
Novel Hybrid Treatment for Pulmonary Arterial Hypertension with or without Eisenmenger Syndrome: Double Lung Transplantation with Simultaneous Endovascular or Classic Surgical Closure of the Patent Ductus Arteriosus (PDA)

 ,
,  , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Case Presentation
2.1. Case 1
2.2. Case 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goerler, H.; Simon, A.; Gohrbandt, B.; Hagl, C.; Oppelt, P.; Weidemann, J.; Haverich, A.; Strueber, M. Heart-lung and lung transplantation in grown-up congenital heart disease: Long-term single centre experience. Eur. J. Cardiothorac. Surg. 2007, 32, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Hjortshøj, C.S.; Gilljam, T.; Dellgren, G.; Pentikäinen, M.O.; Möller, T.; Jensen, A.S.; Turanlahti, M.; Thilén, U.; Gustafsson, F.; Søndergaard, L. Outcome after heart-lung or lung transplantation in patients with Eisenmenger syndrome. Heart 2020, 106, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Fremes, S.E.; Patterson, G.A.; Williams, W.G.; Goldman, B.S.; Todd, T.R.T.; Maurer, J. Single lung transplantation and closure of patent ductus arteriosus for Eisenmenger’s syndrome. J. Thorac. Cardiovasc. Surg. 1990, 100, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Crowe, L.A.; Genecand, L.; Hachulla, A.-L.; Noble, S.; Beghetti, M.; Vallée, J.-P.; Lador, F. Non-invasive cardiac output determination using magnetic resonance imaging and thermodilution in pulmonary hypertension. J. Clin. Med. 2022, 11, 2717. [Google Scholar] [CrossRef]
- Ojrzyńska-Witek, N.; Marczak, M.; Mazurkiewicz, Ł.; Petryka-Mazurkiewicz, J.; Miłosz-Wieczorek, B.; Grzybowski, J.; Śpiewak, M. Role of cardiac magnetic resonance in heart failure of initially unknown etiology: A 10-year observational study. Kardiol. Pol. 2022, 80, 278–285. [Google Scholar] [CrossRef]
- Arvanitaki, A.; Giannakoulas, G.; Baumgartner, H.; Lammers, A.E. Eisenmenger syndrome: Diagnosis, prognosis and clinical management. Heart 2020, 106, 1638–1645. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.J. The patent ductus arteriosus in term infants, children, and adults. Semin. Perinatol. 2012, 36, 146–153. [Google Scholar] [CrossRef]
- Miller, D.P.; Farber, H.W. “Who’ll be the next in line?” The lung allocation score in patients with pulmonary arterial hypertension. J. Heart Lung. Transplant. 2013, 32, 1165–1167. [Google Scholar] [CrossRef]
- Chan, K.M. Idiopathic pulmonary arterial hypertension and equity of donor lung allocation in the era of the lung allocation score: Are we there yet? Am. J. Respir. Crit. Care Med. 2009, 180, 385–387. [Google Scholar] [CrossRef]
- Chen, H.; Shiboski, S.C.; Golden, J.A.; Gould, M.K.; Hays, S.R.; Hoopes, C.W.; De Marco, T. Impact of the lung allocation score on lung transplantation for pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2009, 180, 468–474. [Google Scholar] [CrossRef]
- Schaffer, J.M.; Singh, S.K.; Joyce, D.L.; Reitz, B.A.; Robbins, R.C.; Zamanian, R.T.; Mallidi, H.R. Transplantation for idiopathic pulmonary arterial hypertension: Improvement in the lung allocation score era. Circulation 2013, 127, 2503–2513. [Google Scholar] [CrossRef] [PubMed]
- Homsi, R.; Luetkens, J.A.; Skowasch, D.; Pizarro, C.; Sprinkart, A.M.; Gieseke, J.; Meyer Zur Heide Gen Meyer-Arend, J.; Schild, H.H.; Naehle, C.P. Left ventricular myocardial fibrosis, atrophy, and impaired contractility in patients with pulmonary arterial hypertension and a preserved left ventricular function: A cardiac magnetic resonance study. J. Thorac. Imaging 2017, 32, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Lewis, R.A.; Johns, C.S.; Swift, A.J.; Capener, D.; Rajaram, S.; Thompson, A.A.R.; Condliffe, R.; Elliot, C.A.; Charalampopoulos, A.; et al. Cardiovascular magnetic resonance predicts all-cause mortality in pulmonary hypertension associated with heart failure with preserved ejection fraction. Int. J. Cardiovasc. Imaging 2021, 37, 3019–3025. [Google Scholar] [CrossRef] [PubMed]
- Kjellström, B.; Lindholm, A.; Ostenfeld, E. Cardiac magnetic resonance imaging in pulmonary arterial hypertension: Ready for clinical practice and guidelines? Curr. Heart Fail. Rep. 2020, 17, 181–191. [Google Scholar] [CrossRef]
- Nowak, J.; Hudzik, B.; Jastrzȩbski, D.; Niedziela, J.T.; Rozentryt, P.; Wojarski, J.; Ochman, M.; Karolak, W.; Żegleń, S.; Gierlotka, M.; et al. Pulmonary hypertension in advanced lung diseases: Echocardiography as an important part of patient evaluation for lung transplantation. Clin. Respir. J. 2018, 12, 930–938. [Google Scholar] [CrossRef]
- Ius, F.; Tudorache, I.; Warnecke, G. Extracorporeal support, during and after lung transplantation: The history of an idea. J. Thorac. Dis. 2018, 10, 5131–5148. [Google Scholar] [CrossRef]
- Moser, B.; Jaksch, P.; Taghavi, S.; Muraközy, G.; Lang, G.; Hager, H.; Krenn, C.; Roth, G.; Faybik, P.; Bacher, A.; et al. Lung transplantation for idiopathic pulmonary arterial hypertension on intraoperative and postoperatively prolonged extracorporeal membrane oxygenation provides optimally controlled reperfusion and excellent outcome. Eur. J. Cardiothorac. Surg. 2018, 53, 178–185. [Google Scholar] [CrossRef]
- Benza, R.L.; Kanwar, M.K.; Raina, A.; Scott, J.V.; Zhao, C.L.; Selej, M.; Elliott, C.G.; Farber, H.W. Development and validation of an abridged version of the REVEAL 2.0 risk score calculator, REVEAL Lite 2, for use in patients with pulmonary arterial hypertension. Chest 2021, 159, 337–346. [Google Scholar] [CrossRef]
- Benza, R.L.; Gomberg-Maitland, M.; Miller, D.P.; Frost, A.; Frantz, R.P.; Foreman, A.J.; Badesch, D.B.; McGoon, M.D. The REVEAL Registry risk score calculator in patients newly diagnosed with pulmonary arterial hypertension. Chest 2012, 141, 354–362. [Google Scholar] [CrossRef]
- Shigemura, N.; Bhama, J.; Gries, C.J.; Kawamura, T.; Crespo, M.; Johnson, B.; Zaldonis, D.; Pilewski, J.; Toyoda, Y.; Bermudez, C. Lung transplantation in patients with prior cardiothoracic surgical procedures: Lung transplantation and prior cardiothoracic procedures. Am. J. Transplant. 2012, 12, 1249–1255. [Google Scholar] [CrossRef]
- Abrams, D.C.; Brodie, D.; Rosenzweig, E.B.; Burkart, K.M.; Agerstrand, C.L.; Bacchetta, M.D. Upper-body extracorporeal membrane oxygenation as a strategy in decompensated pulmonary arterial hypertension. Pulm. Circ. 2013, 3, 432–435. [Google Scholar] [CrossRef]
- Biscotti, M.; Bacchetta, M. The “sport model”: Extracorporeal membrane oxygenation using the subclavian artery. Ann. Thorac. Surg. 2014, 98, 1487–1489. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Shigeta, A.; Terada, J.; Tanabe, N.; Sugiura, T.; Sakao, S.; Taniguchi, K.; Oto, T.; Tatsumi, K. Severe thrombocytopenia in patients with idiopathic pulmonary arterial hypertension provided several strategies for lung transplantation. Pulm. Circ. 2020, 10, 2045894020969103. [Google Scholar] [CrossRef] [PubMed]
- Aytekin, M.; Aulak, K.S.; Haserodt, S.; Chakravarti, R.; Cody, J.; Minai, O.A.; Dweik, R.A. Abnormal platelet aggregation in idiopathic pulmonary arterial hypertension: Role of nitric oxide. Am. J. Physiol. Lung Cell Mol. Physiol. 2012, 302, L512–L520. [Google Scholar] [CrossRef]
- Friedman, E.A.; Ogletree, M.L.; Haddad, E.V.; Boutaud, O. Understanding the role of prostaglandin E2 in regulating human platelet activity in health and disease. Thromb. Res. 2015, 136, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Stącel, T.; Antończyk, R.; Latos, M.; Nęcki, M.; Przybyłowski, P.; Zembala, M.; Ochman, M.; Urlik, M. Extracorporeal membrane oxygenation as a postoperative left ventricle conditioning tool after lung transplantation in patients with primary pulmonary artery hypertension: First Polish experience. Transplant. Proc. 2020, 52, 2113–2117. [Google Scholar] [CrossRef]
- Hwalek, A.; Rosenheck, J.P.; Whitson, B.A. Lung transplantation for pulmonary hypertension. J. Thorac. Dis. 2021, 13, 6708–6716. [Google Scholar] [CrossRef]
- Quezada-Loaiza, C.A.; de Pablo Gafas, A.; Pérez, V.; Alonso, R.; Juarros, L.; Real, M.I.; López, E.; Cortes, M.; Meneses, J.C.; González, I.H.; et al. Lung transplantation in pulmonary hypertension: A multidisciplinary unit’s management experience. Transplant. Proc. 2018, 50, 1496–1503. [Google Scholar] [CrossRef]
- de Perrot, M.; Granton, J.T.; McRae, K.; Pierre, A.F.; Singer, L.G.; Waddell, T.K.; Keshavjee, S. Outcome of patients with pulmonary arterial hypertension referred for lung transplantation: A 14-year single-center experience. J. Thorac. Cardiovasc. Surg. 2012, 143, 910–918. [Google Scholar] [CrossRef]
- Kearney, K.; Lau, E.M.; Darley, D.; Romfh, A.; Bart, N.; Kotlyar, E.; Hayes, D.; Khush, K.; Keogh, A. Waitlist and post-transplant outcomes for Eisenmenger syndrome: A comparison of transplant strategies. J. Heart Lung. Transplant. 2021, 40, 841–849. [Google Scholar] [CrossRef]
- Weill, D.; Benden, C.; Corris, P.A.; Dark, J.H.; Davis, R.D.; Keshavjee, S.; Lederer, D.J.; Mulligan, M.J.; Patterson, G.A.; Singer, L.G.; et al. A consensus document for the selection of lung transplant candidates: 2014—An update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J. Heart Lung. Transplant. 2015, 34, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lala, A. Transplantation in end-stage pulmonary hypertension (Third International Right Heart Failure Summit, part 3). Pulm. Circ. 2014, 4, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Simon, A.R.; Welte, T.; Hoeper, M.M.; Meyer, A.; Tessmann, R.; Gohrbandt, B.; Gottlieb, J.; Haverich, A.; Strueber, M. Bridge to lung transplantation with the novel pumpless interventional lung assist device NovaLung. J. Thorac. Cardiovasc. Surg. 2006, 131, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Kapur, N.K.; Paruchuri, V.; Jagannathan, A.; Steinberg, D.; Chakrabarti, A.K.; Pinto, D.; Aghili, N.; Najjar, S.; Finley, J.; Orr, N.M.; et al. Mechanical circulatory support for right ventricular failure. JACC Heart Fail. 2013, 1, 127–134. [Google Scholar] [CrossRef]
- Punnoose, L.; Burkhoff, D.; Rich, S.; Horn, E.M. Right ventricular assist device in end-stage pulmonary arterial hypertension: Insights from a computational model of the cardiovascular system. Prog. Cardiovasc. Dis. 2012, 55, 234–243.e2. [Google Scholar] [CrossRef]
- Kotloff, R.M.; Thabut, G. Lung transplantation. Am. J. Respir. Crit. Care Med. 2011, 184, 159–171. [Google Scholar] [CrossRef]
- Humbert, M.; McLaughlin, V.; Gibbs, J.S.R.; Gomberg-Maitland, M.; Hoeper, M.M.; Preston, I.R.; Souza, R.; Waxman, A.; Escribano Subias, P.; Feldman, J.; et al. Sotatercept for the treatment of pulmonary arterial hypertension. N. Engl. J. Med. 2021, 384, 1204–1215. [Google Scholar] [CrossRef]
- Joshi, S.R.; Liu, J.; Bloom, T.; Karaca Atabay, E.; Kuo, T.-H.; Lee, M.; Belcheva, E.; Spaits, M.; Grenha, R.; Maguire, M.C.; et al. Sotatercept analog suppresses inflammation to reverse experimental pulmonary arterial hypertension. Sci. Rep. 2022, 12, 7803. [Google Scholar] [CrossRef]
- Janus, M.; Sławek-Szmyt, S.; Araszkiewicz, A.; Mularek-Kubzdela, T.; Lesiak, M.; Grygier, M. Atrial flow regulator as a bridge to lung transplant in a young patient with drug-resistant idiopathic pulmonary arterial hypertension. Kardiol. Pol. 2020, 78, 461–462. [Google Scholar] [CrossRef]
- Sivakumar, K.; Rohitraj, G.R.; Rajendran, M.; Thivianathan, N. Study of the effect of Occlutech Atrial Flow Regulator on symptoms, hemodynamics, and echocardiographic parameters in advanced pulmonary arterial hypertension. Pulm. Circ. 2021, 11, 2045894021989966. [Google Scholar] [CrossRef]
- Stącel, T.; Latos, M.; Urlik, M.; Nęcki, M.; Antończyk, R.; Hrapkowicz, T.; Kurzyna, M.; Ochman, M. Interventional and surgical treatments for pulmonary arterial hypertension. J. Clin. Med. 2021, 10, 3326. [Google Scholar] [CrossRef] [PubMed]
- The Prophet Trial-Pilot Study to Assess Safety and Efficacy of a Novel Atrial Flow Regulator (AFR) in Patients With Pulmonary Hypertension. NCT03022851. Available online: https://clinicaltrials.gov/ct2/show/NCT03022851 (accessed on 18 January 2017).
- Benza, R.L.; Gomberg-Maitland, M.; Elliott, C.G.; Farber, H.W.; Foreman, A.J.; Frost, A.E.; McGoon, M.D.; Pasta, D.J.; Selej, M.; Burger, C.D.; et al. Predicting survival in patients with pulmonary arterial hypertension. Chest 2019, 156, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Daliento, L.; Somerville, J.; Presbitero, P.; Menti, L.; Brach-Prever, S.; Rizzoli, G.; Stone, S. Eisenmenger syndrome. Factors relating to deterioration and death. Eur. Heart J. 1998, 19, 1845–1855. [Google Scholar] [CrossRef] [PubMed]
- Wedemeyer, A.L.; Edson, J.R.; Krivit, W. Coagulation in cyanotic congenital heart disease. Am. J. Dis. Child. 1972, 124, 656–660. [Google Scholar] [CrossRef]
- Quatredeniers, M.; Mendes-Ferreira, P.; Santos-Ribeiro, D.; Nakhleh, M.K.; Ghigna, M.-R.; Cohen-Kaminsky, S.; Perros, F. Iron deficiency in pulmonary arterial hypertension: A deep dive into the mechanisms. Cells 2021, 10, 477. [Google Scholar] [CrossRef]
- Quatredeniers, M.; Montani, D.; Cohen-Solal, A.; Perros, F. Iron deficiency in pulmonary arterial hypertension: Perspectives. Pulm. Circ. 2021, 11, 20458940211021301. [Google Scholar] [CrossRef]
- Taylor, A.J.; Salerno, M.; Dharmakumar, R.; Jerosch-Herold, M. T1 mapping: Basic techniques and clinical applications. JACC Cardiovasc. Imaging 2016, 9, 67–81. [Google Scholar] [CrossRef]
- García-Álvarez, A.; García-Lunar, I.; Pereda, D.; Fernández-Jimenez, R.; Sánchez-González, J.; Mirelis, J.G.; Nuño-Ayala, M.; Sánchez-Quintana, D.; Fernández-Friera, L.; García-Ruiz, J.M.; et al. Association of myocardial T1-mapping CMR with hemodynamics and RV performance in pulmonary hypertension. JACC Cardiovasc. Imaging 2015, 8, 76–82. [Google Scholar] [CrossRef]
- Pereda, D.; García-Lunar, I.; Sierra, F.; Sánchez-Quintana, D.; Santiago, E.; Ballesteros, C.; Encalada, J.F.; Sánchez-González, J.; Fuster, V.; Ibáñez, B.; et al. Magnetic resonance characterization of cardiac adaptation and myocardial fibrosis in pulmonary hypertension secondary to systemic-to-pulmonary shunt. Circ. Cardiovasc. Imaging 2016, 9, e004566. [Google Scholar] [CrossRef]
- Cerro, M.J.; Abman, S.; Diaz, G.; Freudenthal, A.H.; Freudenthal, F.; Harikrishnan, S.; Haworth, S.G.; Ivy, D.; Lopes, A.A.; Raj, J.U.; et al. A consensus approach to the classification of pediatric pulmonary hypertensive vascular disease: Report from the PVRI Pediatric Taskforce, Panama 2011. Pulm. Circ. 2011, 1, 286–298. [Google Scholar] [CrossRef]
- Haworth, S.G.; Hislop, A.A. Treatment and survival in children with pulmonary arterial hypertension: The UK Pulmonary Hypertension Service for Children 2001-2006. Heart 2008, 95, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Kopeć, G.; Kurzyna, M.; Mroczek, E.; Chrzanowski, Ł.; Mularek-Kubzdela, T.; Skoczylas, I.; Kuśmierczyk, B.; Pruszczyk, P.; Błaszczak, P.; Lewicka, E.; et al. Database of Pulmonary Hypertension in the Polish Population (BNP-PL): Design of the registry. Kardiol. Pol. 2019, 77, 972–974. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. 1 | Referral and Qualification for LTx | Preoperative Conditioning, after Qualification | |
|---|---|---|---|
| At admission | Before surgery | ||
| LV EF (%) | 66 | 45 | 53 |
| IVC insp. (mm) | 18 | 25 | LoD |
| IVC exp. (mm) | 18 | 20 | LoD |
| RVSP (mmHg) | 107 | 125 | 126 |
| RVFAC (%) | 17 | 13 | LoD |
| Ring TV (mm) | LoD | 55 | 50 |
| TAPSE (mm) | 14 | 8 | 11 |
| Pericardial effusion | NO | YES | NO |
| Leftward ventricular septum shift | YES | YES | YES |
| Severe tricuspid valve regurgitation | NO | YES | YES |
| Laboratory Tests | ||||||
|---|---|---|---|---|---|---|
| Date | NT-proBNP (pg/mL) | Albumin (g/L) | Creatinine (µmol/L) | Cystatin C (mg/L) | eGFR (mL/min/1.73 m2) | INR |
| Referral | 4353 | 35 | 81 | LoD | >60 | 1.24 |
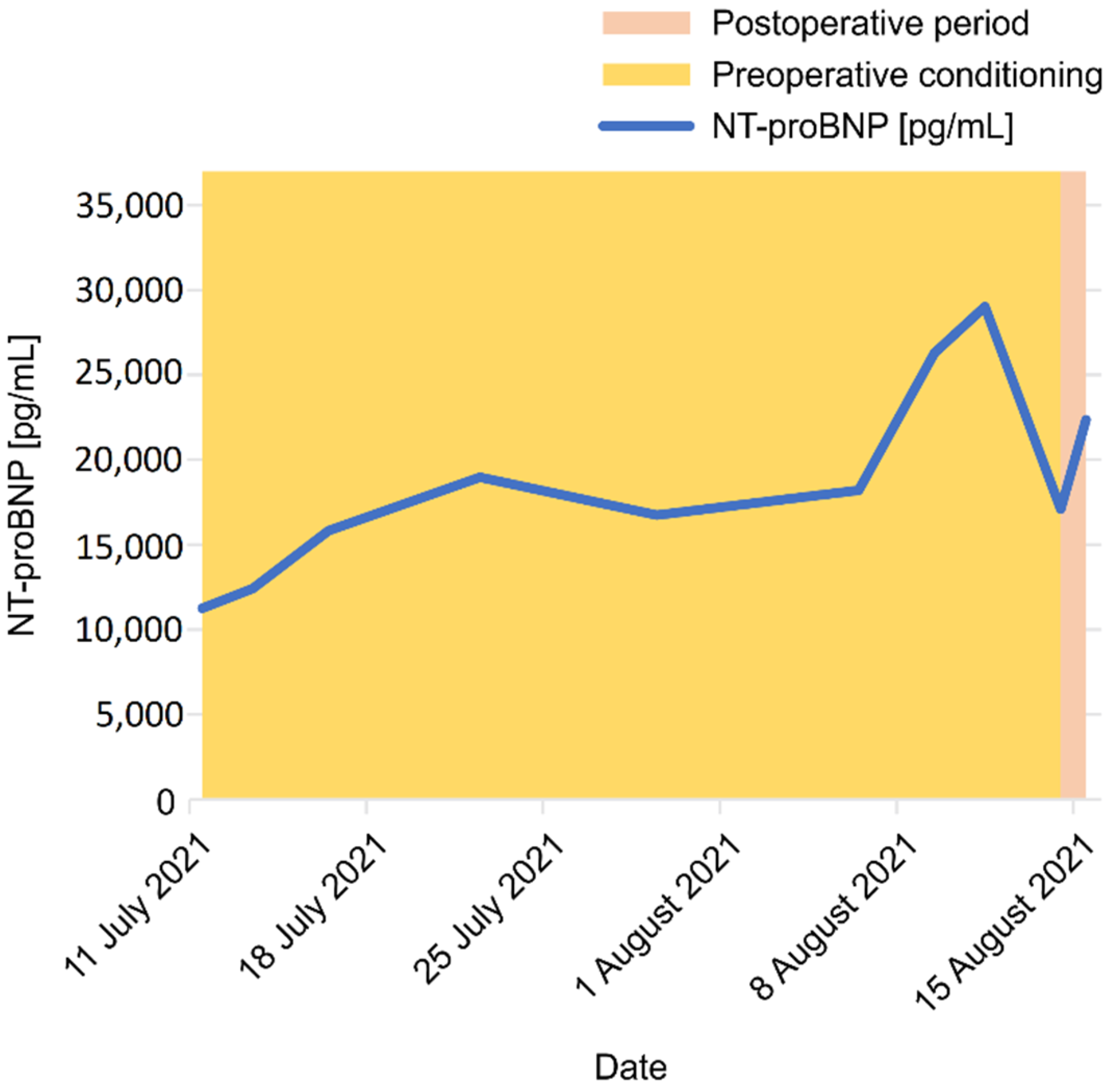
| Admission to LTC (for conditioning—bridging to LTx) | 11,251 | 39 | 60 | 1.08 | >60 | 1.42 |
| Before surgery | 29,028 | 51 | 113 | 1.88 | 56 | 1.34 |
| After surgery | 22,372 | 29 | 1351 | LoD | 45 1 | 2.86 |
| Patient 2 | Qualification 31 August 2021 | Before Surgery—Preoperative Conditioning | 1 Month after Surgery | 3 Months after Surgery | 6 Months after Surgery |
|---|---|---|---|---|---|
| LV EF (%) | 44 | 42 | 55 | 55 | 52 |
| IVC insp. (mm) | 23 | 22 | LoD | 14 | 7 |
| IVC exp. (mm) | 29 | 27 | LoD | 23 | 14 |
| RVSP (mmHg) | 105 | 115 | LoD | 36 | LoD |
| RVFAC (%) | 16 | 19 | LoD | 35 | 30 |
| Ring TV (mm) | 45 | 53 | LoD | LoD | LoD |
| TAPSE (mm) | 8 | 14 | 25 | 22 | 25 |
| Pericardial effusion (YES/NO) | YES | NO | trace separation of pericardial layers in systole | NO | NO |
| Leftward ventricular septum shift (YES/NO) | YES | YES | NO | NO | NO |
| Severe tricuspid valve regurgitation (YES/NO) | YES | YES | NO | NO | NO |
| Laboratory Tests | ||||||
|---|---|---|---|---|---|---|
| Date | NT-proBNP (pg/mL) | Albumin (g/L) | Creatinine (µmol/L) | Cystatin C (mg/L) | eGFR (mL/min/1.73 m2) | INR |
| Referral, admission to LTC (31 August 2021) | 14,135 | 45 | 168 | LoD | 31 | 1.39 |
| Before surgery | 1859 | 52 | 64 1 | 1.85 | >60 1 | 1.16 |
| After surgery (1st day) | 2450 | 47 | 95 | 1.77 | >60 | 1.2 |
| After surgery (1st week) | 26,278 | 38 | 106 | 1.69 | 53 | 1.12 |
| After surgery (1st month) | 2269 | 43 | 44 | LoD | >60 | 1.13 |
| After surgery (6th month) | 184 | 39 | 59 | 1.26 | >60 | 1.06 |
| Pulmonary Arterial Hypertension |
|---|
| 1.1 Idiopathic PAH |
| 1.2 Heritable PAH |
| 1.3 Drug- and toxin-induced |
| 1.4 PAH associated with: |
| Connective tissue disease |
| HIV infection |
| Portal hypertension |
| Congenital heart diseases |
| Schistosomiasis |
| 1.5 PAH long-term responders to CCBs |
| 1.6 PAH with overt features of PVOD/PCH |
| 1.7 Persistent PH of the newborn |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stącel, T.; Sybila, P.; Mędrala, A.; Ochman, M.; Latos, M.; Zawadzki, F.; Pióro, A.; Pasek, P.; Przybyłowski, P.; Hrapkowicz, T.; et al. Novel Hybrid Treatment for Pulmonary Arterial Hypertension with or without Eisenmenger Syndrome: Double Lung Transplantation with Simultaneous Endovascular or Classic Surgical Closure of the Patent Ductus Arteriosus (PDA). J. Cardiovasc. Dev. Dis. 2022, 9, 457. https://doi.org/10.3390/jcdd9120457
Stącel T, Sybila P, Mędrala A, Ochman M, Latos M, Zawadzki F, Pióro A, Pasek P, Przybyłowski P, Hrapkowicz T, et al. Novel Hybrid Treatment for Pulmonary Arterial Hypertension with or without Eisenmenger Syndrome: Double Lung Transplantation with Simultaneous Endovascular or Classic Surgical Closure of the Patent Ductus Arteriosus (PDA). Journal of Cardiovascular Development and Disease. 2022; 9(12):457. https://doi.org/10.3390/jcdd9120457
Chicago/Turabian StyleStącel, Tomasz, Paweł Sybila, Agata Mędrala, Marek Ochman, Magdalena Latos, Fryderyk Zawadzki, Anna Pióro, Piotr Pasek, Piotr Przybyłowski, Tomasz Hrapkowicz, and et al. 2022. "Novel Hybrid Treatment for Pulmonary Arterial Hypertension with or without Eisenmenger Syndrome: Double Lung Transplantation with Simultaneous Endovascular or Classic Surgical Closure of the Patent Ductus Arteriosus (PDA)" Journal of Cardiovascular Development and Disease 9, no. 12: 457. https://doi.org/10.3390/jcdd9120457
APA StyleStącel, T., Sybila, P., Mędrala, A., Ochman, M., Latos, M., Zawadzki, F., Pióro, A., Pasek, P., Przybyłowski, P., Hrapkowicz, T., Mroczek, E., Kuczaj, A., Kopeć, G., Fiszer, R., Pawlak, S., Stanjek-Cichoracka, A., & Urlik, M. (2022). Novel Hybrid Treatment for Pulmonary Arterial Hypertension with or without Eisenmenger Syndrome: Double Lung Transplantation with Simultaneous Endovascular or Classic Surgical Closure of the Patent Ductus Arteriosus (PDA). Journal of Cardiovascular Development and Disease, 9(12), 457. https://doi.org/10.3390/jcdd9120457