
Head to Head Comparison between Different 3-Dimensional Echocardiographic Rendering Tools in the Imaging of Percutaneous Edge-to-Edge Mitral Valve Repair

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
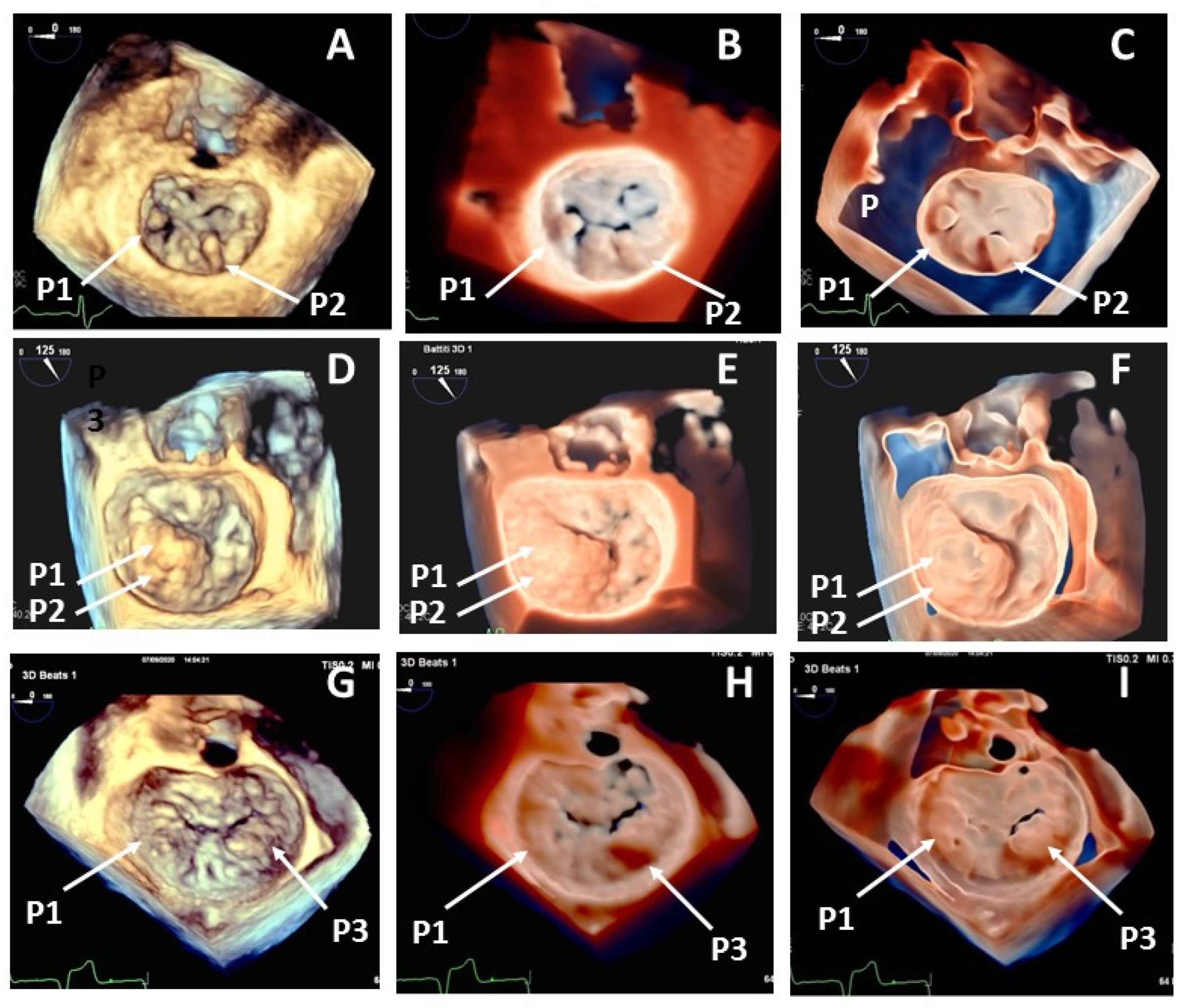
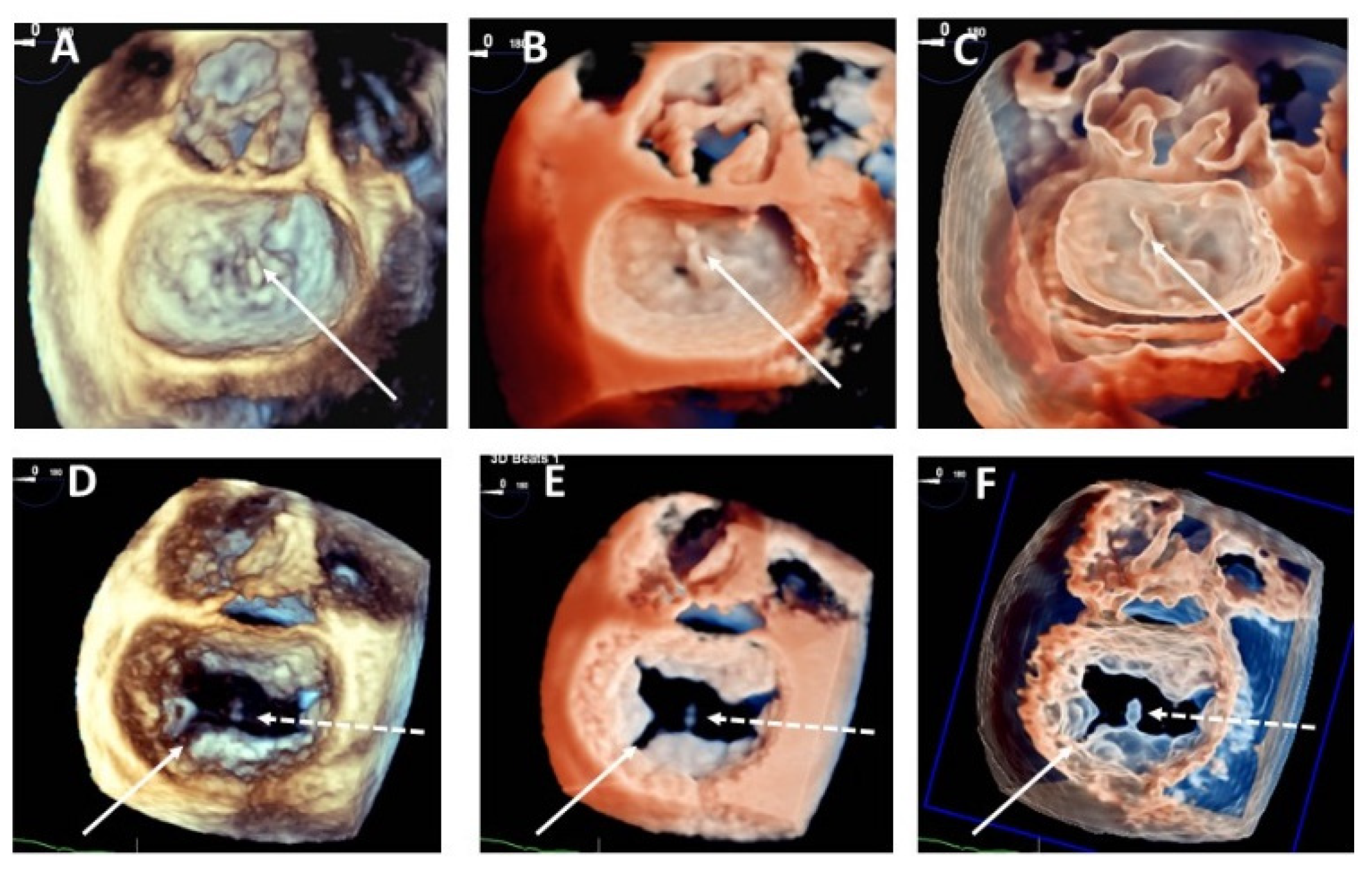
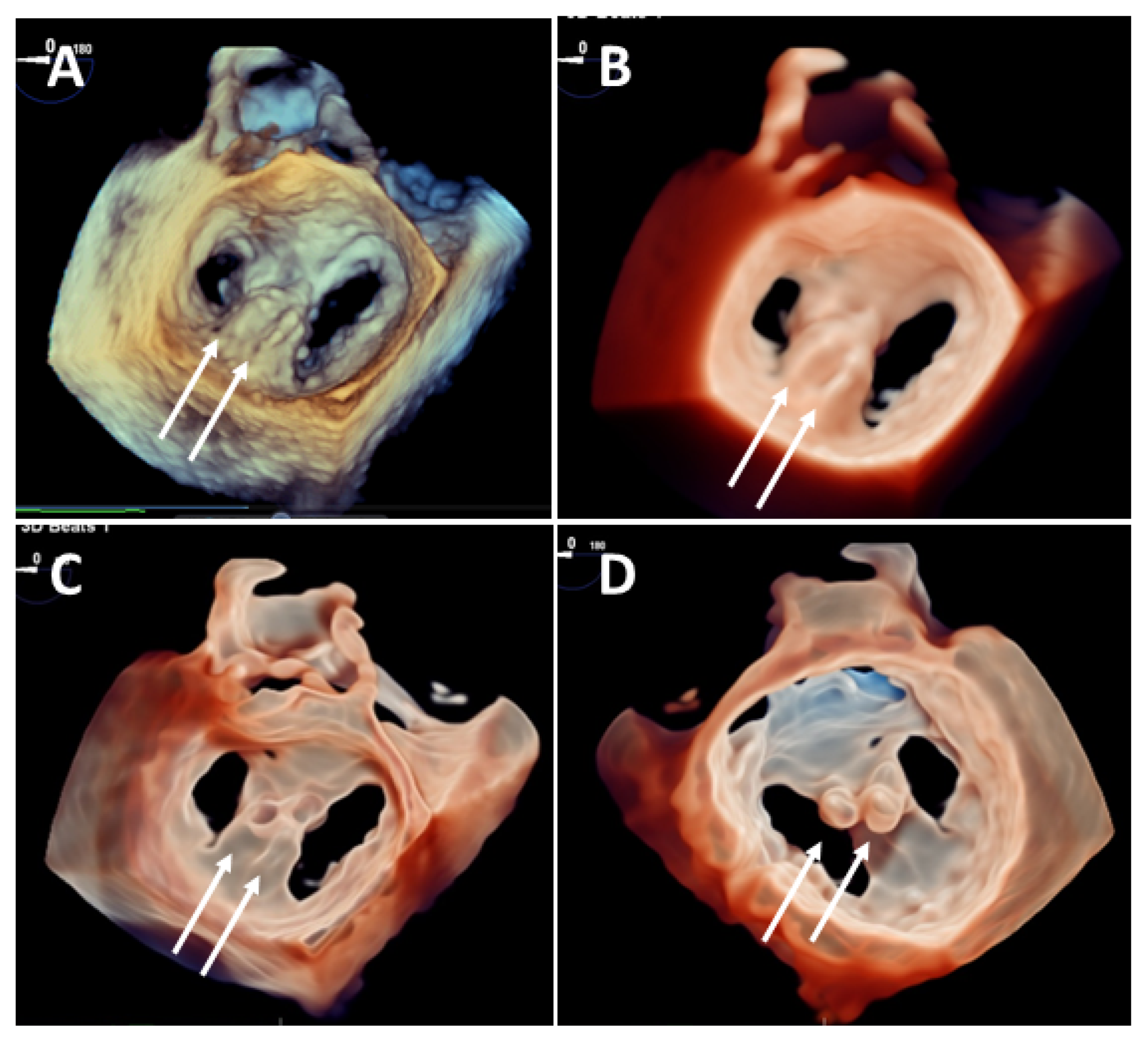
3.1. Mitral Valve Anatomy
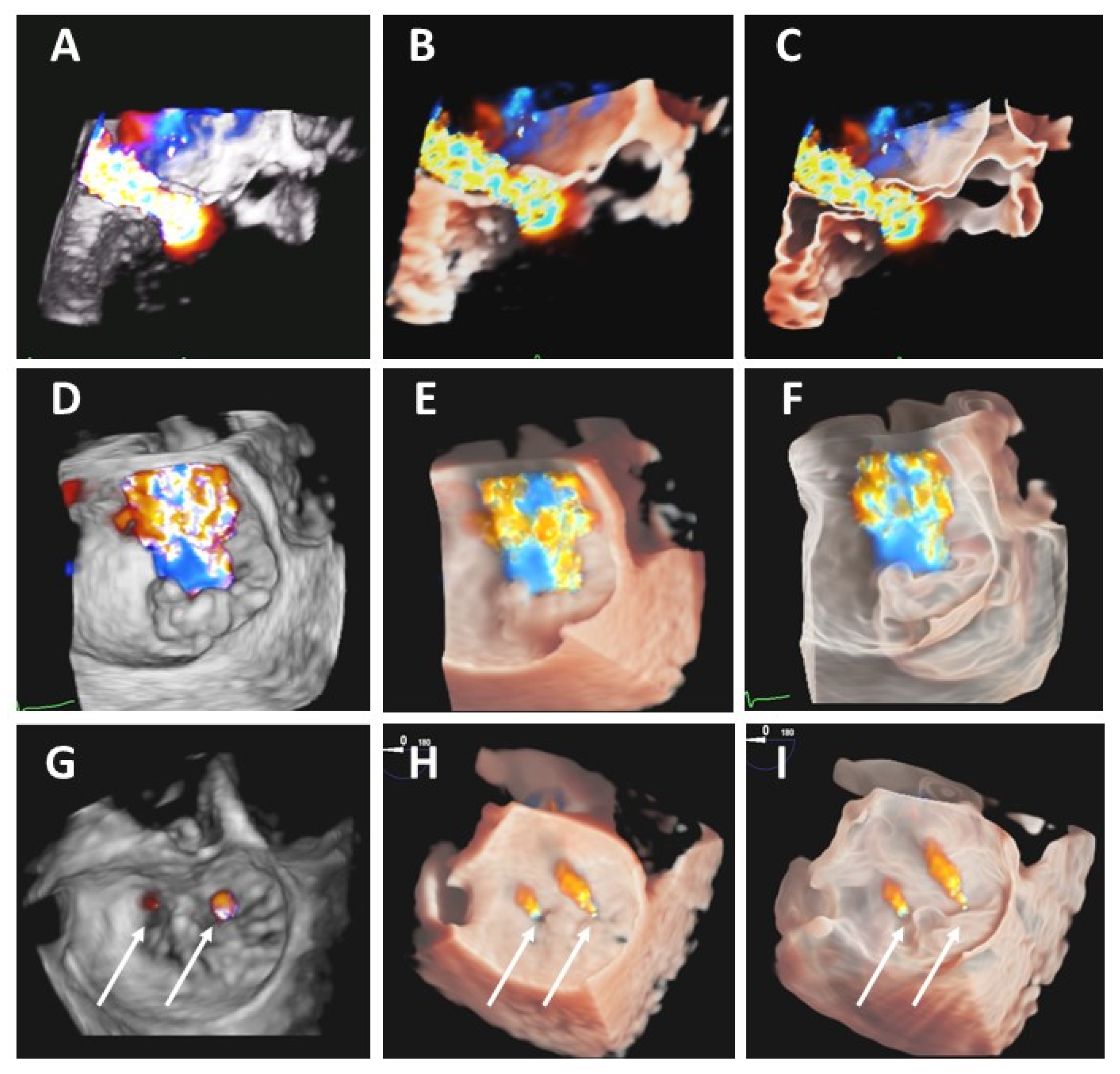
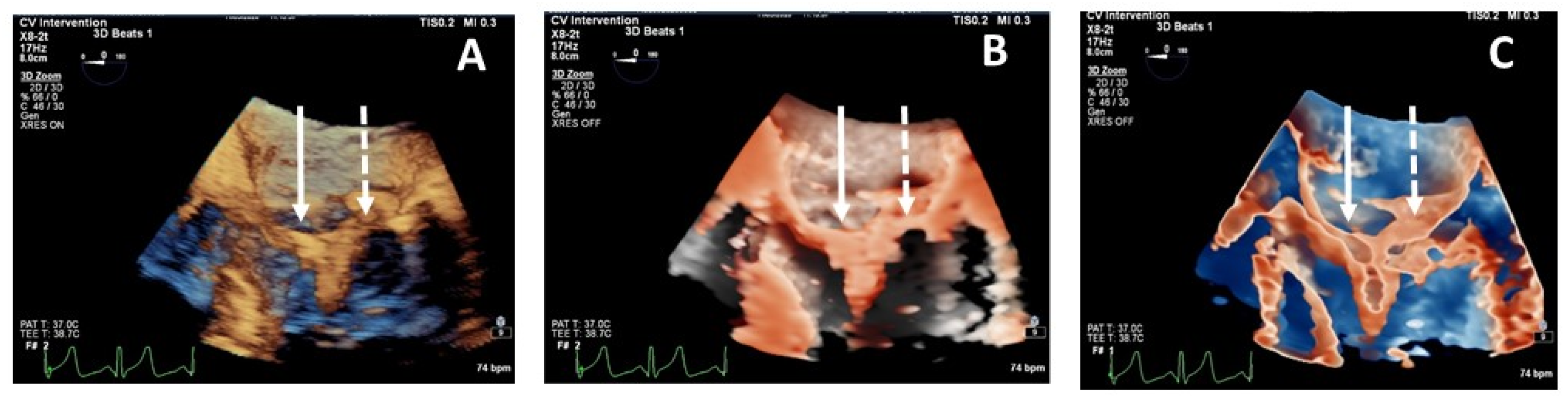
3.2. Regurgitant Color Jets
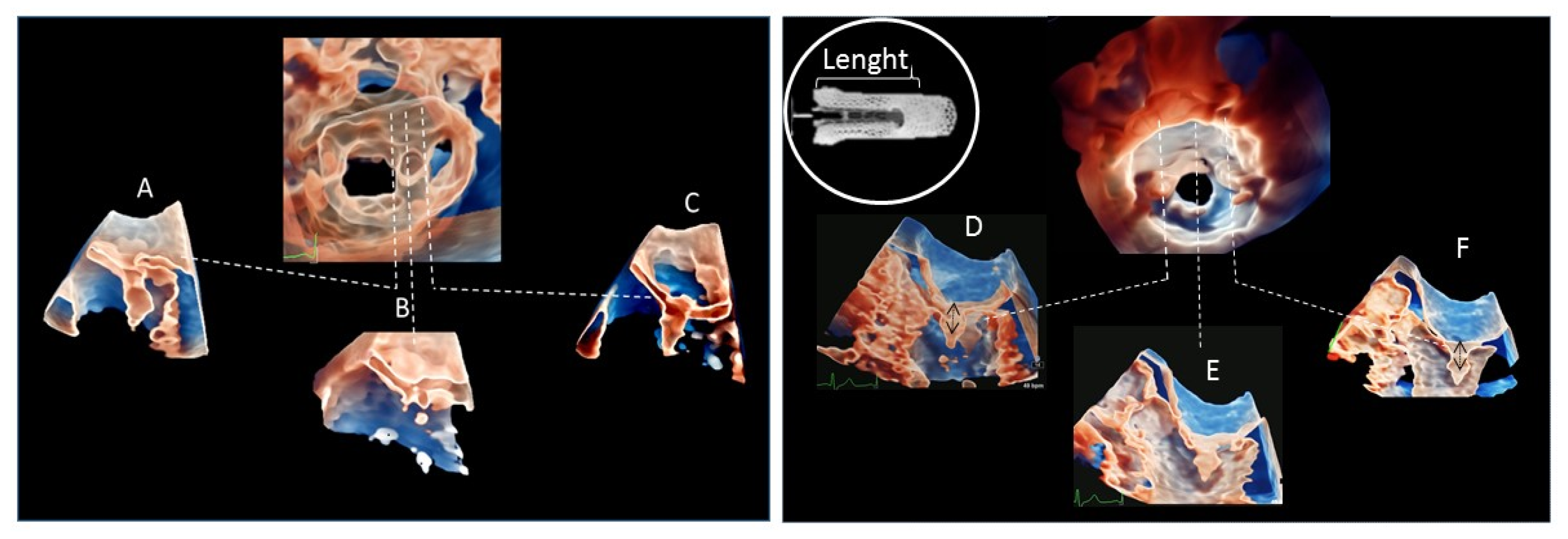
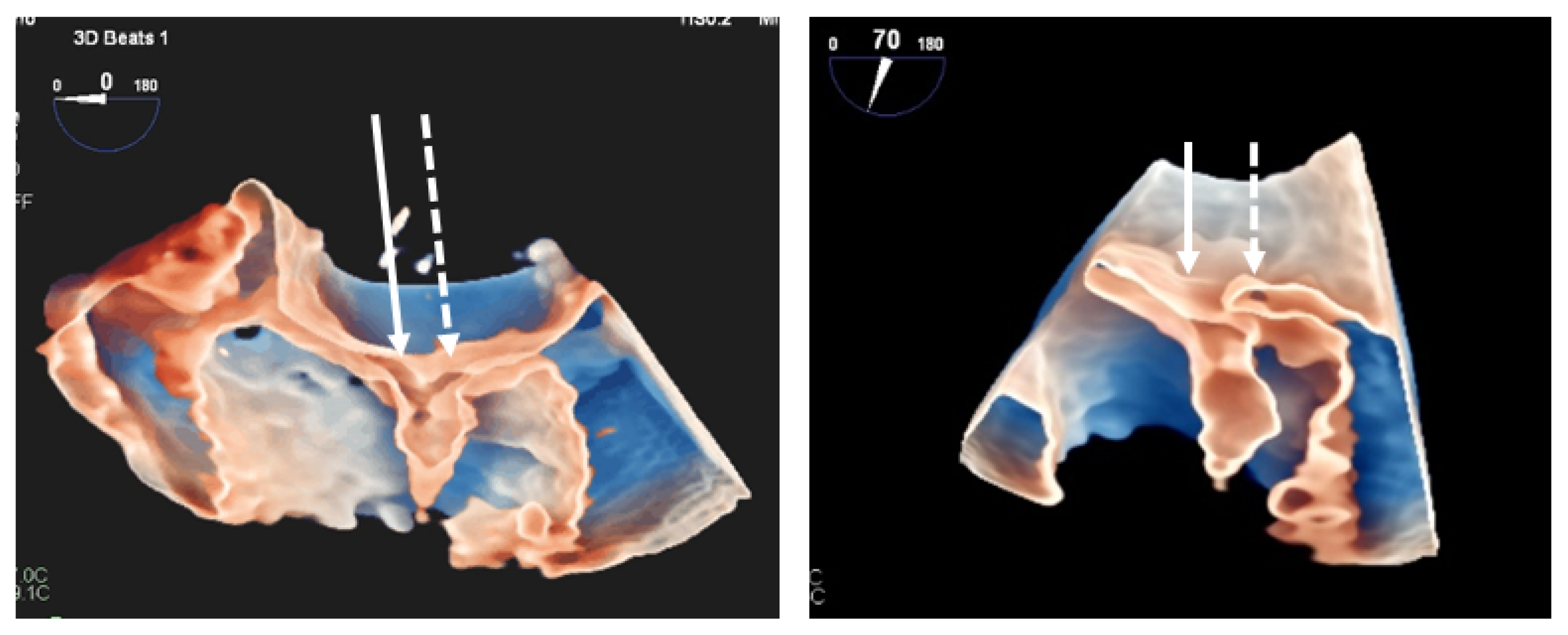
3.3. Clip Implantation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feldman, T.; Kar, S.; Elmariah, S.; Smart, S.C.; Trento, A.; Siegel, R.J.; Apruzzese, P.; Fail, P.; Rinaldi, M.J.; Smalling, R.W.; et al. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. J. Am. Coll. Cardiol. 2015, 66, 2844–2854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falk, V.; Baumgartner, H.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac1, E.; Muñoz, D.R.; et al. ESC/EACTS Guidelines on the management of valvular heart disease. Eur. J. Cardiothorac. Surg. 2017, 52, 616–664. [Google Scholar] [CrossRef]
- Mantegazza, V.; Pasquini, A.; Agati, L.; Fusini, L.; Muratori, M.; Gripari, P.; Ali, S.G.; Vignati, C.; Bartorelli, A.L.; Ferrari, C.; et al. Comprehensive Assessment of Mitral Valve Geometry and Cardiac Remodeling with 3-Dimensional Echocardiography After Percutaneous Mitral Valve Repair. Am. J. Cardiol. 2018, 122, 1195–1203. [Google Scholar] [CrossRef]
- Cavalcante, J.L.; Rodriguez, L.L.; Kapadia, S.; Tuzcum, E.M.; Stewardm, W.J. Role of echocardiography in percutaneous mitral valve interventions. J. Am. Coll. Cardiol. Imaging 2012, 5, 733–746. [Google Scholar] [CrossRef] [Green Version]
- Gripari, P.; Maffessanti, F.; Tamborini, G.; Muratori, M.; Fusini, L.; Ali, S.G.; Ferrari, C.; Alamanni, F.; Bartorelli, A.L.; Fiorentini, C.; et al. Patients selection for MitraClip: Time to move to transthoracic echocardiographic screening? Int. J. Cardiol. 2014, 176, 491–494. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Badano, L.P.; Bruce, C.; Chan, K.L.; Gonçalves, A.; Hahn, R.T.; Keane, M.G.; Canna, G.L.; Monaghan, M.J.; Nihoyannopoulos, P.; et al. EAE/ASE recommendations for the use of echocardiography in new transcatheter interventions for valvular heart disease. Eur. Heart J. 2011, 32, 2189–2214. [Google Scholar] [CrossRef]
- Faletra, F.F.; Berrebi, A.; Pedrazzini, G.; Leo, L.A.; Paiocchi, V.L.; Cautilli, G.; Casso, G.; Cassina, T.; Moccetti, T.; Malouf, J.F. 3D transesophageal echocardiography: A new imaging tool for assessment of mitral regurgitation and for guiding percutaneous edge-to-edge mitral valve repair. Prog. Cardiovasc. Dis. 2017, 60, 305–321. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, K.T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Karagodin, I.; Addetia, K.; Singh, A.; Dow, A.; Rivera, L.; DeCara, J.M.; Soulat-Dufour, L.; Yamat, M.; Kruse, E.; Shah, A.P.; et al. Improved Delineation of Cardiac Pathology Using a Novel Three-Dimensional Echocardiographic Tissue Transparency Tool. J. Am. Soc. Echocardiogr. 2020, 33, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Volpato, V.; Mantegazza, V.; Tamborini, G.; Muratori, M.; Gripari, P.; Andreini, D.; Fusini, L.; Alù, S.G.; Cefalù, C.; Italiano, G.; et al. Diagnostic Accuracy of Transillumination in Mitral Valve Prolapse: Side-by-Side Comparison of Standard Transthoracic Three-Dimensional Echocardiography against Surgical Findings. J. Am. Soc. Echocardiogr. 2021, 34, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Nagura, F.; Kataoka, A.; Watanabe, Y.; Kozuma, K. New three-dimensional rendering image of transoesophageal echocardiography for second transseptal puncture for transcatheter mitral valve repair. EuroIntervention 2019, 15, e764–e765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreiro-Perez, M.; Cruz-González, I.; Villa Gil-Ortega, M.; Guisado Rasco, A.; Sánchez, P.L. Photo-Realistic Echocardiography Imaging During Percutaneous Paravalvular Leak Closure. JACC Cardiovasc. Interv. 2020, 13, e185–e187. [Google Scholar] [CrossRef] [PubMed]
- Genovese, D.; Addetia, K.; Kebed, K.; Kruse, E.; Yamat, M.; Narang, A.; Patel, A.R.; Badano, L.P.; Muraru, D.; Gonçalves, A.; et al. First Clinical Experience with 3-Dimensional Echocardiographic Transillumination Rendering. JACC Cardiovasc. Imaging 2018, 12, 1868–1871. [Google Scholar] [CrossRef]
- Izumo, M.; Okuyama, K.; Akashi, Y. A Novel 3-Dimensional Echocardiographic Transillumination Rendering with Transparency in the Evaluation of Paravalvular Leak After Transcatheter Aortic Valve Implantation. Circ. J. 2021, 85, 317. [Google Scholar] [CrossRef]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A report from the American Society of Echocardiography developed in collaboration with the society for cardiovascular magneticesonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L. Recommendations for the echocardiographic assessment on native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [Green Version]
- Gruner, C.; Herzog, B.; Bettex, D.; Felix, C.; Datta, S.; Greutmann, M.; Gaemperli, O.; Müggler, S.A.; Tanner, F.C.; Gruenenfelder, J.; et al. Quantification of mitral regurgitation by real time three-dimensional color Doppler flow echocardiography pre- and post-percutaneous mitral valve repair. Echocardiography 2015, 32, 1140–1146. [Google Scholar] [CrossRef] [PubMed]
- Silvestry, F.E.; Kerber, R.E.; Brook, M.M.; Carroll, J.D.; Eberman, K.M.; Goldstein, S.A.; Herrmann, H.C.; Homma, S.; Mehran, R.; Packer, D.L.; et al. Echocardiography-guided interventions. J. Am. Soc. Echocardiogr. 2009, 22, 213–231. [Google Scholar] [CrossRef]
- Perk, G.; Lang, R.M.; Garcia-Fernandez, M.A.; Lodato, J.; Sugeng, L.; Lopez, J.; Knight, B.P.; Messika-Zeitoun, D.; Shah, S.; Slater, J.; et al. Use of real time three-dimensional transesophageal echocardiography in intracardiac catheter based interventions. J. Am. Soc. Echocardiogr. 2009, 22, 865–882. [Google Scholar] [CrossRef]
- Pepi, M.; Tamborini, G.; Maltagliati, A.; Galli, C.A.; Sisillo, E.; Salvi, L.; Naliato, M.; Porqueddu, M.; Parolari, A.; Zanobini, M.; et al. Head-to-head comparison of two- and three-dimensional transthoracic and transesophageal echocardiography in the localization of mitral valve prolapse. J. Am. Coll. Cardiol. 2006, 48, 2524–2530. [Google Scholar] [CrossRef] [Green Version]
- Tamborini, G.; Muratori, M.; Maltagliati, A.; Galli, C.A.; Naliato, M.; Zanobini, M.; Alamanni, F.; Salvi, L.; Sisillo, E.; Fiorentini, C.; et al. Pre-operative transthoracic real-time three-dimensional echocardiography in patients undergoing mitral valve repair: Accuracy in cases with simple vs. complex prolapse lesions. Eur. J. Echocardiogr. 2010, 11, 778–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Badano, L.P.; Tsang, W.; Adams, D.H.; Agricola, E.; Buck, T.; Faletra, F.F.; Franke, A.; Hung, J.; Pérez de Isla, L.; et al. American Society of Echocardiography; European Association of Echocardiography. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 1–46. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° of Patients | 30 |
|---|---|
| Age (Years) | 79 ± 8 |
| Males/Females | 14/16 |
| BSA (m2) | 1.7 ± 0.2 |
| Functional MR (N°) | 5 |
| Primary MR (N°) | 25 |
| Procedural details | |
| 1 clip implanted (N° of cases) | 17 |
| NTR | 5 |
| XTR | 12 |
| 2 Clip implanted (N° of cases) | 13 |
| NTR + NTR | 1 |
| NTR + XTR | 4 |
| XTR + XTR | 8 |
| Standard 3DTEE Display | 3DTEE True View | 3DTEE True View with Transparency | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Median | Mean ± SD | Median | Mean ± SD | Median | ||
| Pre-procedural mitral valve anatomy | 3.5 ± 0.6 | 4.0 | 4.0 ± 0.8 * | 4.0 | 4.8 ± 0.5 * † | 5.0 | <0.001 |
| Post-procedural mitral valve anatomy | 3.5 ± 0.6 | 3.5 | 3.8 ± 0.6 * | 4.0 | 4.3 ± 0.5 * † | 4.0 | <0.001 |
| Pre-procedural mitrale regurgitation color jet | 3.6 ± 0.6 | 4.0 | 3.9 ± 0.6 * | 4.0 | 4.3 ± 0.6 * † | 4.0 | <0.001 |
| Post-procedural mitral regurgitation color jet | 3.5 ± 0.6 | 4.0 | 3.8 ± 0.6 * | 4.0 | 4.1 ± 0.7 * † | 4.0 | <0.001 |
| Clip | 3.5 ± 0.7 | 4.0 | 3.8 ± 0.4 * | 4.0 | 4.8 ± 0.4 * † | 5.0 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamborini, G.; Mantegazza, V.; Garlaschè, A.; Muratori, M.; Fusini, L.; Ghulam Ali, S.; Cefalù, C.; Italiano, G.; Gripari, P.; Maltagliati, A.; et al. Head to Head Comparison between Different 3-Dimensional Echocardiographic Rendering Tools in the Imaging of Percutaneous Edge-to-Edge Mitral Valve Repair. J. Cardiovasc. Dev. Dis. 2021, 8, 73. https://doi.org/10.3390/jcdd8070073
Tamborini G, Mantegazza V, Garlaschè A, Muratori M, Fusini L, Ghulam Ali S, Cefalù C, Italiano G, Gripari P, Maltagliati A, et al. Head to Head Comparison between Different 3-Dimensional Echocardiographic Rendering Tools in the Imaging of Percutaneous Edge-to-Edge Mitral Valve Repair. Journal of Cardiovascular Development and Disease. 2021; 8(7):73. https://doi.org/10.3390/jcdd8070073
Chicago/Turabian StyleTamborini, Gloria, Valentina Mantegazza, Anna Garlaschè, Manuela Muratori, Laura Fusini, Sarah Ghulam Ali, Claudia Cefalù, Gianpiero Italiano, Paola Gripari, Anna Maltagliati, and et al. 2021. "Head to Head Comparison between Different 3-Dimensional Echocardiographic Rendering Tools in the Imaging of Percutaneous Edge-to-Edge Mitral Valve Repair" Journal of Cardiovascular Development and Disease 8, no. 7: 73. https://doi.org/10.3390/jcdd8070073
APA StyleTamborini, G., Mantegazza, V., Garlaschè, A., Muratori, M., Fusini, L., Ghulam Ali, S., Cefalù, C., Italiano, G., Gripari, P., Maltagliati, A., Penso, M., & Pepi, M. (2021). Head to Head Comparison between Different 3-Dimensional Echocardiographic Rendering Tools in the Imaging of Percutaneous Edge-to-Edge Mitral Valve Repair. Journal of Cardiovascular Development and Disease, 8(7), 73. https://doi.org/10.3390/jcdd8070073