

Short-Term Atrioventricular Dysfunction Recovery after Post-TAVI Pacemaker Implantation

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Baseline Data
2.3. TAVI Procedure
2.4. PPI and Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Baseline Findings
3.2. Indication for Permanent Pacemaker Implantation and Device Programming
3.3. Recovery of Conduction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Siontis, G.C.M.; Overtchouk, P.; Cahill, T.J.; Modine, T.; Prendergast, B.; Praz, F.; Pilgrim, T.; Petrinic, T.; Nikolakopoulou, A.; Salanti, G.; et al. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: An updated meta-analysis. Eur. Heart J. 2019, 40, 3143–3153. [Google Scholar] [CrossRef] [PubMed]
- Ueshima, D.; Fovino, L.N.; Mojoli, M.; Napodano, M.; Fraccaro, C.; Tarantini, G. The interplay between permanent pacemaker implantation and mortality in patients treated by transcatheter aortic valve implantation: A systematic review and meta-analysis. Catheter. Cardiovasc. Interv. 2018, 92, E159–E167. [Google Scholar] [CrossRef] [PubMed]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Siontis, G.C.; Jüni, P.; Pilgrim, T.; Stortecky, S.; Büllesfeld, L.; Meier, B.; Wenaweser, P.; Windecker, S. Predictors of Permanent Pacemaker Implantation in Patients With Severe Aortic Stenosis Undergoing TAVR: A Meta-Analysis. J. Am. Coll. Cardiol. 2014, 64, 129–140. [Google Scholar] [CrossRef]
- Nuis, R.-J.; Van Mieghem, N.M.; Schultz, C.J.; Tzikas, A.; Van Der Boon, R.M.; Maugenest, A.-M.; Cheng, J.; Piazza, N.; Van Domburg, R.T.; Serruys, P.W.; et al. Timing and potential mechanisms of new conduction abnormalities during the implantation of the Medtronic CoreValve System in patients with aortic stenosis. Eur. Heart J. 2011, 32, 2067–2074. [Google Scholar] [CrossRef]
- Giustino, G.; Van der Boon, R.; de Nicolas, J.M.-M.; Dumonteil, N.; Chieffo, A.; de Jaegere, P.; Tchetche, D.; Marcheix, B.; Millischer, D.; Cassagneau, R.; et al. Impact of permanent pacemaker on mortality after transcatheter aortic valve implantation: The PRAGMATIC (Pooled Rotterdam-Milan-Toulouse in Collaboration) Pacemaker substudy. EuroIntervention 2016, 12, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.M.; Yadlapati, A.; Cantey, E.P.; Passman, R.S.; Gajjar, M.; Knight, B.P.; Sweis, R.; Ricciardi, M.J.; Pham, D.T.; Churyla, A.; et al. Conduction recovery following pacemaker implantation after transcatheter aortic valve replacement. Pacing Clin. Electrophysiol. 2018, 42, 146–152. [Google Scholar] [CrossRef]
- Raelson, C.A.; Gabriels, J.; Ruan, J.; Ip, J.E.; Thomas, G.; Liu, C.F.; Cheung, J.W.; Lerman, B.B.; Patel, A.; Markowitz, S.M. Recovery of atrioventricular conduction in patients with heart block after transcatheter aortic valve replacement. J. Cardiovasc. Electrophysiol. 2017, 28, 1196–1202. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. J. Cardio-Thorac. Surg. 2017, 52, 616–664. [Google Scholar] [CrossRef]
- Lilly, S.M.; Deshmukh, A.J.; Epstein, A.E.; Ricciardi, M.J.; Shreenivas, S.; Velagapudi, P.; Wyman, J.F. 2020 ACC Expert Consensus Decision Pathway on Management of Conduction Disturbances in Patients Undergoing Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 76, 2391–2411. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F.; Otto, C.M. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 372–392. [Google Scholar] [CrossRef]
- Urena, M.; Webb, J.G.; Tamburino, C.; Muñoz-Garcia, A.; Cheema, A.; Dager, A.E.; Serra, V.; Amat-Santos, I.J.; Barbanti, M.; Immè, S.; et al. Permanent Pacemaker Implantation After Transcatheter Aortic Valve Implantation. Circulation 2014, 129, 1233–1243. [Google Scholar] [CrossRef] [PubMed]
- Mohananey, D.; Jobanputra, Y.; Kumar, A.; Krishnaswamy, A.; Mick, S.; White, J.M.; Kapadia, S.R. Clinical and Echocardiographic Outcomes Following Permanent Pacemaker Implantation After Transcatheter Aortic Valve Replacement. Circ. Cardiovasc. Interv. 2017, 10, e005046. [Google Scholar] [CrossRef] [PubMed]
- Costa, G.; Zappulla, P.; Barbanti, M.; Cirasa, A.; Todaro, D.; Rapisarda, G.; Picci, A.; Platania, F.; Tosto, A.; Di Grazia, A.; et al. Pacemaker dependency after transcatheter aortic valve implantation: Incidence, predictors and long-term outcomes. EuroIntervention 2019, 15, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Marzahn, C.; Koban, C.; Seifert, M.; Isotani, A.; Neuß, M.; Hölschermann, F.; Butter, C. Conduction recovery and avoidance of permanent pacing after transcatheter aortic valve implantation. J. Cardiol. 2018, 71, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Gaede, L.; Kim, W.-K.; Liebetrau, C.; Dörr, O.; Sperzel, J.; Blumenstein, J.; Berkowitsch, A.; Walther, T.; Hamm, C.; Elsässer, A.; et al. Pacemaker implantation after TAVI: Predictors of AV block persistence. Clin. Res. Cardiol. 2017, 107, 60–69. [Google Scholar] [CrossRef]
- Rodés-Cabau, J.; Ellenbogen, K.A.; Krahn, A.D.; Latib, A.; Mack, M.; Mittal, S.; Muntané-Carol, G.; Nazif, T.M.; Sondergaard, L.; Urena, M.; et al. Management of Conduction Disturbances Associated With Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2019, 74, 1086–1106. [Google Scholar] [CrossRef]
- Schernthaner, C.; Kraus, J.; Danmayr, F.; Hammerer, M.; Schneider, J.; Hoppe, U.C.; Strohmer, B. Short-term pacemaker dependency after transcatheter aortic valve implantation. Wien. Klin. Wochenschr. 2016, 128, 198–203. [Google Scholar] [CrossRef]
- Pereira, E.; Ferreira, N.; Caeiro, D.; Primo, J.; Adão, L.; Oliveira, M.; Gonçalves, H.; Ribeiro, J.; Santos, E.; Leite, D.; et al. Transcatheter Aortic Valve Implantation and Requirements of Pacing Over Time. Pacing Clin. Electrophysiol. 2013, 36, 559–569. [Google Scholar] [CrossRef]
- Elzeneini, M.; Assaf, Y.; Aalaei-Andabili, S.H.; Mahmoud, A.; Hamburger, R.; Goel, R.; Bavry, A.A. Predictors of ventricular pacing burden after permanent pacemaker implantation following transcatheter aortic valve replacement. Clin. Cardiol. 2020, 43, 1334–1342. [Google Scholar] [CrossRef] [PubMed]
- Auffret, V.; Webb, J.G.; Eltchaninoff, H.; Muñoz-García, A.J.; Himbert, D.; Tamburino, C.; Nombela-Franco, L.; Nietlispach, F.; Morís, C.; Ruel, M.; et al. Clinical Impact of Baseline Right Bundle Branch Block in Patients Undergoing Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2017, 10, 1564–1574. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | All Population (n = 50) |
|---|---|
| Clinical characteristics | |
| Age, y, mean ± SD | 82 ± 6 |
| Male, n (%) | 29 (58) |
| BMI, kg/m2, mean ± SD | 27 ± 5 |
| Hypertension, n (%) | 44 (88) |
| Diabetes, n (%) | 14 (28) |
| Smokers, n (%) | 4 (8) |
| Dyslipidemia, n (%) | 28 (56) |
| Familiar history of CVD, n (%) | 12 (24) |
| Obesity, n (%) | 12 (24) |
| Peripheral artery disease, n (%) | 9 (18) |
| Chronic renal diseases, n (%) | 18 (36) |
| NYHA class III-IV, n (%) | 36 (72) |
| Coronary artery diseases, n (%) | 21 (42) |
| Euroscore, %, mean ± SD | 7.8 ± 3.3 |
| STS score mortality, %, mean ± SD | 5 ± 2.8 |
| ECG characteristics | |
| ECG-PR, ms, mean ± SD | 203 ± 52 |
| ECG-QRS, ms, mean ± SD | 118 ± 23 |
| ECG-QT, ms, mean ± SD | 415 ± 36 |
| Atrial Fibrillation, n (%) | 8 (16) |
| ECG-BBS, n (%) | 3 (6) |
| ECG-BBD, n (%) | 5 (10) |
| Procedural characteristics | |
| Elective, n (%) | 42 (84) |
| Delay from TAVI and PM implantation, d, mean ± SD | 6 ± 6 |
| Valvolar CT area, mm2, mean ± SD | 420 ± 51 |
| Apical Approach, n (%) | 3 (6) |
| Valve in valve, n (%) | 1 (2) |
| Bicuspid native valve, n (%) | 1 (2) |
| TAVI balloon expandable, n (%) | 3 (6) |
| Pre-TAVI aortic systolic blood pressure, mmHg, mean ± SD | 142 ± 17 |
| Post-TAVI aortic systolic blood pressure, mmHg, mean ± SD | 163 ± 20 |
| Severe post-TAVI aortic regurgitation | 2 (4) |
| Variables | Group 1 (n = 13) | Group 2 (n = 37) | p-value |
|---|---|---|---|
| Age, y, mean ± SD | 83 ± 5 | 81 ± 7 | 0.71 |
| Male, n (%) | 9 (64) | 20 (55) | 0.75 |
| BMI, kg/m2, mean ± SD | 26 ± 6 | 28 ± 3 | 0.47 |
| Hypertension, n (%) | 12 (92) | 32 (89) | 1.00 |
| Diabetes, n (%) | 6 (46) | 8 (23) | 0.16 |
| Smokers, n (%) | 0 (0) | 4 (11) | 0.56 |
| Dyslipidemia, n (%) | 7 (54) | 21 (58) | 1.00 |
| Familiar history of CVD, n (%) | 1 (8) | 11 (31) | 0.14 |
| Obesity, n (%) | 2 (15) | 10 (28) | 0.47 |
| Peripheral artery disease, n (%) | 2 (15) | 7 (19) | 1.00 |
| Chronic renal disease, n (%) | 6 (46) | 12 (33) | 0.51 |
| NYHA class III-IV, n (%) | 9 (69) | 27 (75) | 0.72 |
| Coronary artery diseases, n (%) | 4 (33) | 17 (47) | 0.51 |
| Euroscore, %, mean ± SD | 8.2 ± 3.5 | 7.7 ± 3.2 | 0.62 |
| STS mortality, %, mean ± SD | 4.9 ± 2.4 | 5.0 ± 3.0 | 0.91 |
| TAVI-to-PPI-time, days, mean ± SD | 9 ± 6 | 5 ± 5 | 0.03 |
| PR pre-TAVI,ms, mean ± SD | 198 ± 36 | 207 ± 50 | 0.78 |
| PR post-TAVI,ms, mean ± SD | 200 ± 35 | 230 ± 51 | 0.16 |
| QRS pre-TAVI,ms, mean ± SD | 107 ± 14 | 124 ± 23 | 0.018 |
| QRS post-TAVI,ms, mean ± SD | 127 ± 24 | 147 ± 16 | 0.018 |
| QT pre-TAVI,ms, mean ± SD | 403 ± 35 | 420 ± 36 | 0.28 |
| QT post-TAVI,ms, mean ± SD | 430 ± 54 | 462 ± 59 | 0.27 |
| Atrial Fibrillation, n (%) | 3 (21) | 5 (14) | 0.54 |
| ECG-LBBB, n (%) | 7 (19) | 4 (29) | 0.25 |
| ECG-RBBB, n (%) | 0 (0) | 6 (17) | 0.11 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | CI 95% | p | OR | CI 95% | p | |
| PR Pre-TAVI | 0.989 | 0.890–1.100 | 0.844 | |||
| QRS Pre-TAVI | 1.039 | 1.004–1.076 | 0.029 | 1.002 | 0.969–1.036 | 0.916 |
| Age | 0.989 | 0.890–1.100 | 0.844 | |||
| Euroscore | 0.966 | 0.796–1.172 | 0.724 | |||
| TAVI-PM Implant (days) | 0.882 | 0.774–1.006 | 0.061 | 0.944 | 0.845–1.215 | 0.890 |
| AF | 0.632 | 0.129–3.102 | 0.572 | |||
| LBBB | 2.750 | 0.524–14.439 | 0.232 | |||
| LBBB post | 0.865 | 0.217–3.458 | 0.838 | |||
| PR post-TAVI | 1.018 | 0.993–1.044 | 0.168 | |||
| QRS post-TAVI | 1.054 | 1.004–1.107 | 0.034 | 1.036 | 0.985–1.090 | 0.171 |
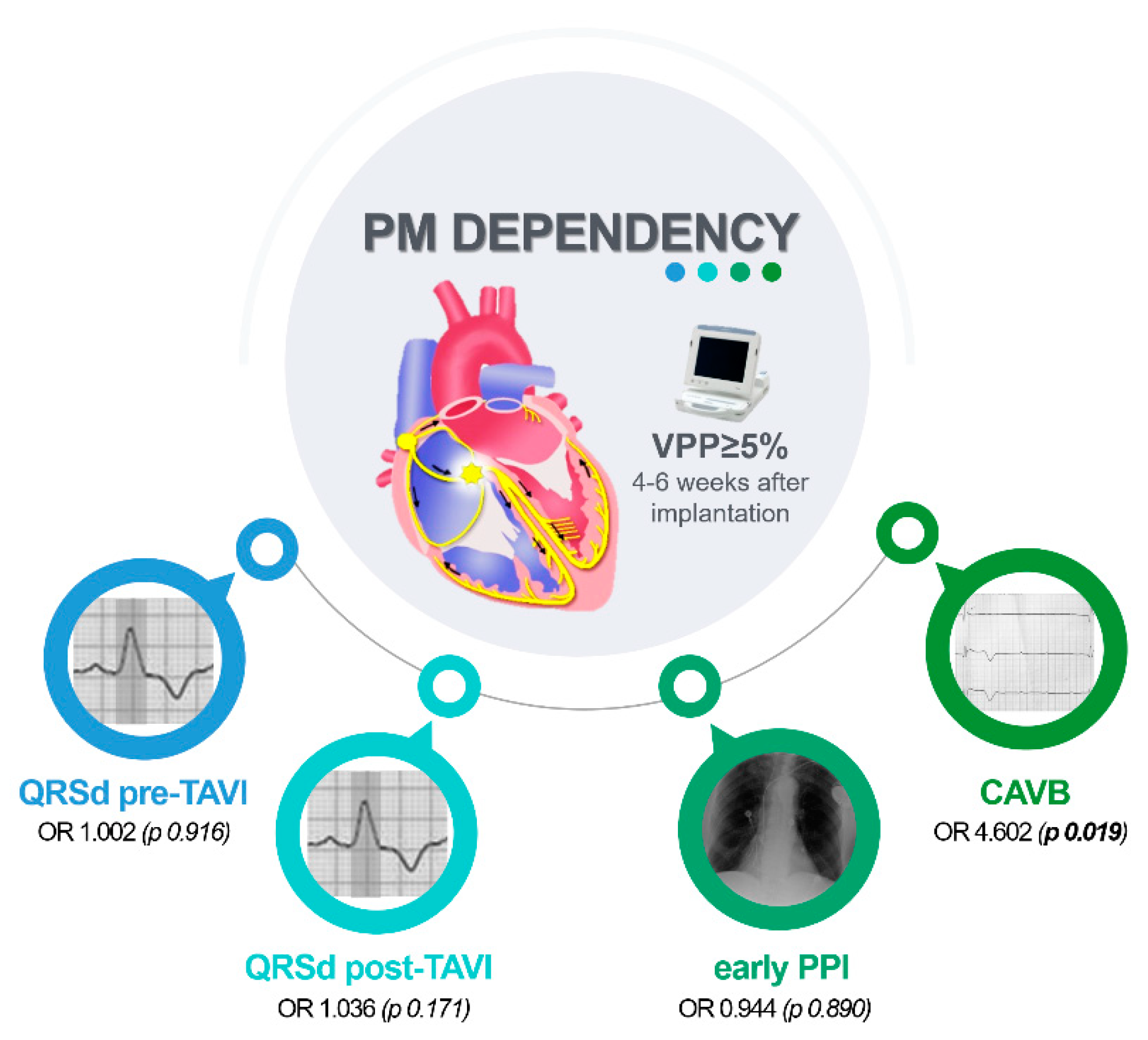
| Complete AVB | 4.354 | 1.032–18.367 | 0.045 | 4.602 | 1.280–9.408 | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinnacchio, G.; Ruscio, E.; Rocco, E.; Trani, C.; Burzotta, F.; Aurigemma, C.; Romagnoli, E.; Scacciavillani, R.; Narducci, M.L.; Bencardino, G.; et al. Short-Term Atrioventricular Dysfunction Recovery after Post-TAVI Pacemaker Implantation. J. Cardiovasc. Dev. Dis. 2022, 9, 324. https://doi.org/10.3390/jcdd9100324
Pinnacchio G, Ruscio E, Rocco E, Trani C, Burzotta F, Aurigemma C, Romagnoli E, Scacciavillani R, Narducci ML, Bencardino G, et al. Short-Term Atrioventricular Dysfunction Recovery after Post-TAVI Pacemaker Implantation. Journal of Cardiovascular Development and Disease. 2022; 9(10):324. https://doi.org/10.3390/jcdd9100324
Chicago/Turabian StylePinnacchio, Gaetano, Eleonora Ruscio, Erica Rocco, Carlo Trani, Francesco Burzotta, Cristina Aurigemma, Enrico Romagnoli, Roberto Scacciavillani, Maria Lucia Narducci, Gianluigi Bencardino, and et al. 2022. "Short-Term Atrioventricular Dysfunction Recovery after Post-TAVI Pacemaker Implantation" Journal of Cardiovascular Development and Disease 9, no. 10: 324. https://doi.org/10.3390/jcdd9100324
APA StylePinnacchio, G., Ruscio, E., Rocco, E., Trani, C., Burzotta, F., Aurigemma, C., Romagnoli, E., Scacciavillani, R., Narducci, M. L., Bencardino, G., Perna, F., Spera, F. R., Comerci, G., Bisignani, A., & Pelargonio, G. (2022). Short-Term Atrioventricular Dysfunction Recovery after Post-TAVI Pacemaker Implantation. Journal of Cardiovascular Development and Disease, 9(10), 324. https://doi.org/10.3390/jcdd9100324