Nodular Lymphangitis (Sporotrichoid Lymphocutaneous Infections). Clues to Differential Diagnosis


Abstract
:1. Introduction
2. Sporotrichosis
3. Infections by Mycobacterium marinum and Other Mycobacteria
3.1. Nocardiosis
3.2. Mycetoma
3.3. Leishmaniasis
3.4. Tularemia
3.5. Bacillus
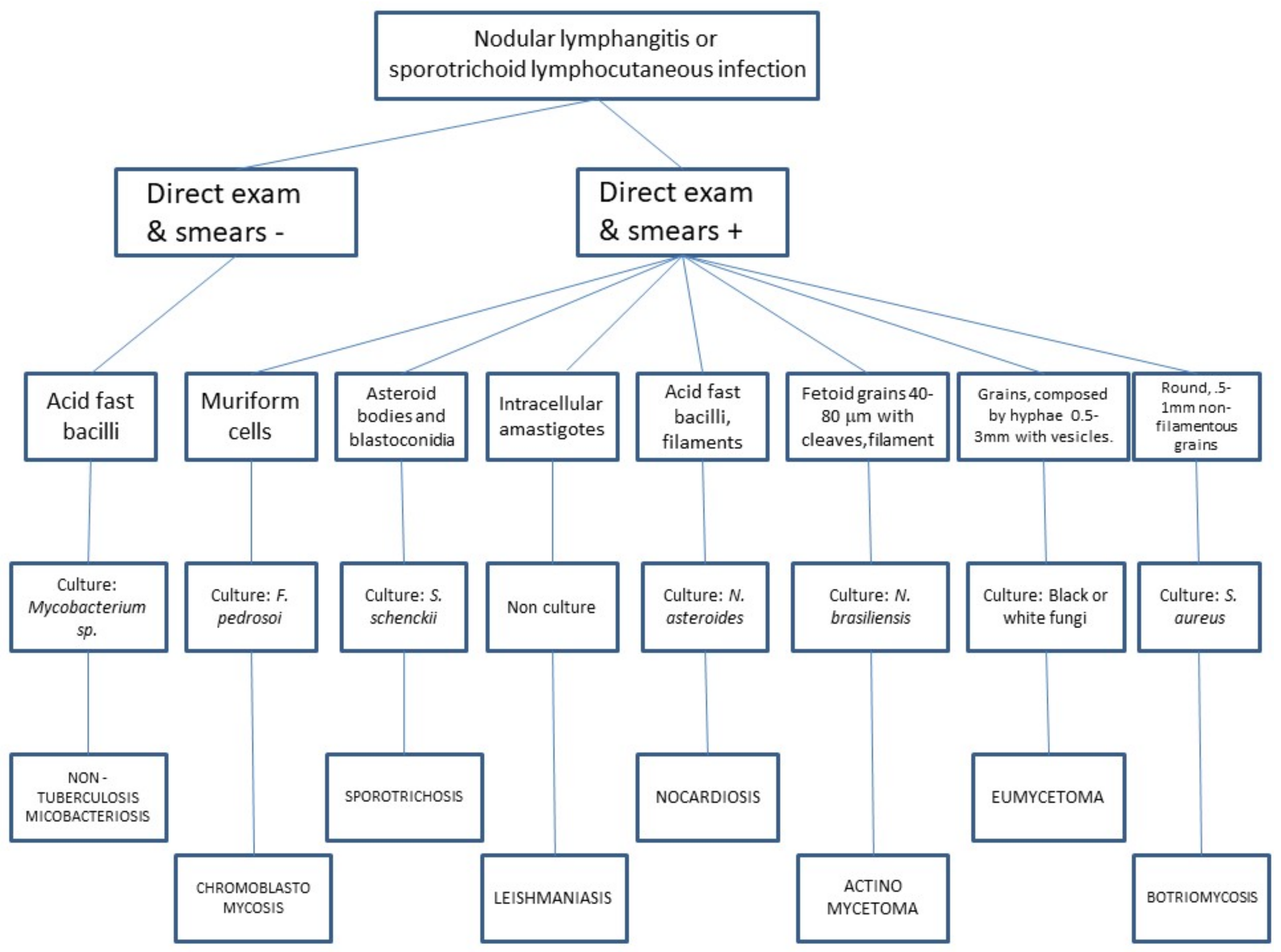
4. Clues to Differential Diagnosis
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Aragüés, M.; González-Arriba, A. Primary cutaneous infections due to Staphylococcus and Streptococcus. Actas Dermosifiliogr. 2007, 98, 4–14. [Google Scholar] [CrossRef]
- Heller, H.M.; Swartz, M.N. Nodular lymphangitis: Clinical features, differential diagnosis and management. Curr. Clin. Top. Infect. Dis. 1994, 14, 142–158. [Google Scholar] [PubMed]
- Kostman, J.R.; DiNubile, M.J. Nodular lymphangitis: A distinctive but often unrecognized syndrome. Ann. Intern. Med. 1993, 118, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Giordano, C.N.; Kalb, R.E.; Brass, C.; Lin, L.; Helm, T.N. Nodular lymphangitis: Report of a case with presentation of a diagnostic paradigm. Dermatol. Online J. 2010, 16, 1. [Google Scholar] [PubMed]
- Hashish, E.; Merwad, A.; Elgaml, S.; Amer, A.; Kamal, H.; Elsadek, A.; Marei, A.; Sitohy, M. Mycobacterium marinum infection in fish and man: Epidemiology, pathophysiology and management: A review. Vet. Q. 2018, 38, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Baradkar, V.P.; Mathur, M.; Kulkarni, S.D.; Kumar, S. Sporotrichoid pattern of cutaneous nocardiasis due to Nocardia asteroids. Indian J. Pathol. Microbiol. 2008, 51, 432–434. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, L.M.V.; Pimentel, M.I.F.; Conceição-Silva, F.; Vasconcellos, É.C.F.E.; Valete-Rosalino, C.M.; Lyra, M.R.; Salgueiro, M.M.; Saheki, M.N.; Madeira, M.F.; Mouta-Confort, E.; et al. Sporotrichoid leishmaniasis: A cross-sectional clinical, epidemiological and laboratory study in Rio de Janeiro State, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2017, 59, e33. [Google Scholar] [CrossRef] [PubMed]
- Maurin, M.; Gyuranecz, M. Tularaemia: Clinical aspects in Europe. Lancet Infect. Dis. 2016, 16, 113–124. [Google Scholar] [CrossRef]
- Pfisterer, R.M. An anthrax epidemic in Switzerland. Clinical, diagnostic and epidemiological aspects of a mostly forgotten disease. Schweiz. Med. Wochenschr. 1991, 121, 813–825. [Google Scholar] [PubMed]
- Rotemberg, V.; Valins, W.; Husan, S.; Grossman, M. Staphylococcus aureus sporotrichoid lymphangitis without bacteremia in a transplant recipient. Transpl. Inf. Dis. 2015, 17, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Smego, R.A., Jr.; Castiglia, M.; Asperilla, M.O. Lymphocutaneous syndrome. A review of non-sporothrix causes. Medicine 1999, 78, 38–63. [Google Scholar] [CrossRef] [PubMed]
- DiNubile, M.J. Nodular lymphangitis: A distinctive clinical entity with finite etiologies. Curr. Infect. Dis. Rep. 2008, 10, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Tobin, E.H.; Jih, W.W. Sporotrichoid lymphocutaneous infections: Etiology, diagnosis and therapy. Am. Fam. Phys. 2001, 63, 326–332. [Google Scholar]
- Barros, M.B.; de Almeida Paes, R.; Schubach, A.O. Sporothrixschenckii and Sporotrichosis. Clin. Microbiol. Rev. 2011, 24, 633–654. [Google Scholar] [CrossRef] [PubMed]
- Welsh, R.D. Sporotrichosis. J. Am. Vet. Med. Assoc. 2003, 223, 1123–1126. [Google Scholar] [CrossRef] [PubMed]
- Bonifaz, A.; Araiza, J.; Pérez-Mejía, A.; Ochoa, L.A.; Toriello, C. Intradermal test with sporotrichin in a community in the Sierra Norte de Puebla. Dermatol. Rev. Mex. 2013, 57, 428–432. [Google Scholar]
- Bonifaz, A.; Tirado-Sánchez, A. Cutaneous Disseminated and Extracutaneous Sporotrichosis: Current Status of a Complex Disease. J. Fungi 2017, 3, 6. [Google Scholar] [CrossRef] [PubMed]
- Bonifaz, A.; Vázquez-González, D. Sporotrichosis: An update. G. Ital. Dermatol. Venereol. 2010, 145, 659–673. [Google Scholar] [PubMed]
- Bonifaz, A.; Tirado-Sánchez, A.; Paredes-Solís, V.; Cepeda-Valdés, R.; González, G.M.; Treviño-Rangel, R.J.; Fierro-Arias, L. Cutaneous disseminated sporotrichosis: Clinical experience of 24 cases. J. Eur. Acad. Dermatol. Venereol. 2018, 32, e77–e79. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.Q.; Xu, X.G.; Zhang, M.; Jiang, P.; Zhou, X.Y.; Li, Z.Z.; Zhang, M.F. Sporotrichosis: Clinical and histopathological manifestations. Am. J. Dermatopathol. 2011, 33, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Orofino-Costa, R.; Macedo, P.M.; Rodrigues, A.M.; Bernardes-Engemann, A.R. Sporotrichosis: An update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics. An. Bras. Dermatol. 2017, 92, 606–620. [Google Scholar] [CrossRef] [PubMed]
- Fichman, V.; Valle, A.C.F.D.; De Macedo, P.M.; Freitas, D.F.S.; Oliveira, M.M.E.; Almeida-Paes, R.; Gutierrez-Galhardo, M.C. Cryosurgery for the treatment of cutaneous sporotrichosis in four pregnant women. PLOS Negl. Trop. Dis. 2018, 12, E0006434. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, S.; Zaini, F.; Kordbacheh, P.; Safara, M.; Heidari, M. Sporothrixschenckii complex in Iran: Molecular identification and antifungal susceptibility. Med. Mycol. 2016, 54, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Tirado, S.A.; Díaz, M.V.; Morales, P.N.; Bonifaz, T.A.; Ponce, O.R.M. Granuloma de las peceras (piscinas). Comunicación de trescasos. Dermatol. Rev. Mex. 2009, 53, 150–152. [Google Scholar]
- Uner, M.C.; Hasçelik, G.; Müştak, H.K. Antimicrobial susceptibilities of clinical Nocardia isolates identified by 16S rRNA gene sequence analysis. Mikrobiyol. Bul. 2016, 50, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Comellas, J.; Morales, M.; Granell, F. Nodular lymphangitis caused by Nocardiaasteroides. Enferm. Infecc. Microbiol. Clin. 2000, 18, 385–388. [Google Scholar] [PubMed]
- Bonifaz, A.; Tirado-Sánchez, A.; Calderón, L.; Saúl, A.; Araiza, J.; Hernández, M.; González, G.M.; Ponce, R.M. Mycetoma: Experience of 482 cases in a single center in Mexico. PLOS Negl. Trop. Dis. 2014, 8, e3102. [Google Scholar] [CrossRef] [PubMed]
- López-Martínez, R.; Méndez-Tovar, L.J.; Bonifaz, A.; Arenas, R.; Mayorga, J.; Welsh, O.; Vera-Cabrera, L.; Padilla-Desgarennes, M.C.; Contreras Pérez, C.; Chávez, G.; et al. Updateontheepidemiology of mycetoma in Mexico. A review of 3933 cases. Gac. Med. Mex. 2013, 149, 586–592. [Google Scholar] [PubMed]
- Boyce, Z.; Collins, N. Scedosporiumapiospermum: An unreported cause of fungal sporotrichoid-like lymphocutaneous infection in Australia and review of the literature. Australas. J. Dermatol. 2015, 56, e39–e42. [Google Scholar] [CrossRef] [PubMed]
- Heath, C.H.; Slavin, M.A.; Sorrell, T.C.; Handke, R.; Harun, A.; Phillips, M.; Nguyen, Q.; Delhaes, L.; Ellis, D.; Meyer, W.; et al. Australian Scedosporium Study Group. Population-based surveillance for scedosporiosis in Australia: Epidemiology, disease manifestations and emergence of Scedosporiumaurantiacum infection. Clin. Microbiol. Infect. 2009, 15, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Soares, V.B.; Almeida, A.S.; Sabroza, P.C.; Vargas, W.P. Epidemiological surveillance of tegumentaryleishmaniasis: Local territorial analysis. Rev. Saude Publica 2017, 51, 51. [Google Scholar] [CrossRef] [PubMed]
- Maleki, M.; Yousefi, M.; Bazzaz, S.M.M.; Tabassi, S.A.S.; Rakhshandeh, H.; Hamedi, S.S.; Haghighi, G. An overview of skin lesions adapted to Cutaneous Leishmaniasis in Persian Medicine. Electron. Phys. 2017, 9, 5854–5862. [Google Scholar] [CrossRef] [PubMed]
- Heras-Mosteiro, J.; Monge-Maillo, B.; Pinart, M.; Lopez Pereira, P.; Reveiz, L.; Garcia-Carrasco, E.; CampuzanoCuadrado, P.; Royuela, A.; Mendez Roman, I.; López-Vélez, R. Interventions for Old World cutaneous leishmaniasis. Cochrane Database Syst. Rev. 2017, 11, CD005067. [Google Scholar] [PubMed]
- Stidham, R.A.; Freeman, D.B.; von Tersch, R.L.; Sullivan, P.J.; Tostenson, S.D. Epidemiological Review of FrancisellaTularensis: A Case Study in the Complications of Dual Diagnoses. PLoS Curr. 2018, 10. [Google Scholar] [CrossRef]
- Berger, T.; Kassirer, M.; Aran, A.A. Injectional anthrax—New presentation of an old disease. Euro Surveill. 2014, 19, 20877. [Google Scholar] [CrossRef] [PubMed]
- Doganay, M.; Demiraslan, H. Human anthrax as a re-emerging disease. Recent Pat. Antiinfect. Drug Discov. 2015, 10, 10–29. [Google Scholar] [CrossRef] [PubMed]
- Head, B.M.; Rubinstein, E.; Meyers, A.F. Alternative pre-approved and novel therapies for the treatment of anthrax. BMC Infect. Dis. 2016, 16, 621. [Google Scholar] [CrossRef] [PubMed]
- Badali, H.; Bonifaz, A.; Barrón-Tapia, T.; Vázquez-González, D.; Estrada-Aguilar, L.; Oliveira, N.M.; Sobral Filho, J.F.; Guarro, J.; Meis, J.F.; De Hoog, G.S. Rhinocladiellaaquaspersa, proven agent of verrucous skin infection and a novel type ofchromoblastomycosis. Med. Mycol. 2010, 48, 696–703. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sporothrix schenckii |
| Blastomyces dermatitidis |
| Coccidioides immitis |
| Histoplasma capsulatum |
| Cryptococcus neoformans |
| Scedosporium apiospermum |
| Fusarium sp. |
| Scopulariopsis blochii |
| Nocardia sp. (N. brasiliensis, N. asteroides, N. otitidiscaviarum (caviae), N. transvalensis) |
| Pseudomonas (Burkholderia) pseudomallei |
| Francisella tularensis |
| Staphylococcus aureus |
| Streptococcus pyogenes |
| Bacillus anthracis |
| Mycobacterium sp. (M. marinum, M. chelonae, M. kansasii, M. avium-intracellulare, M. tuberculosis, M. fortuitum, M. flavescens, M. abscessus, M. haemophilum) |
| Leishmania (viannia) sp. (L. brasiliensis (guyanensis/panamensis), L. tropica, L. major) |
| Cowpox virus (Vaccinia virus) |
| Herpes simplex |
| Erysipelothrix rhusiopathiae |
| Agent | Geographical Distribution | Risk Factors (Sources) | Incubation Period | Primary Lesion | Pathology/Culture | Treatment |
|---|---|---|---|---|---|---|
| Sporothrix schenckii (complex) [2] | Tropical and subtropical América | Gardening (roses), corn crop, soil contact, sphagnum moss, animal scratches (cats) or bites. | 1 week–3 months | Painless ulcerated nodule. | Granulomatous infiltrate with asteroids bodies and elongated yeast/Culture (Sabouraud agar at 32 °C) | Itraconazole 200 mg/daily; SSKI 5 drops in water 3 times daily, increasing slowly to 40–50 drops 3 times daily as tolerated; terbinafine 250 mg bid. Duration: 2 months after the resolution of lesions |
| Mycobacterium marinum [5] | Worldwide | Aquariums, fish-handling (fresh and saltwater fish), swimming in oceans, lakes, pools. | 1–6 weeks | Mildly tender, often ulcerated nodule, with scant seropurulent exudate. | Suppurative granulomas/Culture on Lowenstein Jensen or Middlebrok agar at 30–32 °C. | Rifampin (15 mg/kg qd) + ethambutol (25 mg/kg qd); minocycline 100 mg bid; Rifampin (same dose) + clarithromycin (30 mg/kg qd); duration: 2–3 months after resolution of symptoms. |
| Nocardia brasiliensis/N. asteroids [6] | Worldwide | Soil exposure, botanicals, cat scratch. | 3 days–6 weeks | Tender nodules commonly ulcerated with mild to abundant purulent drainage. | Granulomas and sulphur granules, giant cells, abscess formation/Culture in most media. | TMP-SMX 160/800 mg tid; minocycline 200 mg bid. Duration: 3 months. Amikacin, surgical excision are also effective options. |
| Leishmania brasiliensis [7] | Central and South America | Residence in or travel to endemic areas. | 2–24 weeks | Painless, well-demarcated shallow ulcer with indurated borders. | Amastigotes within histiocytes/Culture on tissue biopsy or impression smears usually in Nicolle-Novy-Macneal medium or animals. | Stibogluconatesodium 20 mg/kg qd or meglumine antimonite 20 mg/kg qd; amphotericin B 0.25–1 mg/kg qd. Duration 20 days. Antimonials, itraconazole, ketoconazole and allopurinol are also effective options. |
| Francisella tularensis [8] | Northern hemisphere | Hunting and other rural outdoor activities, transmitted through ticks, deer flies, wild mammals (rabbits, squirrels, voles), cats. | 1–6 days | Painful ulcerated papule with suppuration. | Granulomatous reaction, multinucleated giant cells, epithelioid cells, neutrophils with focal necrosis/Serology, culture isolation with safety hood. | Streptomycin, tetracycline and gentamicin are useful treatment options. |
| Bacillus anthracis [9] | Worldwide | Exposure to infected animals, animal products, or spores in the soil. | Painless ulcer with vesicles, edema. | Gram stain and culture; serologic testing and punch biopsy at the edge of the lesion, examined by silver staining and immunohistochemical testing. | Penicillin G, ciprofloxacin and doxycycline. | |
| Staphylococcus aureus [10] | Worldwide | 4–10 days | Nodular lesions, frequently abscessed, with drainage of purulent fluid. | Botryomycotic grains/Culture on most media. | Antibiotics mainly beta lactams (Cefazolin, Cefadroxil). | |
| Coccidioides immitis/C. posadasii [11] | Southwest USA and Northern Mexico | Soil, laboratory contamination, thorns. | 1–4 weeks | Verrucous plaques and ulcerated nodules. | Chronic granulomatous infiltrate with plasma cells and spherules/Culture on Sabouraud agar at 32 °C. | Itraconazole, fluconazole, amphotericin B. |
| Blastomyces dermatitidis [11] | Worldwide usually North America | Soil, cat scratches, dog bites, laboratory contamination. | 1–5 weeks | Verrucous plaques and ulcerated nodules. | Chronic granulomatous infiltrate with plasma cells/Culture on Sabouraud agar at 32 °C. | Itraconazole, fluconazole, amphotericin B. |
| Histoplasma capsulatum [11] | Worldwide | Soil, birds, chickens, laboratory contamination. | 5–18 days | Umbilicated papules, ulcerated nodules with necrosis, vesicles (rash herpetiformis), pustules, acneiform rashes, verrucous plaques, psoriasis-like papulosquamous lesions and purpura. | Chronic granulomatous infiltrate with plasma cells/Culture on Sabouraud agar at 32 °C. | Itraconazole, fluconazole, amphotericin B. |
| Scedosporium sp. [11] | Worldwide | Soil, water, sewage (immunosuppresion) | Unknown | Partly suppurating nodules. | Chronic granulomatous infiltrate/Culture on Sabouraud agar at room temperature. | Itraconazole and ketoconazole. |
| Herpes simplex [11] | Worldwide | 2–12 days | Vesicles distributed on a linear fashion. | Multinucleated giant cells with intranuclear inclusion bodies / tissue cell culture, Tzanksmear and serology. | Acyclovir, famciclovir and valacyclovir. Foscarnet. | |
| Cowpox virus [11] | Cattle, cats. | Unknown | Unspecific histology/electron microscopy (brick-shaped virus using tungstic acid-stained native material) and serology. | Supportive |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tirado-Sánchez, A.; Bonifaz, A. Nodular Lymphangitis (Sporotrichoid Lymphocutaneous Infections). Clues to Differential Diagnosis. J. Fungi 2018, 4, 56. https://doi.org/10.3390/jof4020056
Tirado-Sánchez A, Bonifaz A. Nodular Lymphangitis (Sporotrichoid Lymphocutaneous Infections). Clues to Differential Diagnosis. Journal of Fungi. 2018; 4(2):56. https://doi.org/10.3390/jof4020056
Chicago/Turabian StyleTirado-Sánchez, Andrés, and Alexandro Bonifaz. 2018. "Nodular Lymphangitis (Sporotrichoid Lymphocutaneous Infections). Clues to Differential Diagnosis" Journal of Fungi 4, no. 2: 56. https://doi.org/10.3390/jof4020056
APA StyleTirado-Sánchez, A., & Bonifaz, A. (2018). Nodular Lymphangitis (Sporotrichoid Lymphocutaneous Infections). Clues to Differential Diagnosis. Journal of Fungi, 4(2), 56. https://doi.org/10.3390/jof4020056