
Clinical and Eco-Epidemiological Aspects of a Novel Hyperendemic Area of Paracoccidioidomycosis in the Tocantins-Araguaia Basin (Northern Brazil), Caused by Paracoccidioides sp.

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Cases and Diagnostics
2.2. Molecular Diagnostics
2.3. Molecular Identification of Paracoccidioides sp. in Soil Samples
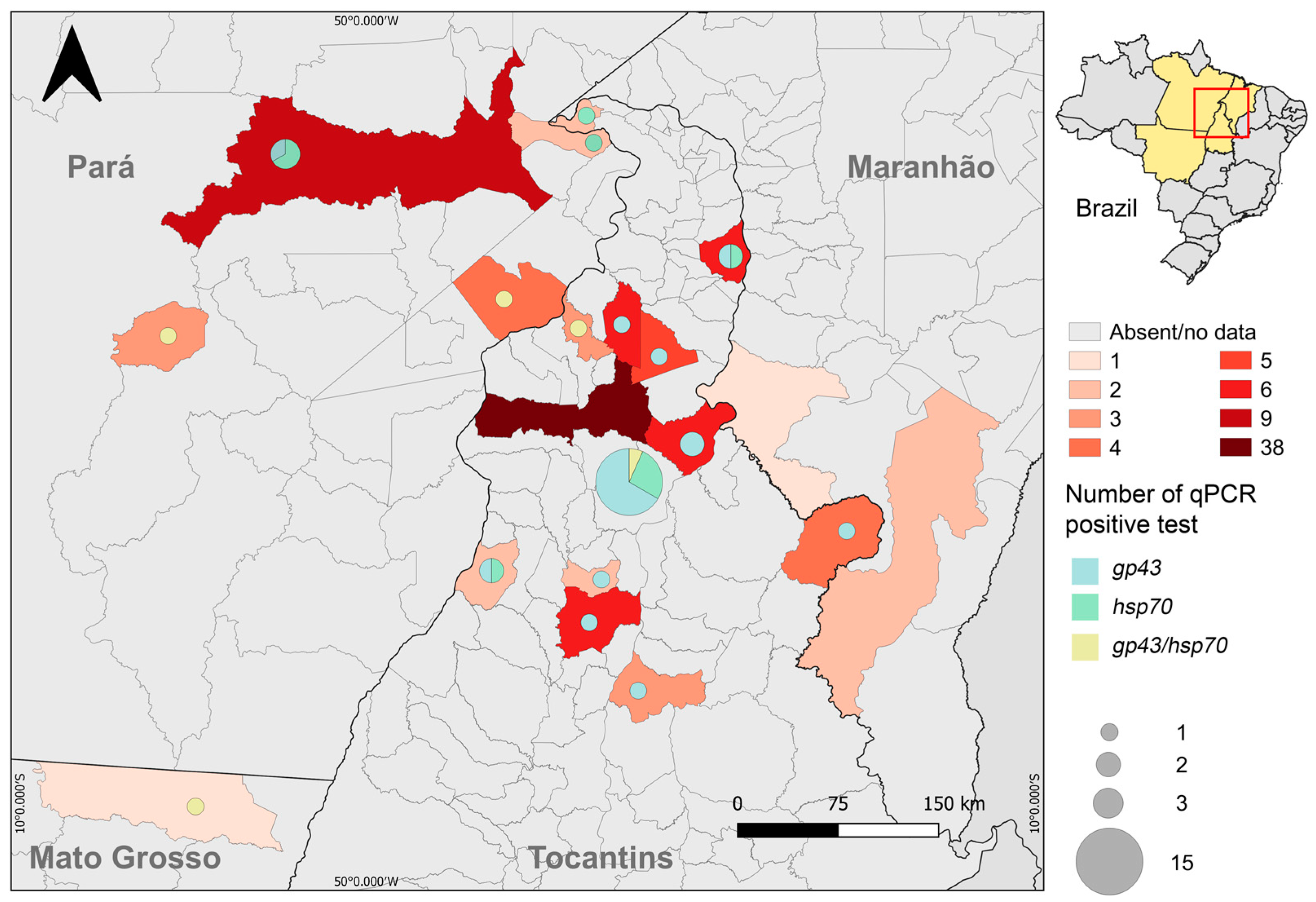
2.4. Georeferencing of PCM Cases
3. Results
3.1. Clinical Characteristics of PCM in Araguaína
3.2. Molecular Identification of Paracoccidioides sp.
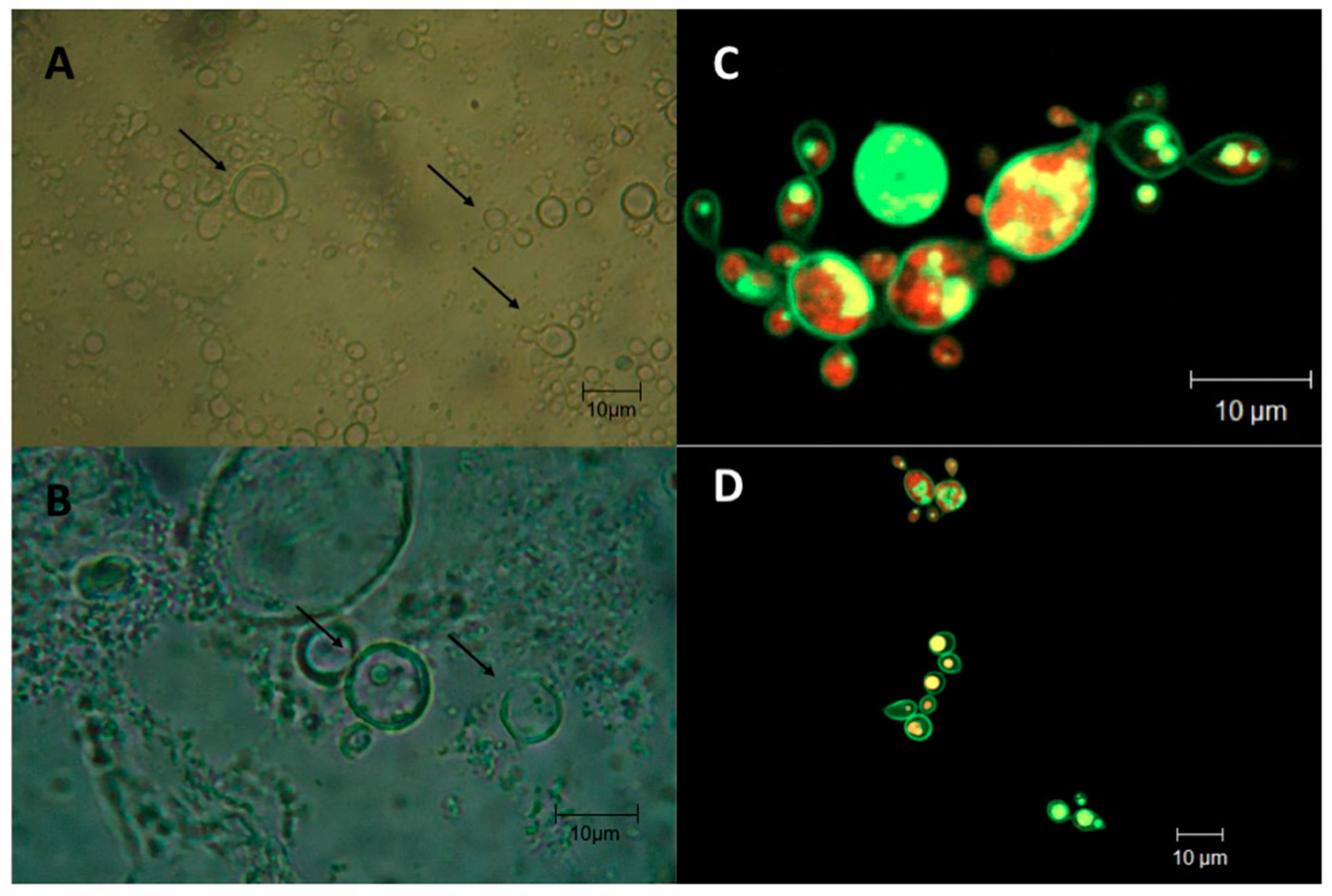
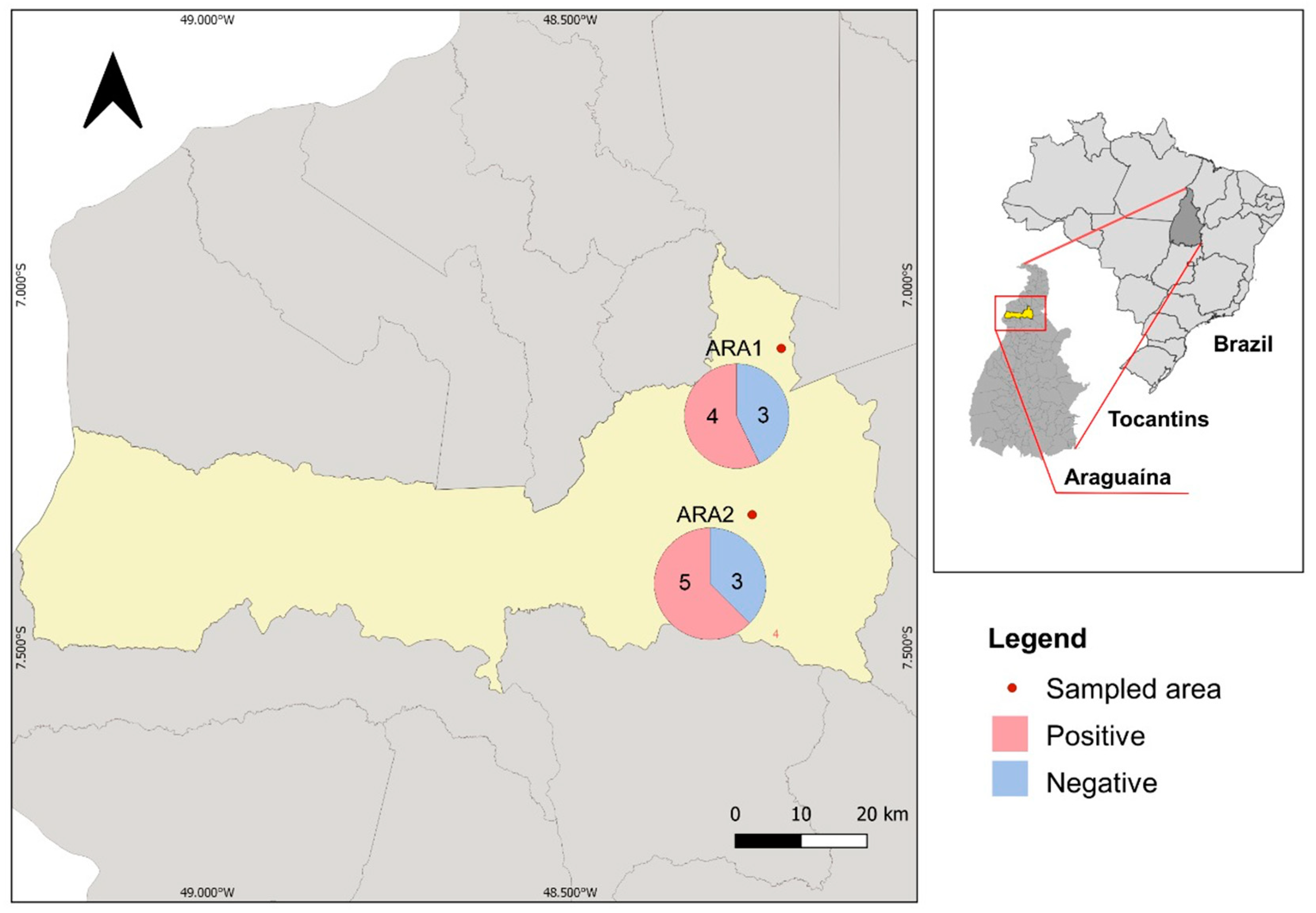
3.3. Environmental Detection of Paracoccidioides sp. in Araguaína
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fisher, M.C.; Gurr, S.J.; Cuomo, C.A.; Blehert, D.S.; Jin, H.; Stukenbrock, E.H.; Stajich, J.E.; Kahmann, R.; Boone, C.; Denning, D.W.; et al. Threats Posed by the Fungal Kingdom to Humans, Wildlife, and Agriculture. mBio 2020, 11, e00449-20. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R. New Trends in Paracoccidioidomycosis Epidemiology. J. Fungi 2017, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turissini, D.A.; Gomez, O.M.; Teixeira, M.M.; McEwen, J.G.; Matute, D.R. Species boundaries in the human pathogen Paracoccidioides. Fungal Genet. Biol. 2017, 106, 9–25. [Google Scholar] [CrossRef]
- De Melo Teixeira, M.; Theodoro, R.C.; De Oliveira, F.F.M.; Machado, G.C.; Hahn, R.C.; Bagagli, E.; San-Blas, G.; Soares Felipe, M.S. Paracoccidioides lutziisp. nov.: Biological and clinical implications. Med. Mycol. 2014, 52, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Vilela, R.; Huebner, M.; Vilela, C.; Vilela, G.; Pettersen, B.; Oliveira, C.; Mendoza, L. The taxonomy of two uncultivated fungal mammalian pathogens is revealed through phylogeny and population genetic analyses. Sci. Rep. 2021, 11, 18119. [Google Scholar] [CrossRef] [PubMed]
- San-Blas, G.; Nino-Vega, G.; Iturriaga, T. Paracoccidioides brasiliensis and paracoccidioidomycosis: Molecular approaches to morphogenesis, diagnosis, epidemiology, taxonomy and genetics. Med. Mycol. 2002, 40, 225–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordova, L.A.; Torres, J. Paracoccidioidomycosis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Coutinho, Z.F.; Wanke, B.; Travassos, C.; Oliveira, R.M.; Xavier, D.R.; Coimbra, C.E.A., Jr. Hospital morbidity due to paracoccidioidomycosis in Brazil (1998–2006). Trop. Med. Int. Health 2015, 20, 8. [Google Scholar] [CrossRef]
- Coutinho, Z.F.; Silva, D.; Lazera, M.; Petri, V.; Oliveira, R.M.; Sabroza, P.C.; Wanke, B. Paracoccidioidomycosis mortality in Brazil (1980–1995). Cad. De Saúde Pública 2002, 18, 1441–1454. [Google Scholar] [CrossRef] [Green Version]
- Queiroz-Telles, F.; Fahal, A.H.; Falci, D.R.; Caceres, D.H.; Chiller, T.; Pasqualotto, A.C. Neglected endemic mycoses. Lancet Infect. Dis. 2017, 17, e367–e377. [Google Scholar] [CrossRef]
- Griffiths, J.; Lopes Colombo, A.; Denning, D.W. The case for paracoccidioidomycosis to be accepted as a neglected tropical (fungal) disease. PLoS Negl. Trop. Dis. 2019, 13, e0007195. [Google Scholar] [CrossRef]
- Martinez, R. Paracoccidioidomycosis: The dimension of the problem of a neglected disease. Rev. Soc. Bras. Med. Trop. 2010, 43, 480. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, M.A. The natural habitat of the fungus Paracoccidioides brasiliensis, how to draw the limit between the rural and the urban environment? Biomedica 2014, 34, 5–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, R. Epidemiology of Paracoccidioidomycosis. Rev. Inst. Med. Trop. 2015, 57 (Suppl. 19), 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera, M.A.P.; Martinez, G.C.; Villafranca, M.C.M. Histopathological diagnosis of 98 cases of deep mycosis Dom Orione Hospital. In Proceedings of the VI Congreso Virtual Hispanoamericano de Anatomia Patológica, Havana, Cuba, 1–31 March 2004. [Google Scholar]
- Teixeira, M.M.; Theodoro, R.C.; Nino-Vega, G.; Bagagli, E.; Felipe, M.S. Paracoccidioides species complex: Ecology, phylogeny, sexual reproduction, and virulence. PLoS Pathog. 2014, 10, e1004397. [Google Scholar] [CrossRef] [Green Version]
- Hahn, R.C.; Rodrigues, A.M.; Della Terra, P.P.; Nery, A.F.; Hoffmann-Santos, H.D.; Gois, H.M.; Fontes, C.J.F.; de Camargo, Z.P. Clinical and epidemiological features of paracoccidioidomycosis due to Paracoccidioides lutzii. PLoS Negl. Trop. Dis. 2019, 13, e0007437. [Google Scholar] [CrossRef] [Green Version]
- Gegembauer, G.; Araujo, L.M.; Pereira, E.F.; Rodrigues, A.M.; Paniago, A.M.; Hahn, R.C.; de Camargo, Z.P. Serology of paracoccidioidomycosis due to Paracoccidioides lutzii. PLoS Negl. Trop. Dis. 2014, 8, e2986. [Google Scholar] [CrossRef]
- Zancope-Oliveira, R.M.; Pizzini, C.V.; de Medeiros Muniz, M.; do Valle, A.C.F.; Almeida-Paes, R. Diagnostic Aspects of Paracoccidioidomycosis. Curr. Trop. Med. Rep. 2014, 1, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Semighini, C.P.; de Camargo, Z.P.; Puccia, R.; Goldman, M.H.S.; Goldman, G.H. Molecular identification of Paracoccidioides brasiliensis by 5′ nuclease assay. Diagn. Microbiol. Infect. Dis. 2002, 44, 383–386. [Google Scholar] [CrossRef]
- Arantes, T.D.; Theodoro, R.C.; Teixeira Mde, M.; Bosco Sde, M.; Bagagli, E. Environmental Mapping of Paracoccidioides spp. in Brazil Reveals New Clues into Genetic Diversity, Biogeography and Wild Host Association. PLoS Negl. Trop. Dis. 2016, 10, e0004606. [Google Scholar] [CrossRef] [Green Version]
- White, T.J.; Bruns, T.; Lee, S.; Taylor, J.W. Amplification and direct sequencing of fungal ribosomal RNA Genes for phylogenetics. In PCR Protocols: A Guide to Methods and Applications; Innis, M.A., Gelfand, D.H., Sninsky, J.J., White, T.J., Eds.; Academic Press: Cambridge, MA, USA, 1990; pp. 315–322. [Google Scholar]
- Altschul, S.F.; Gish, W.; Miller, W.; Myers, E.W.; Lipman, D.J. Basic local alignment search tool. J. Mol. Biol. 1990, 215, 403–410. [Google Scholar] [CrossRef]
- Campbell, C.C. Paracoccidioidomycosis. In Proceedings of the 1st Pan American Symposium, Medellín, Colombia, 25–27 October 1971; pp. 306–312. [Google Scholar]
- Matos, W.M.; Santos, G.M.C.; Silva, V.E.B.; Gonçalves, E.G.R.; Silva, A.R. Paracoccidioidomycosis in the state of Maranhão, Brazil: Geographical and clinical aspects. Rev. Soc. Bras. Med. Trop. 2012, 45, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- do Valle, A.C.F.; Marques de Macedo, P.; Almeida-Paes, R.; Romao, A.R.; Lazera, M.D.S.; Wanke, B. Paracoccidioidomycosis after Highway Construction, Rio de Janeiro, Brazil. Emerg. Infect. Dis. 2017, 23, 1917–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giusiano, G.; Aguirre, C.; Vratnica, C.; Rojas, F.; Corallo, T.; Cattana, M.E.; Fernandez, M.; Mussin, J.; de Los Angeles Sosa, M. Emergence of acute/subacute infant-juvenile paracoccidioidomycosis in Northeast Argentina: Effect of climatic and anthropogenic changes? Med. Mycol. 2018, 57, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Zilli, M.; Scarabello, M.; Soterroni, A.C.; Valin, H.; Mosnier, A.; Leclère, D.; Havlík, P.; Kraxner, F.; Lopes, M.A.; Ramos, F.M. The impact of climate change on Brazil’s agriculture. Sci. Total Environ. 2020, 740, 139384. [Google Scholar] [CrossRef] [PubMed]
- Dionizio, E.A.; Pimenta, F.M.; Lima, L.B.; Costa, M.H. Carbon stocks and dynamics of different land uses on the Cerrado agricultural frontier. PLoS ONE 2020, 15, e0241637. [Google Scholar] [CrossRef] [PubMed]
- Bellissimo-Rodrigues, F.; Machado, A.A.; Martinez, R. Paracoccidioidomycosis epidemiological features of a 1000-cases series from a hyperendemic area on the southeast of Brazil. Am. J. Trop. Med. Hyg. 2011, 85, 546–550. [Google Scholar] [CrossRef]
- Vieira Gde, D.; Alves Tda, C.; Lima, S.M.; Camargo, L.M.; Sousa, C.M. Paracoccidioidomycosis in a western Brazilian Amazon State: Clinical-epidemiologic profile and spatial distribution of the disease. Rev. Soc. Bras. Med. Trop. 2014, 47, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Campos, M.V.S.; Penna, G.O.; Castro, C.N.; Moraes, M.A.P.; Ferreira, M.S.; Santos, J.B. Paracoccidioidomycosis at Brasilia’s University Hospital. Rev. Soc. Bras. Med. Trop. 2008, 41, 4. [Google Scholar] [CrossRef] [Green Version]
- Loth, E.A.; Castro, S.V.; Silva, J.R.; Gandra, R.F. Occurrence of 102 cases of paracoccidioidomycosis in 18 months in the Itaipu Lake region, Western Paraná. Rev. Soc. Bras. Med. Trop. 2011, 44, 2. [Google Scholar] [CrossRef] [Green Version]
- Severo, L.C.; Roesch, E.W.; Oliveira, E.A.; Rocha, M.M.; Londero, A.T. Paracoccidioidomycosis in women. Rev. Iberoam. Micol. 1998, 15, 88–89. [Google Scholar]
- Paniago, A.M.; Aguiar, J.I.; Aguiar, E.S.; da Cunha, R.V.; Pereira, G.R.; Londero, A.T.; Wanke, B. Paracoccidioidomycosis: A clinical and epidemiological study of 422 cases observed in Mato Grosso do Sul. Rev. Soc. Bras. Med. Trop. 2003, 36, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Shankar, J.; Restrepo, A.; Clemons, K.V.; Stevens, D.A. Hormones and the resistance of women to paracoccidioidomycosis. Clin. Microbiol. Rev. 2011, 24, 296–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, A.L.; Tobon, A.; Restrepo, A.; Queiroz-Telles, F.; Nucci, M. Epidemiology of endemic systemic fungal infections in Latin America. Med. Mycol. 2011, 49, 785–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, J.; Wu, T.D.; Clemons, K.V.; Monteiro, J.P.; Mirels, L.F.; Stevens, D.A. Influence of 17beta-estradiol on gene expression of Paracoccidioides during mycelia-to-yeast transition. PLoS ONE 2011, 6, e28402. [Google Scholar] [CrossRef] [Green Version]
- Shikanai-Yasuda, M.A.; Mendes, R.P.; Colombo, A.L.; Queiroz-Telles, F.; Kono, A.S.G.; Paniago, A.M.; Nathan, A.; Valle, A.; Bagagli, E.; Benard, G.; et al. Brazilian guidelines for the clinical management of paracoccidioidomycosis. Rev. Soc. Bras. Med. Trop. 2017, 50, 715–740. [Google Scholar] [CrossRef]
- Barrozo, L.V.; Mendes, R.P.; Marques, S.A.; Benard, G.; Silva, M.E.; Bagagli, E. Climate and acute/subacute paracoccidioidomycosis in a hyper-endemic area in Brazil. Int. J. Epidemiol. 2009, 38, 1642–1649. [Google Scholar] [CrossRef] [Green Version]
- Restrepo, A.; McEwen, J.G.; Castaneda, E. The habitat of Paracoccidioides brasiliensis: How far from solving the riddle? Med. Mycol. 2001, 39, 233–241. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Gender | Total n = 106 | Female n = 29 | Male n = 77 | p | |
|---|---|---|---|---|---|
| Clinical form | Acute | 35 (33%) | 13 (44.8%) | 22 (28.6%) | NS |
| Chronic | 71 (67%) | 16 | 55 | ||
| Age | <50 years | 43 | 14 (48.3%) | 29 (37.7%) | NS |
| ≥50 years | 63 | 15 (51.7%) | 48 (62.3%) | ||
| Origin | Maranhão | 3 | 2 | 1 | NS |
| Mato Grosso | 1 | 0 | 1 | ||
| Pará | 19 | 5 | 14 | ||
| Tocantins | 83 (78.3%) | 22 (75.9%) | 61 (79.2%) | ||
| Occupation | Political advisor | 1 | 0 | 1 | p < 0.05 |
| Housewife | 17 (16%) | 17 | 0 | ||
| Student | 2 | 0 | 2 | ||
| Manager | 1 | 0 | 1 | ||
| Farmer | 71 (67%) | 10 | 61 | ||
| Driver | 2 | 0 | 2 | ||
| Machine operator | 3 | 0 | 3 | ||
| Locksmith | 1 | 0 | 1 | ||
| General services | 1 | 1 | 0 | ||
| Electronic technician | 1 | 0 | 1 | ||
| Technical nursing | 1 | 1 | 0 | ||
| Salesperson | 5 | 0 | 5 | ||
| Exposure (*) | In-house activities | 19 | 17 | 2 | p < 0.001 |
| Outdoor activities | 87 | 12 | 75 | ||
| Comorbidities | Cancer | 3 | 3 | 0 | NS |
| Leprosy | 1 | 0 | 1 | ||
| HIV | 2 | 0 | 2 | ||
| HIV/Tuberculosis | 1 | 0 | 1 | ||
| Cutaneous Leishmaniasis | 2 | 0 | 2 | ||
| Malaria | 1 | 1 | 0 | ||
| Tuberculosis | 3 | 0 | 3 | ||
| No coinfection | 93 | 25 (86.2%) | 68 (88.3%) | ||
| Total Positive for qPCR Assay n = 37 | gp43 Marker n = 21 | hsp70 Marker n = 11 | gp43/hsp70 Marker n = 5 | |||
|---|---|---|---|---|---|---|
| Age | <50 years | 14 | 6 | 5 | 3 | NS |
| ≥50 years | 23 | 15 | 6 | 2 | ||
| Gender | Female | 8 | 4 | 3 | 1 | NS |
| Male | 29 | 17 | 8 | 4 | ||
| Origin | Mato Grosso | 1 | 0 | 0 | 1 | p < 0.05 |
| Pará | 7 | 1 | 4 | 2 | ||
| Tocantins | 29 | 20 | 7 | 2 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krakhecke-Teixeira, A.G.; Yamauchi, D.H.; Rossi, A.; de Sousa, H.R.; Garces, H.G.; Júnior, J.L.; Júnior, A.O.S.; Felipe, M.S.S.; Bagagli, E.; de Andrade, H.F., Jr.; et al. Clinical and Eco-Epidemiological Aspects of a Novel Hyperendemic Area of Paracoccidioidomycosis in the Tocantins-Araguaia Basin (Northern Brazil), Caused by Paracoccidioides sp. J. Fungi 2022, 8, 502. https://doi.org/10.3390/jof8050502
Krakhecke-Teixeira AG, Yamauchi DH, Rossi A, de Sousa HR, Garces HG, Júnior JL, Júnior AOS, Felipe MSS, Bagagli E, de Andrade HF Jr., et al. Clinical and Eco-Epidemiological Aspects of a Novel Hyperendemic Area of Paracoccidioidomycosis in the Tocantins-Araguaia Basin (Northern Brazil), Caused by Paracoccidioides sp. Journal of Fungi. 2022; 8(5):502. https://doi.org/10.3390/jof8050502
Chicago/Turabian StyleKrakhecke-Teixeira, Alessandra G., Danielle H. Yamauchi, Alexsandra Rossi, Herdson R. de Sousa, Hans G. Garces, Joaquim L. Júnior, Antônio O. S. Júnior, Maria Sueli S. Felipe, Eduardo Bagagli, Heitor F. de Andrade, Jr., and et al. 2022. "Clinical and Eco-Epidemiological Aspects of a Novel Hyperendemic Area of Paracoccidioidomycosis in the Tocantins-Araguaia Basin (Northern Brazil), Caused by Paracoccidioides sp." Journal of Fungi 8, no. 5: 502. https://doi.org/10.3390/jof8050502
APA StyleKrakhecke-Teixeira, A. G., Yamauchi, D. H., Rossi, A., de Sousa, H. R., Garces, H. G., Júnior, J. L., Júnior, A. O. S., Felipe, M. S. S., Bagagli, E., de Andrade, H. F., Jr., & Teixeira, M. d. M. (2022). Clinical and Eco-Epidemiological Aspects of a Novel Hyperendemic Area of Paracoccidioidomycosis in the Tocantins-Araguaia Basin (Northern Brazil), Caused by Paracoccidioides sp. Journal of Fungi, 8(5), 502. https://doi.org/10.3390/jof8050502