
Cardiac Complications of Hypertensive Emergency: Classification, Diagnosis and Management Challenges


Abstract
:1. Introduction
2. Epidemiology
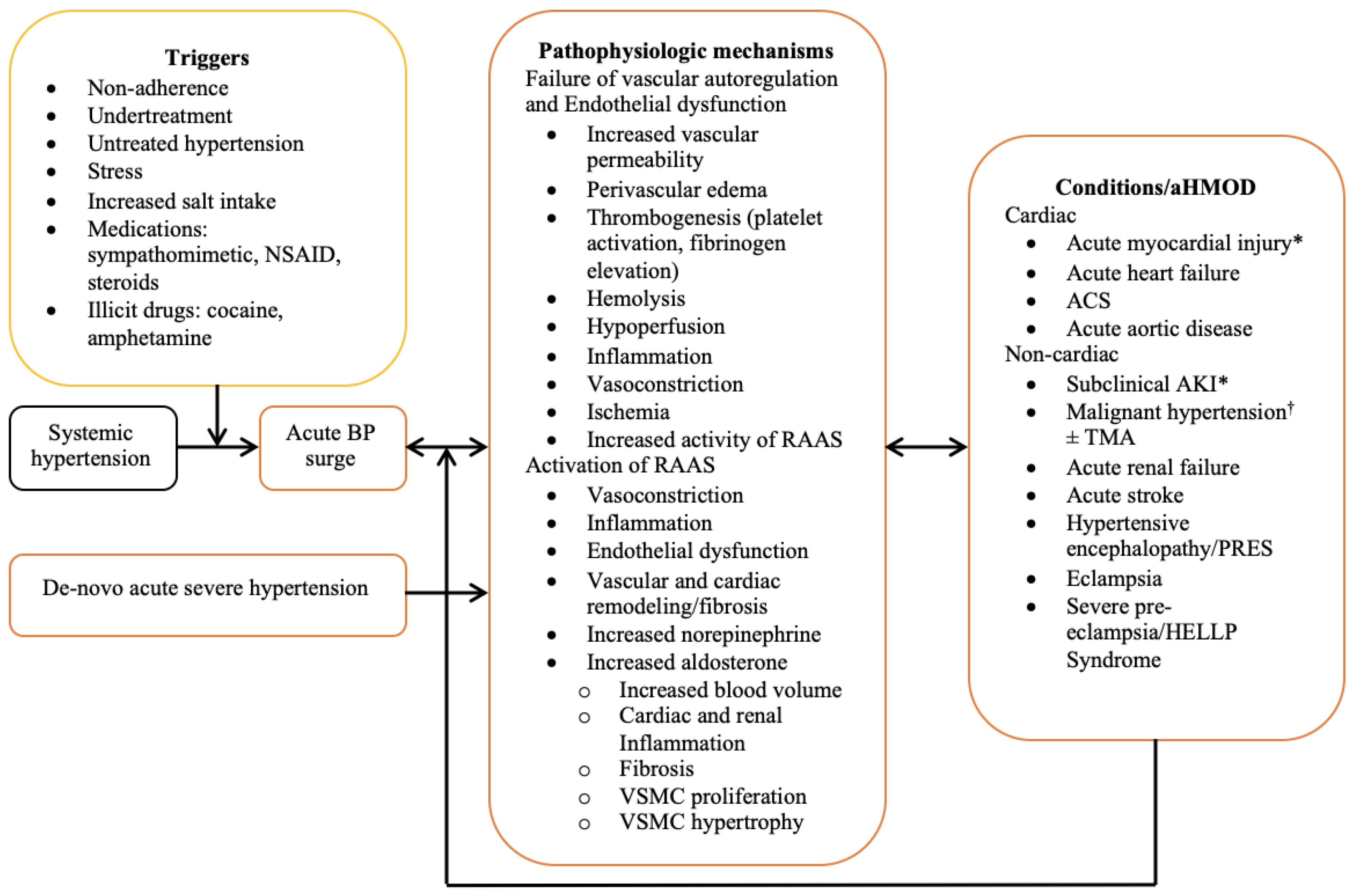
3. Pathophysiology
4. Specific Cardiac Complications of Hypertensive Emergency
4.1. Acute Heart Failure and Cardiogenic Pulmonary Edema
4.2. Acute Coronary Syndrome
4.3. Acute Myocardial Injury
4.4. Acute Aortic Syndrome
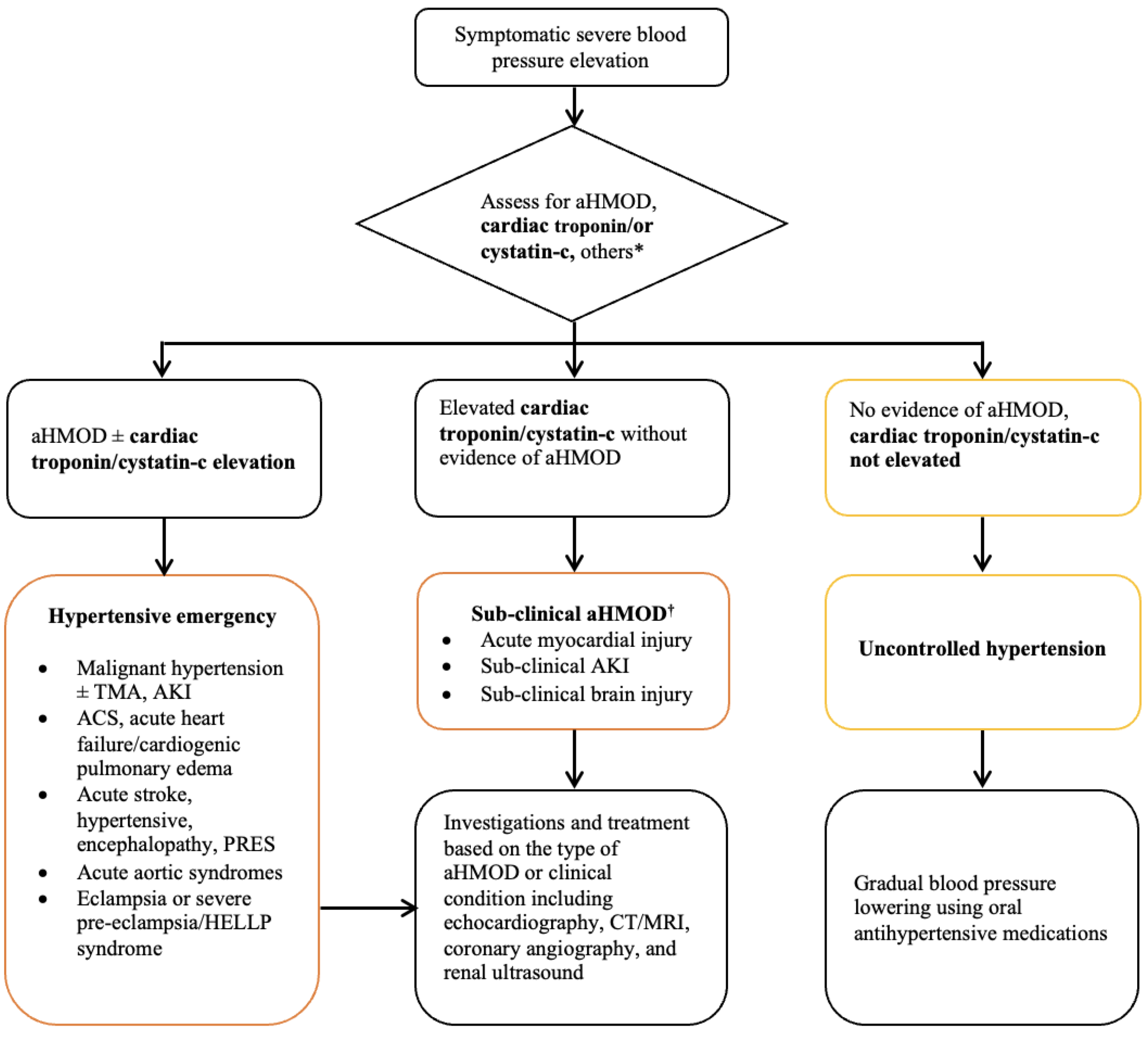
5. Challenges in Evaluation, Classifications, and Treatment of Cardiac Complications of Hypertensive Emergencies
5.1. Sub-Clinical Acute Target Organ Damage
5.2. Nomenclature and Classification
5.3. Treatment
5.4. Biomarkers of Subclinical Myocardial Injury
6. Recommendations for the Future
- i.
- Subclinical acute hypertensive target organ damage/dysfunction should be actively sought and added to the categories of acute hypertension-mediated organ damage (Table 2). This should include subclinical cardiac (acute myocardial injury), renal (subclinical acute kidney injury) and brain injury.
- ii.
- There is a need for consistency in the nomenclature and classification of acute hypertension-mediated organ damage. Acute heart failure should be used instead of cardiogenic pulmonary edema. The different types of myocardial infarction should be categorically identified as defined in the universal definition of myocardial infarction and included in studies reporting cardiac complications of hypertensive emergency.
- iii.
- There is the need for a properly designed study to: (i) accurately determine the true burden of acute hypertension-mediated organ damage in patients with hypertensive emergencies; (ii) determine the markers and long-term outcomes of subclinical acute hypertension-mediated organ damage; (iii) provide evidence-based strategies for immediate and long-term management of the different forms of acute hypertension-mediated organ damage; (iv) validate the use of oral medications in the treatment of hypertensive emergency; (v) develop well-defined strategies for the evaluation and management of acute myocardial injury and Type 2 myocardial infarction in patients with hypertensive emergencies.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arima, H.; Barzi, F.; Chalmers, J. Mortality patterns in hypertension. J. Hypertens. 2011, 29, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global Disparities of Hypertension Prevalence and Control. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Berry, K.M.; Parker, W.A.; Mchiza, Z.J.; Sewpaul, R.; Labadarios, D.; Rosen, S.; Stokes, A. Quantifying unmet need for hypertension care in South Africa through a care cascade: Evidence from the SANHANES, 2011–2012. BMJ Glob. Health 2017, 2, e000348. [Google Scholar] [CrossRef] [PubMed]
- van den Born, B.-J.H.; Lip, G.Y.; Brguljan-Hitij, J.; Cremer, A.; Segura, J.; Morales, E.; Mahfoud, F.; Amraoui, F.; Persu, A.; Kahan, T.; et al. ESC Council on hypertension position document on the management of hypertensive emergencies. Eur. Heart J. Cardiovasc. Pharmacother. 2019, 5, 37–46. [Google Scholar] [CrossRef]
- Mishima, E.; Funayama, Y.; Suzuki, T.; Mishima, F.; Nitta, F.; Toyohara, T.; Kikuchi, K.; Kunikata, H.; Hashimoto, J.; Miyazaki, M.; et al. Concurrent analogous organ damage in the brain, eyes, and kidneys in malignant hypertension: Reversible encephalopathy, serous retinal detachment, and proteinuria. Hypertens. Res. 2021, 44, 88–97. [Google Scholar] [CrossRef]
- Fragoulis, C.; Dimitriadis, K.; Siafi, E.; Iliakis, P.; Kasiakogias, A.; Kalos, T.; Leontsinis, I.; Andrikou, I.; Konstantinidis, D.; Nihoyannopoulos, P.; et al. Profile and management of hypertensive urgencies and emergencies in the emergency cardiology department of a tertiary hospital: A 12-month registry. Eur. J. Prev. Cardiol. 2022, 29, 194–201. [Google Scholar] [CrossRef]
- Pacheco, H.G.; Victorino, N.M.; Urquiza, J.P.N.; Castillo, A.A.; Herrera, U.J.; Mendoza, A.A.; Manzur, F.A.; de la Cruz, J.L.B.; Sánchez, C.M. Patients with hypertensive crises who are admitted to a coronary care unit: Clinical characteristics and outcomes. J. Clin. Hypertens. 2013, 15, 210–214. [Google Scholar] [CrossRef]
- Salvetti, M.; Paini, A.; Colonetti, E.; Tarozzi, L.; Bertacchini, F.; Aggiusti, C.; Stassaldi, D.; Rosei, C.A.; Rosei, E.A.; Muiesan, M.L. Hypertensive emergencies and urgencies: A single-centre experience in Northern Italy 2008–2015. J. Hypertens. 2020, 38, 52–58. [Google Scholar] [CrossRef]
- Astarita, A.; Covella, M.; Vallelonga, F.; Cesareo, M.; Totaro, S.; Ventre, L.; Apra, F.; Veglio, F.; Milan, A. Hypertensive emergencies and urgencies in emergency departments: A systematic review and meta-analysis. J. Hypertens. 2020, 38, 1203–1210. [Google Scholar] [CrossRef]
- Gonzalez, R.; Morales, E.; Segura, J.; Ruilope, L.M.; Praga, M. Long-term renal survival in malignant hypertension. Nephrol. Dial. Transplant. 2010, 25, 3266–3272. [Google Scholar] [CrossRef]
- Cremer, A.; Amraoui, F.; Lip, G.Y.H.; Morales, E.; Rubin, S.; Segura, J.; Van den Born, B.J.; Gosse, P. From malignant hypertension to hypertension-MOD: A modern definition for an old but still dangerous emergency. J. Hum. Hypertens. 2016, 30, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Kim, B.S.; Kim, H.-J.; Lee, J.H.; Shin, J.; Shin, J.-H. Clinical implications of cardiac troponin-I in patients with hypertensive crisis visiting the emergency department. Ann. Med. 2022, 54, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Janke, A.T.; McNaughton, C.D.; Brody, A.M.; Welch, R.D.; Levy, P.D. Trends in the Incidence of Hypertensive Emergencies in US Emergency Departments From 2006 to 2013. J. Am. Heart Assoc. 2020, 5, e004511. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Beevers, M.; Beevers, G. The failure of malignant hypertension to decline—A survey of 24 years experience in a multiracial population in England. J. Hypertens. 1994, 12, 1297–1305. Available online: http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=7868878&site=ehost-live&scope=site (accessed on 6 February 2022). [CrossRef]
- Zampaglione, B.; Pascale, C.; Marchisio, M.; Cavallo-Perin, P. Hypertensive urgencies and emergencies. Prevalence and clinical presentation. Hypertension 1996, 27, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Lane, D.A.; Lip, G.Y.H.; Beevers, D.G. Improving Survival of Malignant Hypertension Patients Over 40 Years. Am. J. Hypertens. 2009, 22, 1199–1204. [Google Scholar] [CrossRef]
- Martin, J.F.V.; Higashiama, E.; Garcia, E.; Luizon, M.R.; Cipullo, J.P. Hypertensive crisis profile. Prevalence and clinical presentation. Arq. Bras. Cardiol. 2004, 83, 130–131. [Google Scholar] [CrossRef]
- Rubin, S.; Cremer, A.; Boulestreau, R.; Rigothier, C.; Kuntz, S.; Gosse, P. Malignant hypertension: Diagnosis, treatment and prognosis with experience from the Bordeaux cohort. J. Hypertens. 2019, 37, 316–324. Available online: https://journals.lww.com/jhypertension/Fulltext/2019/02000/Malignant_hypertension__diagnosis,_treatment_and.13.aspx (accessed on 8 February 2022). [CrossRef]
- Nkoke, C.; Noubiap, J.J.; Dzudie, A.; Jingi, M.A.; Njume, D.; Teuwafeu, D.; Aseneh, J.; Nkouonlack, C.; Menanga, A.; Kingue, S. Epidemiology of hypertensive crisis in the Buea Regional Hospital, Cameroon. J. Clin. Hypertens. 2020, 22, 2105–2110. [Google Scholar] [CrossRef]
- Guiga, H.; Decroux, C.; Michelet, P.; Loundou, A.; Cornand, D.; Silhol, F.; Vaisse, B.; Sarlon-Bartoli, G. Hospital and out-of-hospital mortality in 670 hypertensive emergencies and urgencies. J. Clin. Hypertens. 2017, 19, 1137–1142. [Google Scholar] [CrossRef]
- Vilela-Martin, J.F.; Vaz-de-Melo, R.O.; Kuniyoshi, C.H.; Abdo, A.N.R.; Yugar-Toledo, J.C. Hypertensive crisis: Clinical-epidemiological profile. Hypertens. Res. 2011, 34, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Acosta, G.; Amro, A.; Aguilar, R.; Abusnina, W.; Bhardwaj, N.; Koromia, G.A.; Studeny, M.; Irfan, A. Clinical Determinants of Myocardial Injury, Detectable and Serial Troponin Levels among Patients with Hypertensive Crisis. Cureus 2020, 12, e6787. [Google Scholar] [CrossRef] [PubMed]
- Pattanshetty, D.J.; Bhat, P.K.; Aneja, A.; Pillai, D.P. Elevated troponin predicts long-term adverse cardiovascular outcomes in hypertensive crisis: A retrospective study. J. Hypertens. 2012, 30, 2410–2415. [Google Scholar] [CrossRef]
- Beishon, L.C.; Minhas, J.S. Cerebral Autoregulation and Neurovascular Coupling in Acute and Chronic Stroke. Front. Neurol. 2021, 12, 720770. [Google Scholar] [CrossRef] [PubMed]
- Strandgaard, S.; Haunsø, S. Why does antihypertensive treatment prevent stroke but not myocardial infarction? Lancet 1987, 330, 658–661. [Google Scholar] [CrossRef]
- Westerhof, N.; Boer, C.; Lamberts, R.R.; Sipkema, P. Cross-Talk Between Cardiac Muscle and Coronary Vasculature. Physiol. Rev. 2006, 86, 1263–1308. [Google Scholar] [CrossRef]
- van den Born, B.-J.H.; Löwenberg, E.C.; van der Hoeven, N.V.; de Laat, B.; Meijers, J.C.; Levi, M.; van Montfrans, G.A. Endothelial dysfunction, platelet activation, thrombogenesis and fibrinolysis in patients with hypertensive crisis. J. Hypertens. 2011, 29, 922–927. [Google Scholar] [CrossRef]
- van den Born, B.-J.H.; Koopmans, R.P.; van Montfrans, G.A. The renin-angiotensin system in malignant hypertension revisited: Plasma renin activity, microangiopathic hemolysis, and renal failure in malignant hypertension. Am. J. Hypertens. 2007, 20, 900–906. [Google Scholar] [CrossRef]
- te Riet, L.; van Esch, J.H.M.; Roks, A.J.M.; van den Meiracker, A.H.; Danser, A.H.J. Hypertension: Renin-angiotensin-aldosterone system alterations. Circ. Res. 2015, 116, 960–975. [Google Scholar] [CrossRef]
- Rocha, R.; Stier, C.T., Jr.; Kifor, I.; Ochoa-Maya, M.R.; Rennke, H.G.; Williams, G.H.; Adler, G.K. Aldosterone: A Mediator of Myocardial Necrosis and Renal Arteriopathy. Endocrinology 2000, 141, 3871–3878. [Google Scholar] [CrossRef]
- Koenig, J.B.; Jaffe, I.Z. Direct Role for Smooth Muscle Cell Mineralocorticoid Receptors in Vascular Remodeling: Novel Mechanisms and Clinical Implications. Curr. Hypertens. Rep. 2014, 16, 427. [Google Scholar] [CrossRef] [PubMed]
- Kusche-Vihrog, K.; Jeggle, P.; Oberleithner, H. The role of ENaC in vascular endothelium. Pflügers Arch. Eur. J. Physiol. 2014, 466, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Galmiche, G.; Pizard, A.; Gueret, A.; El Moghrabi, S.; Ouvrard-Pascaud, A.; Berger, S.; Challande, P.; Jaffe, I.Z.; Labat, C.; Lacolley, P. Smooth Muscle Cell Mineralocorticoid Receptors Are Mandatory for Aldosterone–Salt to Induce Vascular Stiffness. Hypertension 2014, 63, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, K. Renin-Angiotensin System and Sympathetic Neurotransmitter Release in the Central Nervous System of Hypertension. Int. J. Hypertens. 2012, 2012, 1–11. [Google Scholar] [CrossRef]
- Gustafsson, F. Hypertensive arteriolar necrosis revisited. Blood Press 1997, 6, 71–77. [Google Scholar] [CrossRef]
- Kincaid-Smith, P.; McMicheal, J.; Murphy, E.A. The clinical course and pathology of hypertension with papilloedema (malignant hypertension). QJM Int. J. Med. 1958, 27, 117–154. [Google Scholar]
- Olsen, F. Acute hypertensive damage of arterial vessels of the heart. Acta Pathol. Microbiol. Scand. Sect. A Pathol. 1978, 86, 199–200. [Google Scholar] [CrossRef]
- Viau, D.M.; Sala-Mercado, J.A.; Spranger, M.D.; O’Leary, D.S.; Levy, P.D. The pathophysiology of hypertensive acute heart failure. Heart 2015, 101, 1861–1867. [Google Scholar] [CrossRef]
- D’Aloia, A.; Fiorina, C.; Vizzardi, E.; Faggiano, P.; Dei Cas, L. Hypertensive crisis and acute, reversible, left ventricular systolic dysfunction: A case report. Eur. J. Heart Fail. 2002, 4, 655–660. [Google Scholar] [CrossRef]
- Jularic, M.; Cupa, J.; Rosenberg, M.; Frey, N.; Langer, C. Takotsubo cardiomyopathy in complicated Pickering syndrome: Endovascular therapy of an occluded renal artery. Clinical Research in Cardiology 2014, 103, 759–761. [Google Scholar] [CrossRef]
- Chiang, Y.-L.; Chen, P.-C.; Lee, C.-C.; Chua, S.-K. Adrenal pheochromocytoma presenting with Takotsubo-pattern cardiomyopathy and acute heart failure. Medicine 2016, 95, e4846. [Google Scholar] [CrossRef] [PubMed]
- ’Rosanna, V. Postoperative Takotsubo cardiomyopathy triggered by intraoperative fluid overload and acute hypertensive crisis. Rom. J. Anaesth. Intensive Care 2015, 21, 47–50. [Google Scholar]
- Alam, M.; Zhang, L.; Stampehl, M.; Lakkis, N.; Dokainish, H. Usefulness of Speckle Tracking Echocardiography in Hypertensive Crisis and the Effect of Medical Treatment. Am. J. Cardiol. 2013, 112, 260–265. [Google Scholar] [CrossRef]
- Cotter, G.; Moshkovitz, Y.; Kaluski, E.; Milo, O.; Nobikov, Y.; Schneeweiss, A.; Krakover, R.; Vered, Z. The role of cardiac power and systemic vascular resistance in the pathophysiology and diagnosis of patients with acute congestive heart failure. Eur. J. Heart Fail. 2003, 5, 443–451. [Google Scholar] [CrossRef]
- Heart Failure Society of America. Executive Summary: HFSA 2006 Comprehensive Heart Failure Practice Guideline. J. Card. Fail. 2006, 12, 10–38. [Google Scholar] [CrossRef] [PubMed]
- Peacock, F.; Amin, A.; Granger, C.B.; Pollack Jr, C.V.; Levy, P.; Nowak, R.; Kleinschmidt, K.; Varon, J.; Wyman, A.; Gore, J.M.; et al. Hypertensive heart failure: Patient characteristics, treatment, and outcomes. Am. J. Emerg. Med. 2011, 29, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Peacock IV, W.F.; De Marco, T.; Fonarow, G.C.; Diercks, D.; Wynne, J.; Apple, F.S.; Wu, A.H. Cardiac troponin and outcome in acute heart failure. N. Engl. J. Med. 2008, 358, 2117–2126. [Google Scholar] [CrossRef] [PubMed]
- Wettersten, N.; Maisel, A. Role of Cardiac Troponin Levels in Acute Heart Failure. Card. Fail. Rev. 2015, 1, 102. [Google Scholar] [CrossRef]
- Chapman, A.R.; Shah, A.S.; Lee, K.K.; Anand, A.; Francis, O.; Adamson, P.; McAllister, D.A.; Strachan, F.E.; Newby, D.E.; Mills, N.L. Long-Term Outcomes in Patients with Type 2 Myocardial Infarction and Myocardial Injury. Circulation 2018, 137, 1236–1245. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. and Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction. J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar]
- Bularga, A.; Hung, J.; Daghem, M.; Stewart, S.; Taggart, C.; Wereski, R.; Singh, T.; Meah, M.N.; Fujisawa, T.; Ferry, A.V.; et al. Coronary Artery and Cardiac Disease in Patients with Type 2 Myocardial Infarction: A Prospective Cohort Study. Circulation 2022, 145, 1188–1200. [Google Scholar] [CrossRef] [PubMed]
- Neri, E.; Toscano, T.; Papalia, U.; Frati, G.; Massetti, M.; Capannini, G.; Tucci, E.; Buklas, D.; Muzzi, L.; Oricchio, L.; et al. Proximal aortic dissection with coronary malperfusion: Presentation, management, and outcome. J. Thorac. Cardiovasc. Surg. 2001, 121, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Grossman, E. Should a Moratorium Be Placed on Sublingual Nifedipine Capsules Given for Hypertensive Emergencies and Pseudoemergencies? JAMA J. Am. Med. Assoc. 1996, 276, 1328. [Google Scholar] [CrossRef]
- Burton, T.J.; Wilkinson, I.B. The dangers of immediate-release nifedipine in the emergency treatment of hypertension. J. Hum. Hypertens. 2008, 22, 301–302. [Google Scholar] [CrossRef]
- Gibson, T. Blood pressure levels in acute myocardial infarction. Am. Heart J. 1978, 96, 475–480. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension global hypertension practice guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Maludum, O.; Shah, M.; Mezue, K.; Biso, S.; Rodriguez-Ziccardi, M.; Alnabelsi, T.; Nwakile, C.; Figueredo, V.M. Factors that influence decision for ischemic work-up in hypertensive emergency. Int. J. Cardiol. 2016, 214, 331–332. [Google Scholar] [CrossRef]
- Sarkisian, L.; Saaby, L.; Poulsen, T.S.; Gerke, O.; Jangaard, N.; Hosbond, S.; Diederichsen, A.C.; Thygesen, K.; Mickley, H. Clinical Characteristics and Outcomes of Patients with Myocardial Infarction, Myocardial Injury, and Nonelevated Troponins. Am. J. Med. 2016, 129, 446.e5–446.e21. [Google Scholar] [CrossRef]
- McCarthy, C. Potential Implications Related to Diagnosing Type 2 MI Versus Myocardial Injury; American College of Cardiology: Washington, DC, USA, 14 February 2020. [Google Scholar]
- McCarthy, C.; Murphy, S.; Cohen, J.A.; Rehman, S.; Jones-O’Connor, M.; Olshan, D.S.; Singh, A.; Vaduganathan, M.; Januzzi, J.L.; Wasfy, J.H. Misclassification of Myocardial Injury as Myocardial Infarction. JAMA Cardiol. 2019, 4, 460. [Google Scholar] [CrossRef]
- Cediel, G.; Sandoval, Y.; Sexter, A.; Carrasquer, A.; González-del-Hoyo, M.; Bonet, G.; Boqué, C.; Schulz, K.; Smith, S.W.; Bayes-Genis, A.; et al. Risk Estimation in Type 2 Myocardial Infarction and Myocardial Injury: The TARRACO Risk Score. Am. J. Med. 2019, 132, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, J.A.F.; Nieto, J.A.C.; Arguello, J.; Arias, M.R.G.; Benitez, J.R.; Aguilera, D.; Jaime, J.F. Triple acute aortic syndrome: Concomitant presentation of dissection, penetrating atherosclerotic ulcer and hematoma with adequate resolution through interventional therapy. J. Am. Coll. Cardiol. 2022, 79 (Suppl. 9), 3315. Available online: https://www.jacc.org/doi/full/10.1016/S0735-1097%2822%2904306-6 (accessed on 26 July 2022).
- Hagan, P.G.; Nienaber, C.A.; Isselbacher, E.M.; Bruckman, D.; Karavite, D.J.; Russman, P.L.; Evangelista, A.; Fattori, R.; Suzuki, T.; Oh, J.K.; et al. The International Registry of Acute Aortic Dissection (IRAD). JAMA 2000, 283, 897. [Google Scholar] [CrossRef]
- Melvinsdottir, I.H.; Lund, S.H.; Agnarsson, B.A.; Sigvaldason, K.; Gudbjartsson, T.; Geirsson, A. The incidence and mortality of acute thoracic aortic dissection: Results from a whole nation study. Eur. J. Cardio Thorac. Surg. 2016, 50, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.P.J.; Banerjee, A.; Fairhead, J.F.; Perkins, J.; Silver, L.E.; Rothwell, P.M. Population-Based Study of Incidence and Outcome of Acute Aortic Dissection and Premorbid Risk Factor Control. Circulation 2013, 127, 2031–2037. [Google Scholar] [CrossRef] [PubMed]
- Mészáros, I.; Morocz, J.; Szlavi, J.; Schmidt, J.; Tornoci, L.; Nagy, L.; Szép, L. Epidemiology and Clinicopathology of Aortic Dissection. Chest 2000, 117, 1271–1278. [Google Scholar] [CrossRef]
- Tsai, T.T.; Fattori, R.; Trimarchi, S.; Isselbacher, E.; Myrmel, T.; Evangelista, A.; Hutchison, S.; Sechtem, U.; Cooper, J.V.; Smith, D.E.; et al. Long-Term Survival in Patients Presenting with Type B Acute Aortic Dissection. Circulation 2006, 114, 2226–2231. [Google Scholar] [CrossRef]
- Brewster, R.; Gertler, D.; Moncure, J.; Gusberg, A.; Tilson, R.; Darling, D.; Hammond, C.; Megerman, G.; Abbot, J.; Cambria, W. Vascular complications associated with spontaneous aortic dissection. J. Vasc. Surg. 1988, 7, 199–209. [Google Scholar]
- Vrsalovic, M. Prognostic effect of cardiac troponin elevation in acute aortic dissection: A meta-analysis. Int. J. Cardiol. 2016, 214, 277–278. [Google Scholar] [CrossRef]
- Maisch, B.; Seferović, P.M.; Ristić, A.D.; Erbel, R.; Rienmüller, R.; Adler, Y.; Tomkowski, W.Z.; Thiene, G.; Yacoub, M.H.; Task Force on the Diagnosis and Management of Pricardial Diseases of the European Society of Cardiology. Guidelines on the Diagnosis and Management of Pericardial Diseases Executive SummaryThe Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Eur. Heart J. 2004, 25, 587–610. [Google Scholar] [CrossRef]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Barón-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C.; et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur. Heart J. 2015, 36, 2921–2964. [Google Scholar] [CrossRef]
- Marber, M.S.; Mills, N.L.; Morrow, D.A.; Mueller, C. Cardiac myosin-binding protein C as a biomarker of acute myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 963–965. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year, Country | Design | AHF (%) | AMI (%) | AAS (%) | Cumulative (%) | NIMI (%) | Comments |
|---|---|---|---|---|---|---|---|
| Fragoulis [6], 2021, Greece | Prospective | 58 | 22.6 | 2 | 82.6 | NR | National cardiac referral centre registry data. Potential for bias towards cardiac complications. |
| Rubin [18], 2019, France | Prospective | 31 | NR | NR | 31% | 63 | Excluded myocardial infarction from their cohorts and 63% had elevated troponin while 83% had left ventricular hypertrophy. |
| Zampaglione [15], 1996, Italy | Prospective | 36.8 | 12 | 2 | 50.8 | NR | Cerebral infarction was the most common acute hypertension-mediated organ damage. However, composite of cardiac complications occurred in 50.8%. |
| Kim [12], 2022, Korea | CS | NR | 40.5 | NR | 40.5 | 60.4 | Focused on prognostic role of cardiac troponin in acute severe hypertension. Elevated (occurred in 41.6%) and detectable (occurred in 36.5%) cardiac troponin associated with higher mortality at 3 years. |
| Guiga [20], 2017, France | CS | 37.4 | 13.8 | 1.8 | 53 | NR | Reported higher mortality in hypertensive emergency than hypertensive urgency (12.5 vs. 1.8%). |
| Salvetti [8], 2021, Italy 2008 data 2015 data | Prospective | 34 37.5 | 25 25 | 1 0.5 | 60 63 | NR NR | Excluded resuscitated cardiac arrest and patients requiring urgent cardiac catheterization. |
| Pacheco [7], 2103, Mexico | Prospective | 25.2 | 59.5 | 6.3 | 91 | NR | Their cohorts composed of a high-risk group admitted into coronary care unit. Reported high rate of acute coronary syndrome and acute aortic syndrome. |
| Martin [17], 2004, Brazil | Retrospective | 25 | 13 | 0 | 33 | NR | Reported unstable angina (5%) separately from myocardial infarction (8%). |
| Vilela-Martin [21], 2011, Brazil | CS | 30.7 | 25.1 | 3.5 | 47.2 | NR | Reported unstable angina (12.1%) separately from myocardial infarction (13%). |
| Nkoke [19], 2020, Cameroon | CS | 44.6 | 3.6 | 0 | 48.2 | NR | Myocardial infarction occurred in 3.6% of their cohorts. Low rate of detection of myocardial infarction may be related to lack of facilities including low rates of ECG and cardiac troponin assay. |
| Acosta [22], 2020, USA | Retrospective | NR | 1 | 0 | 1 | 15 | Assessed acute myocardial injury using serial cardiac troponin assay. Excluded acute coronary syndrome from their cohorts. |
| Pattanshetty [23], 2012, USA | Retrospective | 20.5 | 11.7 | 2.3 | 34.5 | NR | Obstructive coronary artery disease present in 76.5% of their cohorts with elevated cardiac troponin that had angiogram. |
| Acute hypertension mediated-organ damage |
| Acute heart failure/acute pulmonary edema * |
| Acute coronary syndrome * |
| ST-elevation myocardial infarction |
| Non-ST-elevation myocardial infarction |
| Unstable angina |
| Acute aortic syndrome |
| Acute aortic dissection * |
| Intramural hemorrhage/hematoma |
| Penetrating atherosclerotic aortic ulcer |
| Aortic aneurysm |
| Aortic rupture |
| Sub-clinical cardiac target organ injury § |
| Acute myocardial injury |
| Myocardial Injury | Type 2 Myocardial Infarction | Comment | |
|---|---|---|---|
| Definition | At least 1 cardiac troponin concentration above the 99th percentile URL without features of myocardial ischemia/infarction | Rise and/or fall in cardiac troponin level with at least 1 value above the 99th percentile URL with at least one of the following: (1) Symptoms of myocardial ischemia (2) New ischemic ECG changes (3) Development of pathological Q waves (4) Imaging evidence of new loss of viable myocardium or new ischemic RWMA. | • Signs and/or symptoms of myocardial ischemia/myocardial infarction may be atypical. • LVH limits the use of ECG repolarization abnormalities in detection of myocardial ischemia. |
| Mechanism of troponin rise | Myocardial strain, inflammation, apoptosis, and cell injury. | Myocardial infarction due to mismatch in myocardial oxygen supply–demand in the absence of atherothrombotic event. | Pathophysiologic mechanisms in hypertensive emergency involve inflammation and demand-supply mismatch [27,50]. Myocardial injury and Type 2 myocardial infarction can occur in hypertensive emergencies. |
| Management strategies | Undefined | Undefined | |
| Coronary anatomy and left ventricular function | Not systematically studied | CAD in 68% (obstructive in 30%), LVSD in 34% [51]. | Both predict the presence of coronary artery disease and MACE. |
| Outcomes | The similarities in outcome measures reflects shared pathophysiologic mechanisms. | ||
| In-hospital all-cause [61] | ~11% | ~9% | |
| Post-discharge 30-day [61] | ~7% | ~4% | |
| 5-year all-cause [49] | ~72% | ~63% | |
| 5-year MACE [49] | ~31% | ~30% | |
| 30-day readmission [61] | ~21% | ~21% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Talle, M.A.; Ngarande, E.; Doubell, A.F.; Herbst, P.G. Cardiac Complications of Hypertensive Emergency: Classification, Diagnosis and Management Challenges. J. Cardiovasc. Dev. Dis. 2022, 9, 276. https://doi.org/10.3390/jcdd9080276
Talle MA, Ngarande E, Doubell AF, Herbst PG. Cardiac Complications of Hypertensive Emergency: Classification, Diagnosis and Management Challenges. Journal of Cardiovascular Development and Disease. 2022; 9(8):276. https://doi.org/10.3390/jcdd9080276
Chicago/Turabian StyleTalle, Mohammed A., Ellen Ngarande, Anton F. Doubell, and Philip G. Herbst. 2022. "Cardiac Complications of Hypertensive Emergency: Classification, Diagnosis and Management Challenges" Journal of Cardiovascular Development and Disease 9, no. 8: 276. https://doi.org/10.3390/jcdd9080276
APA StyleTalle, M. A., Ngarande, E., Doubell, A. F., & Herbst, P. G. (2022). Cardiac Complications of Hypertensive Emergency: Classification, Diagnosis and Management Challenges. Journal of Cardiovascular Development and Disease, 9(8), 276. https://doi.org/10.3390/jcdd9080276