

Predictive Value of the Transthoracic Echocardiography Index for Acute Kidney Injury after Cardiac Valve Surgery

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
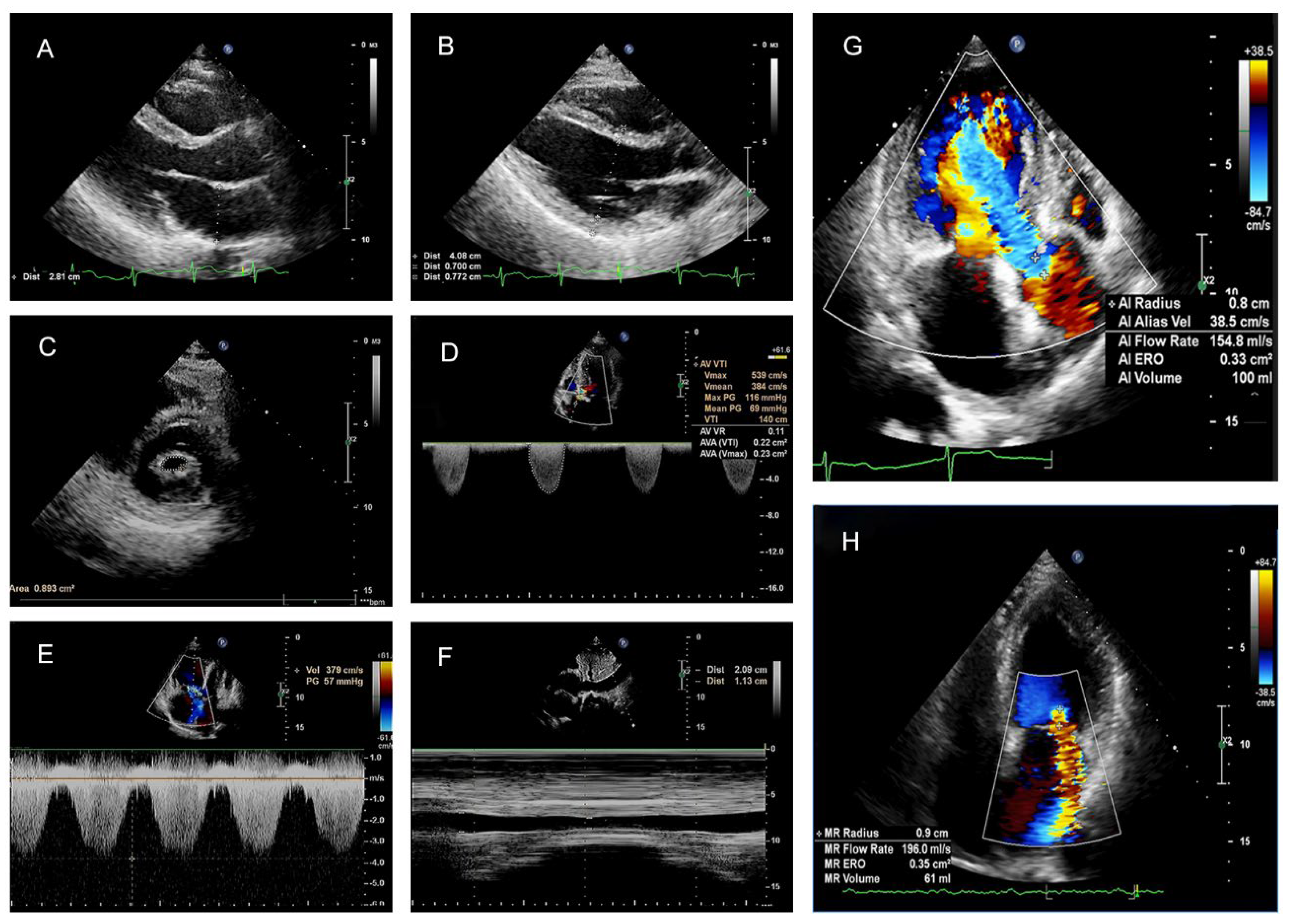
2.2. Echocardiographic Parameters
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Transthoracic Doppler Echocardiography Index (TTEI)
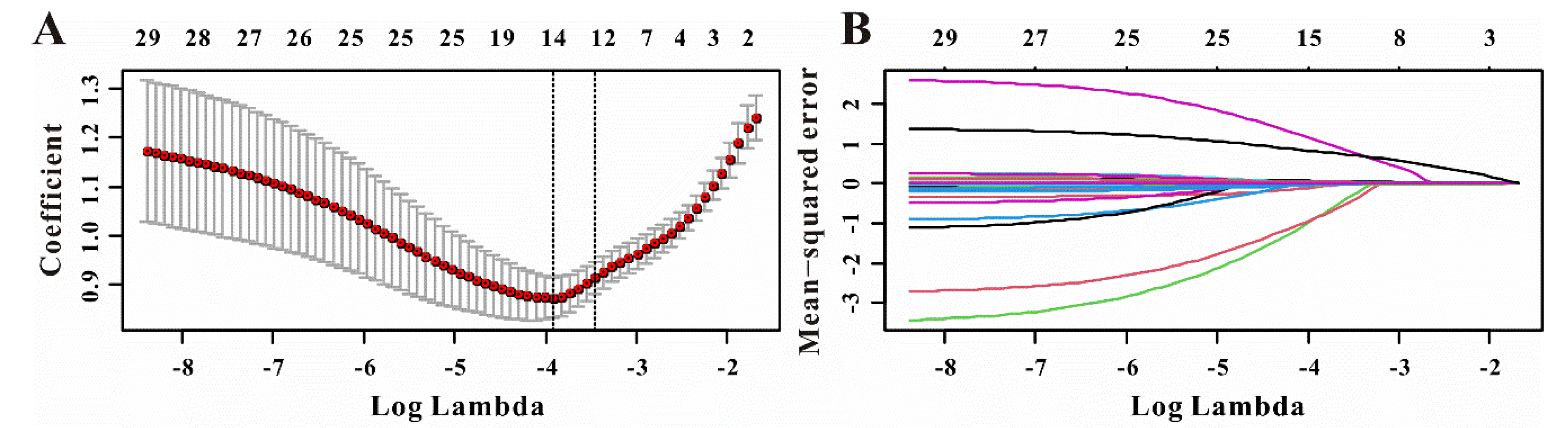
3.3. Model Construction Based on TTEI Established by LASSO Regression and Clinical Features
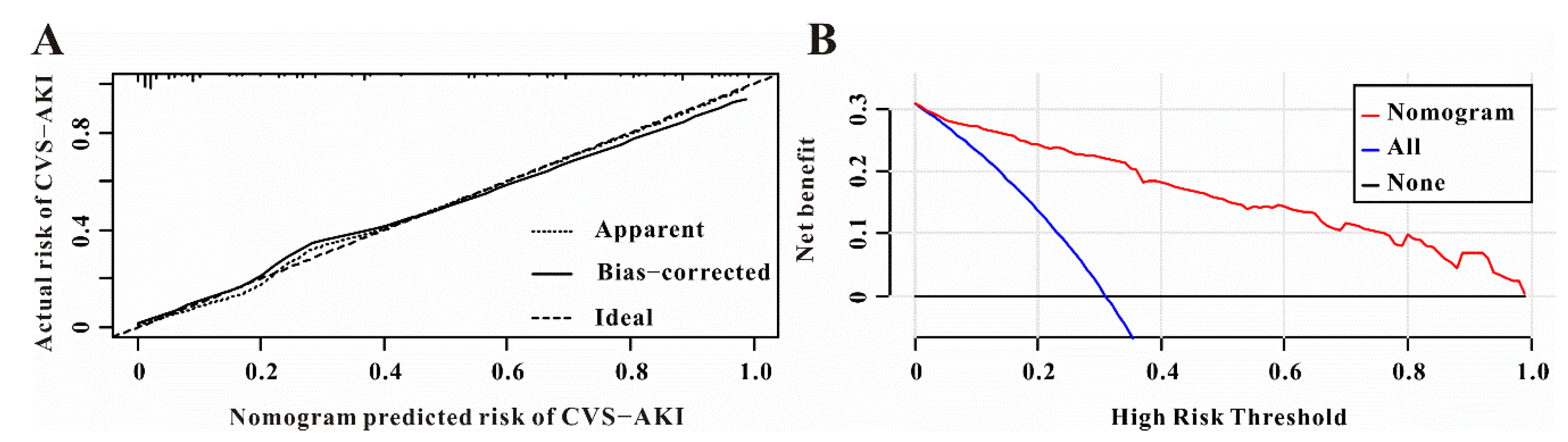
3.4. The Performance of the Nomogram for CVS−AKI
3.5. The Improvement of TTEI for CVS−AKI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostermann, M.; Kunst, G.; Baker, E.; Weerapolchai, K.; Lumlertgul, N. Cardiac Surgery Associated AKI Prevention Strategies and Medical Treatment for CSA-AKI. J. Clin. Med. 2021, 10, 5285. [Google Scholar] [CrossRef] [PubMed]
- Schurle, A.; Koyner, J.L. CSA-AKI: Incidence, Epidemiology, Clinical Outcomes, and Economic Impact. J. Clin. Med. 2021, 10, 5746. [Google Scholar] [CrossRef]
- Wang, Y.; Bellomo, R. Cardiac surgery-associated acute kidney injury: Risk factors, pathophysiology and treatment. Nat. Rev. Nephrol. 2017, 13, 697–711. [Google Scholar] [CrossRef] [PubMed]
- Serraino, G.F.; Provenzano, M.; Jiritano, F.; Michael, A.; Ielapi, N.; Mastroroberto, P.; Andreucci, M.; Serra, R. Risk factors for acute kidney injury and mortality in high risk patients undergoing cardiac surgery. PLoS ONE 2021, 16, e0252209. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.B.; Suneja, M.; Bayman, E.O.; Weide, G.D.; Tarasi, M. Association between postoperative acute kidney injury and duration of cardiopulmonary bypass: A meta-analysis. J. Cardiothorac. Vasc. Anesth. 2012, 26, 64–69. [Google Scholar] [CrossRef]
- Yang, J.J.; Lei, W.H.; Hu, P.; Bin Wu, B.; Chen, J.X.; Ni, Y.M.; Lai, E.Y.; Han, F.; Chen, J.H.; Yang, Y. Preoperative Serum Fibrinogen is Associated With Acute Kidney Injury after Cardiac Valve Replacement Surgery. Sci. Rep. 2020, 10, 6403. [Google Scholar] [CrossRef]
- Jin, J.; Chang, S.C.; Shen, B.; Xu, J.; Jiang, W.; Wang, Y.; Zhuang, Y.; Wang, C.; Teng, J.; Ding, X. Usefulness of High Estimated Pulmonary Artery Systolic Pressure to Predict Acute Kidney Injury After Cardiac Valve Operations. Am. J. Cardiol. 2019, 123, 440–445. [Google Scholar] [CrossRef]
- Kinno, M.; Cantey, E.P.; Rigolin, V.H. The transition from transesophageal to transthoracic echocardiography during transcatheter aortic valve replacement: An evolving field. J. Echocardiogr. 2019, 17, 25–34. [Google Scholar] [CrossRef]
- Michalowska, I.; Stoklosa, P.; Milkowska, M.; Zakrzewski, D.; Nieznanska, M.; Kwiatek, P.; Lewandowska, S.; Kusmierski, K.; Kolsut, P.; Kusmierczyk, M.; et al. The role of cardiac computed tomography in the diagnosis of prosthetic valve endocarditis—A comparison with transthoracic and transesophageal echocardiography and intra-operative findings. Eur. J. Radiol. 2021, 138, 109637. [Google Scholar] [CrossRef]
- Heiberg, J.; El-Ansary, D.; Royse, C.F.; Royse, A.G.; Alsaddique, A.A.; Canty, D.J. Transthoracic and transoesophageal echocardiography: A systematic review of feasibility and impact on diagnosis, management and outcome after cardiac surgery. Anaesthesia 2016, 71, 1210–1221. [Google Scholar] [CrossRef] [Green Version]
- Korshin, A.; Gronlykke, L.; Nilsson, J.C.; Moller-Sorensen, H.; Ihlemann, N.; Kjoller, M.; Damgaard, S.; Lehnert, P.; Hassager, C.; Kjaergaard, J.; et al. The feasibility of tricuspid annular plane systolic excursion performed by transesophageal echocardiography throughout heart surgery and its interchangeability with transthoracic echocardiography. Int. J. Cardiovasc. Imaging 2018, 34, 1017–1028. [Google Scholar] [CrossRef] [PubMed]
- Mauermann, E.; Bouchez, S.; Bove, T.; Vandenheuvel, M.; Wouters, P. Assessing Left Ventricular Early Diastolic Velocities with Tissue Doppler and Speckle Tracking by Transesophageal and Transthoracic Echocardiography. Anesth. Analg. 2021, 132, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Waldmann, V.; Milleron, O.; Iung, B.; Messika-Zeitoun, D.; Lepage, L.; Ghodbane, W.; Brochet, E.; Vahanian, A.; Nataf, P.; Jondeau, G. Is Transesophageal Echocardiography Needed before Hospital Discharge in Patients after Bentall Surgery? J. Am. Soc. Echocardiogr. 2017, 30, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Sapp, A.; Drahos, A.; Lashley, M.; Christie, A.; Christie, D.B. The Impact of Hemodynamic Transesophageal Echocardiography on Acute Kidney Injury Management and Use of Continuous Renal Replacement Therapy in Trauma. Am. Surg. 2020, 86, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-J.; Park, J.-S.; Kim, H.-H. Diastolic dysfunction is associated with an increased risk of postcontrast acute kidney injury. Medicine 2019, 98, e17994. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.-S.; Wang, Y.-W.; Tai, C.-C.; Hsieh, Y.-C.; Lee, P.-C.; Huang, C.-C.; Huang, Y.-H.; Hou, M.-C.; Lin, H.-C.; Lee, K.-C. Early echocardiographic signs of diastolic dysfunction predict acute kidney injury in cirrhotic patients. J. Chin. Med. Assoc. 2020, 83, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Lameire, N. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.R.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Munoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Rev. Esp. Cardiol. (Engl. Ed.) 2018, 71, 110. [Google Scholar]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk, N.A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [PubMed]
- Catalano, M.; Lin, D.; Cassiere, H.; Kohn, N.; Rutkin, B.; Maurer, G.; Berg, J.A.; Jahn, J.; Esposito, R.; Hartman, A.; et al. Incidence of Acute Kidney Injury in Patients with Chronic Renal Insufficiency: Transcatheter versus Surgical Aortic Valve Replacement. J. Interv. Cardiol. 2019, 2019, 9780415. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zou, G.; Liu, J. Preoperative Glucose-to-Lymphocyte Ratio is an Independent Predictor for Acute Kidney Injury After Cardiac Surgery in Patients in Intensive Care Unit. Int. J. Gen. Med. 2021, 14, 6529–6537. [Google Scholar] [CrossRef] [PubMed]
- Remer, E.M.; Papanicolaou, N.; Casalino, D.D.; Bishoff, J.T.; Blaufox, M.D.; Coursey, C.A.; Dighe, M.; Eberhardt, S.C.; Goldfarb, S.; Harvin, H.J.; et al. ACR Appropriateness Criteria(®) on renal failure. Am. J. Med. 2014, 127, 1041–1048.e1. [Google Scholar] [CrossRef]
- Wang, X.Y.; Pang, Y.P.; Jiang, T.; Wang, S.; Li, J.T.; Shi, B.M.; Yu, C. Value of early diagnosis of sepsis complicated with acute kidney injury by renal contrast-enhanced ultrasound. World J. Clin. Cases 2019, 7, 3934–3944. [Google Scholar] [CrossRef]
- Yoon, H.E.; Kim, D.W.; Kim, D.; Kim, Y.; Shin, S.J.; Shin, Y.R. A pilot trial to evaluate the clinical usefulness of contrast-enhanced ultrasound in predicting renal outcomes in patients with acute kidney injury. PLoS ONE 2020, 15, e0235130. [Google Scholar] [CrossRef]
- Selby, N.M.; Williams, J.P.; Phillips, B.E. Application of dynamic contrast enhanced ultrasound in the assessment of kidney diseases. Curr. Opin. Nephrol. Hypertens. 2021, 30, 138–143. [Google Scholar] [CrossRef]
- Watchorn, J.; Huang, D.Y.; Joslin, J.; Bramham, K.; Hutchings, S.D. Critically Ill COVID-19 Patients with Acute Kidney Injury Have Reduced Renal Blood Flow and Perfusion Despite Preserved Cardiac Function: A Case-Control Study Using Contrast-Enhanced Ultrasound. Shock 2021, 55, 479–487. [Google Scholar] [CrossRef]
- Pettey, G.; Hermansen, J.L.; Nel, S.; Moutlana, H.J.; Muteba, M.; Juhl-Olsen, P.; Tsabedze, N.; Chakane, P.M. Ultrasound Hepatic Vein Ratios Are Associated with the Development of Acute Kidney Injury After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2022, 36, 1326–1335. [Google Scholar] [CrossRef]
- Beaubien-Souligny, W.; Denault, A.; Robillard, P.; Desjardins, G. The Role of Point-of-Care Ultrasound Monitoring in Cardiac Surgical Patients with Acute Kidney Injury. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2781–2796. [Google Scholar] [CrossRef] [PubMed]
- Aslaner, M.A.; Yasar, E.; Kilicaslan, I.; Cerit, M.N.; Emren, S.V.; Yuksek, B.; Karakok, B.; Baykus, B.A.; Bildik, F.; Guz, G.; et al. Accuracy of Multi-organ Point-of-Care Ultrasound for Acute Kidney Injury Etiologies. Ultrasound Med. Biol. 2022, 48, 2009–2018. [Google Scholar] [CrossRef] [PubMed]
- Nepal, S.; Dachsel, M.; Smallwood, N. Point-of-care ultrasound rapidly and reliably diagnoses renal tract obstruction in patients admitted with acute kidney injury. Clin. Med. 2020, 20, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Young, A.; Crawford, T.; Pierre, A.S.; Trent, M.J.; Fraser, C.; Conte, J.; Whitman, G.; Sciortino, C. Renal ultrasound provides low utility in evaluating cardiac surgery associated acute kidney injury. J. Cardiothorac. Surg. 2017, 12, 75. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Dong, Y.; Zhao, B.; Liu, K. Preoperative NT-proBNP and LVEF for the prediction of acute kidney injury after noncardiac surgery: A single-centre retrospective study. BMC Anesthesiol. 2022, 22, 196. [Google Scholar] [CrossRef]
- Khoury, S.; Steinvil, A.; Gal-Oz, A.; Margolis, G.; Hochstatd, A.; Topilsky, Y.; Keren, G.; Shacham, Y. Association between central venous pressure as assessed by echocardiography, left ventricular function and acute cardio-renal syndrome in patients with ST segment elevation myocardial infarction. Clin. Res. Cardiol. 2018, 107, 937–944. [Google Scholar] [CrossRef]
- Yockelson, S.R.; Heitner, S.B.; Click, S.; Geleto, G.; Treggiari, M.M.; Hutchens, M.P. Right Ventricular Systolic Performance Determined by 2D Speckle-Tracking Echocardiography and Acute Kidney Injury After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2019, 33, 725–731. [Google Scholar] [CrossRef]
- Kajal, K.; Chauhan, R.; Negi, S.L.; Gourav, K.P.; Panda, P.; Mahajan, S.; Sarna, R. Intraoperative evaluation of renal resistive index with transesophageal echocardiography for the assessment of acute renal injury in patients undergoing coronary artery bypass grafting surgery: A prospective observational study. Ann. Card. Anaesth. 2022, 25, 158–163. [Google Scholar]
- Hu, Y.; Zhou, J.; Cao, Q.; Wang, H.; Yang, Y.; Xiong, Y.; Zhou, Q. Utilization of Echocardiography After Acute Kidney Injury Was Associated with Improved Outcomes in Patients in Intensive Care Unit. Int. J. Gen. Med. 2021, 14, 2205–2213. [Google Scholar] [CrossRef]
- Han, S.S.; Park, S.; Kang, S.H.; Cho, G.Y.; Kim, D.K.; Kim, S.; Chin, H.J.; Chae, D.W.; Na, K.Y. Usefulness of Preoperative Echocardiography to Predict Acute Kidney Injury and Long-Term Mortality After Coronary Artery Bypass Grafting. Am. J. Cardiol. 2017, 119, 231–236. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. BMJ 2015, 350, g7594. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No AKI (n = 147) | AKI (n = 66) | p-Value |
|---|---|---|---|
| Age, years old | 57.2 ± 9.3 | 62.9 ± 8.9 | <0.001 |
| Gender, male, n (%) | 100 (68.0) | 44 (66.7) | 0.844 |
| Types of valvular surgery, n (%) | 0.840 | ||
| One valve | 43 (29.3) | 19 (28.8) | |
| Two valves | 54 (36.7) | 24 (36.4) | |
| Three valves | 13 (8.8) | 8 (12.1) | |
| Valves + CABG | 20 (13.6) | 6 (9.1) | |
| Valves + aortoplasty | 17 (11.6) | 9 (13.6) | |
| Cardiopulmonary bypass time, minutes | 162.0 ± 39.2 | 177.7 ± 46.8 | 0.012 |
| Comorbidities, n (%) | |||
| Hypertension | 51 (34.7) | 37 (56.1) | 0.003 |
| Diabetes mellitus | 5 (3.4) | 7 (10.6) | 0.035 |
| Chronic kidney disease | 14 (9.5) | 11 (16.7) | 0.134 |
| COPD | 4 (2.7) | 4 (6.1) | 0.236 |
| History of PCI | 6 (4.1) | 1 (1.5) | 0.334 |
| Preoperative drug usage, n (%) | |||
| ACEI/ARB | 38 (26.0) | 19 (29.2) | 0.629 |
| NSAID | 17 (11.6) | 8 (12.1) | 0.907 |
| Proton pump inhibitor | 81 (55.1) | 39 (59.1) | 0.587 |
| Antibiotics | 10 (6.8) | 7 (10.6) | 0.344 |
| Usage of contrast medium recently, n (%) | 101 (68.7) | 48 (72.7) | 0.556 |
| Transthoracic echocardiography parameters | |||
| Left ventricular end-diastolic dimension, mm | 53.1 ± 8.6 | 51.8 ± 10.1 | 0.349 |
| ≤44 | 22 (15.0) | 17 (25.8) | |
| >44 | 125 (85.0) | 17 (25.8) | |
| Left atrial end-systolic diameter, mm | 46.8 ± 12.0 | 47.1 ± 8.6 | 0.870 |
| ≤40 | 45 (30.6) | 10 (15.2) | |
| >40 | 102 (69.4) | 56 (84.8) | |
| Interventricular septal thickness, mm | 10.6 ± 1.7 | 11.3 ± 1.8 | 0.015 |
| ≤10.5 | 80 (54.4) | 22 (33.3) | |
| >10.5 | 67 (45.6) | 44 (66.7) | |
| Left ventricular posterior wall thickness, mm | 10.2 ± 1.5 | 10.8 ± 1.5 | 0.011 |
| ≤11.5 | 125 (85.0) | 44 (66.7) | |
| >11.5 | 22 (15.0) | 22 (33.3) | |
| Pulmonary arterial systolic pressure, mmHg | 34.4 ± 7.4 | 40.7 ± 14.0 | <0.001 |
| ≤43 | 129 (87.8) | 45 (68.2) | |
| >43 | 18 (12.2) | 21 (31.8) | |
| Left ventricular ejection fraction, % | 55.5 ± 5.4 | 52.0 ± 6.9 | <0.001 |
| ≤55 | 57 (38.8) | 38 (57.6) | |
| >55 | 90 (61.2) | 28 (42.4) | |
| Moderate or severe aortic regurgitation, n (%) | 56 (38.1) | 19 (28.8) | 0.190 |
| Moderate or severe mitral regurgitation, n (%) | 62 (42.2) | 34 (51.5) | 0.207 |
| Moderate or severe aortic stenosis, n (%) | 14 (9.5) | 10 (15.2) | 0.232 |
| Moderate or severe mitral stenosis, n (%) | 15 (10.2) | 9 (13.6) | 0.466 |
| Laboratory results | |||
| White blood cells, × 109/L | 6.8 ± 2.3 | 6.6 ± 2.9 | 0.648 |
| Hemoglobin, g/L | 127.4 ± 21.0 | 128.0 ± 21.0 | 0.838 |
| Platelets, × 109/L | 180.6 ± 68.4 | 188.2 ± 72.9 | 0.463 |
| Albumin, g/L | 39.5 ± 4.2 | 40.2 ± 5.1 | 0.283 |
| Total bilirubin, µmol/L | 16.4 ± 5.1 | 17.7 ± 8.9 | 0.455 |
| ALT/AST | 0.9 ± 0.4 | 1.0 ± 0.4 | 0.071 |
| Blood urea nitrogen, µmol/L | 7.2 ± 2.9 | 7.3 ± 2.6 | 0.745 |
| eGFR, ml/min | 91.7 ± 21.6 | 73.7 ± 18.0 | <0.001 |
| Uric acid, µmol/L | 361.5 ± 130.9 | 459.5 ± 146.2 | <0.001 |
| NT-pro BNP, ng/L | 361.0 (124.0, 1079.0) | 2080.0 (995.0, 2993.5) | <0.001 |
| cTnI, ng/mL | 0.02 (0.01, 0.06) | 0.01 (0.01, 0.03) | 0.178 |
| Potassium, mmol/L | 4.0 ± 0.5 | 4.0 ± 0.4 | 0.330 |
| Sodium, mmol/L | 139.2 ± 10.1 | 140.7 ± 3.6 | 0.243 |
| Magnesium, mmol/L | 0.8 ± 0.1 | 0.8 ± 0.1 | 0.513 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| β | OR (95%CI) | p | β | OR (95%CI) | p | |
| LVEDD | −0.017 | 0.98 (0.95–1.02) | 0.323 | |||
| LAESD | 0.002 | 1.00 (0.98–1.03) | 0.869 | |||
| IVSD | 0.208 | 1.23 (1.04–1.46) | 0.016 | 0.062 | 1.06 (0.78–1.45) | 0.697 |
| LVPW | 0.257 | 1.29 (1.06–1.58) | 0.013 | 0.346 | 1.41 (1.14–1.76) | 0.002 |
| PASP | 0.058 | 1.06 (1.03–1.09) | <0.001 | 0.068 | 1.07 (1.04–1.11) | <0.001 |
| LVEF > 55% | −0.762 | 0.47 (0.26–0.84) | 0.011 | −0.742 | 0.48 (0.25–0.90) | 0.021 |
| MAR or SAR | −0.420 | 0.66 (0.35–1.23) | 0.190 | |||
| MMR or SMR | 0.376 | 1.46 (0.81–2.61) | 0.206 | |||
| MAS or SAS | 0.529 | 1.70 (0.71–4.05) | 0.234 | |||
| MMS or SMS | 0.329 | 1.39 (0.58–3.36) | 0.465 | |||
| Constant | −6.579 | <0.001 | ||||
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Age | ||||
| ≤60 years old | Ref. | - | Ref. | - |
| >60 years old | 4.29 (2.30–7.98) | <0.001 | 5.60 (2.23–14.05) | <0.001 |
| Diabetes mellitus | ||||
| Yes | 3.92 (1.23–12.48) | 0.021 | 9.60 (1.39–66.37) | 0.022 |
| No | Ref. | - | Ref. | - |
| Chronic kidney disease | ||||
| Yes | 1.90 (0.81–4.45) | 0.139 | ||
| No | Ref. | - | ||
| CPB time | 11.90 (4.11–34.43) | <0.001 | ||
| ≤200 min | Ref. | - | Ref. | - |
| >200 min | 3.60 (1.88–6.89) | <0.001 | ||
| History of PCI | ||||
| Yes | 0.36 (0.04–3.07) | 0.351 | ||
| No | Ref. | - | ||
| Platelets | ||||
| ≤171 × 109/L | Ref. | - | ||
| >171 × 109/L | 1.63 (0.91–2.94) | 0.102 | ||
| Albumin | ||||
| ≤39 g/L | Ref. | - | ||
| >39 g/L | 1.51 (0.83–2.74) | 0.179 | ||
| Blood urea nitrogen | ||||
| ≤6 µmol/L | Ref. | - | Ref. | - |
| >6 µmol/L | 2.15 (1.18–3.90) | 0.012 | 1.39 (0.57–3.38) | 0.464 |
| eGFR | ||||
| ≤90 mL/min | Ref. | - | Ref. | - |
| >90 mL/min | 0.14 (0.07–0.29) | <0.001 | 0.08 (0.03–0.23) | <0.001 |
| Uric acid | ||||
| ≤386 µmol/L | Ref. | - | Ref. | - |
| >386 µmol/L | 4.20 (2.25–7.85) | <0.001 | 3.12 (1.30–7.48) | 0.011 |
| NT-proBNP | ||||
| ≤900 ng/L | Ref. | - | Ref. | - |
| >900 ng/L | 4.23 (2.29–7.83) | <0.001 | 3.84 (1.59–9.25) | <0.001 |
| TTEI | ||||
| ≤−1.01 | Ref. | - | Ref. | - |
| >−1.01 | 5.54 (2.88–10.68) | <0.001 | 6.57 (2.50–17.23) | <0.001 |
| Outcome | AUC | IDI | NRI a | |||||
|---|---|---|---|---|---|---|---|---|
| Biomarker | Biomaker + Clinical Model | Clinical Model b | p-Value c | Value (95%CI) | p-Value | Value (95%CI) | p-Value | |
| TTEI | 0.734 | 0.810 | 0.693 | <0.001 | 0.164 (0.108–0.219) | <0.001 | 0.421 (0.223–0.618) | <0.001 |
| Nomogram excluded for TTEI | 0.854 | 0.917 | <0.001 | 0.231 (0.137–0.324) | <0.001 | 0.367 (0.182–0.552) | <0.001 | |
| Nomogram | 0.880 | 0.925 | <0.001 | 0.067 (0.011–0.124) | 0.020 | 0.076 (0.014–0.196) | 0.023 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, J.; Hu, Y.; Cao, S.; Feng, C.; Huang, X.; Zhou, Q. Predictive Value of the Transthoracic Echocardiography Index for Acute Kidney Injury after Cardiac Valve Surgery. J. Cardiovasc. Dev. Dis. 2022, 9, 316. https://doi.org/10.3390/jcdd9100316
Guo J, Hu Y, Cao S, Feng C, Huang X, Zhou Q. Predictive Value of the Transthoracic Echocardiography Index for Acute Kidney Injury after Cardiac Valve Surgery. Journal of Cardiovascular Development and Disease. 2022; 9(10):316. https://doi.org/10.3390/jcdd9100316
Chicago/Turabian StyleGuo, Juan, Yugang Hu, Sheng Cao, Chuangli Feng, Xin Huang, and Qing Zhou. 2022. "Predictive Value of the Transthoracic Echocardiography Index for Acute Kidney Injury after Cardiac Valve Surgery" Journal of Cardiovascular Development and Disease 9, no. 10: 316. https://doi.org/10.3390/jcdd9100316
APA StyleGuo, J., Hu, Y., Cao, S., Feng, C., Huang, X., & Zhou, Q. (2022). Predictive Value of the Transthoracic Echocardiography Index for Acute Kidney Injury after Cardiac Valve Surgery. Journal of Cardiovascular Development and Disease, 9(10), 316. https://doi.org/10.3390/jcdd9100316