
A Visual and Comprehensive Review on COVID-19-Associated Pulmonary Aspergillosis (CAPA)

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Methods
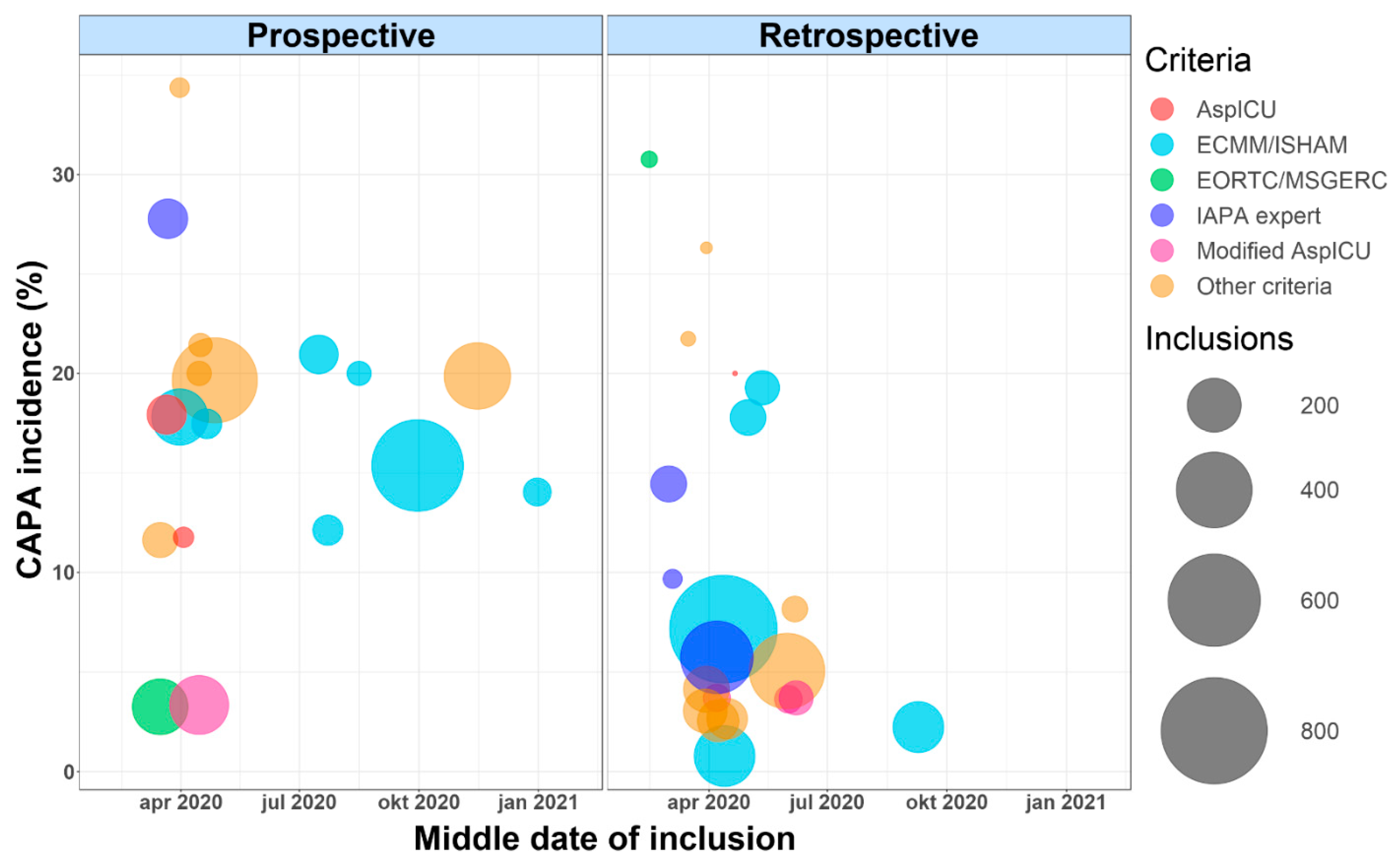
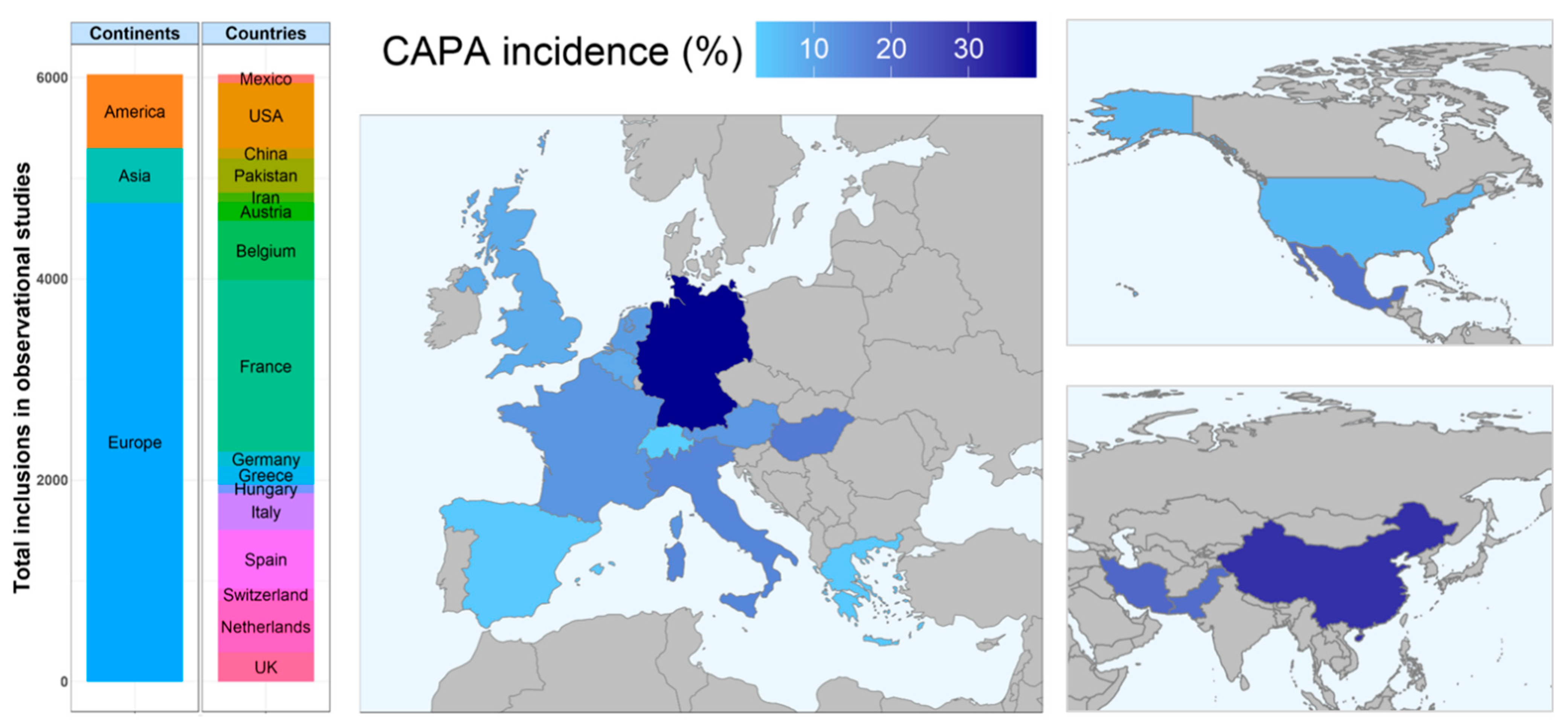
3. Incidence
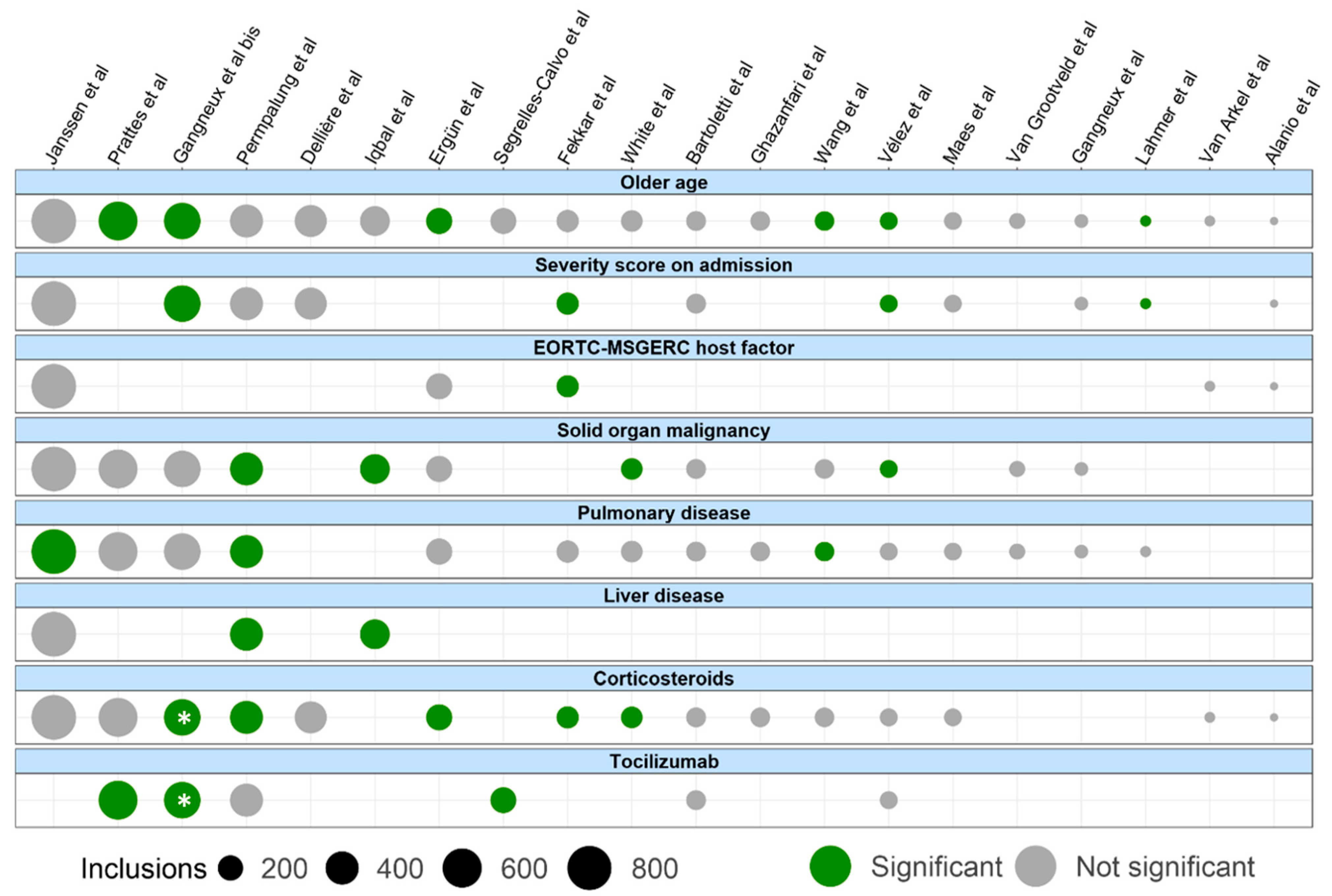
4. Risk Factors
5. Outcome
6. Hypotheses on the Pathophysiology
7. Imaging
8. Mycological Diagnostic Tools
8.1. Systemic Markers
8.2. Bronchoscopy
8.3. Respiratory Samples
9. Diagnostic Criteria
10. Treatment
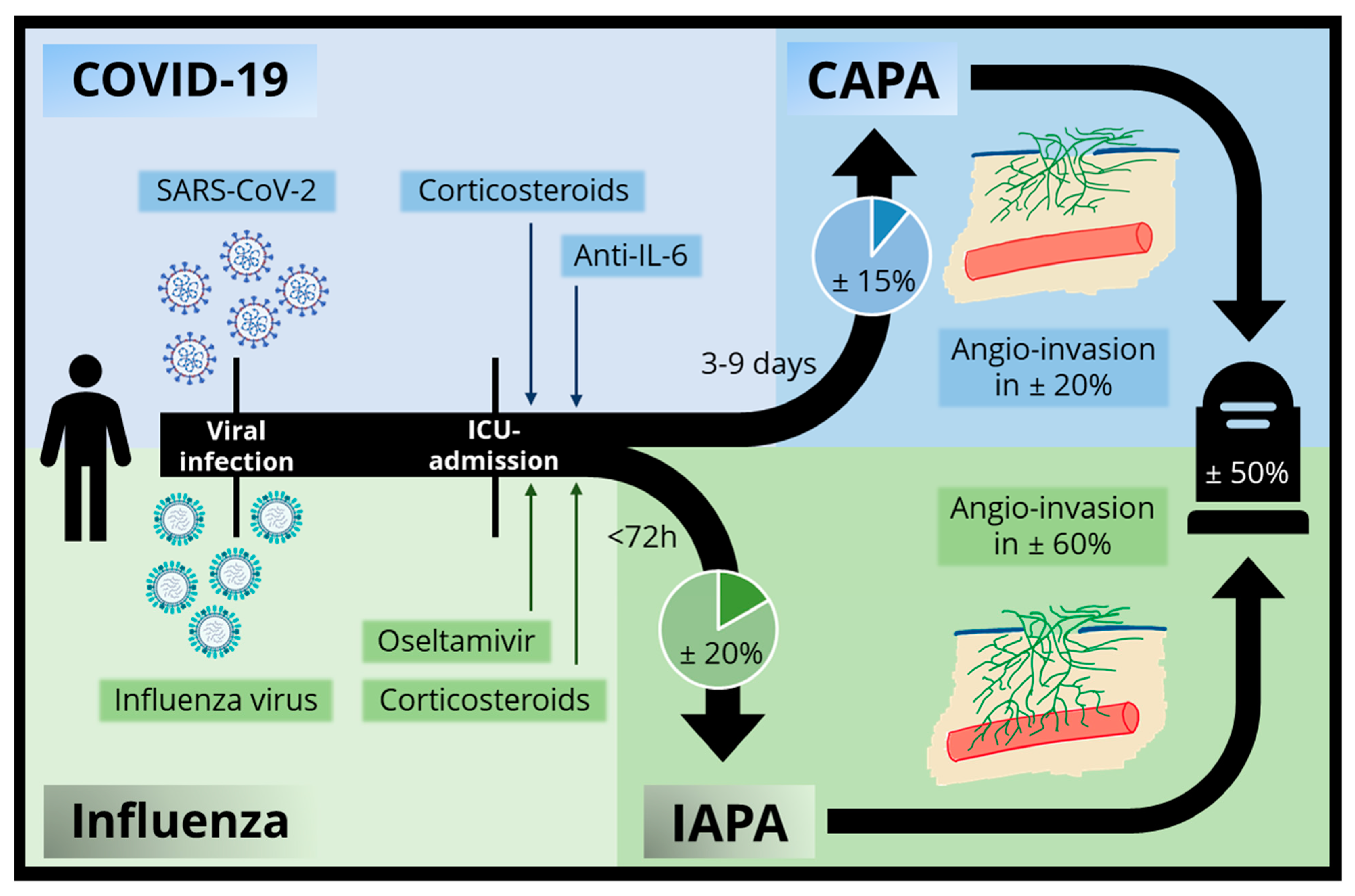
11. Comparison of IAPA and CAPA
12. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Schauwvlieghe, A.F.A.D.; Rijnders, B.J.A.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van de Veerdonk, F.L.; Gommers, D.; et al. Invasive Aspergillosis in Patients Admitted to the Intensive Care Unit with Severe Influenza: A Retrospective Cohort Study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. COVID-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, G.; Almyroudi, M.-P.; Myrianthefs, P.; Rello, J. COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Intensive Med. 2021, 1, 71–80. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blot, S.I.; Taccone, F.S.; Van Den Abeele, A.M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A Clinical Algorithm to Diagnose Invasive Pulmonary Aspergillosis in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verweij, P.; Rijnders, B.; Brüggemann, R.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.; Cornely, O.; Chiller, T. International Expert Review of Influenza-Associated Pulmonary Aspergillosis in ICU Patients and Recommendations for a Case Definition. Intensive Care Med. 2020, 46, 1524–1535. [Google Scholar] [CrossRef]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Verweij, P.E.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Buil, J.B.; Calandra, T.; Chiller, T.; Clancy, C.J.; Cornely, O.A.; et al. Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med. 2021, 47, 819–834. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.-P.; Dannaoui, E.; Fekkar, A.; Luyt, C.-E.; Botterel, F.; De Prost, N.; Tadié, J.-M.; Reizine, F.; Houzé, S.; Timsit, J.-F.; et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2021. [Google Scholar] [CrossRef]
- Kula, B.E.; Clancy, C.J.; Hong Nguyen, M.; Schwartz, I.S. Invasive mould disease in fatal COVID-19: A systematic review of autopsies. Lancet Microbe 2021, 2, e405–e414. [Google Scholar] [CrossRef]
- Borman, A.M.; Palmer, M.D.; Fraser, M.; Patterson, Z.; Mann, C.; Oliver, D.; Linton, C.J.; Gough, M.; Brown, P.; Dzietczyk, A.; et al. COVID-19-associated invasive aspergillosis: Data from the UK national mycology reference laboratory. J. Clin. Microbiol. 2021, 59, e02136-20. [Google Scholar] [CrossRef] [PubMed]
- Rothe, K.; Feihl, S.; Schneider, J.; Wallnöfer, F.; Wurst, M.; Lukas, M.; Treiber, M.; Lahmer, T.; Heim, M.; Dommasch, M.; et al. Rates of bacterial co-infections and antimicrobial use in COVID-19 patients: A retrospective cohort study in light of antibiotic stewardship. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Ichai, P.; Saliba, F.; Baune, P.; Daoud, A.; Coilly, A.; Samuel, D. Impact of negative air pressure in ICU rooms on the risk of pulmonary aspergillosis in COVID-19 patients. Crit. Care 2020, 24, 538. [Google Scholar] [CrossRef] [PubMed]
- Mulet Bayona, J.V.; Tormo Palop, N.; Salvador García, C.; Fuster Escrivá, B.; Chanzá Aviñó, M.; Ortega García, P.; Gimeno Cardona, C. Impact of the SARS-CoV-2 Pandemic in Candidaemia, Invasive Aspergillosis and Antifungal Consumption in a Tertiary Hospital. J. Fungi 2021, 7, 440. [Google Scholar] [CrossRef] [PubMed]
- Hatzl, S.; Reisinger, A.C.; Posch, F.; Prattes, J.; Stradner, M.; Pilz, S.; Eller, P.; Schoerghuber, M.; Toller, W.; Gorkiewicz, G.; et al. Antifungal prophylaxis for prevention of COVID-19-associated pulmonary aspergillosis in critically ill patients: An observational study. Crit. Care 2021, 25, 335. [Google Scholar] [CrossRef]
- Janssen, N.A.F.; Nyga, R.; Vanderbeke, L.; Jacobs, C.; Ergün, M.; Buil, J.B.; van Dijk, K.; Altenburg, J.; Bouman, C.S.C.; van der Spoel, H.I.; et al. Multinational Observational Cohort Study of COVID-19–Associated Pulmonary Aspergillosis1. Emerg. Infect. Dis. 2021, 27, 2892–2898. [Google Scholar] [CrossRef]
- Ergün, M.; Brüggemann, R.J.M.; Alanio, A.; Dellière, S.; van Arkel, A.; Bentvelsen, R.G.; Rijpstra, T.; van der Sar-van der Brugge, S.; Lagrou, K.; Janssen, N.A.F.; et al. Aspergillus Test Profiles and Mortality in Critically Ill COVID-19 Patients. J. Clin. Microbiol. 2021, 59, e0122921. [Google Scholar] [CrossRef]
- Prattes, J.; Wauters, J.; Giacobbe, D.R.; Salmanton-García, J.; Maertens, J.; Bourgeois, M.; Reynders, M.; Rutsaert, L.; Van Regenmortel, N.; Lormans, P.; et al. Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients—a multinational observational study by the European Confederation of Medical Mycology. Clin. Microbiol. Infect. 2021, S1198, 743X. [Google Scholar] [CrossRef]
- Van Ackerbroeck, S.; Rutsaert, L.; Roelant, E.; Dillen, K.; Wauters, J.; Van Regenmortel, N. Inhaled liposomal amphotericin-B as a prophylactic treatment for COVID-19-associated pulmonary aspergillosis/aspergillus tracheobronchitis. Crit. Care 2021, 25, 298. [Google Scholar] [CrossRef]
- Szabo, B.G.; Lakatos, B.; Bobek, I.; Szabo, E.; Szlavik, J.; Vályi-Nagy, I. Invasive fungal infections among critically ill adult COVID-19 patients: First experiences from the national centre in Hungary. J. Med. Mycol. 2021, 31, 101198. [Google Scholar] [CrossRef]
- Iqbal, A.; Ramzan, M.; Akhtar, A.; Ahtesham, A.; Aslam, S.; Khalid, J. COVID-Associated Pulmonary Aspergillosis and Its Related Outcomes: A Single-Center Prospective Observational Study. Cureus 2021, 13, e16982. [Google Scholar] [CrossRef] [PubMed]
- Paramythiotou, E.; Dimopoulos, G.; Koliakos, N.; Siopi, M.; Vourli, S.; Pournaras, S.; Meletiadis, J. Epidemiology and Incidence of COVID-19-Associated Pulmonary Aspergillosis (CAPA) in a Greek Tertiary Care Academic Reference Hospital. Infect. Dis. 2021, 10, 1779–1792. [Google Scholar] [CrossRef]
- Vélez Pintado, M.; Camiro-Zúñiga, A.; Aguilar Soto, M.; Cuenca, D.; Mercado, M.; Crabtree-Ramirez, B. COVID-19-associated invasive pulmonary aspergillosis in a tertiary care center in Mexico City. Med. Mycol. 2021, 59, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Fortarezza, F.; Boscolo, A.; Pezzuto, F.; Lunardi, F.; Acosta, M.J.; Giraudo, C.; Del Vecchio, C.; Sella, N.; Tiberio, I.; Godi, I.; et al. Proven COVID-19—associated pulmonary aspergillosis in patients with severe respiratory failure. Mycoses 2021, 64, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Wasylyshyn, A.I.; Wasylyshyn, G.R.; Linder, K.A.; Miceli, M.H. COVID-19-Associated Pulmonary Aspergillosis at an Academic Medical Center in the Midwestern United States. Mycopathologia 2021, 186, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Ghazanfari, M.; Arastehfar, A.; Davoodi, L.; Yazdani Charati, J.; Moazeni, M.; Abastabar, M.; Haghani, I.; Mirzakhani, R.; Mayahi, S.; Fang, W.; et al. Pervasive but Neglected: A Perspective on COVID-19-Associated Pulmonary Mold Infections among Mechanically Ventilated COVID-19 Patients. Front. Med. 2021, 8, 649675. [Google Scholar] [CrossRef]
- Oliva, A.; Ceccarelli, G.; Borrazzo, C.; Ridolfi, M.; D’Ettorre, G.; Alessandri, F.; Ruberto, F.; Pugliese, F.; Raponi, G.M.; Russo, A.; et al. Comparison of clinical features and outcomes in COVID-19 and influenza pneumonia patients requiring intensive care unit admission. Infection 2021, 49, 965–975. [Google Scholar] [CrossRef] [PubMed]
- Reizine, F.; Pinceaux, K.; Lederlin, M.; Autier, B.; Guegan, H.; Gacouin, A.; Luque-Paz, D.; Boglione-Kerrien, C.; Bacle, A.; Le Daré, B.; et al. Influenza- and COVID-19-Associated Pulmonary Aspergillosis: Are the Pictures Different? J. Fungi 2021, 7, 388. [Google Scholar] [CrossRef]
- Sánchez Martín, C.; Madrid Martínez, E.; González Pellicer, R.; Armero Ibáñez, R.; Martínez González, E.; Llau Pitarch, J.V. Aspergilosis pulmonar invasiva en pacientes con síndrome de distrés respiratorio por COVID-19. Rev. Esp. Anestesiol. Reanim. 2021. [Google Scholar] [CrossRef]
- Ripa, M.; Galli, L.; Poli, A.; Oltolini, C.; Spagnuolo, V.; Mastrangelo, A.; Muccini, C.; Monti, G.; De Luca, G.; Landoni, G.; et al. Secondary infections in patients hospitalized with COVID-19: Incidence and predictive factors. Clin. Microbiol. Infect. 2021, 27, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Lahmer, T.; Kriescher, S.; Herner, A.; Rothe, K.; Spinner, C.D.; Schneider, J.; Mayer, U.; Neuenhahn, M.; Hoffmann, D.; Geisler, F.; et al. Invasive pulmonary aspergillosis in critically ill patients with severe COVID-19 pneumonia: Results from the prospective AspCOVID-19 study. PLoS ONE 2021, 16, e0238825. [Google Scholar] [CrossRef] [PubMed]
- Permpalung, N.; Chiang, T.P.-Y.; Massie, A.B.; Zhang, S.X.; Avery, R.K.; Nematollahi, S.; Ostrander, D.; Segev, D.L.; Marr, K.A. Coronavirus Disease 2019–Associated Pulmonary Aspergillosis in Mechanically Ventilated Patients. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Van Grootveld, R.; van Paassen, J.; de Boer, M.G.J.; Claas, E.C.J.; Kuijper, E.J.; van der Beek, M.T. Systematic screening for COVID-19 associated invasive aspergillosis in ICU patients by culture and PCR on tracheal aspirate. Mycoses 2021, 64, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, E.; Vonk, A.; van den Akker, J.P.C.; Bode, L.; Sips, G.J.; Rijnders, B.J.A.; de Steenwinkel, J.; Verkaik, N.J.; Vogel, M.; van der Eerden, M.; et al. Frequency of positive aspergillus tests in COVID-19 patients in comparison to other patients with pulmonary infections admitted to the intensive care unit. J. Clin. Microbiol. 2021, 59, e02278-20. [Google Scholar] [CrossRef] [PubMed]
- Versyck, M.; Zarrougui, W.; Lambiotte, F.; Elbeki, N.; Saint-Leger, P. Invasive pulmonary aspergillosis in COVID-19 critically ill patients: Results of a French monocentric cohort. J. Mycol. Med. 2021, 31, 101122. [Google Scholar] [CrossRef]
- Meijer, E.F.J.; Dofferhoff, A.S.M.; Hoiting, O.; Meis, J.F. COVID-19–associated pulmonary aspergillosis: A prospective single-center dual case series. Mycoses 2021, 64, 457–464. [Google Scholar] [CrossRef]
- Fekkar, A.; Lampros, A.; Mayaux, J.; Poignon, C.; Demeret, S.; Constantin, J.M.; Marcelin, A.G.; Monsel, A.; Luyt, C.E.; Blaize, M. Occurrence of invasive pulmonary fungal infections in patients with severe COVID-19 admitted to the ICU. Am. J. Respir. Crit. Care Med. 2021, 203, 307–317. [Google Scholar] [CrossRef]
- Maes, M.; Higginson, E.; Pereira-Dias, J.; Curran, M.D.; Parmar, S.; Khokhar, F.; Cuchet-Lourenço, D.; Lux, J.; Sharma-Hajela, S.; Ravenhill, B.; et al. Ventilator-associated pneumonia in critically ill patients with COVID-19. Crit. Care 2021, 25, 25. [Google Scholar] [CrossRef] [PubMed]
- Marr, K.A.; Platt, A.; Tornheim, J.A.; Zhang, S.X.; Datta, K.; Cardozo, C.; Garcia-Vidal, C. Aspergillosis complicating severe coronavirus disease. Emerg. Infect. Dis. 2021, 27, 18–25. [Google Scholar] [CrossRef]
- Razazi, K.; Arrestier, R.; Haudebourg, A.F.; Benelli, B.; Carteaux, G.; Decousser, J.; Fourati, S.; Woerther, P.L.; Schlemmer, F.; Charles-Nelson, A.; et al. Risks of ventilator-associated pneumonia and invasive pulmonary aspergillosis in patients with viral acute respiratory distress syndrome related or not to Coronavirus 19 disease. Crit. Care 2020, 24, 699. [Google Scholar] [CrossRef]
- Dellière, S.; Dudoignon, E.; Fodil, S.; Voicu, S.; Collet, M.; Oillic, P.A.; Salmona, M.; Dépret, F.; Ghelfenstein-Ferreira, T.; Plaud, B.; et al. Risk factors associated with COVID-19-associated pulmonary aspergillosis in ICU patients: A French multicentric retrospective cohort. Clin. Microbiol. Infect. 2021, 27, 790.e1–790.e5. [Google Scholar] [CrossRef]
- Benedetti, M.F.; Alava, K.H.; Sagardia, J.; Cadena, R.C.; Laplume, D.; Capece, P.; Posse, G.; Nusblat, A.D.; Cuestas, M.L. COVID-19 associated pulmonary aspergillosis in ICU patients: Report of five cases from Argentina. Med. Mycol. Case Rep. 2021, 31, 24–28. [Google Scholar] [CrossRef]
- Nebreda-Mayoral, T.; Miguel-Gómez, M.A.; March-Rosselló, G.A.; Puente-Fuertes, L.; Cantón-Benito, E.; Martínez-García, A.M.; Muñoz-Martín, A.B.; Orduña-Domingo, A. Infección bacteriana/fúngica en pacientes con COVID-19 ingresados en un hospital de tercer nivel de Castilla y León, España. Enfermedades Infecciosas y Microbiología Clínica 2020. [Google Scholar] [CrossRef]
- Segrelles-Calvo, G.; Araújo, G.R.S.; Llopis-Pastor, E.; Carrillo, J.; Hernández-Hernández, M.; Rey, L.; Rodríguez Melean, N.; Escribano, I.; Antón, E.; Zamarro, C.; et al. Prevalence of opportunistic invasive aspergillosis in COVID-19 patients with severe pneumonia. Mycoses 2021, 64, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.; Valerio, M.; Álvarez-Uría, A.; Olmedo, M.; Veintimilla, C.; Padilla, B.; De la Villa, S.; Guinea, J.; Escribano, P.; Ruiz-Serrano, M.J.; et al. Invasive pulmonary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2021, 64, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Mitaka, H.; Perlman, D.C.; Javaid, W.; Salomon, N. Putative invasive pulmonary aspergillosis in critically ill patients with COVID-19: An observational study from New York City. Mycoses 2020, 63, 1368–1372. [Google Scholar] [CrossRef]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. A National Strategy to Diagnose Coronavirus Disease 2019–Associated Invasive Fungal Disease in the Intensive Care Unit. Clin. Infect. Dis. 2021, 73, e1634–e1644. [Google Scholar] [CrossRef] [PubMed]
- Dupont, D.; Menotti, J.; Turc, J.; Miossec, C.; Wallet, F.; Richard, J.C.; Argaud, L.; Paulus, S.; Wallon, M.; Ader, F.; et al. Pulmonary aspergillosis in critically ill patients with Coronavirus Disease 2019 (COVID-19). Med. Mycol. 2021, 59, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Sarrazyn, C.; Dhaese, S.; Demey, B.; Vandecasteele, S.; Reynders, M.; Van Praet, J.T. Incidence, risk factors, timing, and outcome of influenza versus COVID-19–associated putative invasive aspergillosis. Infect. Control Hosp. Epidemiol. 2021, 42, 1149–1150. [Google Scholar] [CrossRef] [PubMed]
- Falces-Romero, I.; Ruiz-Bastián, M.; Díaz-Pollán, B.; Maseda, E.; García-Rodríguez, J.; Montero-Vega, M.D.; Romero-Gómez, M.P.; García-Bujalance, S.; Cendejas-Bueno, E.; Toro-Rueda, C.; et al. Isolation of Aspergillus spp. in respiratory samples of patients with COVID-19 in a Spanish Tertiary Care Hospital. Mycoses 2020, 63, 1144–1148. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of Invasive Pulmonary Aspergillosis Among Intubated Patients with COVID-19: A Prospective Study. Clin. Infect. Dis. 2020, 73, ciaa1065. [Google Scholar] [CrossRef]
- Nasir, N.; Farooqi, J.; Mahmood, S.F.; Jabeen, K. COVID-19-associated pulmonary aspergillosis (CAPA) in patients admitted with severe COVID-19 pneumonia: An observational study from Pakistan. Mycoses 2020, 63, 766–770. [Google Scholar] [CrossRef]
- Van Biesen, S.; Kwa, D.; Bosman, R.J.; Juffermans, N.P. Detection of Invasive Pulmonary Aspergillosis in COVID-19 with Nondirected BAL. Am. J. Respir. Crit. Care Med. 2020, 202, 1171. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.P.; Reizine, F.; Guegan, H.; Pinceaux, K.; Le Balch, P.; Prat, E.; Pelletier, R.; Belaz, S.; Le Souhaitier, M.; Le Tulzo, Y.; et al. Is the covid-19 pandemic a good time to include aspergillus molecular detection to categorize aspergillosis in icu patients? A monocentric experience. J. Fungi 2020, 6, 105. [Google Scholar] [CrossRef] [PubMed]
- Lamoth, F.; Glampedakis, E.; Boillat-Blanco, N.; Oddo, M.; Pagani, J.-L. Incidence of invasive pulmonary aspergillosis among critically ill COVID-19 patients. Clin. Microbiol. Infect. 2020, 26, 1706–1708. [Google Scholar] [CrossRef] [PubMed]
- van Arkel, A.L.E.; Rijpstra, T.A.; Belderbos, H.N.A.; van Wijngaarden, P.; Verweij, P.E.; Bentvelsen, R.G. COVID-19–associated Pulmonary Aspergillosis. Am. J. Respir. Crit. Care Med. 2020, 202, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yang, Q.; Zhang, P.; Sheng, J.; Zhou, J.; Qu, T. Clinical characteristics of invasive pulmonary aspergillosis in patients with COVID-19 in Zhejiang, China: A retrospective case series. Crit. Care 2020, 24, 299. [Google Scholar] [CrossRef] [PubMed]
- Rutsaert, L.; Steinfort, N.; Van Hunsel, T.; Bomans, P.; Naesens, R.; Mertes, H.; Dits, H.; Van Regenmortel, N. COVID-19-associated invasive pulmonary aspergillosis. Ann. Intensive Care 2020, 10, 71. [Google Scholar] [CrossRef]
- Alanio, A.; Dellière, S.; Fodil, S.; Bretagne, S.; Mégarbane, B. Prevalence of putative invasive pulmonary aspergillosis in critically ill patients with COVID-19. Lancet Respir. Med. 2020, 8, e48–e49. [Google Scholar] [CrossRef]
- Bongomin, F.; Gago, S.; Oladele, R.; Denning, D. Global and Multi-National Prevalence of Fungal Diseases—Estimate Precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Hofmeyr, A.; Bansal, A.; Thakkar, D.; Lam, L.; Harrington, Z.; Bhonagiri, D. COVID-19 associated pulmonary aspergillosis (CAPA): An Australian case report. Med. Mycol. Case Rep. 2021, 31, 6–10. [Google Scholar] [CrossRef]
- Prattes, J.; Koehler, P.; Hoenigl, M.; Wauters, J.; Giacobbe, D.R.; Lagrou, K.; Salmanton-García, J.; Rautemaa-Richardson, R.; Hatzl, S.; Maertens, J.; et al. COVID-19 associated pulmonary aspergillosis: Regional variation in incidence and diagnostic challenges. Intensive Care Med. 2021, 47, 1339–1340. [Google Scholar] [CrossRef]
- Meersseman, W.; Lagrou, K.; Maertens, J.; Wilmer, A.; Hermans, G.; Vanderschueren, S.; Spriet, I.; Verbeken, E.; Van Wijngaerden, E. Galactomannan in Bronchoalveolar Lavage Fluid: A Tool for Diagnosing Aspergillosis in Intensive Care Unit Patients. Am. J. Respir. Crit. Care Med. 2008, 177, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef]
- Van de Veerdonk, F.L.; Brüggemann, R.J.M.; Vos, S.; de Hertogh, G.; Wauters, J.; Reijers, M.H.E.; Netea, M.G.; Schouten, J.A.; Verweij, P.E. COVID-19-associated Aspergillus tracheobronchitis: The interplay between viral tropism, host defence, and fungal invasion. Lancet Respir. Med. 2021, 9, 795–802. [Google Scholar] [CrossRef]
- Recovery Collaborative Group Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [CrossRef]
- Latgé, J.-P.; Chamilos, G. Aspergillus fumigatus and Aspergillosis in 2019. Clin. Microbiol. Rev. 2019, 33, ee00140-18. [Google Scholar] [CrossRef]
- Meersseman, W.; Lagrou, K.; Maertens, J.; Wijngaerden, E.V. Invasive Aspergillosis in the Intensive Care Unit. Clin. Infect. Dis. 2007, 45, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Bertuzzi, M.; Hayes, G.E.; Icheoku, U.J.; van Rhijn, N.; Denning, D.W.; Osherov, N.; Bignell, E.M. Anti-aspergillus activities of the respiratory epithelium in health and disease. J. Fungi 2018, 4, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewi, I.M.; Janssen, N.A.; Rosati, D.; Bruno, M.; Netea, M.G.; Brüggemann, R.J.; Verweij, P.E.; van de Veerdonk, F.L. Invasive pulmonary aspergillosis associated with viral pneumonitis. Curr. Opin. Microbiol. 2021, 62, 21–27. [Google Scholar] [CrossRef]
- Contou, D.; Dorison, M.; Rosman, J.; Schlemmer, F.; Gibelin, A.; Foulet, F.; Botterel, F.; Carteaux, G.; Razazi, K.; Brun-Buisson, C.; et al. Aspergillus-positive lower respiratory tract samples in patients with the acute respiratory distress syndrome: A 10-year retrospective study. Ann. Intensive Care 2016, 6, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprenkeler, E.G.G.; Gresnigt, M.S.; van de Veerdonk, F.L. LC3-associated phagocytosis: A crucial mechanism for antifungal host defence against Aspergillus fumigatus. Cell. Microbiol. 2016, 18, 1208–1216. [Google Scholar] [CrossRef] [Green Version]
- Van De Veerdonk, F.L.; Gresnigt, M.S.; Romani, L.; Netea, M.G.; Latgé, J.P. Aspergillus fumigatus morphology and dynamic host interactions. Nat. Rev. Microbiol. 2017, 15, 661–674. [Google Scholar] [CrossRef]
- Gafa, V.; Remoli, M.E.; Giacomini, E.; Severa, M.; Grillot, R.; Coccia, E.M. Enhancement of anti-Aspergillus T helper type 1 response by interferon-β-conditioned dendritic cells. Immunology 2010, 131, 282. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, V.; Dutta, O.; McElrath, C.; Du, P.; Chang, Y.-J.; Cicciarelli, B.; Pitler, A.; Whitehead, I.; Obar, J.J.; Durbin, J.E.; et al. Type III interferon is a critical regulator of innate antifungal immunity. Sci. Immunol. 2017, 2, eaan5357. [Google Scholar] [CrossRef] [Green Version]
- Wauters, E.; Van Mol, P.; Garg, A.D.; Jansen, S.; Van Herck, Y.; Vanderbeke, L.; Bassez, A.; Boeckx, B.; Malengier-Devlies, B.; Timmerman, A.; et al. Discriminating mild from critical COVID-19 by innate and adaptive immune single-cell profiling of bronchoalveolar lavages. Cell Res. 2021, 31, 272–290. [Google Scholar] [CrossRef]
- Kyrmizi, I.; Gresnigt, M.S.; Akoumianaki, T.; Samonis, G.; Sidiropoulos, P.; Boumpas, D.; Netea, M.; Van de Veerdonk, F.L.; Kontoyiannis, D.P.; Chamilos, G. Corticosteroids block autophagy protein recruitment in Aspergillus fumigatus phagosomes via targeting Dectin-1/syk kinase signaling. J. Immunol. 2013, 191, 1287–1299. [Google Scholar] [CrossRef] [Green Version]
- Korn, T.; Mitsdoerffer, M.; Croxford, A.L.; Awasthi, A.; Dardalhon, V.A.; Galileos, G.; Vollmar, P.; Stritesky, G.L.; Kaplan, M.H.; Waisman, A.; et al. IL-6 controls Th17 immunity in vivo by inhibiting the conversion of conventional T cells into Foxp3+ regulatory T cells. Proc. Natl. Acad. Sci. USA 2008, 105, 18460–18465. [Google Scholar] [CrossRef] [Green Version]
- Akoumianaki, T.; Vaporidi, K.; Diamantaki, E.; Pène, F.; Beau, R.; Gresnigt, M.; Gkountzinopulou, M.; Venichaki, M.; Drakos, E.; El-Benna, J.; et al. Uncoupling of IL-6 signaling and LC3-associated phagocytosis drives immunoparalysis during sepsis. Cell Host Microbe 2021, 29, 1277–1293.e6. [Google Scholar] [CrossRef]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA—Secondary Publication. J. Thorac. Imaging 2020, 35, 219–227. [Google Scholar] [CrossRef]
- Franquet, T.; Müller, N.L.; Giménez, A.; Guembe, P.; De La Torre, J.; Bagué, S. Spectrum of pulmonary aspergillosis: Histologic, clinical, and radiologic findings. Radiographics 2001, 21, 825–837. [Google Scholar] [CrossRef] [Green Version]
- Herbrecht, R.; Guffroy, B.; Danion, F.; Venkatasamy, A.; Simand, C.; Ledoux, M.-P. Validation by Real-life Data of the New Radiological Criteria of the Revised and Updated Consensus Definition for Invasive Fungal Diseases. Clin. Infect. Dis. 2020, 71, 2773–2774. [Google Scholar] [CrossRef]
- Li, Y.; Xia, L. Coronavirus disease 2019 (COVID-19): Role of chest CT in diagnosis and management. Am. J. Roentgenol. 2020, 214, 1280–1286. [Google Scholar] [CrossRef]
- Mondoni, M.; Papa, G.F.S.; Rinaldo, R.; Faverio, P.; Marruchella, A.; D’Arcangelo, F.; Pesci, A.; Pasini, S.; Henchi, S.; Cipolla, G.; et al. Utility and safety of bronchoscopy during the SARS-CoV-2 outbreak in Italy: A retrospective, multicentre study. Eur. Respir. J. 2020, 56, 2002767. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.H.; Jiang, J.; Kon, Z.N.; Williams, D.M.; Geraci, T.C.; Smith, D.E.; Cerfolio, R.J.; Zervos, M.; Bizekis, C. Safety and Efficacy of Bronchoscopy in Critically Ill Patients with Coronavirus Disease 2019. Chest 2021, 159, 870. [Google Scholar] [CrossRef]
- Levra, S.; Veljkovic, A.; Comune, M.; Bernardi, V.; Sandri, A.; Indellicati, D. Bronchoscopy in times of COVID-19 pandemic: An interventional pulmonology unit experience. Respir. Med. Res. 2021, 80, 100830. [Google Scholar] [CrossRef]
- Gao, C.A.; Bailey, J.I.; Walter, J.M.; Coleman, J.M.; Malsin, E.S.; Argento, A.C.; Prickett, M.H.; Wunderink, R.G.; NU COVID Investigators. Bronchoscopy on Intubated Patients with COVID-19 is Associated with Low Infectious Risk to Operators. Ann. Am. Thorac. Soc. 2021, 18, 1243. [Google Scholar] [CrossRef] [PubMed]
- Torrego, A.; Pajares, V.; Fernández-Arias, C.; Vera, P.; Mancebo, J. Bronchoscopy in Patients with COVID-19 with Invasive Mechanical Ventilation: A Single-Center Experience. Am. J. Respir. Crit. Care Med. 2020, 202, 284–287. [Google Scholar] [CrossRef]
- Wahidi, M.M.; Lamb, C.; Murgu, S.; Musani, A.; Shojaee, S.; Sachdeva, A.; Maldonado, F.; Mahmood, K.; Kinsey, M.; Sethi, S.; et al. American Association for Bronchology and Interventional Pulmonology (AABIP) Statement on the Use of Bronchoscopy and Respiratory Specimen Collection in Patients with Suspected or Confirmed COVID-19 Infection. J. Bronchol. Interv. Pulmonol. 2020, 27, e52–e54. [Google Scholar] [CrossRef]
- Roman-Montes, A.C.M.; Martinez-Gamboa, A.; Diaz-Lomelí, P.; Cervantes-Sanchez, A.; Rangel-Cordero, A.; Sifuentes-Osornio, J.; Ponce-de-Leon, A.; Lara, M.F.G. Accuracy of galactomannan testing on tracheal aspirates in COVID-19-associated pulmonary aspergillosis. Mycoses 2021, 64, 364–371. [Google Scholar] [CrossRef]
- Mercier, T.; Castagnola, E.; Marr, K.A.; Wheat, L.J.; Verweij, P.E.; Maertens, J.A. Defining Galactomannan Positivity in the Updated EORTC/MSGERC Consensus Definitions of Invasive Fungal Diseases. Clin. Infect. Dis. 2021, 72, S89–S94. [Google Scholar] [CrossRef]
- Mercier, T.; Dunbar, A.; Veldhuizen, V.; Holtappels, M.; Schauwvlieghe, A.; Maertens, J.; Rijnders, B.; Wauters, J. Point of care aspergillus testing in intensive care patients. Crit. Care 2020, 24, 642. [Google Scholar] [CrossRef] [PubMed]
- Autier, B.; Prattes, J.; White, P.L.; Valerio, M.; Machado, M.; Price, J.; Egger, M.; Gangneux, J.-P.; Hoenigl, M. Aspergillus Lateral Flow Assay with Digital Reader for the Diagnosis of COVID-19 Associated Pulmonary Aspergillosis (CAPA): A multicenter study. J. Clin. Microbiol. 2021. [Google Scholar] [CrossRef]
- Rijnders, B.J.A.; Schauwvlieghe, A.F.A.D.; Wauters, J. Influenza-Associated Pulmonary Aspergillosis: A Local or Global Lethal Combination? Clin. Infect. Dis. 2020, 71, 1764–1767. [Google Scholar] [CrossRef] [PubMed]
- Coste, A.; Frérou, A.; Raute, A.; Couturaud, F.; Morin, J.; Egreteau, P.-Y.; Blanc, F.-X.; Reignier, J.; Tadié, J.-M.; Tran, A.; et al. The Extent of Aspergillosis in Critically Ill Patients with Severe Influenza Pneumonia. Crit. Care Med. 2021, 49, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Schultz, M.J.; Vincent, J.L.; Alvarez-Lerma, F.; Bos, L.D.; Solé-Violán, J.; Torres, A.; Rodriguez, A. Increased Incidence of Co-Infection in Critically Ill Patients with Influenza. Intensive Care Med. 2017, 43, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Pastores, S.M.; Dulu, A.; Voigt, L.; Raoof, N.; Alicea, M.; Halpern, N.A. Premortem clinical diagnoses and postmortem autopsy findings: Discrepancies in critically ill cancer patients. Crit. Care 2007, 11, R48. [Google Scholar] [CrossRef] [Green Version]
- Jia, S.; Gao, K.; Huang, P.; Guo, R.; Zuo, X.; Xia, Q.; Hu, S.; Yu, Z.; Xie, Y. Interactive Effects of Glucocorticoids and Cytochrome P450 Polymorphisms on the Plasma Trough Concentrations of Voriconazole. Front. Pharm. 2021, 12, 1250. [Google Scholar] [CrossRef] [PubMed]
- Van Daele, R.; Bekkers, B.; Lindfors, M.; Broman, L.M.; Schauwvlieghe, A.; Rijnders, B.; Hunfeld, N.G.M.; Juffermans, N.P.; Taccone, F.S.; Sousa, C.A.C.; et al. A large retrospective assessment of voriconazole exposure in patients treated with extracorporeal membrane oxygenation. Microorganisms 2021, 9, 1543. [Google Scholar] [CrossRef] [PubMed]
- Li, M.X.; Zhu, L.Q.; Chen, L.; Li, N.; Qi, F. Assessment of drug–drug interactions between voriconazole and glucocorticoids. J. Chemother. 2018, 30, 296–303. [Google Scholar] [CrossRef]
- Gautier-Veyret, E.; Truffot, A.; Bailly, S.; Fonrose, X.; Thiebaut-Bertrand, A.; Tonini, J.; Cahn, J.; Stanke-Labesque, F. Inflammation is a potential risk factor of voriconazole overdose in hematological patients. Fundam. Clin. Pharm. 2018, 33, fcp.12422. [Google Scholar] [CrossRef] [PubMed]
- Gautier-Veyret, E.; Thiebaut-Bertrand, A.; Roustit, M.; Bolcato, L.; Depeisses, J.; Schacherer, M.; Schummer, G.; Fonrose, X.; Stanke-Labesque, F. Optimization of voriconazole therapy for treatment of invasive aspergillosis: Pharmacogenomics and inflammatory status need to be evaluated. Br. J. Clin. Pharm. 2021, 87, 2534–2541. [Google Scholar] [CrossRef]
- Ventura, M.A.E.; Van Wanrooy, M.J.P.; Span, L.F.R.; Rodgers, M.G.G.; Van Den Heuvel, E.R.; Uges, D.R.A.; Van Der Werf, T.S.; Kosterink, J.G.W.; Alffenaar, J.W.C. Longitudinal analysis of the effect of inflammation on voriconazole trough concentrations. Antimicrob. Agents Chemother. 2016, 60, 2727–2731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maertens, J.; Selleslag, D.; Heinz, W.J.; Saulay, M.; Rahav, G.; Giladi, M.; Aoun, M.; Kovanda, L.; Kaufhold, A.; Engelhardt, M.; et al. Treatment outcomes in patients with proven/probable vs possible invasive mould disease in a phase III trial comparing isavuconazole vs voriconazole. Mycoses 2018, 61, 868–876. [Google Scholar] [CrossRef] [Green Version]
- Kaindl, T.; Andes, D.; Engelhardt, M.; Saulay, M.; Larger, P.; Groll, A.H. Variability and exposure-response relationships of isavuconazole plasma concentrations in the Phase 3 SECURE trial of patients with invasive mould diseases. J. Antimicrob. Chemother. 2019, 74, 761–767. [Google Scholar] [CrossRef] [Green Version]
- Maertens, J.A.; Rahav, G.; Lee, D.G.; Ponce-de-León, A.; Ramírez Sánchez, I.C.; Klimko, N.; Sonet, A.; Haider, S.; Diego Vélez, J.; Raad, I.; et al. Posaconazole versus voriconazole for primary treatment of invasive aspergillosis: A phase 3, randomised, controlled, non-inferiority trial. Lancet 2021, 397, 499–509. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef]
- Hoenigl, M.; Sprute, R.; Egger, M.; Arastehfar, A.; Cornely, O.A.; Krause, R.; Lass-Flörl, C.; Prattes, J.; Spec, A.; Thompson, G.R.; et al. The Antifungal Pipeline: Fosmanogepix, Ibrexafungerp, Olorofim, Opelconazole, and Rezafungin. Drugs 2021, 81, 1703–1729. [Google Scholar] [CrossRef]
- Liesenborghs, L.; Spriet, I.; Jochmans, D.; Belmans, A.; Gyselinck, I.; Teuwen, L.-A.; ter Horst, S.; Dreesen, E.; Geukens, T.; Engelen, M.M.; et al. Itraconazole for COVID-19: Preclinical studies and a proof-of-concept randomized clinical trial. EBioMedicine 2021, 66, 103288. [Google Scholar] [CrossRef]
- Conte, J.E.; Golden, J.A.; Kipps, J.; McIver, M.; Zurlinden, E. Intrapulmonary pharmacokinetics and pharmacodynamics of itraconazole and 14-hydroxyitraconazole at steady state. Antimicrob. Agents Chemother. 2004, 48, 3823–3827. [Google Scholar] [CrossRef] [Green Version]
- Groves, H.E.; Piché-Renaud, P.-P.; Peci, A.; Farrar, D.S.; Buckrell, S.; Bancej, C.; Sevenhuysen, C.; Campigotto, A.; Gubbay, J.B.; Morris, S.K. The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: A population-based study. Lancet Reg. Health Am. 2021, 1, 100015. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Friedman, D.Z.P.; Zapernick, L.; Dingle, T.C.; Lee, N.; Sligl, W.; Zelyas, N.; Smith, S.W. High Rates of Influenza-Associated Invasive Pulmonary Aspergillosis May Not Be Universal: A Retrospective Cohort Study from Alberta, Canada. Clin. Infect. Dis. 2020, 71, 1760–1763. [Google Scholar] [CrossRef]
- Feys, S.R.L.; Shoham, S.; Rijnders, B.J.A.; Wauters, J. Influenza-Associated Pulmonary Aspergillosis: Seek, and You Shall Find! Crit. Care Med. 2021, 49, e1265–e1266. [Google Scholar] [CrossRef]
- Wauters, J.; Baar, I.; Meersseman, P.; Meersseman, W.; Dams, K.; De Paep, R.; Lagrou, K.; Wilmer, A.; Jorens, P.; Hermans, G. Invasive pulmonary aspergillosis is a frequent complication of critically ill H1N1 patients: A retrospective study. Intensive Care Med. 2012, 38, 1761–1768. [Google Scholar] [CrossRef]
- Van De Veerdonk, F.L.; Kolwijck, E.; Lestrade, P.P.A.; Hodiamont, C.J.; Rijnders, B.J.A.; Van Paassen, J.; Haas, P.J.; Dos Santos, C.O.; Kampinga, G.A.; Bergmans, D.C.J.J.; et al. Influenza-associated aspergillosis in critically ill patients. Am. J. Respir. Crit. Care Med. 2017, 196, 524–527. [Google Scholar] [CrossRef]
- Vanderbeke, L.; Janssen, N.A.F.; Bergmans, D.C.J.J.; Bourgeois, M.; Buil, J.B.; Debaveye, Y.; Depuydt, P.; Feys, S.; Hermans, G.; Hoiting, O.; et al. Posaconazole for prevention of invasive pulmonary aspergillosis in critically ill influenza patients (POSA-FLU): A randomised, open-label, proof-of-concept trial. Intensive Care Med. 2021, 47, 674–686. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Included Patients (n) | Total Proven CAPA (n) | Total Probable or Putative CAPA (n) | Total Possible CAPA (n) | Total Number of Patients with Coloniz-ation (n) | Percentage Proven, Probable or Putative CAPA among All Included Patients | |
|---|---|---|---|---|---|---|
| Observational 1 studies (n = 42) | 6193 | 35 | 638 | 102 | 70 | 10.9% |
| ICU-only observational 1 studies (n = 39) | 5904 | 26 | 631 | 102 | 70 | 11.1% |
| ICU-only retrospective (or partially prospective) observational 1 studies (n = 21) | 2951 | 12 | 198 | 35 | 33 | 7.1% |
| ICU-only prospective observational studies (n = 18) | 2953 | 14 | 433 | 67 | 37 | 15.1% |
| CAPA Patients 1 (n) | Number of CAPA Patients 1 That Died, All-Cause Mortality (n, Percentage) | Total Number of Patients without Arguments for CAPA 2 | Total Number of Patients without Arguments for CAPA That Died 3 (n, Percentage) | |
|---|---|---|---|---|
| Observational trials 2 (n = 37) | 728 | 402 (55.2%) | 4522 | NA |
| Observational trials with data on mortality in patients without arguments for CAPA 3 (n = 21) | 539 | 249 (46.2%) | 3238 | 1014 (31.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feys, S.; Almyroudi, M.P.; Braspenning, R.; Lagrou, K.; Spriet, I.; Dimopoulos, G.; Wauters, J. A Visual and Comprehensive Review on COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Fungi 2021, 7, 1067. https://doi.org/10.3390/jof7121067
Feys S, Almyroudi MP, Braspenning R, Lagrou K, Spriet I, Dimopoulos G, Wauters J. A Visual and Comprehensive Review on COVID-19-Associated Pulmonary Aspergillosis (CAPA). Journal of Fungi. 2021; 7(12):1067. https://doi.org/10.3390/jof7121067
Chicago/Turabian StyleFeys, Simon, Maria Panagiota Almyroudi, Reinout Braspenning, Katrien Lagrou, Isabel Spriet, George Dimopoulos, and Joost Wauters. 2021. "A Visual and Comprehensive Review on COVID-19-Associated Pulmonary Aspergillosis (CAPA)" Journal of Fungi 7, no. 12: 1067. https://doi.org/10.3390/jof7121067
APA StyleFeys, S., Almyroudi, M. P., Braspenning, R., Lagrou, K., Spriet, I., Dimopoulos, G., & Wauters, J. (2021). A Visual and Comprehensive Review on COVID-19-Associated Pulmonary Aspergillosis (CAPA). Journal of Fungi, 7(12), 1067. https://doi.org/10.3390/jof7121067