neumann, P.J.; Bell, C.M. Cost-Effectiveness Studies in the ICU: A Systematic Review. Crit. Care Med. 2019, 47, 1011–1017. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Cohort (n = 217) | Propensity-Matched Cohort (n = 104) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall | Complete Sternotomy | Partial Upper Sternotomy | p | SMD | Complete Sternotomy | Partial Upper Sternotomy | p | SMD | |
| n = 217 | n = 165 | n = 52 | n = 52 | n = 52 | |||||
| Age, years (mean (SD)) | 45.58 (12.74) | 45.48 (12.97) | 45.89 (12.09) | 0.842 | 0.032 | 44.63 (12.03) | 45.89 (12.09) | 0.595 | 0.104 |
| Gender, n (%) | 188 (86.6) | 144 (87.3) | 44 (84.6) | 0.797 | 0.077 | 44 (84.6) | 44 (84.6) | 1 | <0.001 |
| BMI (mean (SD)) | 24.68 (3.54) | 24.83 (3.57) | 24.22 (3.41) | 0.282 | 0.174 | 25.34 (3.58) | 24.22 (3.41) | 0.107 | 0.319 |
| Type A dissection, n (%) | 27 (12.4) | 27 (16.4) | 0 (0.0) | 0.004 | 0.626 | 0 (0) | 0 (0) | 1 | <0.001 |
| Marfan syndrome, n (%) | 19 (8.8) | 14 (8.5) | 5 (9.6) | 1 | 0.039 | 6 (11.5) | 5 (9.6) | 1 | 0.063 |
| BAV, n (%) | 19 (8.8) | 15 (9.1) | 4 (7.7) | 0.976 | 0.05 | 5 (9.6) | 4 (7.7) | 1 | 0.068 |
| Hypertension, n (%) | 81 (37.3) | 63 (38.2) | 18 (34.6) | 0.765 | 0.074 | 21 (40.4) | 18 (34.6) | 0.685 | 0.119 |
| Diabetes, n (%) | 4 (1.8) | 3 (1.8) | 1 (1.9) | 1 | 0.008 | 1 (1.9) | 1 (1.9) | 1 | <0.001 |
| Aortic insufficiency, n (%) | 0.036 | 0.483 | 0.917 | 0.14 | |||||
| None | 15 (6.9) | 13 (7.9) | 2 (3.8) | 2 (3.8) | 2 (3.8) | ||||
| Mild | 69 (31.8) | 59 (35.8) | 10 (19.2) | 11 (21.2) | 10 (19.2) | ||||
| Moderate | 80 (36.9) | 5 (32.1) | 27 (51.9) | 29 (55.8) | 27 (51.9) | ||||
| Severe | 53 (24.4) | 40 (24.2) | 13 (25.0) | 10 (19.2) | 13 (25.0) | ||||
| Total Cohort (n = 217) | Propensity-Matched Cohort (n = 104) | |||||||
|---|---|---|---|---|---|---|---|---|
| Complete Sternotomy | Partial Upper Sternotomy | p | SMD | Complete Sternotomy | Partial Upper Sternotomy | p | SMD | |
| n = 165 | n = 52 | n = 52 | n = 52 | |||||
| Isolated VSRR, n (%) | 130 (78.8) | 46 (88.5) | 0.177 | 0.264 | 48 (92.3) | 46 (88.5) | 0.739 | 0.131 |
| Partial arch replacement, n (%) | 10 (6.1) | 4 (7.7) | 0.925 | 0.065 | 3 (5.8) | 4 (7.7) | 1 | 0.077 |
| Total arch repair, n (%) | 25 (15.2) | 1 (1.9) | 0.021 | 0.487 | 1 (1.9) | 1 (1.9) | 1 | <0.001 |
| Frozen elephant trunk, n (%) | 21 (12.7) | 1 (1.9) | 0.047 | 0.424 | 0 (0.0) | 1 (1.9) | 1 | 0.198 |
| Surgery time, h (mean (SD)) | 6.74 (1.73) | 5.13 (1.06) | <0.001 | 1.123 | 6.40 (1.42) | 5.13 (1.06) | <0.001 | 1.015 |
| Blood loss, mL (median [IQR]) | 800 [780,800] | 710 [660,800] | 0.025 | 0.275 | 800 [761.25,800] | 710 [660,800] | 0.275 | 0.129 |
| CPB time, min (mean (SD)) | 181.84 (55.96) | 138.98 (30.94) | <0.001 | 0.948 | 170.71 (44.65) | 138.98 (30.94) | <0.001 | 0.826 |
| ACC time, min (mean (SD)) | 145.88 (38.54) | 110.56 (19.91) | <0.001 | 1.151 | 137.81 (29.20) | 110.56 (19.91) | <0.001 | 1.09 |
| Graft diameter, mm (mean (SD)) | 28.73 (1.62) | 28.50 (1.36) | 0.36 | 0.153 | 28.73 (1.54) | 28.50 (1.36) | 0.42 | 0.159 |
| RBC input (median [IQR]) | 0 [0.2] | 0 [0,0] | 0.018 | 0.387 | 0 [0.2] | 0 [0,0] | 0.114 | 0.276 |
| Plasma input, ml (median [IQR]) | 0 [0,400] | 0 [0,0] | 0.001 | 0.444 | 0 [0,400] | 0 [0,0] | 0.023 | 0.34 |
| PLT input (median [IQR]) | 1 [1,1] | 1 [0,1] | 0.069 | 0.32 | 1 [1,1] | 1 [0,1] | 0.462 | 0.119 |
| Total Cohort (n = 217) | Propensity-Matched Cohort (n= 104) | |||||||
|---|---|---|---|---|---|---|---|---|
| Complete Sternotomy | Partial Upper Sternotomy | p | SMD | Complete Sternotomy | Partial Upper Sternotomy | p | SMD | |
| n = 165 | n = 52 | n = 52 | n = 52 | |||||
| In hospital mortality, n (%) | 1 (0.6) | 0 (0.0) | 1 | 0.11 | 0 (0.0) | 0 (0.0) | 1 | <0.001 |
| Hospitalization expenses | 152,075.56 (58,064.36) | 123,380.15 (27,062.82) | 0.001 | 0.633 | 135,649.52 (29,992.21) | 123,380.15 (27,062.82) | 0.031 | 0.43 |
| ICU time, h (mean (SD)) | 74.20 (47.21) | 50.94 (30.16) | 0.001 | 0.587 | 70.25 (48.65) | 50.94 (30.16) | 0.017 | 0.477 |
| Mechanical ventilation, h (mean (SD)) | 18.98 (25.81) | 14.50 (8.33) | 0.221 | 0.233 | 18.26 (36.23) | 14.50 (8.33) | 0.468 | 0.143 |
| Drainage Volume 24 h, ml (mean (SD)) | 404.42 (225.52) | 361.54 (177.22) | 0.211 | 0.211 | 375.19 (216.35) | 361.54 (177.22) | 0.726 | 0.069 |
| Postoperative moderate to severe AI, n (%) | 0 (0.0) | 0 (0.0) | 1 | <0.001 | 0 (0.0) | 0 (0.0) | 1 | <0.001 |
| Re exploration, n (%) | 1 (0.6) | 0 (0.0) | 1 | 0.11 | 0 (0.0) | 0 (0.0) | 1 | <0.001 |
| Acute kidney injury, n (%) | 3 (1.8) | 0 (0.0) | 0.766 | 0.192 | 0 (0.0) | 0 (0.0) | 1 | <0.001 |
| Arrhythmia, n (%) | 4 (2.4) | 0 (0.0) | 0.588 | 0.223 | 2 (3.8) | 0 (0.0) | 0.475 | 0.283 |
| Pericardial pleural effusion, n (%) | 6 (3.6) | 2 (3.8) | 1 | 0.011 | 4 (7.7) | 2 (3.8) | 0.674 | 0.166 |
| Overall | Complete Sternotomy | Partial Upper Sternotomy | p | |
|---|---|---|---|---|
| Preoperative | n = 104 | n = 52 | n = 52 | |
| Annulus diameter, mm (mean (SD)) | 26.65 (2.89) | 26.67 (3.07) | 26.63 (2.73) | 0.937 |
| Sinus diameter, mm (mean (SD)) | 51.92 (6.82) | 52.58 (7.27) | 51.27 (6.33) | 0.33 |
| Ascending aorta diameter, mm (mean (SD)) | 42.51 (8.36) | 42.87 (8.88) | 42.15 (7.87) | 0.666 |
| EF, % (mean (SD)) | 63.39 (3.82) | 63.08 (3.37) | 63.71 (4.24) | 0.4 |
| LVEDD, mm (mean (SD)) | 56.51 (9.83) | 56.37 (11.57) | 56.65 (7.84) | 0.882 |
| Moderate to severe AI, n (%) | 79 (76.0) | 39 (75.0) | 40 (76.9) | 1 |
| Postoperative (before Discharge from Hospital) | n = 104 | n = 52 | n = 52 | |
| Aortic Annulus diameter, mm (mean (SD)) | 21.68 (4.57) | 22.82 (2.45) | 20.74 (5.63) | 0.073 |
| Sinus diameter, mm (mean (SD)) | 28.56 (6.00) | 30.11 (3.54) | 27.39 (7.16) | 0.075 |
| Ascending aorta diameter, mm (mean (SD)) | 29.15 (2.96) | 28.71 (3.22) | 29.56 (2.66) | 0.154 |
| EF, % (mean (SD)) | 60.62 (4.44) | 60.56 (4.67) | 60.67 (4.24) | 0.895 |
| LVEDD, mm (mean (SD)) | 48.75 (6.37) | 48.83 (5.53) | 48.67 (7.16) | 0.903 |
| Moderate to severe AI, n (%) | 0 (0) | 0 (0) | 0 (0) | 1 |
| Latest Follow Up | n = 81 | n = 44 | n = 37 | |
| Annulus diameter, mm (mean (SD)) | 22.62 (2.42) | 22.71 (2.79) | 22.50 (1.85) | 0.724 |
| Sinus diameter, mm (mean (SD)) | 29.58 (3.09) | 29.56 (3.32) | 29.61 (2.81) | 0.944 |
| Ascending aorta diameter, mm (mean (SD)) | 29.05 (2.54) | 28.91 (2.89) | 29.23 (2.06) | 0.582 |
| EF, % (mean (SD)) | 63.01 (5.32) | 63.77 (5.47) | 62.11 (5.07) | 0.162 |
| LVEDD, mm (mean (SD)) | 49.84 (7.61) | 48.64 (9.65) | 51.27 (3.66) | 0.121 |
| Moderate to severe AI, n (%) | 5 (6.2) | 3 (6.8) | 2 (5.4) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, B.; Zhao, R.; Wang, D.; Wang, W.; Zhao, Z.; Sun, X.; Qian, X.; Yu, C. Outcomes of the Valve-Sparing Root Replacement Procedure with Partial Upper Sternotomy. J. Cardiovasc. Dev. Dis. 2021, 8, 154. https://doi.org/10.3390/jcdd8110154
Hou B, Zhao R, Wang D, Wang W, Zhao Z, Sun X, Qian X, Yu C. Outcomes of the Valve-Sparing Root Replacement Procedure with Partial Upper Sternotomy. Journal of Cardiovascular Development and Disease. 2021; 8(11):154. https://doi.org/10.3390/jcdd8110154
Chicago/Turabian StyleHou, Bin, Rui Zhao, De Wang, Wei Wang, Zhenhua Zhao, Xiaogang Sun, Xiangyang Qian, and Cuntao Yu. 2021. "Outcomes of the Valve-Sparing Root Replacement Procedure with Partial Upper Sternotomy" Journal of Cardiovascular Development and Disease 8, no. 11: 154. https://doi.org/10.3390/jcdd8110154
APA StyleHou, B., Zhao, R., Wang, D., Wang, W., Zhao, Z., Sun, X., Qian, X., & Yu, C. (2021). Outcomes of the Valve-Sparing Root Replacement Procedure with Partial Upper Sternotomy. Journal of Cardiovascular Development and Disease, 8(11), 154. https://doi.org/10.3390/jcdd8110154