Effects of Statins on Renin–Angiotensin System


 and
and 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
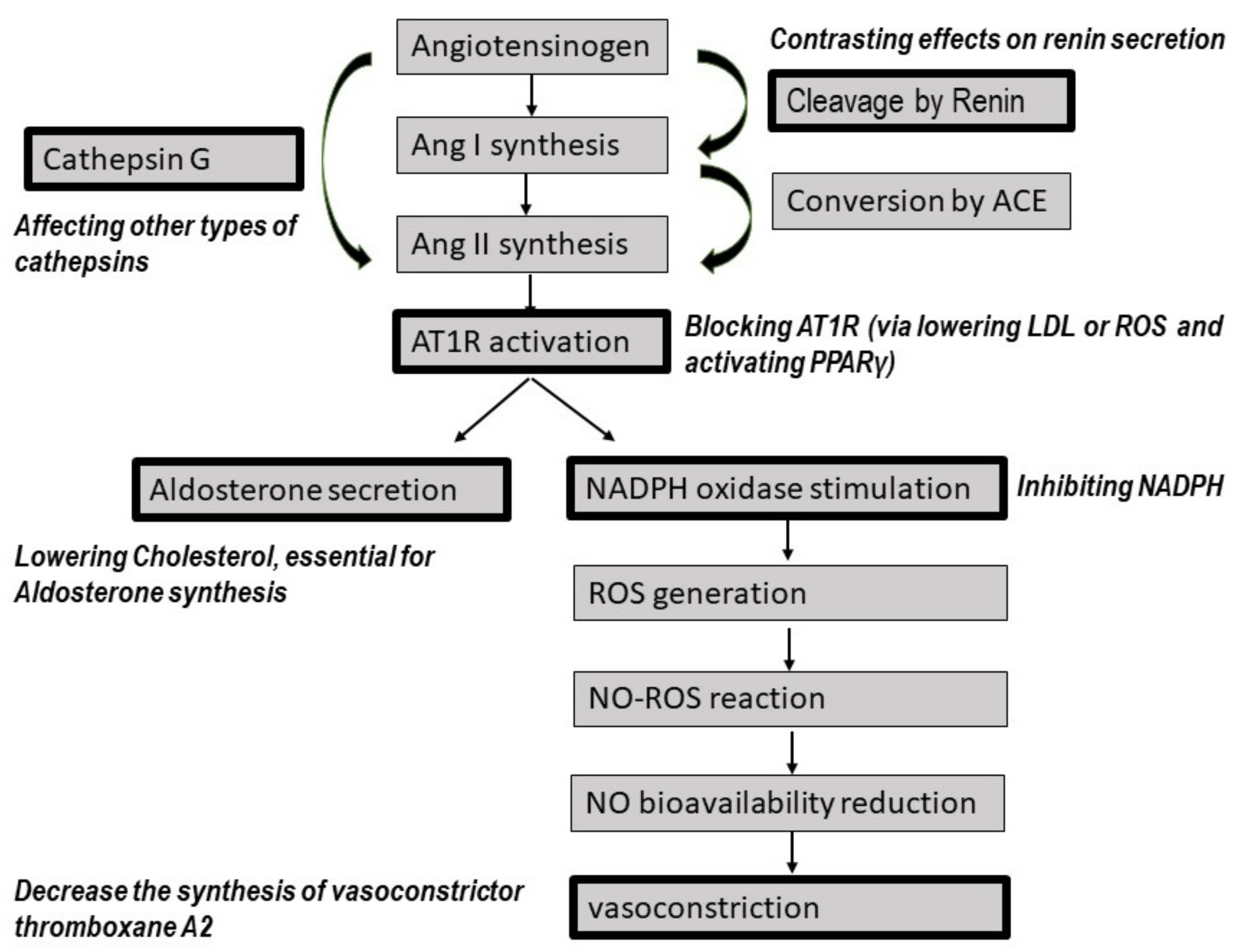
2. Effect of Statins on RAS Pathways
2.1. The Effect of Statins on Renin Secretion
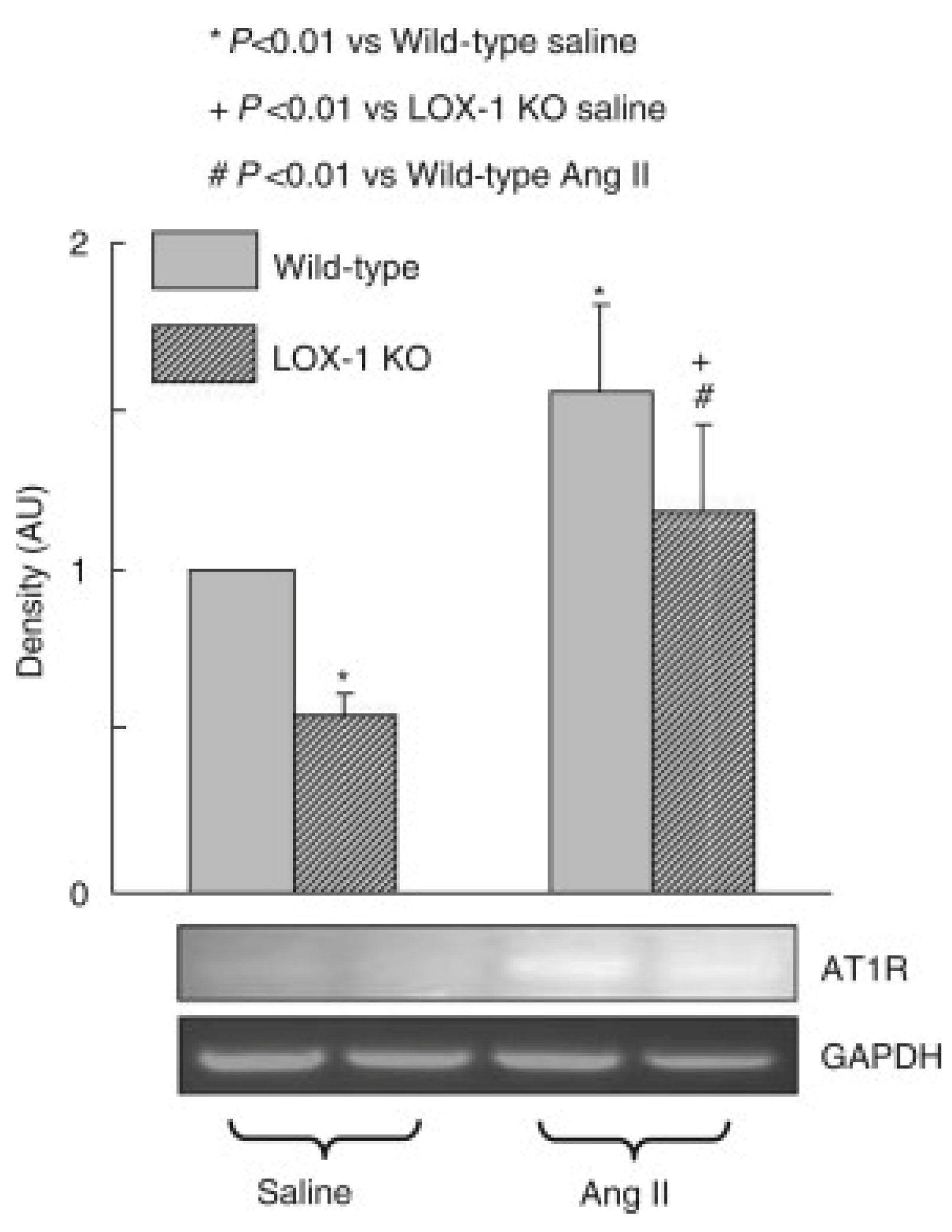
2.2. The Effect of Statins on AT1R Expression and Activation
2.3. The Effect of Statins on AT2R and MasR Activation
2.4. The Effect of Statins on Aldosterone Secretion
2.5. The Effect of Statins on Vasoconstriction
2.6. The Effect of Statins on Sympathetic Activation
3. RAS-Mediated Effects of Statins on COVID-19 Treatment
4. Potential Roles of Statins on Other RAS Elements
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsukamoto, I.; Inoue, S.; Teramura, T.; Takehara, T.; Ohtani, K.; Akagi, M. Activating types 1 and 2 angiotensin II receptors modulate the hypertrophic differentiation of chondrocytes. FEBS Open Bio 2013, 3, 279–284. [Google Scholar] [CrossRef] [Green Version]
- Nickenig, G. Should angiotensin II receptor blockers and statins be combined? Circulation 2004, 110, 1013–1020. [Google Scholar] [CrossRef] [Green Version]
- Spindler, S.R.; Mote, P.L.; Flegal, J.M. Combined statin and angiotensin-converting enzyme (ACE) inhibitor treatment increases the lifespan of long-lived F1 male mice. Age 2016, 38, 379–391. [Google Scholar] [CrossRef] [Green Version]
- Rykl, J.; Thiemann, J.; Kurzawski, S.; Pohl, T.; Gobom, J.; Zidek, W.; Schlüter, H. Renal cathepsin G and angiotensin II generation. J. Hypertens. 2006, 24, 1797–1807. [Google Scholar] [CrossRef]
- Sampaio, W.O.; Souza dos Santos, R.A.; Faria-Silva, R.; da Mata Machado, L.T.; Schiffrin, E.L.; Touyz, R.M. Angiotensin-(1-7) through receptor Mas mediates endothelial nitric oxide synthase activation via Akt-dependent pathways. Hypertension 2007, 49, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Santos, R.A. Angiotensin-(1–7). Hypertension 2014, 63, 1138–1147. [Google Scholar] [CrossRef]
- Deo, S.H.; Fisher, J.P.; Vianna, L.C.; Kim, A.; Chockalingam, A.; Zimmerman, M.C.; Zucker, I.H.; Fadel, P.J. Statin therapy lowers muscle sympathetic nerve activity and oxidative stress in patients with heart failure. Am. J. Physiol. Heart Circ. Physiol. 2012, 303, H377–H385. [Google Scholar] [CrossRef] [Green Version]
- Lewandowski, J.; Siński, M.; Bidiuk, J.; Abramczyk, P.; Dobosiewicz, A.; Ciarka, A.; Gaciong, Z. Simvastatin reduces sympathetic activity in men with hypertension and hypercholesterolemia. Hypertens. Res. 2010, 33, 1038–1043. [Google Scholar] [CrossRef]
- Montezano, A.C.; Cat, A.N.D.; Rios, F.J.; Touyz, R.M. Angiotensin II and vascular injury. Curr. Hypertens. Rep. 2014, 16, 431. [Google Scholar] [CrossRef]
- Silva, G.M.; França-Falcão, M.S.; Calzerra, N.T.M.; Luz, M.S.; Gadelha, D.D.A.; Balarini, C.M.; Queiroz, T.M. Role of Renin-Angiotensin System Components in Atherosclerosis: Focus on Ang-II, ACE2, and Ang-1–7. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef]
- Pignone, A.; Del Rosso, A.; Brosnihan, K.B.; Perfetto, F.; Livi, R.; Fiori, G.; Guiducci, S.; Cinelli, M.; Rogai, V.; Tempestini, A. Reduced circulating levels of angiotensin-(1–7) in systemic sclerosis: A new pathway in the dysregulation of endothelial-dependent vascular tone control. Ann. Rheum. Dis. 2007, 66, 1305–1310. [Google Scholar] [CrossRef] [Green Version]
- Vian, J.; Pereira, C.; Chavarria, V.; Köhler, C.; Stubbs, B.; Quevedo, J.; Kim, S.-W.; Carvalho, A.F.; Berk, M.; Fernandes, B.S. The renin–angiotensin system: A possible new target for depression. BMC Med. 2017, 15, 144. [Google Scholar] [CrossRef]
- Oliveros, E.; Oni, E.T.; Shahzad, A.; Kluger, A.Y.; Lo, K.B.; Rangaswami, J.; McCullough, P.A. Benefits and Risks of Continuing Angiotensin-Converting Enzyme Inhibitors, Angiotensin II Receptor Antagonists, and Mineralocorticoid Receptor Antagonists during Hospitalizations for Acute Heart Failure. Cardiorenal Med. 2020, 10, 69–84. [Google Scholar] [CrossRef]
- Ma, T.K.W.; Kam, K.K.H.; Yan, B.P.; Lam, Y.-Y. Renin-angiotensin-aldosterone system blockade for cardiovascular diseases: Current status. Br. J. Pharmacol. 2010, 160, 1273–1292. [Google Scholar] [CrossRef]
- Momtazi-Borojeni, A.A.; Banach, M.; Reiner, Ž.; Pirro, M.; Bianconi, V.; Al-Rasadi, K.; Sahebkar, A. Interaction Between Coronavirus S-Protein and Human ACE2: Hints for Exploring Efficient Therapeutic Targets to Treat COVID-19. Angiology 2021, 72, 122–130. [Google Scholar] [CrossRef]
- Melissa Hallow, K.; Dave, I. RAAS Blockade and COVID-19: Mechanistic Modeling of Mas and AT1 Receptor Occupancy as Indicators of Pro-Inflammatory and Anti-Inflammatory Balance. Clin. Pharmacol. Ther. 2021, 109, 1092–1103. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Yu, X.; Zhang, B.; Zhang, H.; Fang, Y.; Liu, S.; Liu, T.; Ding, X. Atorvastatin improves survival of implanted stem cells in a rat model of renal ischemia-reperfusion injury. Am. J. Nephrol. 2014, 39, 466–475. [Google Scholar] [CrossRef]
- Aktas, O.; Albrecht, P.; Hartung, H.P. Optic neuritis as a phase 2 paradigm for neuroprotection therapies of multiple sclerosis: Update on current trials and perspectives. Curr. Opin. Neurol. 2016, 29, 199–204. [Google Scholar] [CrossRef]
- Reiner, Ž. Statins in the primary prevention of cardiovascular disease. Nat. Rev. Cardiol. 2013, 10, 453. [Google Scholar] [CrossRef]
- Afshari, A.R.; Mollazadeh, H.; Henney, N.C.; Jamialahmad, T.; Sahebkar, A. Effects of statins on brain tumors: A review. Semin. Cancer Biol. 2021, 73, 116–133. [Google Scholar] [CrossRef]
- Bahrami, A.; Bo, S.; Jamialahmadi, T.; Sahebkar, A. Effects of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors on ageing: Molecular mechanisms. Ageing Res. Rev. 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Gorabi, A.M.; Kiaie, N.; Pirro, M.; Bianconi, V.; Jamialahmadi, T.; Sahebkar, A. Effects of statins on the biological features of mesenchymal stem cells and therapeutic implications. Heart Fail. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mollazadeh, H.; Tavana, E.; Fanni, G.; Bo, S.; Banach, M.; Pirro, M.; von Haehling, S.; Jamialahmadi, T.; Sahebkar, A. Effects of statins on mitochondrial pathways. J. Cachexia Sarcopenia Muscle 2021, 12, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Reiner, Ž.; Hatamipour, M.; Banach, M.; Pirro, M.; Al-Rasadi, K.; Jamialahmadi, T.; Radenkovic, D.; Montecucco, F.; Sahebkar, A. Statins and the Covid-19 main protease: In silico evidence on direct interaction. Arch. Med. Sci. 2020, 16, 490–496. [Google Scholar] [CrossRef]
- Sahebkar, A.; Serban, C.; Ursoniu, S.; Mikhailidis, D.P.; Undas, A.; Lip, G.Y.H.; Bittner, V.; Ray, K.K.; Watts, G.F.; Kees Hovingh, G.; et al. The impact of statin therapy on plasma levels of von Willebrand factor antigen: Systematic review and meta-analysis of Randomised placebo-controlled trials. Thromb. Haemost. 2016, 115, 520–532. [Google Scholar] [CrossRef]
- Serban, C.; Sahebkar, A.; Ursoniu, S.; Mikhailidis, D.P.; Rizzo, M.; Lip, G.Y.H.; Kees Hovingh, G.; Kastelein, J.J.P.; Kalinowski, L.; Rysz, J.; et al. A systematic review and meta-analysis of the effect of statins on plasma asymmetric dimethylarginine concentrations. Sci. Rep. 2015, 5. [Google Scholar] [CrossRef] [Green Version]
- Istvan, E.S.; Deisenhofer, J. Structural mechanism for statin inhibition of HMG-CoA reductase. Science 2001, 292, 1160. [Google Scholar] [CrossRef] [Green Version]
- Ruszkowski, P.; Masajtis-Zagajewska, A.; Nowicki, M. Effects of combined statin and ACE inhibitor therapy on endothelial function and blood pressure in essential hypertension—A randomised double-blind, placebo controlled crossover study. J. Renin Angiotensin Aldosterone Syst. JRAAS 2019, 20, 1470320319868890. [Google Scholar] [CrossRef] [Green Version]
- Kurtz, A. Control of Renin Synthesis and Secretion. Am. J. Hypertens. 2012, 25, 839–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herring, N.; Tapoulal, N.; Kalla, M.; Ye, X.; Borysova, L.; Lee, R.; Dall’Armellina, E.; Stanley, C.; Ascione, R.; Lu, C.-J.; et al. Neuropeptide-Y causes coronary microvascular constriction and is associated with reduced ejection fraction following ST-elevation myocardial infarction. Eur. Heart J. 2019, 40, 1920–1929. [Google Scholar] [CrossRef]
- Levine, L. Statins stimulate arachidonic acid release and prostaglandin I. Lipids Health Dis. 2003, 2, 1. [Google Scholar] [CrossRef]
- Hazra, S.; Lee, G.; Grant, J.; Walser, T.; Prasad, S.; Larsen, J.E.; Minna, J.; Dubinett, S.M. Abstract B57: Modulation of prostaglandin E2 by statins in human bronchial epithelial cells harboring K-ras mutation: The potential advantage of combination therapy. Cancer Prev. Res. 2010, 3, B57. [Google Scholar] [CrossRef]
- Mouawad, C.A.; Mrad, M.F.; El-Achkar, G.A.; Abdul-Sater, A.; Nemer, G.M.; Creminon, C.; Lotersztajn, S.; Habib, A. Statins Modulate Cyclooxygenase-2 and Microsomal Prostaglandin E Synthase-1 in Human Hepatic Myofibroblasts. J. Cell. Biochem. 2016, 117, 1176–1186. [Google Scholar] [CrossRef]
- Yano, M.; Matsumura, T.; Senokuchi, T.; Ishii, N.; Murata, Y.; Taketa, K.; Motoshima, H.; Taguchi, T.; Sonoda, K.; Kukidome, D.; et al. Statins Activate Peroxisome Proliferator-Activated Receptor γ Through Extracellular Signal-Regulated Kinase 1/2 and p38 Mitogen-Activated Protein Kinase–Dependent Cyclooxygenase-2 Expression in Macrophages. Circ. Res. 2007, 100, 1442–1451. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Li, L.-B.; Zhang, J.; Tang, D.-P.; Wei, J.-J.; Zhuang, Z.-H. Simvastatin, but not pravastatin, inhibits the proliferation of esophageal adenocarcinoma and squamous cell carcinoma cells: A cell-molecular study. Lipids Health Dis. 2018, 17, 290. [Google Scholar] [CrossRef] [Green Version]
- Nassar, P.O.; Nassar, C.A.; Guimarães, M.R.; Aquino, S.G.; Andia, D.C.; Muscara, M.N.; Spolidorio, D.M.P.; Rossa, C., Jr.; Spolidorio, L.C. Simvastatin therapy in cyclosporine A-induced alveolar bone loss in rats. J. Periodontal Res. 2009, 44, 479–488. [Google Scholar] [CrossRef]
- Araújo, R.F.d.J.; Souza, T.O.; Moura, L.M.d.; Torres, K.P.; Souza, L.B.d.; Alves, M.d.S.C.F.; Rocha, H.O.; de Araújo, A.A. Atorvastatin Decreases Bone Loss, Inflammation and Oxidative Stress in Experimental Periodontitis. PLoS ONE 2013, 8, e75322. [Google Scholar] [CrossRef]
- Grunwald, S.A.; Popp, O.; Haafke, S.; Jedraszczak, N.; Grieben, U.; Saar, K.; Patone, G.; Kress, W.; Steinhagen-Thiessen, E.; Dittmar, G.; et al. Statin-induced myopathic changes in primary human muscle cells and reversal by a prostaglandin F2 alpha analogue. Sci. Rep. 2020, 10, 2158. [Google Scholar] [CrossRef] [Green Version]
- Koh, Y.Y.; Lim, D.Y. Os 31-08 inhibitory effects of simvastatin on catecholamine secretion from the adrenal medulla. J. Hypertens. 2016, 34, e389. [Google Scholar] [CrossRef]
- Matsuda, T.; Toyohira, Y.; Ueno, S.; Tsutsui, M.; Yanagihara, N. Simvastatin Inhibits Catecholamine Secretion and Synthesis Induced by Acetylcholine via Blocking Na+ and Ca2+ Influx in Bovine Adrenal Medullary Cells. J. Pharmacol. Exp. Ther. 2008, 327, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Koh, Y.K.; Kim, K.H.; Choi, M.S.; Koh, Y.Y.; Lim, D.Y. Simvastatin reduces adrenal catecholamine secretion evoked by stimulation of cholinergic nicotinic and angiotensinergic AT(1) receptors. Arch. Pharm. Res. 2018, 41, 333–346. [Google Scholar] [CrossRef]
- Bucelli, R.C.; Gonsiorek, E.A.; Kim, W.-Y.; Bruun, D.; Rabin, R.A.; Higgins, D.; Lein, P.J. Statins Decrease Expression of the Proinflammatory Neuropeptides Calcitonin Gene-Related Peptide and Substance P in Sensory Neurons. J. Pharmacol. Exp. Ther. 2008, 324, 1172–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garmaroudi, F.S.; Handy, D.E.; Liu, Y.-Y.; Loscalzo, J. Systems Pharmacology and Rational Polypharmacy: Nitric Oxide−Cyclic GMP Signaling Pathway as an Illustrative Example and Derivation of the General Case. PLoS Comput. Biol. 2016, 12, e1004822. [Google Scholar] [CrossRef] [Green Version]
- Wagner, C.; Pfeifer, A.; Ruth, P.; Hofmann, F.; Kurtz, A. Role of cGMP-kinase II in the control of renin secretion and renin expression. J. Clin. Investig. 1998, 102, 1576–1582. [Google Scholar] [CrossRef] [Green Version]
- Schramm, A.; Schweda, F.; Sequeira-Lopez, M.L.S.; Hofmann, F.; Sandner, P.; Schlossmann, J. Protein Kinase G Is Involved in Acute but Not in Long-Term Regulation of Renin Secretion. Front. Pharmacol. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- Beierwaltes, W.H. cGMP stimulates renin secretion in vivo by inhibiting phosphodiesterase-3. Am. J. Physiol. Renal Physiol. 2006, 290, F1376–F1381. [Google Scholar] [CrossRef]
- Neubauer, B.; Machura, K.; Kettl, R.; Lopez Maria Luisa, S.S.; Friebe, A.; Kurtz, A. Endothelium-Derived Nitric Oxide Supports Renin Cell Recruitment Through the Nitric Oxide–Sensitive Guanylate Cyclase Pathway. Hypertension 2013, 61, 400–407. [Google Scholar] [CrossRef] [Green Version]
- Gorabi, A.M.K.N.; Hajighasemi, S.; Banach, M.; Penson, P.E.; Jamialahmadi, T.; Sahebkar, A. Statin-Induced Nitric Oxide Signaling: Mechanisms and Therapeutic Implications. J. Clin. Med. 2019, 8, 2051. [Google Scholar] [CrossRef] [Green Version]
- Prickett, T.; Troughton, R.; Espiner, E. Effect of statin therapy on plasma C-type Natriuretic Peptides and Endothelin-1 in males with and without symptomatic coronary artery disease. Sci. Rep. 2020, 10, 7927. [Google Scholar] [CrossRef]
- Abulhul, E.; McDonald, K.; Martos, R.; Phelan, D.; Spiers, J.P.; Hennessy, M.; Baugh, J.; Watson, C.; O'Loughlin, C.; Ledwidge, M. Long-term statin therapy in patients with systolic heart failure and normal cholesterol: Effects on elevated serum markers of collagen turnover, inflammation, and B-type natriuretic peptide. Clin. Ther. 2012, 34, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Shehata, M.; Samir, A.; Dardiri, M. Prognostic impact of intensive statin therapy on N-terminal pro-BNP level in non-ST-segment elevation acute myocardial infarction patients. J. Interv. Cardiol. 2017, 30, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Teshima, Y.; Yufu, K.; Akioka, H.; Iwao, T.; Anan, F.; Nakagawa, M.; Yonemochi, H.; Takahashi, N.; Hara, M.; Saikawa, T. Early atorvastatin therapy improves cardiac function in patients with acute myocardial infarction. J. Cardiol. 2009, 53, 58–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dirajlal-Fargo, S.; Kinley, B.; Jiang, Y.; Longenecker, C.T.; Hileman, C.O.; Debanne, S.; McComsey, G.A. Statin therapy decreases N-terminal pro-B-type natriuretic peptide in HIV: Randomized placebo-controlled trial. AIDS 2015, 29, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Castejon, A.M.; Zollner, E.; Tristano, A.G.; Cubeddu, L.X. Upregulation of angiotensin II-AT1 receptors during statin withdrawal in vascular smooth muscle cells. J. Cardiovasc. Pharmacol. 2007, 50, 708–711. [Google Scholar] [CrossRef]
- Nickenig, G.; Bäumer, A.T.; Temur, Y.; Kebben, D.; Jockenhövel, F.; Böhm, M. Statin-Sensitive Dysregulated AT1 Receptor Function and Density in Hypercholesterolemic Men. Circulation 1999, 100, 2131–2134. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Iwai, M.; Wu, L.; Liu, H.W.; Chen, R.; Jinno, T.; Suzuki, J.; Tsuda, M.; Gao, X.Y.; Okumura, M.; et al. Fluvastatin enhances the inhibitory effects of a selective AT1 receptor blocker, valsartan, on atherosclerosis. Hypertension 2004, 44, 758–763. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Saldeen, T.; Romeo, F.; Mehta Jawahar, L. Oxidized LDL Upregulates Angiotensin II Type 1 Receptor Expression in Cultured Human Coronary Artery Endothelial Cells. Circulation 2000, 102, 1970–1976. [Google Scholar] [CrossRef]
- Nazzaro, P.; Manzari, M.; Merlo, M.; Triggiani, R.; Scarano, A.; Ciancio, L.; Pirrelli, A. Distinct and Combined Vascular Effects of ACE Blockade and HMG-CoA Reductase Inhibition in Hypertensive Subjects. Hypertension 1999, 33, 719–725. [Google Scholar] [CrossRef] [Green Version]
- Banday, A.A.; Lokhandwala, M.F. Oxidative stress-induced renal angiotensin AT1 receptor upregulation causes increased stimulation of sodium transporters and hypertension. Am. J. Physiol. Renal Physiol. 2008, 295, F698–F706. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.; Kang, B.Y.; Megyesi, J.; Kaushal, G.P.; Safirstein, R.L.; Mehta, J.L. Deletion of LOX-1 attenuates renal injury following angiotensin II infusion. Kidney Int. 2009, 76, 521–527. [Google Scholar] [CrossRef] [Green Version]
- Strehlow, K.; Wassmann, S.; Böhm, M.; Nickenig, G. Angiotensin AT1 receptor over-expression in hypercholesterolaemia. Ann. Med. 2000, 32, 386–389. [Google Scholar] [CrossRef]
- Benson, S.C.; Pershadsingh, H.A.; Ho, C.I.; Chittiboyina, A.; Desai, P.; Pravenec, M.; Qi, N.; Wang, J.; Avery, M.A.; Kurtz, T.W. Identification of telmisartan as a unique angiotensin ii receptor antagonist with selective pparγ–modulating activity. Hypertension 2004, 43, 993–1002. [Google Scholar] [CrossRef] [Green Version]
- Schupp, M.; Janke, J.; Clasen, R.; Unger, T.; Kintscher, U. Angiotensin Type 1 Receptor Blockers Induce Peroxisome Proliferator-Activated Receptor- Activity. Circulation 2004, 109, 2054–2057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiyerili, V.; Becher, U.M.; Camara, B.; Yildirimtürk, C.; Aksoy, A.; Kebschull, M.; Werner, N.; Nickenig, G.; Müller, C. Impact of peroxisome proliferator-activated receptor γ on angiotensin II type 1 receptor-mediated insulin sensitivity, vascular inflammation and atherogenesis in hypercholesterolemic mice. Arch. Med. Sci. AMS 2015, 11, 877–885. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Aguilar, M.; Ibarra-Lara, L.; Mondragón, L.; Rubio-Ruiz, M.; Aguilar-Navarro, A.; Zamorano, A.; Ramírez-Ortega, M.; Hernández, G.; Sánchez-Mendoza, A. Rosiglitazone, a Ligand to PPAR γ, Improves Blood Pressure and Vascular Function through Renin-Angiotensin System Regulation. PPAR Res. 2019, 2019, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Grip, O.; Janciauskiene, S.; Lindgren, S. Atorvastatin activates PPAR-γ and attenuates the inflammatory response in human monocytes. Inflamm. Res. 2002, 51, 58–62. [Google Scholar] [CrossRef]
- Seo, M.; Inoue, I.; Ikeda, M.; Nakano, T.; Takahashi, S.; Katayama, S.; Komoda, T. Statins Activate Human PPARalpha Promoter and Increase PPARalpha mRNA Expression and Activation in HepG2 Cells. PPAR Res. 2008, 2008, 316306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, Y.-W.; Ye, P.; He, J.-Q.; Sheng, L.; Wang, L.-Y.; Du, J. Simvastatin inhibited cardiac hypertrophy and fibrosis in apolipoprotein E-deficient mice fed a “Western-style diet” by increasing PPAR α and γ expression and reducing TC, MMP-9, and Cat S levels. Acta Pharmacol. Sin. 2010, 31, 1350–1358. [Google Scholar] [CrossRef] [PubMed]
- Balakumar, P.; Mahadevan, N. Interplay between statins and PPARs in improving cardiovascular outcomes: A double-edged sword? Br. J. Pharmacol. 2012, 165, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Jana, M.; Kundu, M.; Corbett, G.T.; Rangaswamy, S.B.; Mishra, R.K.; Luan, C.H.; Gonzalez, F.J.; Pahan, K. HMG-CoA Reductase Inhibitors Bind to PPARα to Upregulate Neurotrophin Expression in the Brain and Improve Memory in Mice. Cell Metab. 2015, 22, 253–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, K.D.; Unal, H.; Desnoyer, R.; Karnik, S.S. Mechanism of Hormone Peptide Activation of a GPCR: Angiotensin II Activated State of AT1R Initiated by van der Waals Attraction. J. Chem. Inf. Modeling 2019, 59, 373–385. [Google Scholar] [CrossRef]
- Wingler, L.M.; McMahon, C.; Staus, D.P.; Lefkowitz, R.J.; Kruse, A.C. Distinctive Activation Mechanism for Angiotensin Receptor Revealed by a Synthetic Nanobody. Cell 2019, 176, 479–490.e412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, Y.; Akazawa, H.; Qin, Y.; Sano, M.; Takano, H.; Minamino, T.; Makita, N.; Iwanaga, K.; Zhu, W.; Kudoh, S. Mechanical stress activates angiotensin II type 1 receptor without the involvement of angiotensin II. Nat. Cell Biol. 2004, 6, 499–506. [Google Scholar] [CrossRef]
- Barauna, V.G.; Magalhaes, F.C.; Campos, L.C.; Reis, R.I.; Kunapuli, S.P.; Costa-Neto, C.M.; Miyakawa, A.A.; Krieger, J.E. Shear stress-induced Ang II AT1 receptor activation: G-protein dependent and independent mechanisms. Biochem. Biophys. Res. Commun. 2013, 434, 647–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, A.K.; Gao, L.; Zucker, I.H. Angiotensin II-induced upregulation of AT(1) receptor expression: Sequential activation of NF-kappaB and Elk-1 in neurons. Am. J. Physiol. Cell Physiol. 2010, 299, C561–C569. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-P.; Huang, P.-H.; Lai, C.F.; Chen, J.-W.; Lin, S.-J.; Chen, J.-S. Simvastatin Attenuates Oxidative Stress, NF-κB Activation, and Artery Calcification in LDLR-/- Mice Fed with High Fat Diet via Down-regulation of Tumor Necrosis Factor-α and TNF Receptor 1. PLoS ONE 2015, 10, e0143686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilgendorff, A.; Muth, H.; Parviz, B.; Staubitz, A.; Haberbosch, W.; Tillmanns, H.; Hölschermann, H. Statins differ in their ability to block NF-kappaB activation in human blood monocytes. Int. J. Clin. Pharmacol. Ther. 2003, 41, 397–401. [Google Scholar] [CrossRef]
- Banach-Orłowska, M.; Wyszyńska, R.; Pyrzyńska, B.; Maksymowicz, M.; Gołąb, J.; Miączyńska, M. Cholesterol restricts lymphotoxin β receptor-triggered NF-κB signaling. Cell Commun. Signal. 2019, 17, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Li, Z.; Cao, K.; Fang, D.; Wang, F.; Bi, G.; Yang, J.; He, Y.; Wu, J.; Wei, Y.; et al. Adjunctive therapy with statins reduces residual albuminuria/proteinuria and provides further renoprotection by downregulating the angiotensin II-AT1 pathway in hypertensive nephropathy. J. Hypertens. 2017, 35, 1442–1456. [Google Scholar] [CrossRef]
- Marino, F.; Guasti, L.; Cosentino, M.; Rasini, E.; Ferrari, M.; Maio, R.C.; Loraschi, A.; Cimpanelli, M.G.; Schembri, L.; Legnaro, M.; et al. Simvastatin treatment in subjects at high cardiovascular risk modulates AT1R expression on circulating monocytes and T lymphocytes. J. Hypertens. 2008, 26, 1147–1155. [Google Scholar] [CrossRef]
- Bai, H.Y.; Mogi, M.; Nakaoka, H.; Kan-No, H.; Tsukuda, K.; Wang, X.L.; Shan, B.S.; Kukida, M.; Yamauchi, T.; Higaki, A.; et al. Synergistic Inhibitory Effect of Rosuvastatin and Angiotensin II Type 2 Receptor Agonist on Vascular Remodeling. J. Pharmacol. Exp. Ther. 2016, 358, 352–358. [Google Scholar] [CrossRef]
- Suski, M.; Gębska, A.; Olszanecki, R.; Stachowicz, A.; Uracz, D.; Madej, J.; Korbut, R. Influence of atorvastatin on angiotensin I metabolism in resting and TNF-α-activated rat vascular smooth muscle cells. J. Renin Angiotensin Aldosterone Syst. 2014, 15, 378–383. [Google Scholar] [CrossRef] [Green Version]
- Tikoo, K.; Patel, G.; Kumar, S.; Karpe, P.A.; Sanghavi, M.; Malek, V.; Srinivasan, K. Tissue specific up regulation of ACE2 in rabbit model of atherosclerosis by atorvastatin: Role of epigenetic histone modifications. Biochem. Pharmacol. 2015, 93, 343–351. [Google Scholar] [CrossRef]
- Li, Y.-H.; Wang, Q.-X.; Zhou, J.-W.; Chu, X.-M.; Man, Y.-L.; Liu, P.; Ren, B.-B.; Sun, T.-R.; An, Y. Effects of rosuvastatin on expression of angiotensin-converting enzyme 2 after vascular balloon injury in rats. J. Geriatr. Cardiol. 2013, 10, 151–158. [Google Scholar] [CrossRef]
- Schindler, C.; Guenther, K.; Hermann, C.; Ferrario, C.M.; Schroeder, C.; Haufe, S.; Jordan, J.; Kirch, W. Statin treatment in hypercholesterolemic men does not attenuate angiotensin II-induced venoconstriction. PLoS ONE 2014, 9, e103909. [Google Scholar] [CrossRef] [Green Version]
- Patel, V.B.; Bodiga, S.; Fan, D.; Das, S.K.; Wang, Z.; Wang, W.; Basu, R.; Zhong, J.; Kassiri, Z.; Oudit, G.Y. Cardioprotective effects mediated by angiotensin II type 1 receptor blockade and enhancing angiotensin 1-7 in experimental heart failure in angiotensin-converting enzyme 2-null mice. Hypertension 2012, 59, 1195–1203. [Google Scholar] [CrossRef] [Green Version]
- Hannich, M.; Nauck, H.W.M.; Reincke, M.; Adolf, C.; Völzke, H.; Rettig, R.; Hannemann, A. Physiological Aldosterone Concentrations Are Associated with Alterations of Lipid Metabolism: Observations from the General Population. Int. J. Endocrinol. 2018, 6, 4128174. [Google Scholar] [CrossRef] [Green Version]
- Baudrand, R.; Pojoga, L.H.; Vaidya, A.; Garza, A.E.; Vöhringer, P.A.; Jeunemaitre, X.; Hopkins, P.N.; Yao, T.M.; Williams, J.; Adler, G.K.; et al. Statin Use and Adrenal Aldosterone Production in Hypertensive and Diabetic Subjects. Circulation 2015, 132, 1825–1833. [Google Scholar] [CrossRef] [Green Version]
- Hornik, E.S.; Altman-Merino, A.E.; Koefoed, A.W.; Meyer, K.M.; Stone, I.B.; Green, J.A.; Williams, G.H.; Adler, G.K.; Williams, J.S. A clinical trial to evaluate the effect of statin use on lowering aldosterone levels. BMC Endocr. Dis. 2020, 20, 105. [Google Scholar] [CrossRef]
- Drapala, A.; Sikora, M.; Ufnal, M. Statins, the renin-angiotensin-aldosterone system and hypertension—A tale of another beneficial effect of statins. J. Renin Angiotensin Aldosterone Syst. JRAAS 2014, 15, 250–258. [Google Scholar] [CrossRef]
- Pignatelli, P.; Carnevale, R.; Pastori, D.; Cangemi, R.; Napoleone, L.; Bartimoccia, S.; Nocella, C.; Basili, S.; Violi, F. Immediate antioxidant and antiplatelet effect of atorvastatin via inhibition of Nox2. Circulation 2012, 126, 92–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, M.T.; Fuset, M.P.; Ruano, M.; Moscardó, A.; Valles, J. Effect of atorvastatin on platelet thromboxane A(2) synthesis in aspirin-treated patients with acute myocardial infarction. Am. J. Cardiol. 2009, 104, 1618–1623. [Google Scholar] [CrossRef] [PubMed]
- Undas, A.; Siudak, Z.; Topór-Mądry, R.; Leśniak, M.; Tracz, W. Simvastatin administration reduces thromboxane production in subjects taking aspirin: Links between aspirin resistance and thrombin generation. Int. J. Cardiol. 2012, 154, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Millar Philip, J.; Floras John, S. Statins and the autonomic nervous system. Clin. Sci. 2013, 126, 401–415. [Google Scholar] [CrossRef] [Green Version]
- Lewandowski, J.; Symonides, B.; Gaciong, Z.; Siński, M. The effect of statins on sympathetic activity: A meta-analysis. Clin. Auton. Res. 2015, 25, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Moreira, E.D.; Mostarda, C.T.; Moraes-Silva, I.C.; Ferreira, J.B.; Santos, F.D.; Lacchini, S.; De Angelis, K.; Rodrigues, B.; Irigoyen, M.C. Effect of simvastatin in the autonomic system is dependent on the increased gain/sensitivity of the baroreceptors. Physiol. Rep. 2013, 1. [Google Scholar] [CrossRef]
- Chen, Y.; Michaelis, M.; Janig, W.; Devor, M. Adrenoreceptor subtype mediating sympathetic-sensory coupling in injured sensory neurons. J. Neurophysiol. 1996, 76, 3721–3730. [Google Scholar] [CrossRef]
- Pleiner, J.; Schaller, G.; Mittermayer, F.; Zorn, S.; Marsik, C.; Polterauer, S.; Kapiotis, S.; Wolzt, M. Simvastatin prevents vascular hyporeactivity during inflammation. Circulation 2004, 110, 3349–3354. [Google Scholar] [CrossRef] [Green Version]
- Mühlhäuser, U.; Zolk, O.; Rau, T.; Münzel, F.; Wieland, T.; Eschenhagen, T. Atorvastatin desensitizes β-adrenergic signaling in cardiac myocytes via reduced isoprenylation of G-protein γ-subunits. FASEB J. 2006, 20, 785–787. [Google Scholar] [CrossRef]
- Tennakoon, M.; Kankanamge, D.; Senarath, K.; Fasih, Z.; Karunarathne, A. Statins perturb Gβγ signaling and cell behaviors in a Gγ subtype dependent manner. Mol. Pharmacol. 2019, 95, 361–375. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Adachi, T.; Pimentel, D.R.; Ido, Y.; Colucci, W.S. Statins Inhibit β-Adrenergic Receptor–Stimulated Apoptosis in Adult Rat Ventricular Myocytes via a Rac1-Dependent Mechanism. Circulation 2004, 110, 412–418. [Google Scholar] [CrossRef] [Green Version]
- Kandasamy, K.; Prawez, S.; Choudhury, S.; More, A.S.; Ahanger, A.A.; Singh, T.U.; Parida, S.; Mishra, S.K. Atorvastatin prevents vascular hyporeactivity to norepinephrine in sepsis: Role of nitric oxide and α1-adrenoceptor mRNA expression. Shock 2011, 36, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Carillion, A.; Feldman, S.; Na, N.; Biais, M.; Carpentier, W.; Birenbaum, A.; Cagnard, N.; Loyer, X.; Bonnefont-Rousselot, D.; Hatem, S.; et al. Atorvastatin reduces β-Adrenergic dysfunction in rats with diabetic cardiomyopathy. PLoS ONE 2017, 12, e0180103. [Google Scholar] [CrossRef] [Green Version]
- Vandresen-Filho, S.; França, L.M.; Alcantara-Junior, J.; Nogueira, L.C.; de Brito, T.M.; Lopes, L.; Junior, F.M.; Vanzeler, M.L.; Bertoldo, D.B.; Dias, P.G.; et al. Statins enhance cognitive performance in object location test in albino Swiss mice: Involvement of beta-adrenoceptors. Physiol. Behav. 2015, 143, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Tokuhisa, H.; Murai, H.; Okabe, Y.; Hamaoka, T.; Sugimoto, H.; Mukai, Y.; Inoue, O.; Takashima, S.-I.; Kato, T.; Usui, S.; et al. Differential effects of lipophilic and hydrophilic statins on muscle sympathetic nerve activity in heart failure with preserved left ventricular ejection fraction. Auton. Neurosc. 2018, 213, 8–14. [Google Scholar] [CrossRef]
- Gorabi, A.M.; Kiaie, N.; Bianconi, V.; Jamialahmadi, T.; Al-Rasadi, K.; Johnston, T.P.; Pirro, M.; Sahebkar, A. Antiviral effects of statins. Progress Lipid Res. 2020, 79, 101054. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Ahn, J.; Park, J.; Kyung Kang, C.; Won, S.-H.; Kim, D.W.; Park, J.-H.; Chung, K.-H.; Joh, J.-S.; Bang, J.H. Beneficial Effect of Statins in COVID-19–Related Outcomes—Brief Report: A National Population-Based Cohort Study. Arterioscler. Thromb. Vasc. Biol. 2021, 41, e175–e182. [Google Scholar] [CrossRef]
- Gupta, A.; Madhavan, M.V.; Poterucha, T.J.; DeFilippis, E.M.; Hennessey, J.A.; Redfors, B.; Eckhardt, C.; Bikdeli, B.; Platt, J.; Nalbandian, A. Association between antecedent statin use and decreased mortality in hospitalized patients with COVID-19. Nat. Commun. 2021, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-J.; Qin, J.-J.; Cheng, X.; Shen, L.; Zhao, Y.-C.; Yuan, Y.; Lei, F.; Chen, M.-M.; Yang, H.; Bai, L. In-hospital use of statins is associated with a reduced risk of mortality among individuals with COVID-19. Cell Metab. 2020, 32, 176–187.e174. [Google Scholar] [CrossRef] [PubMed]
- Namsolleck, P.; Moll, G.N. Does activation of the protective Renin-Angiotensin System have therapeutic potential in COVID-19? Mol. Med. 2020, 26, 80. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Xiao, G.; Zhang, J.; He, X.; Ou, M.; Bi, J.; Yang, R.; Di, W.; Wang, Z.; Li, Z.; et al. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Emerg. Microbes Infect. 2020, 9, 757–760. [Google Scholar] [CrossRef]
- D'Ardes, D.; Boccatonda, A.; Rossi, I.; Guagnano, M.T.; Santilli, F.; Cipollone, F.; Bucci, M. COVID-19 and RAS: Unravelling an Unclear Relationship. Int. J. Mol. Sci. 2020, 21, 3003. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e278. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Cavallini, C.; Spanevello, A.; Angeli, F. COVID-19: ACE2centric infective disease? Hypertension 2020, 76, 294–299. [Google Scholar] [CrossRef]
- Verdecchia, P.; Cavallini, C.; Spanevello, A.; Angeli, F. The pivotal link between ACE2 deficiency and SARS-CoV-2 infection. Eur. J. Intern. Med. 2020, 76, 14–20. [Google Scholar] [CrossRef]
- Vicenzi, M.; Di Cosola, R.; Ruscica, M.; Ratti, A.; Rota, I.; Rota, F.; Bollati, V.; Aliberti, S.; Blasi, F. The liaison between respiratory failure and high blood pressure: Evidence from COVID-19 patients. Eur. Respir. J. 2020, 56, 2001157. [Google Scholar] [CrossRef]
- Burrell, L.M.; Johnston, C.I.; Tikellis, C.; Cooper, M.E. ACE2, a new regulator of the renin–angiotensin system. Trends Endocrinol. Metab. 2004, 15, 166–169. [Google Scholar] [CrossRef]
- Michaud, V.; Deodhar, M.; Arwood, M.; Al Rihani, S.B.; Dow, P.; Turgeon, J. ACE2 as a Therapeutic Target for COVID-19; Its Role in Infectious Processes and Regulation by Modulators of the RAAS System. J. Clin. Med. 2020, 9, 2096. [Google Scholar] [CrossRef]
- Subir, R.; Jagat, J.M.; Kalyan, K.G. Pros and cons for use of statins in people with coronavirus disease-19 (COVID-19). Diabetes Metab. Syndr. 2020, 14, 1225–1229. [Google Scholar] [CrossRef]
- Tan, W.Y.T.; Young, B.E.; Lye, D.C.; Chew, D.E.K.; Dalan, R. Statin use is associated with lower disease severity in COVID-19 infection. Sci. Rep. 2020, 10, 17458. [Google Scholar] [CrossRef]
- Sun, T.; Jiang, D.; Zhang, L.; Su, Q.; Mao, W.; Jiang, C. Expression profile of cathepsins indicates the potential of cathepsins B and D as prognostic factors in breast cancer patients. Oncol. Lett. 2016, 11, 575–583. [Google Scholar] [CrossRef] [Green Version]
- Altaf, A.; Qu, P.; Zhao, Y.; Wang, H.; Lou, D.; Niu, N. NLRP3 inflammasome in peripheral blood monocytes of acute coronary syndrome patients and its relationship with statins. Coron. Artery Dis. 2015, 26, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Hurks, R.; Hoefer, I.E.; Vink, A.; Pasterkamp, G.; Schoneveld, A.; Kerver, M.; de Vries, J.P.P.M.; Tangelder, M.J.; Moll, F.L. Different Effects of Commonly Prescribed Statins on Abdominal Aortic Aneurysm Wall Biology. Eur. J. Vasc. Endovasc. Surg. 2010, 39, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abisi, S.; Burnand, K.G.; Humphries, J.; Waltham, M.; Taylor, P.; Smith, A. Effect of statins on proteolytic activity in the wall of abdominal aortic aneurysms. Br. J. Surg. 2008, 95, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Solberg, R.; Jacobsen, L.L.; Voreland, A.L.; Rustan, A.C.; Thoresen, G.H.; Johansen, H.T. Simvastatin Inhibits Glucose Metabolism and Legumain Activity in Human Myotubes. PLoS ONE 2014, 9, e85721. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Shi, X.; Hao, N.; Chen, Z.; Wei, L.; Tan, L.; Chen, Y.; Feng, H.; Chen, Q.; Zhu, G. Simvastatin Reduces Neutrophils Infiltration Into Brain Parenchyma After Intracerebral Hemorrhage via Regulating Peripheral Neutrophils Apoptosis. Front. Neurosci. 2018, 12. [Google Scholar] [CrossRef] [Green Version]
- Chello, M.; Anselmi, A.; Spadaccio, C.; Patti, G.; Goffredo, C.; Di Sciascio, G.; Covino, E. Simvastatin Increases Neutrophil Apoptosis and Reduces Inflammatory Reaction After Coronary Surgery. Ann. Thoracic Surg. 2007, 83, 1374–1380. [Google Scholar] [CrossRef]
- Yamamoto, N.; Fujii, Y.; Kasahara, R.; Tanida, M.; Ohora, K.; Ono, Y.; Suzuki, K.; Sobue, K. Simvastatin and atorvastatin facilitates amyloid β-protein degradation in extracellular spaces by increasing neprilysin secretion from astrocytes through activation of MAPK/Erk1/2 pathways. Glia 2016, 64, 952–962. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiaie, N.; Gorabi, A.M.; Reiner, Ž.; Jamialahmadi, T.; Ruscica, M.; Sahebkar, A. Effects of Statins on Renin–Angiotensin System. J. Cardiovasc. Dev. Dis. 2021, 8, 80. https://doi.org/10.3390/jcdd8070080
Kiaie N, Gorabi AM, Reiner Ž, Jamialahmadi T, Ruscica M, Sahebkar A. Effects of Statins on Renin–Angiotensin System. Journal of Cardiovascular Development and Disease. 2021; 8(7):80. https://doi.org/10.3390/jcdd8070080
Chicago/Turabian StyleKiaie, Nasim, Armita Mahdavi Gorabi, Željko Reiner, Tannaz Jamialahmadi, Massimiliano Ruscica, and Amirhossein Sahebkar. 2021. "Effects of Statins on Renin–Angiotensin System" Journal of Cardiovascular Development and Disease 8, no. 7: 80. https://doi.org/10.3390/jcdd8070080
APA StyleKiaie, N., Gorabi, A. M., Reiner, Ž., Jamialahmadi, T., Ruscica, M., & Sahebkar, A. (2021). Effects of Statins on Renin–Angiotensin System. Journal of Cardiovascular Development and Disease, 8(7), 80. https://doi.org/10.3390/jcdd8070080