
Molecular Diagnosis of Endemic Mycoses

Abstract
:1. Introduction
1.1. Epidemiology of Endemic Mycoses
1.2. Diagnosis of Endemic Mycoses
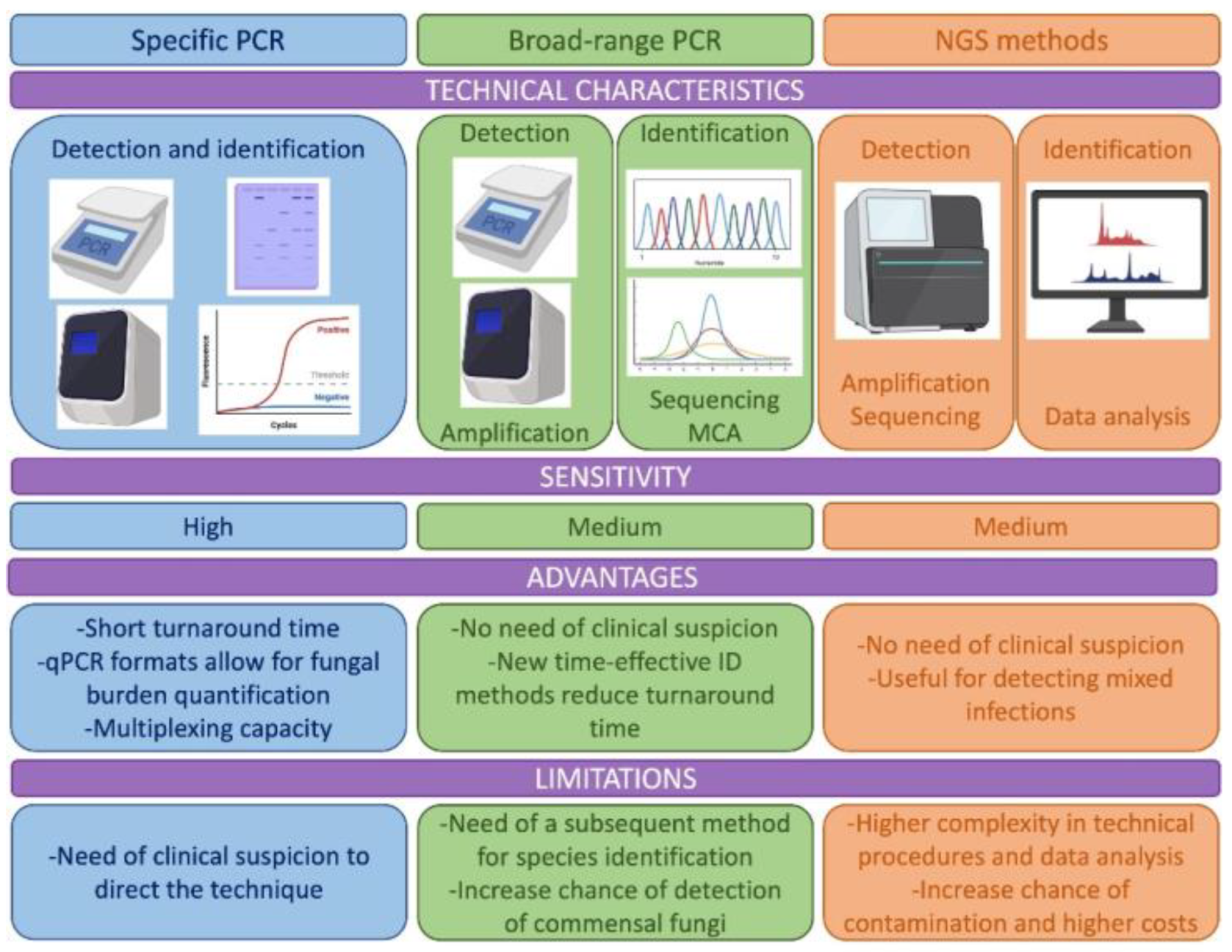
2. Specific PCR Assays
2.1. Histoplasmosis
2.2. Coccidiomycosis
2.3. Paracoccidioidomycosis
2.4. Blastomycosis
2.5. Talaromycosis
2.6. Conclusions

{kind=link}
| PCR Technology | Target | Sample | Sensitivity (Cases)/Specificity | Specificity | Ref |
|---|---|---|---|---|---|
| Histoplasmosis | |||||
| Conventional (nested) | 18S rDNA | Blood, spleen, lung (mice) | 83.1% | ND | [32] |
| Conventional (nested) | 100-kDa-like protein gene | Biopsy | 70% | 100% | [72] |
| Conventional | M antigen gene | ND | 100% | 100% | [39] |
| Conventional (semi-nested) | M antigen gene | Biopsy, blood, mucose, BM | ND (30) | ND | [38] |
| Real-time | ITS rDNA | BAL, lung biopsy, BM | 100% (3) | 100% | [35] |
| Conventional (nested) | 100-kDa-like protein gene | Blood, serum, BAL, BAS, biopsy, CSF, others | 100% (40) | 100% | [41] |
| Real-time | ITS rDNA | Blood, serum, BM, sputum, BAS, BAL, biopsy, CSF, others | 89% Proven H (54) 60% Probable H (13) | 100% | [31] |
| Real-time | ITS rDNA | BAL, biopsy, BM, CSF | 95.4% (348) | 96% | [36] |
| Real-time (multiplex) | ITS rDNA | BAL, biopsy, serum, BM | 92.5% (72) | 100% | [34] |
| Real-time | mtSSU gene | Blood, serum, BAL, BAS, biopsy, CSF, others | 97.7% (44) | ND | [37] |
| Conventional Real-time | PPK, CFP4 | FFPE tissue | 100% (2) | ND | [43] |
| Paracoccidioidomycosis | |||||
| Conventional (nested) | Gp43 | Biopsy (mice) | 91% (23) | ND | [57] |
| LAMP | Gp43 | Sputum | 60% (18) | ND | [59] |
| Conventional (semi-nested) | ITS rDNA | Biopsy (mice) | 100% (4) | 100% | [54] |
| Real-time | ITS rDNA | Serum, blood, sputum | 100% (6) | ND | [73] |
| Conventional | ITS rDNA | Serum, biopsy | ND | ND | [56] |
| Conventional (semi-nested) | ITS rDNA | Sputum | 100% (14) | ND | [74] |
| Conventional (nested) | GP43 gene | BAL, biopsy, sputum | 100% (25) | 100% | [55] |
| Real-time | Pb27 gene | Blood, serum, biopsy and others | 94% (78) | 100% | [58] |
| Coccidioidomycosis | |||||
| Conventional (nested)/real-time | Antigen2/Proline-Rich Antigen, | FFPE- biopsy | 100% (3) | ND | [75] |
| Real-time | ITS rDNA | Respiratory, biopsy, FFPE-biopsy | 89% (480) | 98% | [48] |
| Real-time | ITS rDNA | Mice samples | 98% (44) | 100% | [49] |
| Real-time | GeneSTAT Coccidioides assay | BAL/BW | 100% (332) | 93.85–100% | [52] |
| Blastomycosis | |||||
| Conventional (nested) | WI-1 (BAD 1) | PE-biopsy (dogs) | ND (73) | ND | [76] |
| Real-time | DRK-1 | Respiratory, biopsy and others | 86% (14) | 99.4% | [65] |
| Real-time | BAD-1 | FFPE-biopsy | 83% (12) | 100% | [64] |
| Real-time (duplex) | BAD-1 | FFPE-biopsy, respiratory and others | ND (33) | ND | [77] |
| Talaromycosis | |||||
| Real-time | 5.8S rDNA | Blood | 60% (20) | 100% | [78] |
| Conventional (nested) | 18S rDNA | Serum | 68.6% (35) | 100% | [67] |
| LAMP | ITS rDNA | Biopsy | 100% (12) | 100% | [71] |
| Conventional (nested)/ real-time | ITS rDNA | Blood, serum | 82% (22)/91% (22) | 75%/63% | [68] |
| Real-time | ITS rDNA | Serum | 86.11% (36) | ND | [69] |
3. Broad-Range PCRs
4. Next Generation Sequencing (NGS)
5. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gnat, S.; Lagowski, D.; Nowakiewicz, A.; Dylag, M. A global view on fungal infections in humans and animals: Infections caused by dimorphic fungi and dermatophytoses. J. Appl. Microbiol. 2021, 131, 2688–2704. [Google Scholar] [CrossRef] [PubMed]
- WHO. Fungal Priority Pathogens List to Guide Research, Development and Public Health Action; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Shikanai-Yasuda, M.A.; Mendes, R.P.; Colombo, A.L.; Queiroz-Telles, F.; Kono, A.S.G.; Paniago, A.M.M.; Nathan, A.; Valle, A.; Bagagli, E.; Benard, G.; et al. Brazilian guidelines for the clinical management of paracoccidioidomycosis. Rev. Soc. Bras. Med. Trop. 2017, 50, 715–740. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Le, T.; Chindamporn, A.; Kauffman, C.A.; Alastruey-Izquierdo, A.; Ampel, N.M.; Andes, D.R.; Armstrong-James, D.; Ayanlowo, O.; Baddley, J.W.; et al. Global guideline for the diagnosis and management of the endemic mycoses: An initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology. Lancet Infect. Dis. 2021, 21, e364–e374. [Google Scholar] [CrossRef] [PubMed]
- Gorris, M.E.; Cat, L.A.; Zender, C.S.; Treseder, K.K.; Randerson, J.T. Coccidioidomycosis Dynamics in Relation to Climate in the Southwestern United States. Geohealth 2018, 2, 6–24. [Google Scholar] [CrossRef] [PubMed]
- Salzer, H.J.F.; Stoney, R.J.; Angelo, K.M.; Rolling, T.; Grobusch, M.P.; Libman, M.; Lopez-Velez, R.; Duvignaud, A.; Asgeirsson, H.; Crespillo-Andujar, C.; et al. Epidemiological aspects of travel-related systemic endemic mycoses: A GeoSentinel analysis, 1997-2017. J. Travel Med. 2018, 25, tay055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashraf, N.; Kubat, R.C.; Poplin, V.; Adenis, A.A.; Denning, D.W.; Wright, L.; McCotter, O.; Schwartz, I.S.; Jackson, B.R.; Chiller, T.; et al. Re-drawing the Maps for Endemic Mycoses. Mycopathologia 2020, 185, 843–865. [Google Scholar] [CrossRef]
- Vallabhaneni, S.; Mody, R.K.; Walker, T.; Chiller, T. The Global Burden of Fungal Diseases. Infect. Dis. Clin. N. Am. 2016, 30, 1–11. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; Beale, M.A.; Hagen, F.; Fisher, M.C.; Terra, P.P.D.; de Hoog, S.; Brilhante, R.S.N.; de Aguiar Cordeiro, R.; de Souza Collares Maia Castelo-Branco, D.; Rocha, M.F.G.; et al. The global epidemiology of emerging Histoplasma species in recent years. Stud. Mycol. 2020, 97, 100095. [Google Scholar] [CrossRef]
- Benedict, K.; McCotter, O.Z.; Brady, S.; Komatsu, K.; Sondermeyer Cooksey, G.L.; Nguyen, A.; Jain, S.; Vugia, D.J.; Jackson, B.R. Surveillance for Coccidioidomycosis—United States, 2011-2017. MMWR Surveill Summ. 2019, 68, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Sondermeyer Cooksey, G.L.; Nguyen, A.; Vugia, D.; Jain, S. Regional Analysis of Coccidioidomycosis Incidence—California, 2000-2018. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1817–1821. [Google Scholar] [CrossRef]
- Van Dyke, M.C.C.; Thompson, G.R.; Galgiani, J.N.; Barker, B.M. The Rise of Coccidioides: Forces Against the Dust Devil Unleashed. Front. Immunol. 2019, 10, 2188. [Google Scholar] [CrossRef] [PubMed]
- Narayanasamy, S.; Dat, V.Q.; Thanh, N.T.; Ly, V.T.; Chan, J.F.; Yuen, K.Y.; Ning, C.; Liang, H.; Li, L.; Chowdhary, A.; et al. A global call for talaromycosis to be recognised as a neglected tropical disease. Lancet Glob. Health 2021, 9, e1618–e1622. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and Multi-National Prevalence of Fungal Diseases-Estimate Precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Bonifaz, A.; Gutierrez-Galhardo, M.C.; Mochizuki, T.; Li, S. Global epidemiology of sporotrichosis. Med. Mycol. 2015, 53, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mapengo, R.E.; Maphanga, T.G.; Grayson, W.; Govender, N.P. Endemic mycoses in South Africa, 2010-2020: A decade-long description of laboratory-diagnosed cases and prospects for the future. PLoS Negl. Trop. Dis. 2022, 16, e0010737. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Kenyon, C.; Feng, P.; Govender, N.P.; Dukik, K.; Sigler, L.; Jiang, Y.; Stielow, J.B.; Munoz, J.F.; Cuomo, C.A.; et al. 50 Years of Emmonsia Disease in Humans: The Dramatic Emergence of a Cluster of Novel Fungal Pathogens. PLoS Pathog. 2015, 11, e1005198. [Google Scholar] [CrossRef] [Green Version]
- Goncalves, F.G.; Rosa, P.S.; Belone, A.F.F.; Carneiro, L.B.; de Barros, V.L.Q.; Bispo, R.F.; Sbardelott, Y.; Neves, S.; Vittor, A.Y.; Woods, W.J.; et al. Lobomycosis Epidemiology and Management: The Quest for a Cure for the Most Neglected of Neglected Tropical Diseases. J. Fungi 2022, 8, 494. [Google Scholar] [CrossRef]
- Baker, J.; Setianingrum, F.; Wahyuningsih, R.; Denning, D.W. Mapping histoplasmosis in South East Asia—Implications for diagnosis in AIDS. Emerg. Microbes Infect. 2019, 8, 1139–1145. [Google Scholar] [CrossRef] [Green Version]
- McCotter, O.Z.; Benedict, K.; Engelthaler, D.M.; Komatsu, K.; Lucas, K.D.; Mohle-Boetani, J.C.; Oltean, H.; Vugia, D.; Chiller, T.M.; Sondermeyer Cooksey, G.L.; et al. Update on the Epidemiology of coccidioidomycosis in the United States. Med. Mycol. 2019, 57, S30–S40. [Google Scholar] [CrossRef]
- Amona, F.M.; Denning, D.W.; Moukassa, D.; Develoux, M.; Hennequin, C. Histoplasmosis in the Republic of Congo dominated by African histoplasmosis, Histoplasma capsulatum var. duboisii. PLoS Negl. Trop. Dis. 2021, 15, e0009318. [Google Scholar] [CrossRef]
- Rakislova, N.; Hurtado, J.C.; Palhares, A.E.M.; Ferreira, L.; Freire, M.; Lacerda, M.; Monteiro, W.; Navarro, M.; Casas, I.; Teixeira, M.M.; et al. High prevalence and mortality due to Histoplasma capsulatum in the Brazilian Amazon: An autopsy study. PLoS Negl. Trop. Dis. 2021, 15, e0009286. [Google Scholar] [CrossRef]
- Caceres, D.H.; Echeverri Tirado, L.C.; Bonifaz, A.; Adenis, A.; Gomez, B.L.; Flores, C.L.B.; Canteros, C.E.; Santos, D.W.; Arathoon, E.; Soto, E.R.; et al. Current situation of endemic mycosis in the Americas and the Caribbean: Proceedings of the first international meeting on endemic mycoses of the Americas (IMEMA). Mycoses 2022, 65, 1179–1187. [Google Scholar] [CrossRef]
- Wheat, L.J. Approach to the diagnosis of the endemic mycoses. Clin. Chest Med. 2009, 30, 379–389, viii. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.; Page, I. Role of Serological Tests in the Diagnosis of Mold Infections. Curr. Fungal Infect. Rep. 2018, 12, 127–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassis, C.; Durkin, M.; Holbrook, E.; Myers, R.; Wheat, L. Advances in Diagnosis of Progressive Pulmonary and Disseminated Coccidioidomycosis. Clin. Infect. Dis. 2021, 72, 968–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongomin, F.; Govender, N.P.; Chakrabarti, A.; Robert-Gangneux, F.; Boulware, D.R.; Zafar, A.; Oladele, R.O.; Richardson, M.D.; Gangneux, J.P.; Alastruey-Izquierdo, A.; et al. Essential in vitro diagnostics for advanced HIV and serious fungal diseases: International experts’ consensus recommendations. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1581–1584. [Google Scholar] [CrossRef] [Green Version]
- Cáceres, D.H.; Gómez, B.L.; Tobon, A.M.; Minderman, M.; Bridges, N.; Chiller, T.; Lindsley, M.D. Validation and Concordance Analysis of a New Lateral Flow Assay for Detection of Histoplasma Antigen in Urine. J. Fungi 2021, 7, 799. [Google Scholar] [CrossRef]
- Donovan, F.M.; Ramadan, F.A.; Khan, S.A.; Bhaskara, A.; Lainhart, W.D.; Narang, A.T.; Mosier, J.M.; Ellingson, K.D.; Bedrick, E.J.; Saubolle, M.A.; et al. Comparison of a Novel Rapid Lateral Flow Assay to Enzyme Immunoassay Results for Early Diagnosis of Coccidioidomycosis. Clin. Infect. Dis. 2021, 73, e2746–e2753. [Google Scholar] [CrossRef]
- Van Dyke, M.C.C.; Teixeira, M.M.; Barker, B.M. Fantastic yeasts and where to find them: The hidden diversity of dimorphic fungal pathogens. Curr. Opin. Microbiol. 2019, 52, 55–63. [Google Scholar] [CrossRef]
- Buitrago, M.J.; Bernal-Martinez, L.; Castelli, M.V.; Rodriguez-Tudela, J.L.; Cuenca-Estrella, M. Histoplasmosis and paracoccidioidomycosis in a non-endemic area: A review of cases and diagnosis. J. Travel Med. 2011, 18, 26–33. [Google Scholar] [CrossRef]
- Bialek, R.; Fischer, J.; Feucht, A.; Najvar, L.K.; Dietz, K.; Knobloch, J.; Graybill, J.R. Diagnosis and monitoring of murine histoplasmosis by a nested PCR assay. J. Clin. Microbiol. 2001, 39, 1506–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buitrago, M.J.; Berenguer, J.; Mellado, E.; Rodriguez-Tudela, J.L.; Cuenca-Estrella, M. Detection of imported histoplasmosis in serum of HIV-infected patients using a real-time PCR-based assay. Eur. J. Clin. Microbiol. Infect. Dis. 2006, 25, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Gago, S.; Esteban, C.; Valero, C.; Zaragoza, O.; Puig de la Bellacasa, J.; Buitrago, M.J. A multiplex real-time PCR assay for identification of Pneumocystis jirovecii, Histoplasma capsulatum, and Cryptococcus neoformans/Cryptococcus gattii in samples from AIDS patients with opportunistic pneumonia. J. Clin. Microbiol. 2014, 52, 1168–1176. [Google Scholar] [CrossRef] [Green Version]
- Martagon-Villamil, J.; Shrestha, N.; Sholtis, M.; Isada, C.M.; Hall, G.S.; Bryne, T.; Lodge, B.A.; Reller, L.B.; Procop, G.W. Identification of Histoplasma capsulatum from culture extracts by real-time PCR. J. Clin. Microbiol. 2003, 41, 1295–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, S.; Veron, V.; Boukhari, R.; Blanchet, D.; Aznar, C. Detection of Histoplasma capsulatum DNA in human samples by real-time polymerase chain reaction. Diagn. Microbiol. Infect. Dis. 2010, 66, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Alanio, A.; Gits-Muselli, M.; Lanternier, F.; Sturny-Leclère, A.; Benazra, M.; Hamane, S.; Rodrigues, A.M.; García-Hermoso, D.; Lortholary, O.; Dromer, F.; et al. Evaluation of a New Histoplasma spp. Quantitative RT-PCR Assay. J. Mol. Diagn. 2021, 23, 698–709. [Google Scholar] [CrossRef] [PubMed]
- Bracca, A.; Tosello, M.E.; Girardini, J.E.; Amigot, S.L.; Gomez, C.; Serra, E. Molecular detection of Histoplasma capsulatum var. capsulatum in human clinical samples. J. Clin. Microbiol. 2003, 41, 1753–1755. [Google Scholar] [CrossRef] [Green Version]
- Guedes, H.L.; Guimaraes, A.J.; Muniz Mde, M.; Pizzini, C.V.; Hamilton, A.J.; Peralta, J.M.; Deepe, G.S., Jr.; Zancopé-Oliveira, R.M. PCR assay for identification of Histoplasma capsulatum based on the nucleotide sequence of the M antigen. J. Clin. Microbiol. 2003, 41, 535–539. [Google Scholar] [CrossRef] [Green Version]
- López, L.F.; Munoz, C.O.; Cáceres, D.H.; Tobon, A.M.; Loparev, V.; Clay, O.; Chiller, T.; Litvintseva, A.; Gade, L.; Gonzalez, A.; et al. Standardization and validation of real time PCR assays for the diagnosis of histoplasmosis using three molecular targets in an animal model. PLoS ONE 2017, 12, e0190311. [Google Scholar] [CrossRef]
- Maubon, D.; Simon, S.; Aznar, C. Histoplasmosis diagnosis using a polymerase chain reaction method. Application on human samples in French Guiana, South America. Diagn. Microbiol. Infect. Dis. 2007, 58, 441–444. [Google Scholar] [CrossRef]
- Rickerts, V.; Bialek, R.; Tintelnot, K.; Jacobi, V.; Just-Nubling, G. Rapid PCR-based diagnosis of disseminated histoplasmosis in an AIDS patient. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 821–823. [Google Scholar] [CrossRef]
- Gallo, J.E.; Torres, I.; Gomez, O.M.; Rishishwar, L.; Vannberg, F.; Jordan, I.K.; McEwen, J.G.; Clay, O.K. New Histoplasma Diagnostic Assays Designed via Whole Genome Comparisons. J. Fungi 2021, 7, 544. [Google Scholar] [CrossRef] [PubMed]
- Caceres, D.H.; Knuth, M.; Derado, G.; Lindsley, M.D. Diagnosis of Progressive Disseminated Histoplasmosis in Advanced HIV: A Meta-Analysis of Assay Analytical Performance. J. Fungi 2019, 5, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zatti, M.D.S.; Arantes, T.D.; Fernandes, J.A.L.; Bay, M.B.; Milan, E.P.; Naliato, G.F.S.; Theodoro, R.C. Loop-mediated Isothermal Amplification and nested PCR of the Internal Transcribed Spacer (ITS) for Histoplasma capsulatum detection. PLoS Negl. Trop. Dis. 2019, 13, e0007692. [Google Scholar] [CrossRef] [PubMed]
- Scheel, C.M.; Zhou, Y.; Theodoro, R.C.; Abrams, B.; Balajee, S.A.; Litvintseva, A.P. Development of a loop-mediated isothermal amplification method for detection of Histoplasma capsulatum DNA in clinical samples. J. Clin. Microbiol. 2014, 52, 483–488. [Google Scholar] [CrossRef] [Green Version]
- Buitrago, M.J.; Canteros, C.E.; Frias De Leon, G.; Gonzalez, A.; Marques-Evangelista De Oliveira, M.; Munoz, C.O.; Ramirez, J.A.; Toranzo, A.I.; Zancope-Oliveira, R.; Cuenca-Estrella, M. Comparison of PCR protocols for detecting Histoplasma capsulatum DNA through a multicenter study. Rev. Iberoam Micol. 2013, 30, 256–260. [Google Scholar] [CrossRef]
- Binnicker, M.J.; Buckwalter, S.P.; Eisberner, J.J.; Stewart, R.A.; McCullough, A.E.; Wohlfiel, S.L.; Wengenack, N.L. Detection of Coccidioides species in clinical specimens by real-time PCR. J. Clin. Microbiol. 2007, 45, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Gago, S.; Buitrago, M.J.; Clemons, K.V.; Cuenca-Estrella, M.; Mirels, L.F.; Stevens, D.A. Development and validation of a quantitative real-time PCR assay for the early diagnosis of coccidioidomycosis. Diagn. Microbiol. Infect. Dis. 2014, 79, 214–221. [Google Scholar] [CrossRef]
- Bowers, J.R.; Parise, K.L.; Kelley, E.J.; Lemmer, D.; Schupp, J.M.; Driebe, E.M.; Engelthaler, D.M.; Keim, P.; Barker, B.M. Direct detection of Coccidioides from Arizona soils using CocciENV, a highly sensitive and specific real-time PCR assay. Med. Mycol. 2019, 57, 246–255. [Google Scholar] [CrossRef] [Green Version]
- Lauer, A.; Baal, J.D.; Baal, J.C.; Verma, M.; Chen, J.M. Detection of Coccidioides immitis in Kern County, California, by multiplex PCR. Mycologia 2012, 104, 62–69. [Google Scholar] [CrossRef]
- Saubolle, M.A.; Wojack, B.R.; Wertheimer, A.M.; Fuayagem, A.Z.; Young, S.; Koeneman, B.A. Multicenter Clinical Validation of a Cartridge-Based Real-Time PCR System for Detection of Coccidioides spp. in Lower Respiratory Specimens. J. Clin. Microbiol. 2018, 56, e01277-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnock, D.W. Coccidioides species as potential agents of bioterrorism. Future Microbiol. 2007, 2, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Koishi, T.; Yasuoka, K.; Zeng, X.C.; Fujikawa, S. Molecular dynamics simulations of urea-water binary droplets on flat and pillared hydrophobic surfaces. Faraday Discuss 2010, 146, 185–193; discussion 195–215, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Gaviria, M.; Rivera, V.; Munoz-Cadavid, C.; Cano, L.E.; Naranjo, T.W. Validation and clinical application of a nested PCR for paracoccidioidomycosis diagnosis in clinical samples from Colombian patients. Braz. J. Infect. Dis. 2015, 19, 376–383. [Google Scholar] [CrossRef] [Green Version]
- Dias, L.; de Carvalho, L.F.; Romano, C.C. Application of PCR in serum samples for diagnosis of paracoccidioidomycosis in the southern Bahia-Brazil. PLoS Negl. Trop. Dis. 2012, 6, e1909. [Google Scholar] [CrossRef] [Green Version]
- Bialek, R.; Ibricevic, A.; Aepinus, C.; Najvar, L.K.; Fothergill, A.W.; Knobloch, J.; Graybill, J.R. Detection of Paracoccidioides brasiliensis in tissue samples by a nested PCR assay. J. Clin. Microbiol. 2000, 38, 2940–2942. [Google Scholar] [CrossRef] [Green Version]
- Rocha-Silva, F.; Maria de Figueiredo, S.; Rutren La Santrer, E.F.; Machado, A.S.; Fernandes, B.; Assuncao, C.B.; Goes, A.M.; Caligiorne, R.B. Paracoccidioidomycosis: Detection of Paracoccidioides brasiliensis genome in biological samples by quantitative chain reaction polymerase (qPCR). Microb. Pathog. 2018, 121, 359–362. [Google Scholar] [CrossRef]
- Tatibana, B.T.; Sano, A.; Uno, J.; Kamei, K.; Igarashi, T.; Mikami, Y.; Miyaji, M.; Nishimura, K.; Itano, E.N. Detection of Paracoccidioides brasiliensis gp43 gene in sputa by loop-mediated isothermal amplification method. J. Clin. Lab. Anal. 2009, 23, 139–143. [Google Scholar] [CrossRef]
- Onda, H.; Komine, M.; Murata, S.; Ohtsuki, M. Letter: Imported paracoccidioidomycosis in Japan. Dermatol. Online J. 2011, 17, 11. [Google Scholar] [CrossRef]
- Ginarte, M.; Pereiro, M., Jr.; Toribio, J. Imported paracoccidioidomycosis in Spain. Mycoses 2003, 46, 407–411. [Google Scholar] [CrossRef]
- Botas-Velasco, M.; Jover-Diaz, F.; Ortiz de la Tabla-Duccase, V.; Martinez-Garcia, C. [Imported paracoccidioidomycosis in Spain]. Enferm. Infecc. Microbiol. Clin. 2010, 28, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.W.; Schwan, W.R.; Volk, T.J. PCR-based detection of DNA from the human pathogen Blastomyces dermatitidis from natural soil samples. Med. Mycol. 2006, 44, 741–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidamonidze, K.; Peck, M.K.; Perez, M.; Baumgardner, D.; Smith, G.; Chaturvedi, V.; Chaturvedi, S. Real-time PCR assay for identification of Blastomyces dermatitidis in culture and in tissue. J. Clin. Microbiol. 2012, 50, 1783–1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babady, N.E.; Buckwalter, S.P.; Hall, L.; Le Febre, K.M.; Binnicker, M.J.; Wengenack, N.L. Detection of Blastomyces dermatitidis and Histoplasma capsulatum from culture isolates and clinical specimens by use of real-time PCR. J. Clin. Microbiol. 2011, 49, 3204–3208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, C.; Lai, J.; Wei, W.; Zhou, B.; Huang, J.; Jiang, J.; Liang, B.; Liao, Y.; Zang, N.; Cao, C.; et al. Accuracy of rapid diagnosis of Talaromyces marneffei: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0195569. [Google Scholar] [CrossRef] [Green Version]
- Pongpom, M.; Sirisanthana, T.; Vanittanakom, N. Application of nested PCR to detect Penicillium marneffei in serum samples. Med. Mycol. 2009, 47, 549–553. [Google Scholar] [CrossRef] [Green Version]
- Lu, S.; Li, X.; Calderone, R.; Zhang, J.; Ma, J.; Cai, W.; Xi, L. Whole blood Nested PCR and Real-time PCR amplification of Talaromyces marneffei specific DNA for diagnosis. Med. Mycol. 2016, 54, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Zheng, Y.; Wu, F.; Mo, D.; Liang, G.; Yan, R.; Khader, J.A.; Wu, N.; Cao, C. Evaluation of quantitative real-time PCR and Platelia galactomannan assays for the diagnosis of disseminated Talaromyces marneffei infection. Med. Mycol. 2020, 58, 181–186. [Google Scholar] [CrossRef]
- Hien, H.T.A.; Thanh, T.T.; Thu, N.T.M.; Nguyen, A.; Thanh, N.T.; Lan, N.P.H.; Simmons, C.; Shikuma, C.; Chau, N.V.V.; Thwaites, G.; et al. Development and evaluation of a real-time polymerase chain reaction assay for the rapid detection of Talaromyces marneffei MP1 gene in human plasma. Mycoses 2016, 59, 773–780. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Li, X.; Zeng, H.; Xie, Z.; Lu, C.; Xi, L.; de Hoog, G.S. Development and evaluation of loop-mediated isothermal amplification (LAMP) for the rapid diagnosis of Penicillium marneffei in archived tissue samples. FEMS Immunol. Med. Microbiol. 2010, 58, 381–388. [Google Scholar] [CrossRef]
- Bialek, R.; Feucht, A.; Aepinus, C.; Just-Nubling, G.; Robertson, V.J.; Knobloch, J.; Hohle, R. Evaluation of two nested PCR assays for detection of Histoplasma capsulatum DNA in human tissue. J. Clin. Microbiol. 2002, 40, 1644–1647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buitrago, M.J.; Merino, P.; Puente, S.; Gomez-Lopez, A.; Arribi, A.; Zancope-Oliveira, R.M.; Gutierrez, M.C.; Rodriguez-Tudela, J.L.; Cuenca-Estrella, M. Utility of real-time PCR for the detection of Paracoccidioides brasiliensis DNA in the diagnosis of imported paracoccidioidomycosis. Med. Mycol. 2009, 47, 879–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitz Ade, F.; Koishi, A.C.; Tavares, E.R.; Andrade, F.G.; Loth, E.A.; Gandra, R.F.; Venancio, E.J. An optimized one-tube, semi-nested PCR assay for Paracoccidioides brasiliensis detection. Rev. Soc. Bras. Med. Trop. 2013, 46, 783–785. [Google Scholar] [CrossRef] [PubMed]
- Bialek, R.; Kern, J.; Herrmann, T.; Tijerina, R.; Cecenas, L.; Reischl, U.; Gonzalez, G.M. PCR assays for identification of Coccidioides posadasii based on the nucleotide sequence of the antigen 2/proline-rich antigen. J. Clin. Microbiol. 2004, 42, 778–783. [Google Scholar] [CrossRef] [Green Version]
- Bialek, R.; Cirera, A.C.; Herrmann, T.; Aepinus, C.; Shearn-Bochsler, V.I.; Legendre, A.M. Nested PCR assays for detection of Blastomyces dermatitidis DNA in paraffin-embedded canine tissue. J. Clin. Microbiol. 2003, 41, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, M.; Zhu, Y.; Kus, J.V.; McTaggart, L.; Chaturvedi, V.; Chaturvedi, S. Development of a Duplex Real-Time PCR Assay for the Differentiation of Blastomyces dermatitidis and Blastomyces gilchristii and a Retrospective Analysis of Culture and Primary Specimens from Blastomycosis Cases from New York (2005 to 2019). J. Clin. Microbiol. 2021, 59, e02078-20. [Google Scholar] [CrossRef]
- Pornprasert, S.; Praparattanapan, J.; Khamwan, C.; Pawichai, S.; Pimsarn, P.; Samleerat, T.; Leechanachai, P.; Supparatpinyo, K. Development of TaqMan real-time polymerase chain reaction for the detection and identification of Penicillium marneffei. Mycoses 2009, 52, 487–492. [Google Scholar] [CrossRef]
- Kidd, S.E.; Chen, S.C.; Meyer, W.; Halliday, C.L. A New Age in Molecular Diagnostics for Invasive Fungal Disease: Are We Ready? Front. Microbiol. 2019, 10, 2903. [Google Scholar] [CrossRef] [Green Version]
- White, P.L.; Alanio, A.; Brown, L.; Cruciani, M.; Hagen, F.; Gorton, R.; Lackner, M.; Millon, L.; Morton, C.O.; Rautemaa-Richardson, R.; et al. An overview of using fungal DNA for the diagnosis of invasive mycoses. Expert. Rev. Mol. Diagn. 2022, 22, 169–184. [Google Scholar] [CrossRef]
- Buitrago, M.J.; Valero, C. Diagnosis of Fungal Infections; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Imhof, A.; Schaer, C.; Schoedon, G.; Schaer, D.J.; Walter, R.B.; Schaffner, A.; Schneemann, M. Rapid detection of pathogenic fungi from clinical specimens using LightCycler real-time fluorescence PCR. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 558–560. [Google Scholar] [CrossRef] [Green Version]
- Trubiano, J.A.; Dennison, A.M.; Morrissey, C.O.; Chua, K.Y.; Halliday, C.L.; Chen, S.C.; Spelman, D. Clinical utility of panfungal polymerase chain reaction for the diagnosis of invasive fungal disease: A single center experience. Med. Mycol. 2016, 54, 138–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ala-Houhala, M.; Koukila-Kahkola, P.; Antikainen, J.; Valve, J.; Kirveskari, J.; Anttila, V.J. Clinical use of fungal PCR from deep tissue samples in the diagnosis of invasive fungal diseases: A retrospective observational study. Clin. Microbiol. Infect. 2018, 24, 301–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindner, A.K.; Rickerts, V.; Kurth, F.; Wilmes, D.; Richter, J. Chronic oral ulceration and lip swelling after a long term stay in Guatemala: A diagnostic challenge. Travel. Med. Infect. Dis. 2018, 23, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Wilmes, D.; McCormick-Smith, I.; Lempp, C.; Mayer, U.; Schulze, A.B.; Theegarten, D.; Hartmann, S.; Rickerts, V. Detection of Histoplasma DNA from Tissue Blocks by a Specific and a Broad-Range Real-Time PCR: Tools to Elucidate the Epidemiology of Histoplasmosis. J. Fungi 2020, 6, 319. [Google Scholar] [CrossRef]
- Buitrago, M.J.; Bernal-Martinez, L.; Castelli, M.V.; Rodriguez-Tudela, J.L.; Cuenca-Estrella, M. Performance of panfungal--and specific-PCR-based procedures for etiological diagnosis of invasive fungal diseases on tissue biopsy specimens with proven infection: A 7-year retrospective analysis from a reference laboratory. J. Clin. Microbiol. 2014, 52, 1737–1740. [Google Scholar] [CrossRef] [Green Version]
- Morjaria, S.; Otto, C.; Moreira, A.; Chung, R.; Hatzoglou, V.; Pillai, M.; Banaei, N.; Tang, Y.W.; Figueroa, C.J. Ribosomal RNA gene sequencing for early diagnosis of Blastomyces dermatitidis infection. Int. J. Infect. Dis. 2015, 37, 122–124. [Google Scholar] [CrossRef] [Green Version]
- Rooms, I.; Mugisha, P.; Gambichler, T.; Hadaschik, E.; Esser, S.; Rath, P.M.; Haase, G.; Wilmes, D.; McCormick-Smith, I.; Rickerts, V. Disseminated Emergomycosis in a Person with HIV Infection, Uganda. Emerg. Infect. Dis. 2019, 25, 1750–1751. [Google Scholar] [CrossRef]
- Beltrame, A.; Danesi, P.; Farina, C.; Orza, P.; Perandin, F.; Zanardello, C.; Rodari, P.; Staffolani, S.; Bisoffi, Z. Case Report: Molecular Confirmation of Lobomycosis in an Italian Traveler Acquired in the Amazon Region of Venezuela. Am. J. Trop. Med. Hyg. 2017, 97, 1757–1760. [Google Scholar] [CrossRef] [Green Version]
- Valero, C.; de la Cruz-Villar, L.; Zaragoza, O.; Buitrago, M.J. New Panfungal Real-Time PCR Assay for Diagnosis of Invasive Fungal Infections. J. Clin. Microbiol. 2016, 54, 2910–2918. [Google Scholar] [CrossRef]
- Gade, L.; Hurst, S.; Balajee, S.A.; Lockhart, S.R.; Litvintseva, A.P. Detection of mucormycetes and other pathogenic fungi in formalin fixed paraffin embedded and fresh tissues using the extended region of 28S rDNA. Med. Mycol. 2017, 55, 385–395. [Google Scholar] [CrossRef] [Green Version]
- Gomez, C.A.; Budvytiene, I.; Zemek, A.J.; Banaei, N. Performance of Targeted Fungal Sequencing for Culture-Independent Diagnosis of Invasive Fungal Disease. Clin. Infect. Dis. 2017, 65, 2035–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabino, R.; Simoes, H.; Verissimo, C. Detection of deep fungal infections: A polyphasic approach. J. Med. Microbiol. 2019, 68, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Lefterova, M.I.; Suarez, C.J.; Banaei, N.; Pinsky, B.A. Next-Generation Sequencing for Infectious Disease Diagnosis and Management: A Report of the Association for Molecular Pathology. J. Mol. Diagn. 2015, 17, 623–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forbes, J.D.; Knox, N.C.; Ronholm, J.; Pagotto, F.; Reimer, A. Metagenomics: The Next Culture-Independent Game Changer. Front. Microbiol. 2017, 8, 1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boers, S.A.; Jansen, R.; Hays, J.P. Understanding and overcoming the pitfalls and biases of next-generation sequencing (NGS) methods for use in the routine clinical microbiological diagnostic laboratory. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1059–1070. [Google Scholar] [CrossRef] [Green Version]
- McTaggart, L.R.; Copeland, J.K.; Surendra, A.; Wang, P.W.; Husain, S.; Coburn, B.; Guttman, D.S.; Kus, J.V. Mycobiome Sequencing and Analysis Applied to Fungal Community Profiling of the Lower Respiratory Tract During Fungal Pathogenesis. Front. Microbiol. 2019, 10, 512. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Shen, H.; Yang, C.; Jia, Q.; Li, J.; Chen, Y.; Hu, J.; Huang, W. Clinical performance of metagenomic next-generation sequencing for the rapid diagnosis of talaromycosis in HIV-infected patients. Front. Cell Infect Microbiol. 2022, 12, 962441. [Google Scholar] [CrossRef]
- Zhu, Y.M.; Ai, J.W.; Xu, B.; Cui, P.; Cheng, Q.; Wu, H.; Qian, Y.Y.; Zhang, H.C.; Zhou, X.; Xing, L.; et al. Rapid and precise diagnosis of disseminated T. marneffei infection assisted by high-throughput sequencing of multifarious specimens in a HIV-negative patient: A case report. BMC Infect. Dis. 2018, 18, 379. [Google Scholar] [CrossRef]
- Wang, D.M.; Ma, H.L.; Tan, M.Q.; Wu, Y.M.; Wang, S.N. Next-generation sequencing confirmed the diagnosis of isolated central nervous system infection caused by Talaromyces marneffei in an immunocompetent patient. Chin. Med. J. 2020, 133, 374–376. [Google Scholar] [CrossRef]
- Zhang, W.; Ye, J.; Qiu, C.; Wang, L.; Jin, W.; Jiang, C.; Xu, L.; Xu, J.; Li, Y.; Wang, L.; et al. Rapid and precise diagnosis of T. marneffei pulmonary infection in a HIV-negative patient with autosomal-dominant STAT3 mutation: A case report. Ther. Adv. Respir. Dis. 2020, 14, 1753466620929225. [Google Scholar] [CrossRef]
- Du, R.; Feng, Y.; Liu, L.N.; Liu, Y.B.; Ye, H.; Lu, X.J.; Wang, X.H.; Zong, Z.Y. [Pathogen Diagnosis of a Febrile HIV Case by the Metagenomic Next-generation Sequencing]. Sichuan Da Xue Xue Bao Yi Xue Ban 2020, 51, 257–260. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, D.; Du, J.; Zhou, Y.; Cai, Y.; Sun, R.; Zhou, J.; Tian, J.; Wu, H.; Lu, M.; et al. Rapid diagnosis of Talaromyces marneffei infection assisted by metagenomic next-generation sequencing in a HIV-negative patient. IDCases 2021, 23, e01055. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Wu, L.; Cai, J.; Chen, H. An Iris Tumor Secondary to Talaromyces marneffei Infection in a Patient with AIDS and Syphilis. Ocul. Immunol. Inflamm. 2022, 30, 1129–1132. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Yang, N.; Qian, G. Case Report: Metagenomic Next-Generation Sequencing in Diagnosis of Talaromycosis of an Immunocompetent Patient. Front. Med. 2021, 8, 656194. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Liu, Y.; Wen, Y. Gastrointestinal manifestations of Talaromyces marneffei infection in an HIV-infected patient rapidly verified by metagenomic next-generation sequencing: A case report. BMC Infect. Dis. 2021, 21, 376. [Google Scholar] [CrossRef]
- Shen, Q.; Sheng, L.; Zhou, J. HIV-negative case of Talaromyces marneffei pulmonary infection with a TSC2 mutation. J. Int. Med. Res. 2021, 49, 3000605211016761. [Google Scholar] [CrossRef]
- Wilson, M.R.; O’Donovan, B.D.; Gelfand, J.M.; Sample, H.A.; Chow, F.C.; Betjemann, J.P.; Shah, M.P.; Richie, M.B.; Gorman, M.P.; Hajj-Ali, R.A.; et al. Chronic Meningitis Investigated via Metagenomic Next-Generation Sequencing. JAMA Neurol. 2018, 75, 947–955. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, W.; Ling, H.; Dong, X.; Zhang, Y.; Li, J.; Zhang, Y.; Song, J.; Liu, W.J.; Li, Y.; et al. Identification of Histoplasma causing an unexplained disease cluster in Matthews Ridge, Guyana. Biosaf. Health 2019, 1, 150–154. [Google Scholar] [CrossRef]
- Chen, J.; Li, Y.; Li, Z.; Chen, G.; Liu, X.; Ding, L. Metagenomic next-generation sequencing identified Histoplasma capsulatum in the lung and epiglottis of a Chinese patient: A case report. Int. J. Infect. Dis. 2020, 101, 33–37. [Google Scholar] [CrossRef]
- Muldoon, J.L.; Wysozan, T.R.; Toubin, Y.; Relich, R.F.; Davis, T.E.; Zhang, C.; Alomari, A.K. An unusual presentation of cutaneous histoplasmosis as a recurrent solitary and spontaneously healing lesion in an immunocompetent patient. Access Microbiol. 2020, 2, acmi000156. [Google Scholar] [CrossRef]
- Wang, N.; Zhao, C.; Tang, C.; Wang, L. Case Report and Literature Review: Disseminated Histoplasmosis Infection Diagnosed by Metagenomic Next-Generation Sequencing. Infect. Drug. Resist. 2022, 15, 4507–4514. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.; Yadav, M.; Singhania, N.; Samal, S.; Singhania, G. Blastomycosis Detected by Microbial Cell-Free DNA in Renal Transplant Recipient. Am. J. Med. 2020, 133, e599–e600. [Google Scholar] [CrossRef]
- Wang, N.; Luo, Z.; Deng, S.; Li, Q. A young male with chronic nonproductive cough diagnosed with blastomycosis in China: A case report. BMC Pulm. Med. 2020, 20, 189. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.C.; Zhang, Q.R.; Ai, J.W.; Cui, P.; Wu, H.L.; Zhang, W.H.; Wang, T. The role of bone marrow metagenomics next-generation sequencing to differential diagnosis among visceral leishmaniasis, histoplasmosis, and talaromycosis marneffei. Int. J. Lab. Hematol. 2020, 42, e52–e54. [Google Scholar] [CrossRef]
- Larkin, P.M.K.; Lawson, K.L.; Contreras, D.A.; Le, C.Q.; Trejo, M.; Realegeno, S.; Hilt, E.E.; Chandrasekaran, S.; Garner, O.B.; Fishbein, G.A.; et al. Amplicon-Based Next-Generation Sequencing for Detection of Fungi in Formalin-Fixed, Paraffin-Embedded Tissues: Correlation with Histopathology and Clinical Applications. J. Mol. Diagn. 2020, 22, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Martinez, L.; Herrera, L.; Valero, C.; de la Cruz, P.; Ghimpu, L.; Mesa-Arango, A.C.; Santoni, G.; Goterris, L.; Millan, R.; Buitrago, M.J. Differential Diagnosis of Fungal Pneumonias vs. Tuberculosis in AIDS Patients by Using Two New Molecular Methods. J. Fungi 2021, 7, 336. [Google Scholar] [CrossRef]

| Target | Sample | Post-PCR ID Method | Notes | Ref |
|---|---|---|---|---|
| Histoplasmosis | ||||
| rDNA (18S) | BM | Sanger sequencing | Confirmed by histopathology and culture | [82] |
| rDNA (ITS1) | BM | Sanger sequencing | Confirmed by culture | [83] |
| rDNA (ITS, 28S) | Lung tissue | Sanger sequencing | Confirmed by histopathology | [84] |
| rDNA (28S) | Mucosal biopsy | Sanger sequencing | Confirmed by specific PCR | [85] |
| rDNA (28S) | FFPE tissue | Sanger sequencing | Confirmed by histopathology and specific qPCR | [86] |
| Coccidioidomycosis | ||||
| rDNA (ITS) | Biopsy | Sanger sequencing | Confirmed by histopathology, qPCR format | [87] |
| Blastomycosis | ||||
| rDNA (ITS2 and D2) | FFPE tissue | Sanger sequencing | Confirmed by histopathology | [88] |
| Emergomycosis | ||||
| rDNA (28S, ITS2) | FFPE tissue | Sanger sequencing | Confirmed by histopathology | [89] |
| Lobomycosis | ||||
| rDNA (ITS1-4) | Biopsy | Sanger sequencing | Confirmed by histopathology | [90] |
| Multiple EM identified | ||||
| rDNA (ITS2) | Biopsies | MCA and sanger sequencing | Histoplasmosis, coccidioidomycosis, paracoccidioidomycosis. Confirmed by histopathology | [91] |
| rDNA (28S, ITS2, D1-D2) | FFPE and fresh tissue | Sanger sequencing | Histoplasmosis, talaromycosis, blastomycosis. Some cases confirmed by histopathology | [92] |
| rDNA (ITS2, D2) | FFPE tissue | Sanger sequencing | Histoplasmosis, coccidioidomycosis. Confirmed by histopathology, qPCR format | [93] |
| rDNA (ITS1-2) | FFPE and fresh tissue | Sanger sequencing | Histoplasmosis, paracoccidioidomycosis. Confirmed by culture or histopathology | [94] |
| Target | Samples | Aim | Notes | Ref |
|---|---|---|---|---|
| Talaromycosis | ||||
| Total DNA | BAL, CSF and BM | Diagnosis of a patient with a 3-months record of undiagnosed disease | Confirmed by histopathology and positive culture in skin lesion | [100] |
| Total DNA | CSF | Diagnosis of a patient with meningoencephalitis | [101] | |
| Not mentioned | BAL | Diagnosis of a patient with chronic pneumonia | Confirmed by culture in BAL | [102] |
| Total DNA | Peripheral blood | Diagnosis of HIV febrile patient | Confirmed by panfungal PCR on lymph node biopsy | [103] |
| Not mentioned | BAL | Diagnosis of a patient with chronic pneumonia | Confirmed by culture in BAL | [104] |
| Total DNA | Skin tissue and eye aqueous humor | Diagnosis of a patient with eye tumor | Confirmed by PCR in the aqueous humor | [105] |
| Not mentioned | BAL and blood | Diagnosis of a patient with chronic pneumonia | Confirmed by culture in sputum | [106] |
| Total DNA | FFPE tissue | Differential diagnosis of a patient with peritonitis | [107] | |
| Not mentioned | BAL | Diagnosis of a patient with chronic pneumonia | Confirmed by culture in BAL | [108] |
| Total DNA | BAL, blood, and BM | Assessment of clinical performance of NGS for talaromycosis diagnosis | Sensitivity and specificity values were 98.3 and 98.6%, respectively. The clinical final diagnosis was used as the reference standard. | [99] |
| Histoplasmosis | ||||
| Total RNA | CSF | Differential diagnosis of meningitis | Statistical framework supported by environmental and non-infected control samples | [109] |
| Total DNA | Miscellaneous | Identification of the causative agent causing an outbreak | [110] | |
| Not mentioned | Not mentioned | Diagnosis of a patient with chronic progressive lung lesions | [111] | |
| DNA (ITS region) | FFPE tissue | Diagnosis of a patient with a skin lesion | Confirmed by histopathology | [112] |
| Not mentioned | BM | Diagnosis of non-HIV febrile patient | Confirmed by direct visualization | [113] |
| Blastomycosis | ||||
| Cell-free DNA | Plasma | Diagnosis of a patient with chronic pneumonia | [114] | |
| Not mentioned | BAL and biopsy | Diagnosis of a patient with chronic pneumonia | Confirmed by histopathology of BAL | [115] |
| Multiple EM identified | ||||
| Not mentioned | Peripheral blood and BM | Differential diagnosis in immunocompromised patients | Histoplasmosis (confirmed by histopathology), talaromycosis | [116] |
| DNA (ITS region) | FFPE tissue | Retrospective evaluation of the NGS clinical utility | Confirmed by histopathology | [117] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valero, C.; Martín-Gómez, M.T.; Buitrago, M.J. Molecular Diagnosis of Endemic Mycoses. J. Fungi 2023, 9, 59. https://doi.org/10.3390/jof9010059
Valero C, Martín-Gómez MT, Buitrago MJ. Molecular Diagnosis of Endemic Mycoses. Journal of Fungi. 2023; 9(1):59. https://doi.org/10.3390/jof9010059
Chicago/Turabian StyleValero, Clara, María Teresa Martín-Gómez, and María José Buitrago. 2023. "Molecular Diagnosis of Endemic Mycoses" Journal of Fungi 9, no. 1: 59. https://doi.org/10.3390/jof9010059
APA StyleValero, C., Martín-Gómez, M. T., & Buitrago, M. J. (2023). Molecular Diagnosis of Endemic Mycoses. Journal of Fungi, 9(1), 59. https://doi.org/10.3390/jof9010059