
A History of Heart Failure Is an Independent Risk Factor for Death in Patients Admitted with Coronavirus 19 Disease

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Disclosure for Data Sharing
2.2. Patient Selection
2.3. Data Collection, Exposure, and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Demographics and Comorbilities
3.2. Patient Characteristics at Presentation
3.3. Therapies in House
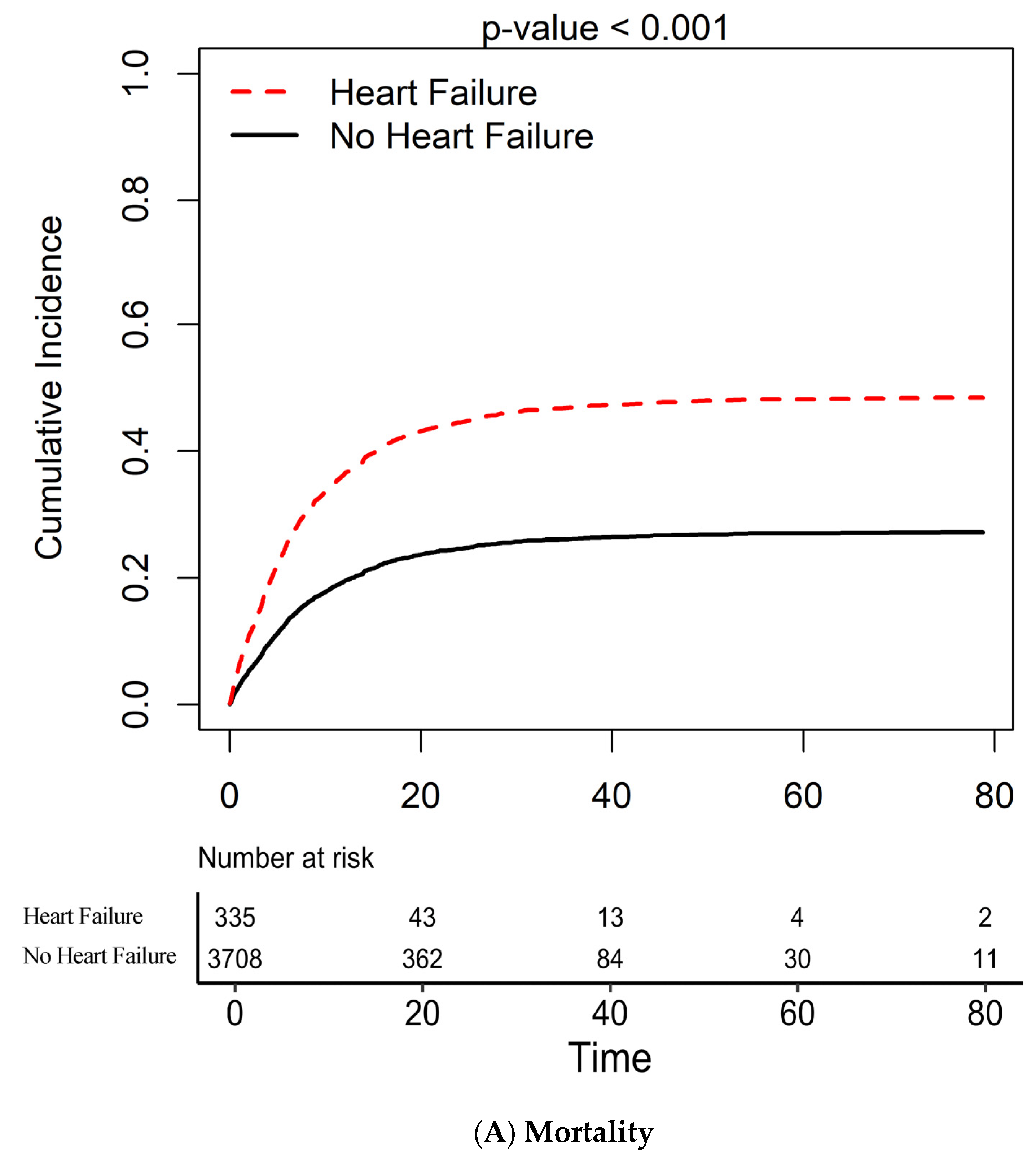
3.4. In-House Mortality and HF
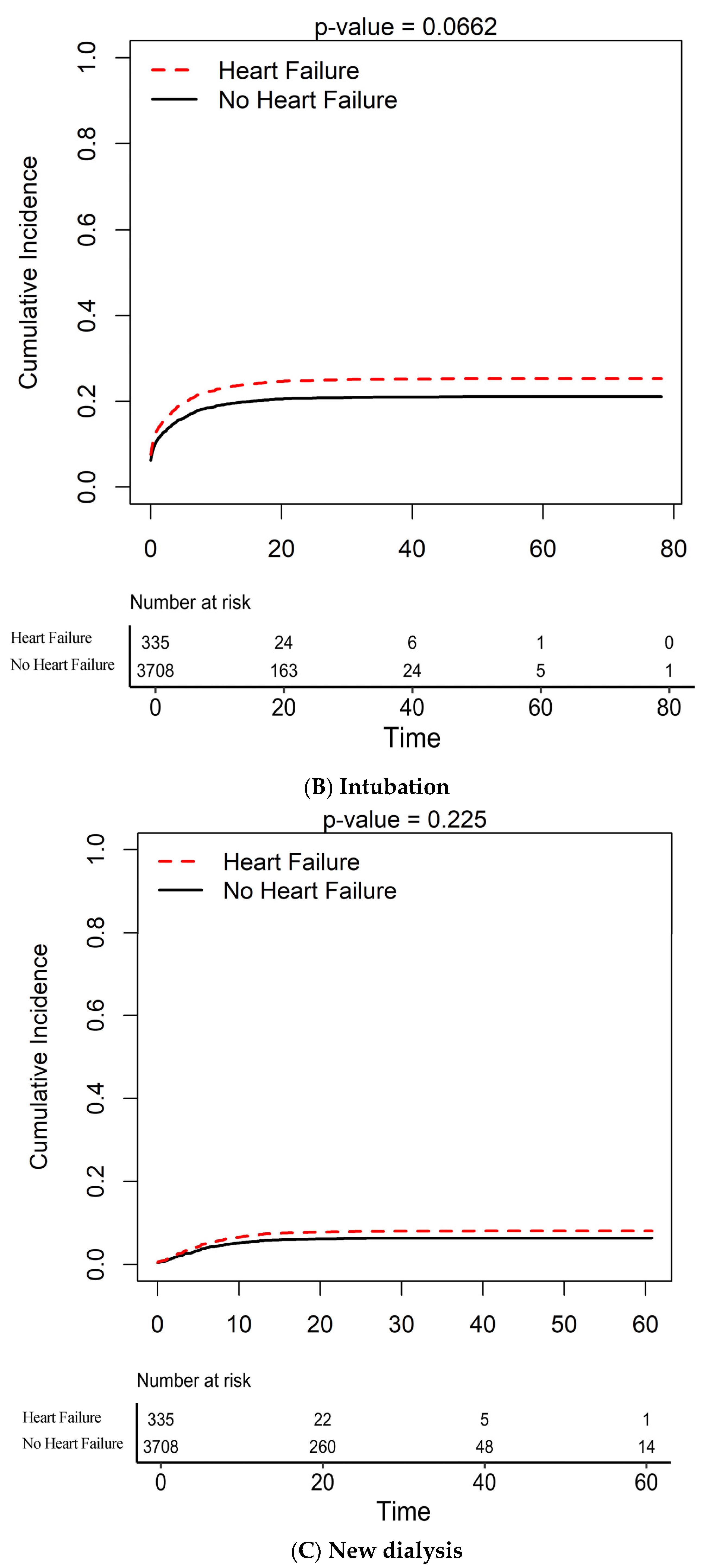
3.5. Need for Intubation and HF
3.6. Need for New Dialysis and HF
4. Discussion
4.1. Baseline and Clinical Presentation
4.2. In-House Mortality
4.3. Intubation, New Hemodialysis, and HF
4.4. HFpEF vs. HFrEF
4.5. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- John Hopkins University. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 15 October 2020).
- Kim, L.; Garg, S.; O’Halloran, A.; Whitaker, M.; Pham, H.; Anderson, E.J.; Armistead, I.; Bennett, N.M.; Billing, L.; Como-Sabetti, K.; et al. Risk Factors for Intensive Care Unit Admission and In-hospital Mortality Among Hospitalized Adults Identified through the US Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET). Clin. Infect. Dis. 2021, 72, e206–e214. [Google Scholar] [CrossRef] [PubMed]
- Mikami, T.; Miyashita, H.; Yamada, T.; Harrington, M.; Steinberg, D.; Dunn, A.; Siau, E. Risk Factors for Mortality in Patients with COVID-19 in New York City. J. Gen. Intern. Med. 2020, 36, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ (Clin. Res.) 2020, 369, m1966. [Google Scholar] [CrossRef]
- Baker, K.F.; Hanrath, A.T.; Schim van der Loeff, I.; Tee, S.A.; Capstick, R.; Marchitelli, G.; Li, A.; Barr, A.; Eid, A.; Ahmed, S.; et al. COVID-19 management in a UK NHS Foundation Trust with a High Consequence Infectious Diseases centre: A detailed descriptive analysis. Med. Sci. 2021, 9, 6. [Google Scholar]
- Gray, R.J. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann. Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Satagopan, J.M.; Ben-Porat, L.; Berwick, M.; Robson, M.; Kutler, D.; Auerbach, A.D. A note on competing risks in survival data analysis. Br. J. Cancer 2004, 91, 1229–1235. [Google Scholar] [CrossRef] [Green Version]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Hendren, N.S.; Lemos, J.A.D.; Ayers, C.; Das, S.R.; Rao, A.; Carter, S.; Rosenblatt, A.; Walchok, J.G.; Omar, W.; Khera, R.; et al. Association of Body Mass Index and Age With Morbidity and Mortality in Patients Hospitalized With COVID-19: Results From the American Heart Association COVID-19 Cardiovascular Disease Registry. Circulation 2021, 143, 135–144. [Google Scholar] [CrossRef]
- Ebinger, J.E.; Achamallah, N.; Ji, H.; Claggett, B.L.; Sun, N.; Botting, P.; Nguyen, T.T.; Luong, E.; Kim, E.H.; Park, E.; et al. Pre-existing traits associated with Covid-19 illness severity. PLoS ONE 2020, 15, e0236240. [Google Scholar] [CrossRef]
- Ji, W.; Huh, K.; Kang, M.; Hong, J.; Bae, G.H.; Lee, R.; Na, Y.; Choi, H.; Gong, S.Y.; Choi, Y.H.; et al. Effect of Underlying Comorbidities on the Infection and Severity of COVID-19 in Korea: A Nationwide Case-Control Study. J. Korean Med. Sci. 2020, 35, e237. [Google Scholar] [CrossRef]
- Giorgi Rossi, P.; Marin, M.; Formisano, D.; Venturelli, F.; Vicentini, M.; Grilli, R.; Reggio Emilia, C.-W.G. Characteristics and outcomes of a cohort of COVID-19 patients in the Province of Reggio Emilia, Italy. PLoS ONE 2020, 15, e0238281. [Google Scholar] [CrossRef] [PubMed]
- Reilev, M.; Kristensen, K.B.; Pottegård, A.; Lund, L.C.; Hallas, J.; Ernst, M.T.; Christiansen, C.F.; Sørensen, H.T.; Johansen, N.B.; Brun, N.C.; et al. Characteristics and predictors of hospitalization and death in the first 11,122 cases with a positive RT-PCR test for SARS-CoV-2 in Denmark: A nationwide cohort. Int. J. Epidemiol. 2020, 49, 1468–1481. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, B.M.; Aggarwal, G.; Wong, J.; Benoit, S.; Vikse, J.; Plebani, M.; Lippi, G. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am. J. Emerg. Med. 2020, 38, 1722–1726. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Without Heart Failure | With Heart Failure | p | |
|---|---|---|---|
| n = 3708 | n = 335 | ||
| Demographics | |||
| Age, year | 65 (54–76) | 73 (65–82) | <0.001 |
| Male gender, no (%) | 1925/3708 (51.9) | 190/335 (56.7) | 0.092 |
| BMI (kg/m2) | 28.8 (24.9–33.3) | 27.9 (24.1–32.9) | 0.063 |
| Past Medical History | |||
| Diabetes, no (%) | 1827/3708 (49.3) | 247/335 (73.7) | <0.001 |
| Hypertension, no (%) | 2577/3708 (69.5) | 308/335 (91.9) | <0.001 |
| CAD, no (%) | 723/3708 (19.5) | 249/335 (74.3) | <0.001 |
| Asthma/COPD, no (%) | 939/3708 (25.3) | 176/335 (52.5) | <0.001 |
| Presentation | |||
| Symptom duration, days | 3 (0–7) | 2 (0–7) | 0.265 |
| Temperature, F | 98.9 (98.2–100.1) | 98.7 (97.9–99.9) | 0.002 |
| Systolic BP, mmHg | 130 (114–147) | 130.5 (113–147) | 0.737 |
| Diastolic BP, mmHg | 75 (65–84) | 73 (60–82) | 0.001 |
| HR, bpm | 99 (87–113) | 92 (78–106) | <0.001 |
| Pulse oximeter saturation, % | 95 (90–98) | 95 (91–98) | 0.047 |
| Respiratory rate, bpm | 20 (18–22) | 20 (18–24) | 0.274 |
| WBC count, k/µL | 7.6 (5.6–10.5) | 7.4 (5.3–10.4) | 0.293 |
| Lymphocytes count, k/µL | 1 (0.7–1.4) | 1 (0.7–1.4) | 0.123 |
| Hemoglobin, g/dL | 13 (11.6–14.3) | 11.9 (10.2–13.6) | <0.001 |
| Platelet count, k/µL | 190 (119–259) | 169.5 (112.3–242.8) | 0.049 |
| Sodium, mEq/L | 137 (134–141) | 137 (134–142) | 0.762 |
| Potassium, mEq/L | 4.3 (3.9–4.7) | 4.6 (4.1–5) | <0.001 |
| Chloride, mEq/L | 99 (95–103) | 99 (95–103) | 0.455 |
| Bicarbonate, mEq/L | 25 (22–27) | 25 (21–28) | 0.07 |
| EGFR, mL/min/BSA | 66 (40.5–89) | 40.7 (22.8–59.2) | <0.001 |
| AST, U/L | 42 (28–67) | 36 (25–57) | 0.001 |
| ALT, U/L | 28 (18–46) | 22 (14–36) | <0.001 |
| Lactic acid, mmol/L | 2.1 (1.6–3) | 2.3 (1.6–3.2) | 0.161 |
| Creatinine Kinase, U/L | 182 (90–451) | 151 (76–342) | 0.008 |
| ProBNP, pg/mL | 306 (90–1096) | 2727 (1068–9108) | <0.001 |
| D-dimer, µg/mL | 1.7 (0.9–4) | 2.5 (1.1–5.4) | 0.024 |
| C-reactive protein, µg/mL | 10.6 (4.4–18.4) | 10 (4.1–21.8) | 0.759 |
| LDH, U/L | 401 (294–549) | 392 (284–562) | 0.846 |
| Ferritin, ng/mL | 739 (357–1472) | 615 (323–1155) | 0.065 |
| IL6, pg/mL | 33.2 (14.5–74.9) | 41.1 (18.9–102.8) | 0.06 |
| Procalcitonin, ng/mL | 0.2 (0.1–0.7) | 0.3 (0.1–1) | 0.024 |
| Troponin T, ng/mL | 0.01 (0.01–0.02) | 0.03 (0.01–0.07) | <0.001 |
| Treatments during admission | |||
| Beta Blocker | 920/3708 (24.8) | 205/335 (61.2) | <0.001 |
| ACE-I | 259/3708 (7.0) | 41/335 (12.5) | <0.001 |
| ARBs | 230/3708 (6.2) | 22/335 (6.6) | 0.792 |
| Pressors, no (%) | 707/3708 (19.1) | 74/335 (22.1) | 0.180 |
| Inotropes, no (%) | 28/3708 (0.8) | 14/335 (4.2) | <0.001 |
| Hydroxychloroquine, no (%) | 2645/3708 (71.3) | 203/335 (60.6) | <0.001 |
| Chloroquine, no (%) | 58/3708 (1.6) | 6/335 (1.8) | 0.75 |
| Azithromycin, no (%) | 1205/3708 (32.5) | 84/335 (25.1) | 0.005 |
| Other antibiotics, no (%) | 2815/3708 (75.9) | 262/335 (78.2) | 0.346 |
| IV steroids, no (%) | 819/3708 (22.1) | 78/335 (23.3) | 0.614 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castagna, F.; Kataria, R.; Madan, S.; Ali, S.Z.; Diab, K.; Leyton, C.; Arfaras-Melainis, A.; Kim, P.; Giorgi, F.M.; Vukelic, S.; et al. A History of Heart Failure Is an Independent Risk Factor for Death in Patients Admitted with Coronavirus 19 Disease. J. Cardiovasc. Dev. Dis. 2021, 8, 77. https://doi.org/10.3390/jcdd8070077
Castagna F, Kataria R, Madan S, Ali SZ, Diab K, Leyton C, Arfaras-Melainis A, Kim P, Giorgi FM, Vukelic S, et al. A History of Heart Failure Is an Independent Risk Factor for Death in Patients Admitted with Coronavirus 19 Disease. Journal of Cardiovascular Development and Disease. 2021; 8(7):77. https://doi.org/10.3390/jcdd8070077
Chicago/Turabian StyleCastagna, Francesco, Rachna Kataria, Shivank Madan, Syed Zain Ali, Karim Diab, Christopher Leyton, Angelos Arfaras-Melainis, Paul Kim, Federico M. Giorgi, Sasa Vukelic, and et al. 2021. "A History of Heart Failure Is an Independent Risk Factor for Death in Patients Admitted with Coronavirus 19 Disease" Journal of Cardiovascular Development and Disease 8, no. 7: 77. https://doi.org/10.3390/jcdd8070077
APA StyleCastagna, F., Kataria, R., Madan, S., Ali, S. Z., Diab, K., Leyton, C., Arfaras-Melainis, A., Kim, P., Giorgi, F. M., Vukelic, S., Saeed, O., Patel, S. R., Sims, D. B., & Jorde, U. P. (2021). A History of Heart Failure Is an Independent Risk Factor for Death in Patients Admitted with Coronavirus 19 Disease. Journal of Cardiovascular Development and Disease, 8(7), 77. https://doi.org/10.3390/jcdd8070077