
Educational Nursing Intervention in Reducing Hospital Readmission and the Mortality of Patients with Heart Failure: A Systematic Review and Meta-Analysis
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Type of Study
2.2. Search Strategy and Eligibility Criteria
2.3. Data Collection
2.4. Statistical Analysis
3. Results
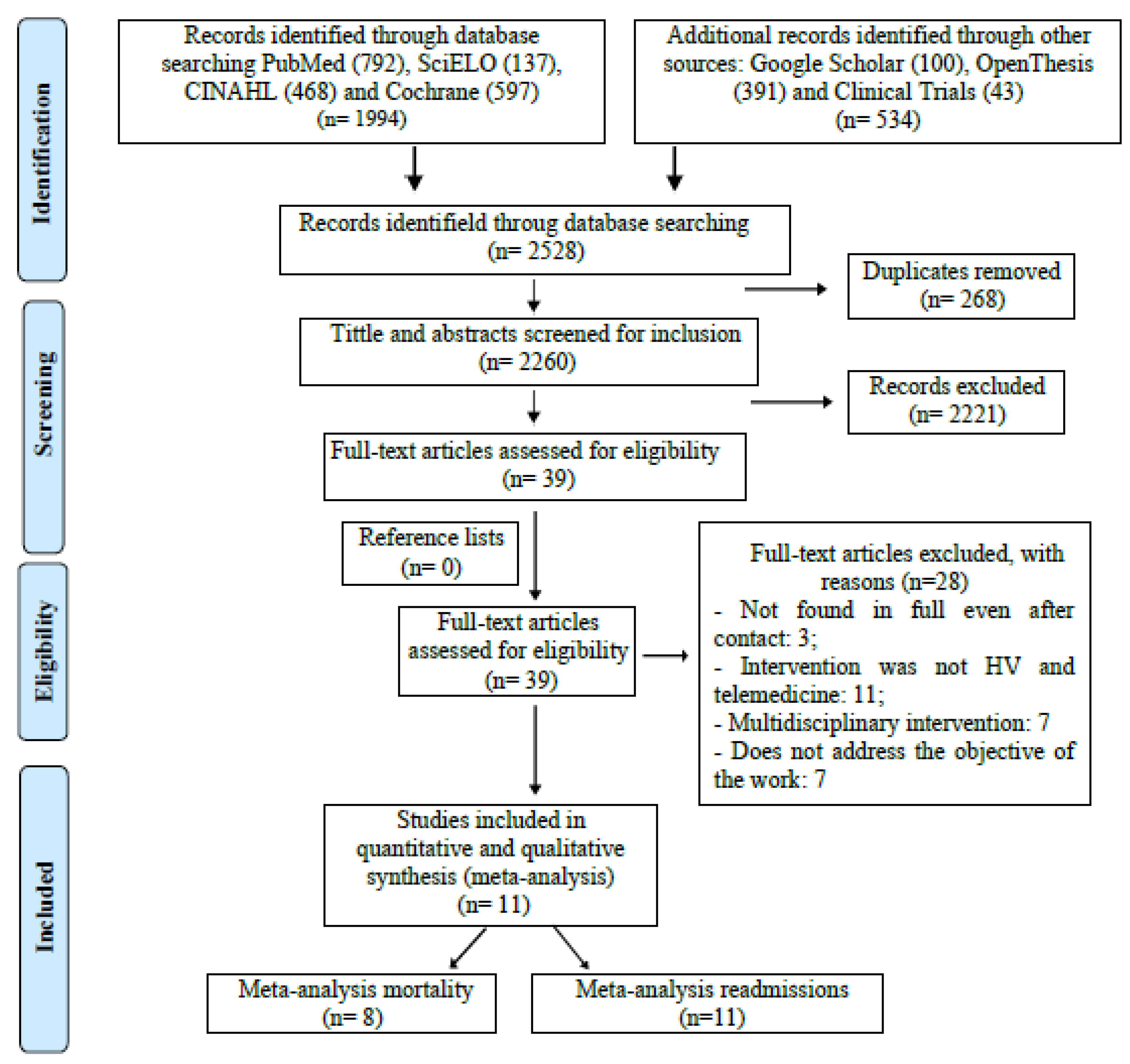
3.1. Included Studies
3.2. Study Characteristics
3.3. Risk of Bias
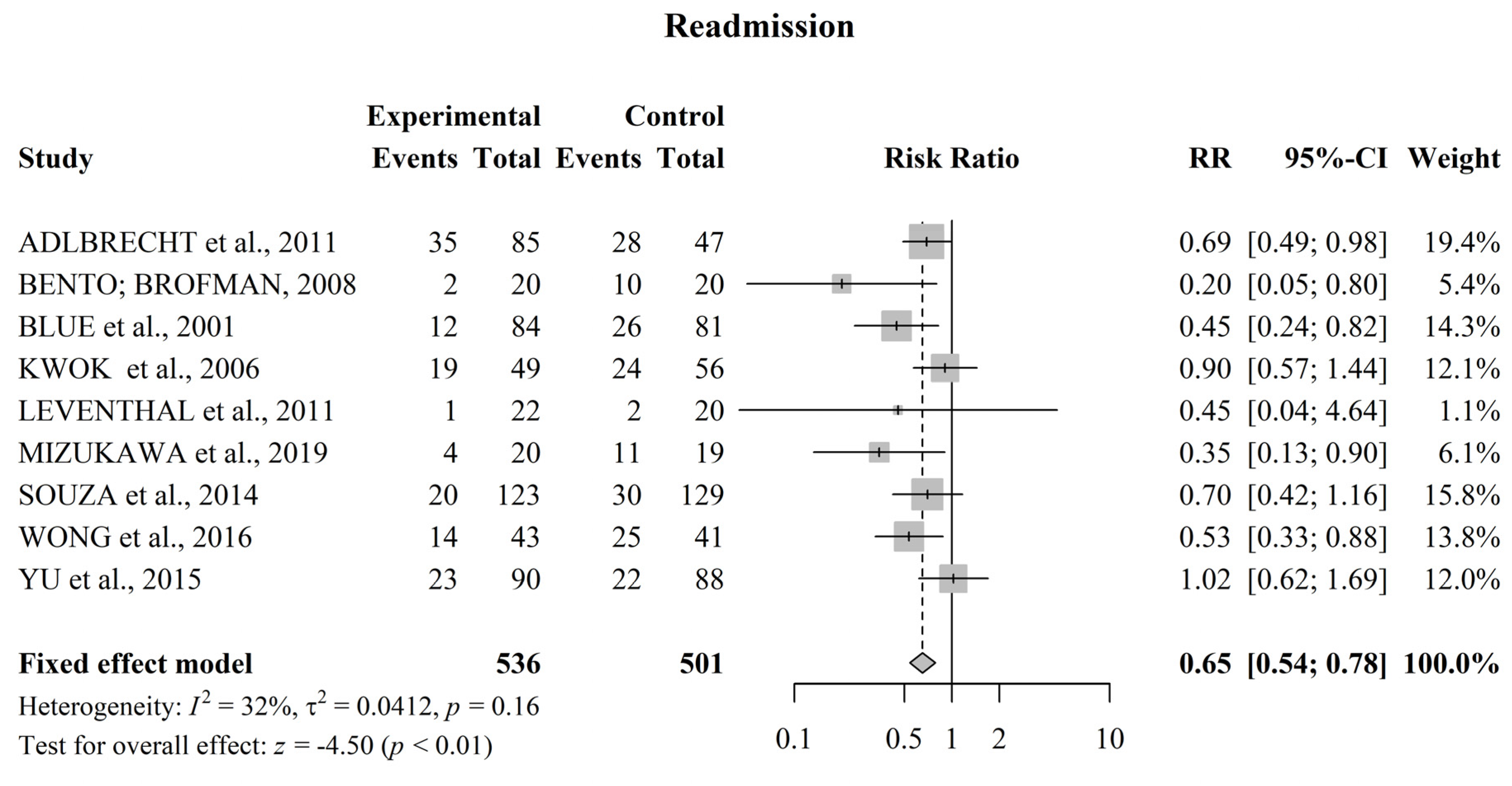
3.4. Meta-Analysis for Readmission
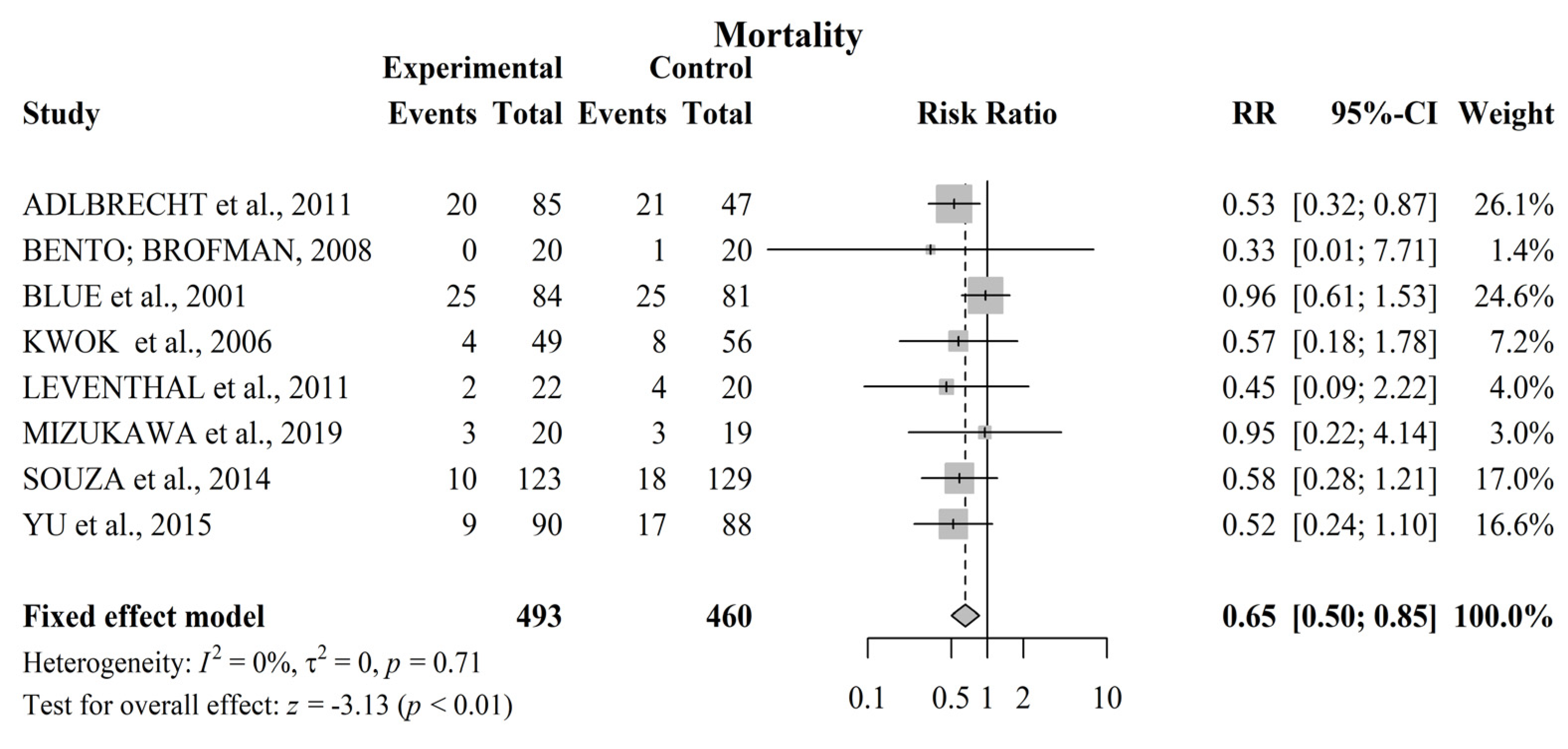
3.5. Meta-Analysis for Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| BASE | Search Strategy |
|---|---|
| PubMed | (((“Heart Failure”[Mesh] OR “Heart Failure” OR “Cardiac Failure” OR “Heart Decompensation” OR “Heart Failure, Right Sided” OR “Right-Sided Heart Failure” OR “Right Sided Heart Failure” OR “Myocardial Failure” OR “Congestive Heart Failure” OR “Heart Failure, Congestive” OR “Heart Failure, Left Sided” OR “Left Sided Heart Failure”)) AND ((“Patient Education as Topic”[Mesh] OR “Education, Patient” OR “Patient Education” OR “Education of Patients” OR “Self Care”[Mesh] OR “Self-Care” OR “Nursing Care”[Mesh] OR “Nursing Care” OR “Care, Nursing” OR “Management, Nursing Care” OR “Nursing Care Management” OR “educative intervention” OR “educational intervention” OR “nursing intervention”))) AND ((((clinical[Title/Abstract] AND trial[Title/Abstract]) OR clinical trials as topic[MeSH Terms] OR clinical trial[Publication Type] OR random*[Title/Abstract] OR random allocation[MeSH Terms] OR therapeutic use[MeSH Subheading]))) |
| SciELO | ((“Heart Failure” OR “Heart Failure, Systolic” OR “Heart Failure, Diastolic”) AND (“Nursing” OR “Nursing Assessment” OR “Nursing Care” OR “Cardiovascular Nursing” OR “Home Health Nursing” OR “Patient Care Planning”) AND (“Patient Education as topic” OR “Patient Education Handout”)) ((“Insuficiência cardíaca” OR “Insuficiência Cardíaca sistólica” OR “Insuficiência Cardíaca diastólica”)) AND ((enfermagem OR “Avaliação em Enfermagem” OR “Cuidados de Enfermagem” OR “Enfermagem Cardiovascular” OR “Enfermagem Domiciliar” OR “Planejamento de Assistência ao Paciente”)) AND ((“Educação de Pacientes como Assunto” OR “Prospecto para Educação de Pacientes”)) ((“Insuficiencia Cardíaca” OR “Insuficiencia Cardíaca Sistólica” OR “Insuficiencia Cardíaca Diastólica” AND (Enfermería OR “Evaluación en Enfermería” OR “Atención de Enfermería” OR “Enfermería Cardiovascular” OR “Cuidados de Enfermería en el Hogar” OR “Planificación de Atención al Paciente”) AND (“Educación del Paciente como Asunto” OR “Folleto Informativo para Pacientes”)) |
| CINAHL | ((MM “Heart Failure”) OR (MM “Heart Injuries”) OR (MM “Heart Hypertrophy”) OR (MM “Heart”) OR (MM “Heart Diseases”) OR (MH “Coronary Disease”) OR (MM “Cardiac Patients”) AND (MM “Education, Nursing, Associate”) OR (MM “Practical Nursing”) OR (MM “Nursing Protocols”) OR (MM “Nursing Interventions”) OR (MM “Nursing Care Plans”) OR (MM “Education, Nursing, Practical”) OR (MH “Nursing Practice”) AND (MM “Patient Education”) OR (MM “Patient Discharge Education”) OR (MM “Cardiac Patients”) OR (MM “Patient Orientation”)) |
| COCHRANE | (“Heart Failure” OR “Heart Failure” OR “Cardiac Failure” OR “Heart Decompensation” OR “Heart Failure, Right Sided” OR “Right-Sided Heart Failure” OR “Right Sided Heart Failure” OR “Myocardial Failure” OR “Congestive Heart Failure” OR “Heart Failure, Congestive” OR “Heart Failure, Left Sided” OR “Left Sided Heart Failure”) AND (“Patient Education as Topic” OR “Education, Patient” OR “Patient Education” OR “Education of Patients” OR “Self Care” OR “Self-Care”) AND (“Nursing Care” OR “Nursing Care” OR “Care, Nursing” OR “Management, Nursing Care” OR “Nursing Care Management” OR “educative intervention” OR “educational intervention” OR “nursing intervention”) |
| Google Scholar | (“Heart Failure”) and (“Nursing” or “Patient Education”) |
| Open Thesis | ((“Heart Failure”) AND (“Nurse” OR “Nursing” OR “Nurses”) AND (“Patient education” OR “Self-care”)) |
| Clinicaltrials.gov | “Nursing” and “Heart Failure” and “Patient Education” |
| Authors | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Professionals | Blinding of Outcome Evaluators | Incomplete Outcomes | Selective Outcome Report | Other Sources of Bias |
|---|---|---|---|---|---|---|---|
| Adlbrecht et al., 2011 [12] |  | |  | | | |  |
| Bento; Brofman, 2008 [13] | | | | | | | |
| Blue et al., 2001 [14] | | | | | | | |
| Kwok et al., 2006 [15] | | | | | | | |
| Leventhal et al., 2011 [16] | | | | | | | |
| Mizukawa et al., 2019 [17] | | | | | | | |
| Quinn, 2006 [18] | | | | | | | |
| Riegel et al., 2002 [19] | | | | | | | |
| Souza et al., 2014 [20] | | | | | | | |
| Wong et al., 2016 [21] | | | | | | | |
| Yu et al., 2015 [22] | | | | | | | |
References
- BocchiI, E.A.; BragaI, F.G.M.; FerreiraI, S.M.A.; Rohde, L.E.P.; de Oliveira, W.A.; de Almeida, D.R.; Moreir, M.d.C.V.; Bestetti, R.B.; Bordignon, S.; Azevedo, C.; et al. Diretriz Brasileira de Insuficiência Cardíaca Crônica. Arq. Bras. Cardiol. 2009, 93, 3–70. [Google Scholar]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [PubMed]
- Oscalices, M.I.L.; Okuno, M.F.P.; Lopes, M.C.B.T.; Campanharo, C.R.V.; Batista, R.E.A. Discharge guidance and telephone follow-up in the therapeutic adherence of heart failure: Randomized clinical trial. Rev. Lat. Am. Enferm. 2019, 27, e3159. [Google Scholar] [CrossRef] [PubMed]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.; Sato, N.; Shah, A.N.; et al. The Global Health and Economic Burden of Hospitalizations for Heart Failure. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y. Multidisciplinary management of heart failure just beginning in Japan. J. Cardiol. 2015, 66, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Barros e Silva, P.G.M.; Ribeiro, D.J.; Fernandes, V.A.; Rinaldi, D.; Ramos, D.; Okada, M. Initial Impact of a Disease Management Program on Heart Failure in a Private Cardiology Hospital. Rev. Bras. Cardiol. 2014, 27, 90–96. [Google Scholar]
- Ezekowitz, J.A.; O’Meara, E.; McDonald, M.A.; Abrams, H.; Chan, M.; Ducharme, A.; Giannetti, N.; Grzeslo, A.; Hamilton, P.G.; Heckman, G.A.; et al. Comprehensive update of the Canadian cardiovascular society guidelines for the management of heart failure. Can. J. Cardiol. 2017, 33, 1342–1433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohde, L.E.P.; Montera, M.W.; Bocchi, E.A.; Clausell, N.O.; Albuquerque, D.C.d.; Rassi, S.; Colafranceschi, A.S.; Freitas, A.F.d., Jr.; Ferraz, A.S.; Biolo, A.; et al. Coordinating committee on heart failure guideline. Brazilian guideline of chronic and acute heart failure. Arq. Bras. Cardiol. 2018, 111, 436–539. [Google Scholar]
- Azeka, E.; Jatene, M.B.; Jatene, I.B.; Horowitz, E.S.K.; Branco, K.C.; Neto, J.D.S.; Miura, N.; Mattos, S.; Afiune, J.Y.; Tanaka, A.C.; et al. Brazilian guideline of heart failure and heart transplantation, in fetus, children and adults with congenital heart disease, of the Brazilian Society of Cardiology. Arq. Bras. Cardiol. 2014, 103, 1–126. [Google Scholar] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Updated September 2020); John Wiley & Sons: Cochrane, AB, Canada, 2020. [Google Scholar]
- Adlbrecht, C.; Huelsmann, M.; Berger, R.; Moertl, D.; Strunk, G.; Oesterle, A.; Ahmadi, R.; Szucs, T.; Pacher, R. Cost analysis and cost-effectiveness of NT-proBNP-guided heart failure specialist care in addition to home-based nurse care. Eur. J. Clin. Investig. 2011, 41, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Bento, V.F.R.; Brofman, P.R.S. Impact of the nursing consultation on the frequency of hospitalizations in patients with heart failure in Curitiba, Parana State. Arq. Bras. Cardiol. 2009, 92, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Blue, L.; Lang, E.; McMurray, J.J.V.; Davie, A.P.; McDonagh, T.A.; Murdoch, D.R.; Petrie, M.C.; Connolly, E.; Norrie, J.; Round, C.E.; et al. Randomised controlled trial of specialist nurse intervention in heart failure. BMJ 2001, 323, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Kwok, T.; Lee, J.; Woo, J.; Lee, D.T.; Griffith, S. A randomized controlled trial of a community nurse-supported hospital discharge programme in older patients with chronic heart failure. J. Clin. Nurs. 2008, 1, 109–117. [Google Scholar] [CrossRef]
- Leventhal, M.E.; Denhaerynck, K.; Rocca, H.-P.B.-L.; Burnand, B.; Conca-Zeller, A.; Bernasconi, A.T.; Mahrer-Imhof, R.; Froelicher, E.S.; De Geest, S. Swiss Interdisciplinary Management Programme for Heart Failure (SWIM-HF): A randomised controlled trial study of an outpatient inter-professional management programme for heart failure patients in Switzerland. Swiss Med. Wkly. 2011, 141, w13171. [Google Scholar] [CrossRef] [PubMed]
- Mizukawa, M.; Moriyama, M.; Yamamoto, H.; Rahman, M.; Naka, M.; Kitagawa, T.; Kobayashi, S.; Oda, N.; Yasunobu, Y.; Tomiyama, M.; et al. Nurse-Led Collaborative Management Using Telemonitoring Improves Quality of Life and Prevention of Rehospitalization in Patients with Heart Failure. Int. Heart J. 2019, 60, 1293–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinn, C. Low-technology heart failure care in home health: Improving patient outcomes. Home Healthc. Now 2006, 8, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Carlson, B.; Kopp, Z.; LePetri, B.; Glaser, D.; Unger, A. Effect of a standardized nurse case-management telephone intervention on resource use in patients with chronic heart failure. Arch. Intern. Med. 2002, 6, 705–712. [Google Scholar] [CrossRef] [PubMed]
- de Souza, E.N.; Rohde, L.E.; Ruschel, K.B.; Mussi, C.M.; Beck-da-Silva, L.; Biolo, A.; Clausell, N.; Rabelo-Silva, E.R. A nurse-based strategy reduces heart failure morbidity in patients admitted for acute decompensated heart failure in Brazil: The HELEN-II clinical trial. Eur. J. Heart Fail. 2014, 9, 1002–1008. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.K.Y.; Ng, A.Y.M.; Lee, P.H.; Lam, P.-T.; Ng, J.S.C.; Ng, N.H.Y.; Sham, M.M.K. Effects of a transitional palliative care model on patients with end-stage heart failure: A randomised controlled trial. Heart 2016, 102, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.S.F.; Lee, D.T.F.; Stewart, S.; Thompson, D.R.; Choi, K.; Yu, C. Effect of Nurse-Implemented Transitional Care for Chinese Individuals with Chronic Heart Failure in Hong Kong: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1583–1593. [Google Scholar] [CrossRef] [PubMed]
- Van Spall, H.G.C.; Rahman, T.; Mytton, O.; Ramasundarahettige, C.; Ibrahim, Q.; Kabali, C.; Coppens, M.; Haynes, R.B.; Connolly, S. Comparative effectiveness of transitional care services in patients discharged from the hospital with heart failure: A systematic review and network meta-analysis. Eur. J. Heart Fail. 2017, 19, 1427–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slyer, J.T.; Concert, C.M.; Eusebio, A.M.; Rogers, M.E.; Singleton, J. A systematic review of the effectiveness of nurse coordinated transitioning of care on readmission rates for patients with heart failure. JBI Evid. Synth. 2011, 9, 464–490. [Google Scholar]
- Gandhi, S.; Mosleh, W.; Sharma, U.C.; Demers, C.; Farkouh, M.E.; Schwalm, J.-D. Multidisciplinary heart failure clinics are associated with lower heart failure hospitalization and mortality: Systematic review and meta-analysis. Can. J. Cardiol. 2017, 33, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Aliti, G.B.; Rabelo, E.R.; Domingues, F.B.; Clausell, N. Educational settings in the management of patients with heart failure. Rev. Lat. Am. Enferm. 2007, 15, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Strömberg, A. The crucial role of patient education in heart failure. Eur. J. Heart Fail. 2005, 3, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Joynt, K.E.; Jha, A.K. Thirty-day readmissions—Truth and consequences. N. Engl. J. Med. 2012, 15, 1366–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au, A.G.; McAlister, F.A.; Bakal, J.A.; Ezekowitz, J.; Kaul, P.; van Walraven, C. Predicting the risk of unplanned readmission or death within 30 days of discharge after a heart failure hospitalization. Am. Heart J. 2012, 164, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Sahay, A.; Kapoor, J.R.; Pham, M.X.; Massie, B. Divergent trends in survival and readmission following a hospitalization for heart failure in the Veterans Affairs health care system 2002 to 2006. J. Am. Coll. Cardiol. 2010, 56, 362–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, A.S.; Stevenson, L.W. Rehospitalization for heart failure: Predict or prevent? Circulation 2012, 126, 501–506. [Google Scholar] [CrossRef] [Green Version]
- do Amaral, D.R.; Rossi, M.B.; Lopes, C.T.; de Lima Lopes, J. Nonpharmacological interventions to improve quality of life in heart failure: An integrative review. Rev. Bras. Enferm. 2017, 70, 198–209. [Google Scholar]
- Pinheiro, R.J.; Viacava, F.; Travassos, C.; Brito, A.S. Gender, morbidity, access and utilization of health services in Brazil. Ciência Saúde Coletiva 2002, 7, 105–109. [Google Scholar]
- Dunbar, S.B.; Reilly, C.M.; Gary, R.; Higgins, M.K.; Culler, S.; Butts, B.; Butler, J. Randomized clinical trial of an integrated self-care intervention for persons with heart failure and diabetes: Quality of life and physical functioning outcomes. J. Card. Fail. 2015, 21, 719–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheorghiade, M.; Vaduganathan, M.; Fonarow, G.C.; Bonow, R.O. Rehospitalization for heart failure: Problems and perspectives. J. Am. Coll. Cardiol. 2013, 61, 391–403. [Google Scholar] [CrossRef]



| Author, Year and Country | Population (IG) (CG) | Sex | Mean Age | Intervention | Readmission/Re-Hospitalization | Follow-Up Time(HV and Telephone Contact) | Mortality | Main Findings | Limitations |
|---|---|---|---|---|---|---|---|---|---|
| Adlbrecht et al., 2011 (Austria) [12] | IG 85 CG 47 | ♀ 28% & ♂ 71% ♀ 29% & ♂ 70% | 72.6 73.7 | 4 HV: 1°, 3°, 6° & 12° month. Does not specify total or frequency of telephone contact. | IG 35 CG 28 | 18 months | IG 20 CG 21 | - IG with lower outcomes compared to CG: combined outcome of death or re-hospitalization (53% vs. 66%), number of deaths (24% vs. 45%), re-hospitalizations from any cause (75% vs. 83%) and HF (41% vs. 60%), re-hospitalization costs for any reason (12,391 vs. 12,450 euros) and by HF (5225 vs. 7109 euros), cost-effectiveness at one year of survival after discharge from non-HF readmission (0.83 euros/less in the IG) and by HF (26.36 euros/less in the IG). | - Does not report/establish telephone contact number; - Does not report the causes of re-hospitalization related to HF. |
| Bento; Brofman, 2008 (Brazil) [13] | IG 20 CG 20 | ♀ 35% & ♂ 65% ♀ 25% & ♂ 75% | 54.2 60.6 | HV monthly or biweekly as needed. Does not specify the total. Telephone contact biweekly. Does not specify the total. | IG 2CG 10 | Not reported | IG 0 CG 1 | - IG had a lower number of readmitted patients (2) and a lower frequency of hospitalizations (5) compared to the CG (10 and 22, respectively). | - Small sample. - Does not cite patient follow-up time and does not establish HV number and telephone contact. |
| Blue et al., 2001 (Scotland) [14] | IG 84 CG 81 | ♀ 36% & ♂64% ♀ 49% & ♂ 51% | 74.4 75.6 | HV: Does not specify the total. Telephone contact as needed. Does not specify the total. | IG 12 CG 26 | 12 months | IG 25 CG 25 | - IG with a lower number of readmissions for HF (12 vs. 26) and non-HF (47 vs. 49), length of hospital stay (8 × 9 days) and reduced risk of hospitalization (62%) compared to CG. | - Does not describe HV number and/or telephone contact. |
| Kwok et al., 2006 (China) [15] | IG 49 CG 56 | ♀ 55% & ♂ 45% ♀ 55% & ♂ 45% | 79.5 76.8 | 9 HV: weekly in the first month, the first in up to seven days after discharge and monthly in the remaining months. Telephone contacts as needed. | IG 19 CG 24 | 6 months | CG 4 IG 8 | - IG with lower outcomes compared to CG: unplanned readmission (19 vs. 24), health care costs (HK $5229 vs. HK $20,916) and physical limitation (44 m vs. 25 m); - Main cause of readmission was exacerbation of HF symptoms (52%). | - Moderate follow-up time; - Only included patients over 60 years old; - Small sample; - Does not specify the causes of readmissions by analyzed group. |
| Leventhal et al., 2011 (Switzerland) [16] | IG 22 CG 20 | ♀ 40% & ♂ 59% ♀ 35% & ♂ 65% | 76.7 77.6 | 1 HV: until 7 days after discharge. 17 Telephone contacts: weekly ×4, bimonthly ×4 and monthly ×6. | IG 01 CG 02 | 12 months | IG 02 CG 04 | - IG had better outcomes in relation to CG: death (2 vs. 4), HF readmission (1 vs. 2) and QoL. - CG had better outcomes in relation to IG in: number of readmissions for any cause (6 vs. 10) and for non-HF cardiac cause (2 vs. 3). | - Small sample; - Number of HV in relation to follow-up time |
| Mizukawa et al., 2019 (Japan) [17] | IG 20 CG 19 | ♀ 50% & ♂ 50% ♀47% & ♂ 53% | 70.5 74.5 | 6 HV: mensal. Telephone contacts as needed (162 in total). | IG 4 CG 11 | 24 months | IG 3 CG 3 | - IG had better outcomes in relation to CG: readmissions for cardiac cause (4 vs. 11) and non-cardiac cause (12 vs. 13), patients who had at least one readmission (1 vs. 7), less days of hospitalization (59 vs. 66); - IG improved QoL during follow-up (p = 0.002, p = 0.012, p = 0.003, p = 0.018); - IG improved self-efficacy (p < 0.001) and self-care behavior (p = 0.002). | - Short follow-up time; - Does not describe HV number and/or telephone contact. |
| Quinn, 2006 (USA) [18] | IG 17 CG 05 | ♀47% & ♂ 52% ♀ 60% & ♂ 40% | 76.5 76.2 | 8 HV: six in the 1st month, one in the 2nd and 3rd months. 4 telephone contacts: one in the 1st month and three in the 2nd month. | IG 2 CG 4 | 3 months | Not reported | - IG with report of decreased symptoms of the disease: angina (13.3%), dyspnea (9.7%) and fatigue (33.3%), fewer readmissions (29%) compared to CG (80%) and increase in QoL (from 20% good or excellent to 47%). | - Short follow-up time; - Small sample; - Non-fulfillment of HV strategy and established telephone contact; - Does not report cause of readmission. |
| Riegel et al., 2002 (USA) [19] | IG 130 CG 228 | ♀ 46% & ♂53% ♀ 53% & ♂ 46% | 72.5 74.6 | Total HV and frequency not reported. 17 telephone contacts: the first 5 days after discharge and the others varied. | IG 23 CG 63 | 6 months | Not reported | - IG with better outcomes in relation to CG in: number of hospitalizations per HF (23 vs. 63), non-HF (56 vs. 114), hospitalization costs (1192 vs. 2186 dollars), HF hospitalized days (1.1 vs. 2.1), non-HF hospitalized days (3.5 vs. 4.8), time to post- discharge hospitalization (129 vs. 116 days), multiple readmissions (17 vs. 52) and satisfaction with care (22.88 vs. 21.66). | - Selective outcome report (satisfaction and use of outpatient resources); - Does not report mortality rate; HV frequency; telephone contact pattern and the causes of readmissions. |
| Souza et al., 2014 (Brazil) [20] | IG 123 CG 129 | ♀ 39% & ♂ 61% ♀ 35% & ♂ 64% | 62.063.0 | 4 HV: one in up to 10 days after discharge and the others after 30, 60 and 120 days. 4 telephone contacts. Does not specify frequency. | IG 20 CG 30 | 6 months | IG 10 CG 18 | - IG with better baseline (55%) and final (71%) knowledge about HF in relation to CG (54 and 55, respectively); - IG with better baseline (35%) and final (23%) self-care assessment in relation to CG (34% and 30%, respectively); - IG with lower number of urgent visits (24), readmission for HF (20) or other causes (18) in relation to CG (35, 30 and 19, respectively). | - Does not report the cause of readmission. |
| Wong et al., 2016 (China) [21] | IG 43 CG 41 | ♀ 56% & ♂ 43% ♀ 39% & ♂ 61% | 78.3 78.4 | 4 HV: two in the first month, one each week, and monthly in the second and third months. 4 telephone contacts: two in the first month, one each week, monthly in the 2nd and 3rd months. | IG 14 CG 25 | 3 months | Not reported | - IG with best outcomes in relation to CG: number of readmission in 12 weeks (14 25), intensity of symptoms (23.97 vs. 32.39), functional status in palliative care (66.8 vs. 66.85), QoL (7.57 vs. 6.46), questionnaire on HF (5.26 vs. 4.47) and degree of satisfaction of care (48.84 vs. 36.55). | - Included only patients in palliative care; - Does not report mortality value; - Limited description of the established therapeutic plan. |
| Yu et al., 2015 (china) [22] | IG 90 CG 88 | ♀ 46% & ♂ 53% ♀ 63% & ♂ 36% | 78.6 78.7 | 2 HV: one per week in the first month after discharge. 9 phone contacts: one every 2 weeks for 3 months and one every 2 months for 6 months. | IG 23 CG 22 | 9 months | IG 9 CG 17 | - IG had better outcomes than CG in: death (9 vs. 17), better survival without events (67% vs. 63%), total readmission time (229 vs. 408), days of hospitalization (7 vs. 11), self-care (maintenance 53 vs. 40 and self-confidence (39 vs. 26), QoL (70 vs. 59), knowledge (7.9 vs. 6.2), and self-assessment of health (visual scale 67.5 vs. 58, utility index 76 vs. 62) - IG had lower mortality risk (45%). | - Inclusion of patients aged 60 and over; - Does not provide clear data regarding the number of HV; - Does not report causes of readmissions. |
| Intervention Group Care | Control Group Care |
|---|---|
- Verification of vital signs (blood pressure, heart rate, temperature, respiratory rate and heart rate), peripheral oxygen saturation with pulse oximeter) and anthropometric measurements (weight, height, and body mass index); - Instructions regarding pharmacological treatment (dosage, schedule, indications, contraindications, therapeutic and side effects), clinical manifestations typical of the disease, signs of decompensation, eating habits with emphasis on fluid and salt restrictions and a diet rich in vegetables and fresh fruits, and regular and moderate physical activity.
| Follow-up was carried out with usual care according to the protocol of each institution in which the patient had been admitted. It was not described by the authors. Each countries might have different healthcare systems in this area |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, C.R.d.G.; de Menezes, A.F.; Ferrari, Y.A.C.; Oliveira, A.S.; Tavares, A.C.M.; Barreto, A.S.; Vieira, R.d.C.A.; da Fonseca, C.D.; Santana-Santos, E. Educational Nursing Intervention in Reducing Hospital Readmission and the Mortality of Patients with Heart Failure: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2022, 9, 420. https://doi.org/10.3390/jcdd9120420
Marques CRdG, de Menezes AF, Ferrari YAC, Oliveira AS, Tavares ACM, Barreto AS, Vieira RdCA, da Fonseca CD, Santana-Santos E. Educational Nursing Intervention in Reducing Hospital Readmission and the Mortality of Patients with Heart Failure: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2022; 9(12):420. https://doi.org/10.3390/jcdd9120420
Chicago/Turabian StyleMarques, Cleidinaldo Ribeiro de Goes, Andreia Freire de Menezes, Yasmim Anayr Costa Ferrari, Alan Santos Oliveira, Arthur César Melo Tavares, André Sales Barreto, Rita de Cássia Almeida Vieira, Cassiane Dezoti da Fonseca, and Eduesley Santana-Santos. 2022. "Educational Nursing Intervention in Reducing Hospital Readmission and the Mortality of Patients with Heart Failure: A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 9, no. 12: 420. https://doi.org/10.3390/jcdd9120420
APA StyleMarques, C. R. d. G., de Menezes, A. F., Ferrari, Y. A. C., Oliveira, A. S., Tavares, A. C. M., Barreto, A. S., Vieira, R. d. C. A., da Fonseca, C. D., & Santana-Santos, E. (2022). Educational Nursing Intervention in Reducing Hospital Readmission and the Mortality of Patients with Heart Failure: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease, 9(12), 420. https://doi.org/10.3390/jcdd9120420