
COVID-19-Associated Pulmonary Aspergillosis (CAPA) in Northern Greece during 2020–2022: A Comparative Study According to the Main Consensus Criteria and Definitions

 , and
, and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
- Adult patient (over 18 years of age) with SARS-CoV-2 infection confirmed molecularly by polymerase chain reaction (PCR).
- Admission to the ICU exclusively for the treatment of COVID-19 due to the concomitant respiratory failure. Patients with admission to the ICU due to other conditions, apart from the SARS-CoV-2 infection, were excluded.
- Direct microscopy of the respiratory samples for the detection of fungal elements (hyphae, conidia, etc).
- Mycology cultures by inoculation of the relevant respiratory samples on Sabouraud dextrose agar, malt extract agar and Czapek’s dox agar plates. All cultures were incubated at two temperatures (30 °C and 35 °C) for ten to twelve days in order to confirm the negative result.
- Mycology cultures of peripheral and central venous catheter blood for investigating sepsis, with 5–10 mL of blood incubated up to 10–12 days and sub-cultured twice during this period.
- Detection of galactomannan (GM) in respiratory samples and/or serum by the use of Platelia TM Aspergillus antigen assay (Bio-Rad, Marnes-la-Coquette, France) according to the manufacturer’s instructions. The cut-off for positivity was set at ≥0.5 for serum and ≥1.0 for bronchoalveolar lavage (BAL) or non-directed bronchoscopic lavage (NBL) specimens such as bronchial or tracheal secretions.
- Implementation of qualitative in-house PCR for Aspergillus genus. Samples’ DNA was extracted according to the NucleoSpin® Blood QuickPure method (Macherey-Nagel, Düren, Germany).
- Detection of (1-3)-β-D-glucan (β-DG) in serum by the use of Fungitell® assay (Associates of Cape Cod, E. Falmouth, MA, USA) or Dynamiker Fungus (1-3)-β-D-glucan assay (Dynamiker Biotechnology Co, Tianjin, China) following the manufacturers’ instructions, with a positivity threshold set at 80 pg/mL or 95 pg/mL, respectively.
- Full identification (phenotypic and/or molecular) of the cultured fungi, either those grown on the inoculated samples in the mycology lab or those that were referred from the units of patients’ hospitalisation.
- Antifungal susceptibility testing mainly by the use of appropriate strips of gradient antifungal concentration, Etest (bioMérieux SA, Marcy-l’Etoile, France) and MIC test strip (Liofilchem srl, Roseto degli Abruzzi, Italy).
3. Results
3.1. Classification of Cases
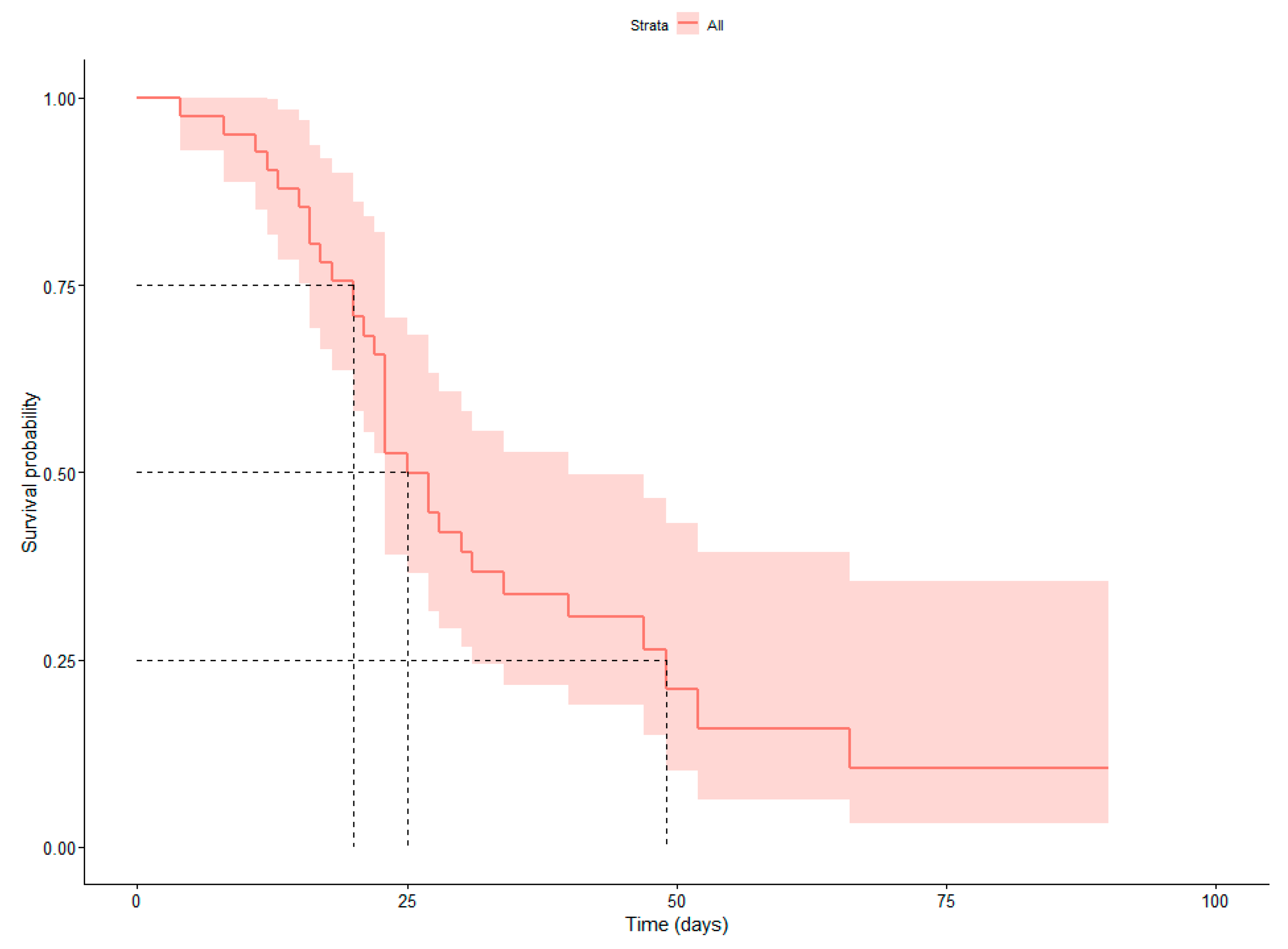
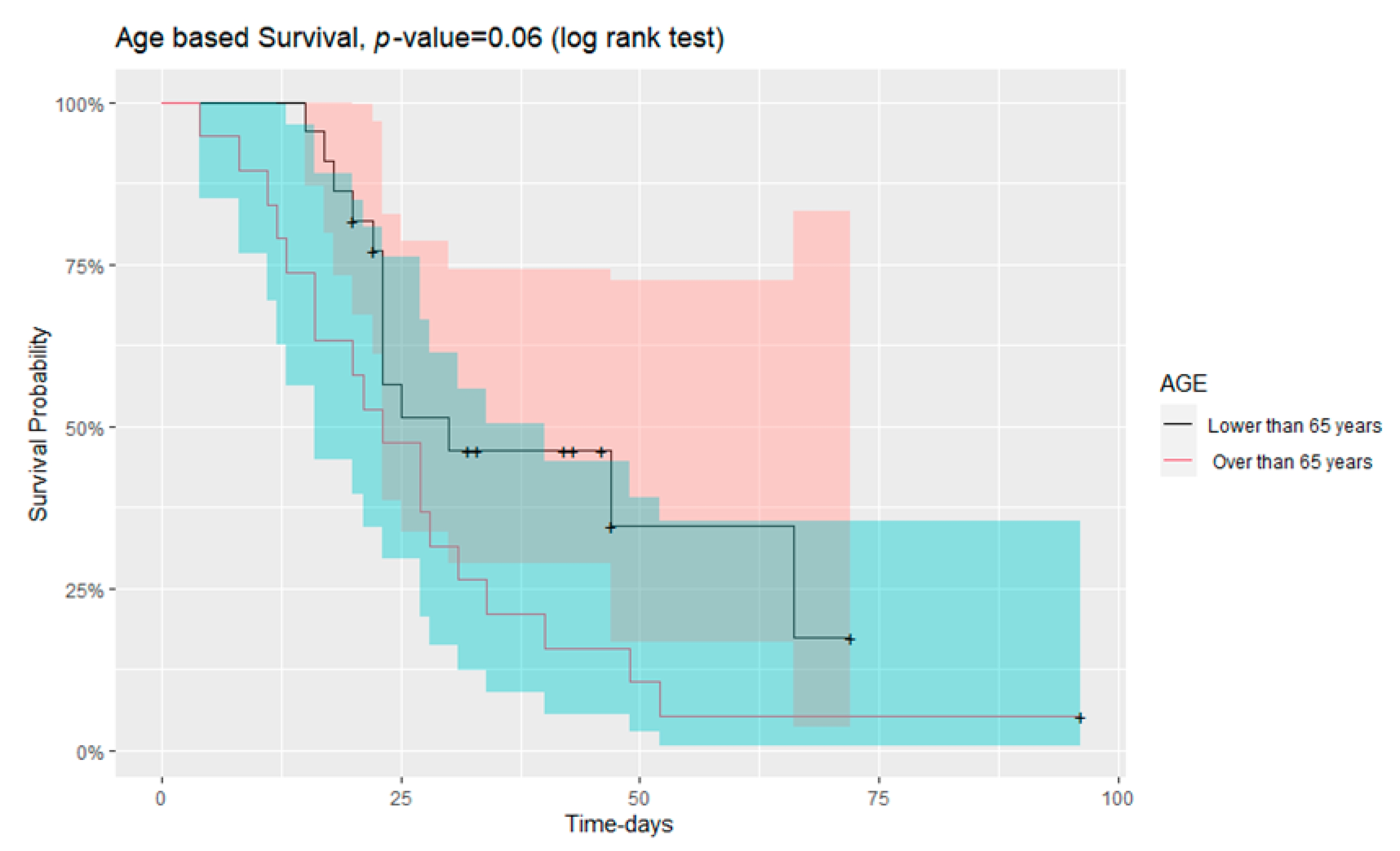
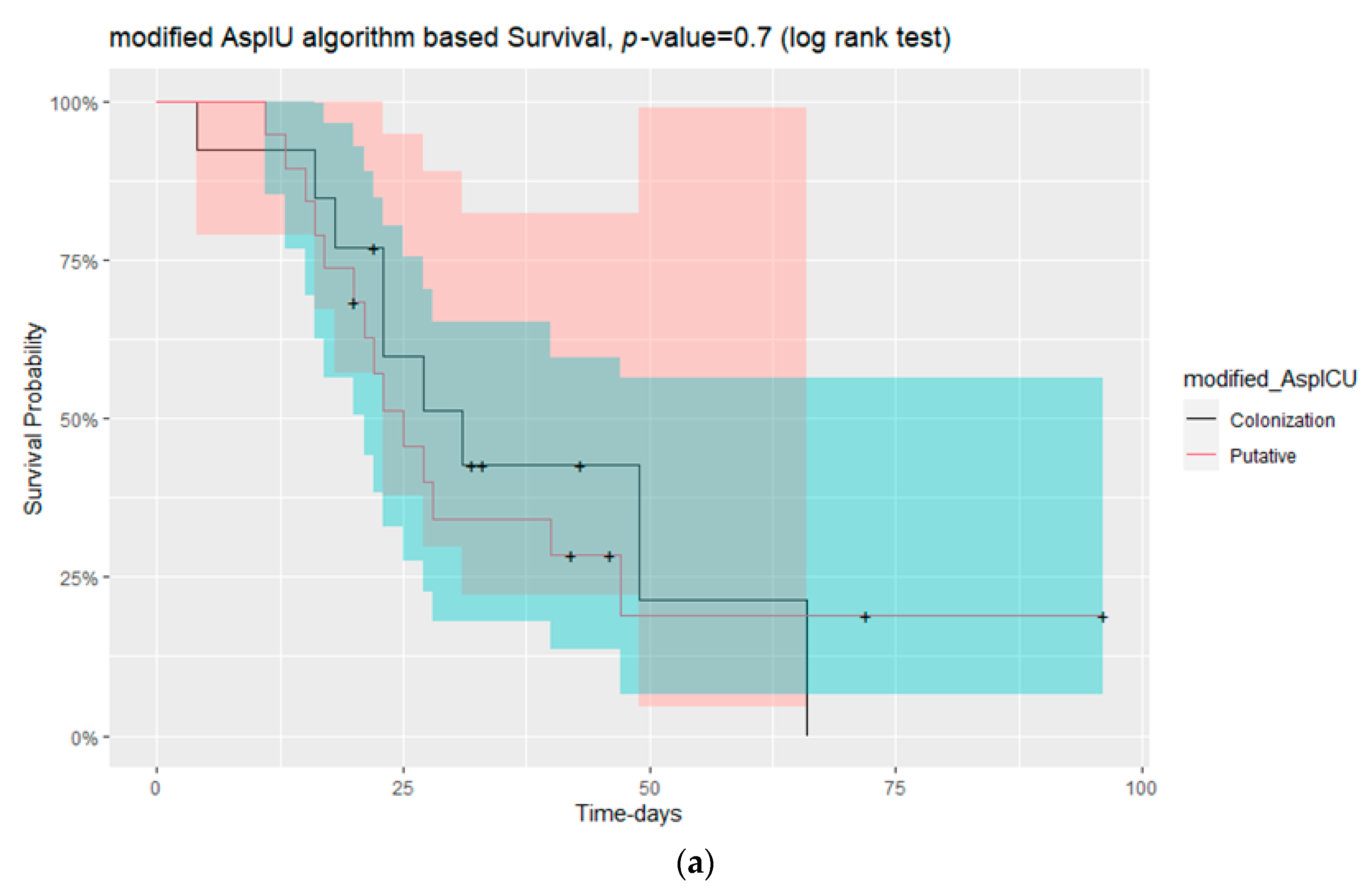
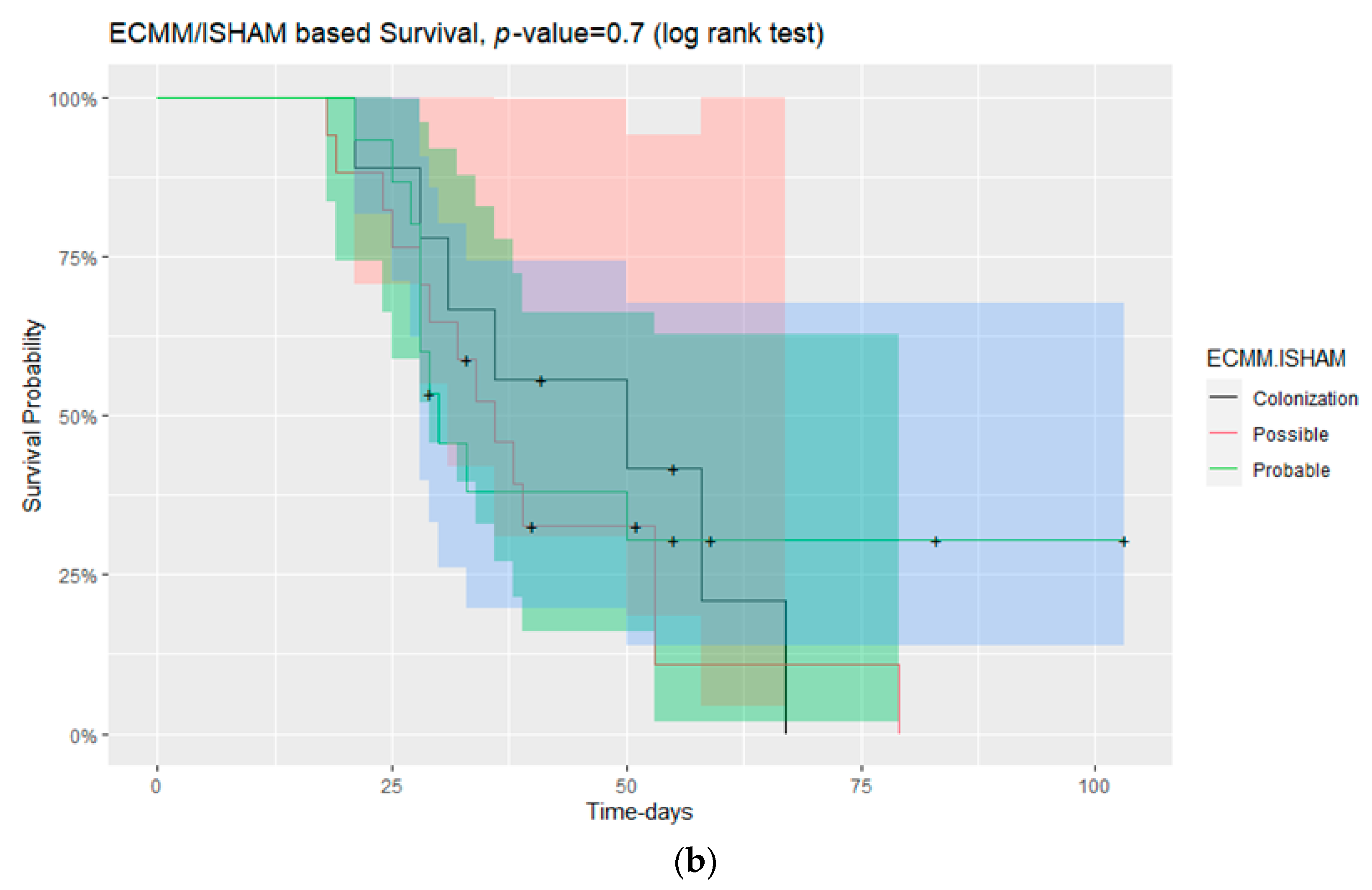
3.2. Survival in Those with and without CAPA
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arastehfar, A.; Carvalho, A.; Van De Veerdonk, F.L.; Jenks, J.D.; Koehler, P.; Krause, R.; Cornely, O.A.; Perlin, D.S.; Lass-Flörl, C.; Hoenigl, M. COVID-19 Associated Pulmonary Aspergillosis (CAPA)—From Immunology to Treatment. J. Fungi 2020, 6, 91. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Rijnders, B.J.A.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.J.; Cornely, O.A.; Chiller, T.; et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: An expert opinion. Intensive Care Med. 2020, 46, 1524–1535. [Google Scholar] [CrossRef]
- Salmanton-García, J.; Sprute, R.; Stemler, J.; Bartoletti, M.; Dupont, D.; Valerio, M.; Garcia-Vidal, C.; Falces-Romero, I.; Machado, M.; de la Villa, S.; et al. COVID-19–Associated Pulmonary Aspergillosis, March–August 2020. Emerg. Infect. Dis. 2021, 27, 1077–1086. [Google Scholar] [CrossRef]
- Shyu, D.; Patil, S.; Wilhite, R.; Karle, E.; Beck, P.; Athey, M.; Nelson, T.; Holliday, Z. Invasive Pulmonary Aspergillosis Due to Aspergillus Niger and COVID-19 Pneumonia. Am. J. Respir. Crit. Care Med. 2021, 203, A4011. [Google Scholar] [CrossRef]
- Verweij, P.E.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Buil, J.B.; Calandra, T.; Chiller, T.; Clancy, C.J.; Cornely, O.A.; et al. Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensiv. Care Med. 2021, 47, 819–834. [Google Scholar] [CrossRef]
- Jenks, J.D.; Mehta, S.R.; Taplitz, R.; Aslam, S.; Reed, S.L.; Hoenigl, M. Point-of-care diagnosis of invasive aspergillosis in non-neutropenic patients: Aspergillus Galactomannan Lateral Flow Assay versus Aspergillus-specific Lateral Flow Device test in bronchoalveolar lavage. Mycoses 2019, 62, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef] [PubMed]
- Lass-Flörl, C.; Samardzic, E.; Knoll, M. Serology anno 2021—Fungal infections: From invasive to chronic. Clin. Microbiol. Infect. 2021, 27, 1230–1241. [Google Scholar] [CrossRef]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef]
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.-M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A Clinical Algorithm to Diagnose Invasive Pulmonary Aspergillosis in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Schauwvlieghe, A.F.A.D.; Rijnders, B.J.A.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van De Veerdonk, F.L.; Gommers, D.; et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: A retrospective cohort study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef]
- Available online: https://www.worldometers.info/coronavirus/country/greece/ (accessed on 17 May 2022).
- Verweij, P.E.; Gangneux, J.P.; Bassetti, M.; Brüggemann, R.J.M.; Cornely, O.A.; Koehler, P.; Lass-Flörl, C.; van de Veerdonk, F.L.; Chakrabarti, A.; Hoenigl, M. Diagnosing COVID-19-associated pulmonary aspergillosis. Lancet Microbe 2020, 1, e53–e55. [Google Scholar] [CrossRef] [PubMed]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. A National Strategy to Diagnose Coronavirus Disease 2019–Associated Invasive Fungal Disease in the Intensive Care Unit. Clin. Infect. Dis. 2021, 73, e1634–e1644. [Google Scholar] [CrossRef] [PubMed]
- Ghizlane, E.A.; Manal, M.; Abderrahim, E.K.; Abdelilah, E.; Mohammed, M.; Rajae, A.; Amine, B.M.; Houssam, B.; Naima, A.; Brahim, H. Lymphopenia in COVID-19: A single center retrospective study of 589 cases. Ann. Med. Surg. 2021, 69, 102816. [Google Scholar] [CrossRef] [PubMed]
- Tavakolpour, S.; Rakhshandehroo, T.; Wei, E.X.; Rashidian, M. Lymphopenia during the COVID-19 infection: What it shows and what can be learned. Immunol. Lett. 2020, 225, 31–32. [Google Scholar] [CrossRef]
- Yang, L.; Liu, S.; Liu, J.; Zhang, Z.; Wan, X.; Huang, B.; Chen, Y.; Zhang, Y. COVID-19: Immunopathogenesis and Immunotherapeutics. Signal Transduct. Target. Ther. 2020, 5, 128. [Google Scholar] [CrossRef]
- Aigner, M.; Wanner, M.; Kreidl, P.; Lass-Flörl, C.; Lackner, M. Candida in the Respiratory Tract Potentially Triggers Galactomannan Positivity in Nonhematological Patients. Antimicrob. Agents Chemother. 2019, 63, e00138-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. 1), e1–e38. [Google Scholar] [CrossRef] [Green Version]
- Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Izcovich, A.; Kum, E.; Pardo-Hernandez, H.; Qasim, A.; Martinez, J.P.D.; Rochwerg, B.; et al. Drug treatments for COVID-19: Living systematic review and network meta-analysis. BMJ 2020, 370, m2980. [Google Scholar] [CrossRef] [PubMed]
- Prattes, J.; Valentin, T.; Hoenigl, M.; Talakic, E.; Reisinger, A.C.; Eller, P. Invasive pulmonary aspergillosis complicating COVID-19 in the ICU—A case report. Med Mycol. Case Rep. 2020, 31, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Lescure, F.-X.; Bouadma, L.; Nguyen, D.; Parisey, M.; Wicky, P.-H.; Behillil, S.; Gaymard, A.; Bouscambert-Duchamp, M.; Donati, F.; Le Hingrat, Q.; et al. Clinical and virological data of the first cases of COVID-19 in Europe: A case series. Lancet Infect. Dis. 2020, 20, 697–706, Correction in Lancet Infect. Dis. 2020, 20, e148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gangneux, J.-P.; Reizine, F.; Guegan, H.; Pinceaux, K.; Le Balch, P.; Prat, E.; Pelletier, R.; Belaz, S.; Le Souhaitier, M.; Le Tulzo, Y.; et al. Is the COVID-19 Pandemic a Good Time to Include Aspergillus Molecular Detection to Categorize Aspergillosis in ICU Patients? A Monocentric Experience. J. Fungi 2020, 6, 105. [Google Scholar] [CrossRef]
- Rutsaert, L.; Steinfort, N.; Van Hunsel, T.; Bomans, P.; Naesens, R.; Mertes, H.; Dits, H.; Van Regenmortel, N. COVID-19-associated invasive pulmonary aspergillosis. Ann. Intensive Care 2020, 10, 71. [Google Scholar] [CrossRef]
- Marr, K.A.; Platt, A.; Tornheim, J.A.; Zhang, S.X.; Datta, K.; Cardozo, C.; Garcia-Vidal, C. Aspergillosis Complicating Severe Coronavirus Disease. Emerg. Infect. Dis. 2021, 27, 18–25. [Google Scholar] [CrossRef]
- Flikweert, A.W.; Grootenboers, M.J.; Yick, D.C.; du Mée, A.W.; van der Meer, N.J.; Rettig, T.C.; Kant, M.K. Late histopathologic characteristics of critically ill COVID-19 patients: Different phenotypes without evidence of invasive aspergillosis, a case series. J. Crit. Care 2020, 59, 149–155. [Google Scholar] [CrossRef]
- Mitaka, H.; Perlman, D.C.; Javaid, W.; Salomon, N. Putative invasive pulmonary aspergillosis in critically ill patients with COVID-19: An observational study from New York City. Mycoses 2020, 63, 1368–1372. [Google Scholar] [CrossRef] [PubMed]
- Falces-Romero, I.; Ruiz-Bastián, M.; Díaz-Pollán, B.; Maseda, E.; García-Rodríguez, J.; SARS-CoV-2 Working Group. Isolation of Aspergillus spp. in respiratory samples of patients with COVID-19 in a Spanish Tertiary Care Hospital. Mycoses 2020, 63, 1144–1148. [Google Scholar] [CrossRef]
- Meersseman, W.; Lagrou, K.; Maertens, J.; Van Wijngaerden, E. Invasive Aspergillosis in the Intensive Care Unit. Clin. Infect. Dis. 2007, 45, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, M.; Simon, M.; Katchanov, J.; Wijaya, C.; Rohde, H.; Christner, M.; Laqmani, A.; Wichmann, D.; Fuhrmann, V.; Kluge, S. Does galactomannan testing increase diagnostic accuracy for IPA in the ICU? A prospective observational study. Crit. Care 2016, 20, 139. [Google Scholar] [CrossRef]
- Meersseman, W.; Lagrou, K.; Maertens, J.; Wilmer, A.; Hermans, G.; Vanderschueren, S.; Spriet, I.; Verbeken, E.; van Wijngaerden, E. Galactomannan in bronchoalveolar lavage fluid: A tool for diagnosing aspergillosis in intensive care unit patients. Am. J. Respir. Crit. Care Med. 2008, 177, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alanio, A.; Dellière, S.; Fodil, S.; Bretagne, S.; Mégarbane, B. Prevalence of putative invasive pulmonary aspergillosis in critically ill patients with COVID-19. Lancet Respir. Med. 2020, 8, e48–e49. [Google Scholar] [CrossRef] [PubMed]
- Prattes, J.; Wauters, J.; Giacobbe, D.R.; Salmanton-García, J.; Maertens, J.; Bourgeois, M.; Reynders, M.; Rutsaert, L.; Van Regenmortel, N.; Lormans, P.; et al. Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients—A multinational observational study by the European Confederation of Medical Mycology. Clin. Microbiol. Infect. 2022, 28, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Gregoire, E.; Pirotte, B.F.; Moerman, F.; Altdorfer, A.; Gaspard, L.; Firre, E.; Moonen, M.; Fraipont, V.; Ernst, M.; Darcis, G. Incidence and Risk Factors of COVID-19-Associated Pulmonary Aspergillosis in Intensive Care Unit—A Monocentric Retrospective Observational Study. Pathogens 2021, 10, 1370. [Google Scholar] [CrossRef] [PubMed]
- Marta, G.-C.; Lorena, F.-E.; Laura, M.-V.; Angela, L.-M.; Blanca, L.-G.; Rodrigo, A.-A.; Marta, S.-G.; Santiago, M.-G.; Liliana, P.-M.; Luisa, S.-N.M.; et al. COVID-19-Associated Pulmonary Aspergillosis in a Tertiary Hospital. J. Fungi 2022, 8, 97. [Google Scholar] [CrossRef]
- Hoenigl, M. Invasive Fungal Disease Complicating Coronavirus Disease 2019: When It Rains, It Spores. Clin. Infect. Dis. 2021, 73, e1645–e1648. [Google Scholar] [CrossRef]
- Jabeen, K.; Farooqi, J.; Irfan, M.; Ali, S.A.; Denning, D.W. Diagnostic dilemma in COVID-19-associated pulmonary aspergillosis. Lancet Infect. Dis. 2021, 21, 767. [Google Scholar] [CrossRef]
- Koehler, P.; White, P.L.; E Verweij, P.; Cornely, O.A. Diagnostic dilemma in COVID-19-associated pulmonary aspergillosis—Authors’ reply. Lancet Infect. Dis. 2021, 21, 767–769. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Annual Increase (%) 2020–2021 | |
|---|---|
| Respiratory samples | 52.5 |
| Positive cultures for Aspergillus spp | 131.3 |
| Ag Aspergillus | 32.5 |
| PCR for Aspergillus genus | 43.4 |
| Median (1st Qu–3rd Qu) | ||||
|---|---|---|---|---|
| Demographics | Total | CAPA Patients * | Aspergillus Colonisation * | p-Value |
| Males/Females | 26/17 | 20/13 | 6/4 | |
| Vaccinated against SARS-CoV-2 | 23.3% (10/43) | 15.2% (5/33) | 50% (5/10) | |
| Age (years) | 64 (53.5–70.5) | 64 (55–70) | 64 (51.25–70.50) | 0.86 |
| Antifungal treatment- duration (days) | 17 (10–30.5) | 20 (12–35) | 10 (7–18.75) | 0.029 |
| Stay in the ICU (days) | 23 (19–37) | 27 (20–42) | 22.5 (14.75–28.25) | 0.24 |
| Days from diagnosis of COVID-19 infection by SARS-CoV-2 until admission at the ICU (days) | 11 (7–15) | 10 (6–14) | 16.5 (13.5–21) | 0.0007 |
| Days of culture result after ICU admission (days) | 21 (17–26.5) | 21 (18–26) | 20.5 (14.25–26.25) | 0.45 |
| Respiratory sampling time after ICU admission (days) | 11 (6–16.5) | 11 (8–15) | 10.5 (4.25–17.25) | 0.52 |
| BMI | 29 (26.4–31.55) | 29.15 (26.82–31.77) | 28 (25–31) | 0.45 |
| SOFA score (admission in ICU) | 7 (7–8.75) | 7 (7–8) | 7 (6–9) | 0.84 |
| SOFA score (sampling) | 8 (7–9) | 8 (7–9) | 8 (7–8) | 0.88 |
| corticosteroid use- duration (days) | 10 (10–17.5) | 10 (10–14) | 10.5 (10–23.75) | 0.58 |
| WBC(a) (cells/μL) | 13,400 (9425–18,510) | 13,900 (10,300–17,600) | 8435 (6258–20,675) | 0.66 |
| NEUT(a) (cells/μL) | 11,422 (7965–16,625) | 12,232 (8806–16,450) | 6862 (5485–15,609) | 0.20 |
| LYMP(a) (cells/μL) | 630 (471–930) | 592.6 (491–880) | 803.2 (446.9–1250.3) | 0.28 |
| PLT(a) (platelets/μL) | 291,000 (172,500–343,500) | 292,000 (212,000–322,000) | 182,500 (126,500–355,250) | 0.49 |
| Hb(a) (mg/dL) | 12.5 (10.7–13.2) | 12.8 (11.9–13.2) | 11.25 (8.95–13.10) | 0.21 |
| HCT(a) (%) | 37.2 (32–40.1) | 37.6 (34.8–40) | 33.4 (27.75–40.02) | 0.20 |
| CRP(a) (mg/dL) | 10.3 (6.3–16.45) | 10.35 (5.73–16.3) | 9.65 (7.28–15.98) | 0.93 |
| PCT(a) (μg/L) | 0.195 (0.08–0.56) | 0.2 (0.1–0.5) | 0.2 (0.1–0.6) | 0.62 |
| Cr(a) (mg/dL) | 0.7 (0.58–1.22) | 0.7 (0.6–1.1) | 0.7 (0.6–1.275) | 0.98 |
| WBC(s) (cells/μL) | 11,530 (9135–16,555) | 11,590 (8980–17,470) | 10,420 (9708–12,848) | 0.51 |
| NEUT(s) (cells/μL) | 9300 (7406–14,742) | 9570 (7302–15,897) | 8430 (7701–10,568) | 0.19 |
| LYMP(s) (cells/μL) | 810 (520–1172) | 810 (504–1070) | 888.7 (570.6–1881.5) | 0.55 |
| PLT(s) (platelets/μL) | 216,000 (132,750–279,750) | 229,500 (145,500–277,250) | 182,000 (101,500–378,250) | 0.62 |
| Hb(s) (mg/dL) | 10 (8.65–11.25) | 10.1 (8.7–11.4) | 9.15 (7.98–10.7) | 0.32 |
| HCT(s) (%) | 30 (26.95–34.25) | 30.4 (27.1–34.4) | 28.65 (26.93–31.8) | 0.38 |
| CRP(s) (mg/dL) | 12.27 (4.93–22.05) | 13.4 (4.98–22.45) | 7.95 (4.78–15.93) | 0.50 |
| PCT(s) (μg/L) | 0.33 (0.15–0.94) | 0.3 (0.2–1.1) | 0.4 (0.1–0.5) | 0.54 |
| Cr(s) (mg/dL) | 0.75 (0.57–1.16) | 0.8 (0.6–1.1) | 0.8 (0.625–1.25) | 0.42 |
| VOR (treatment duration days) | 8.95 (0–14) | 6 (0–14.5) | 2.5 (0–6.25) | 0.51 |
| GM BAL (Index) | 2.19 (1.16–3.63) | 1.945 (1.157–3.357) | 0.14 (0.125–0.175) | 0.001 |
| GM NBL (Index) | 3.9 (3.1–4.33) | 4.075 (3.6–4.5) | 1.3 (1.205–2.515) | 0.051 |
| GM serum (Index) | 0.84 (0.6–1.06) | 0.2 (0.09–0.4225) | 0,09 (0.06–0.335) | 0.24 |
| Type of samples, n (%) | ||||
| BAL, n (%) | 23 (53.5%) | 16 (48.49%) | 7 (70%) | |
| NBL, n (%) | 15 (34.9%) | 12 (36.36%) | 3 (30%) | |
| Culture plates (NBL), n (%) | 5 (11.6%) | 5 (15.15%) | 0 | |
| Comorbidities | Total Patients n (%) | * CAPA Patients n (%) | * Aspergillus Colonisation Patients n (%) |
|---|---|---|---|
| Cardiovascular system | |||
| Arterial hypertension | 20/43 (46.5) | 15/43 (34.9) | 5/43 (11.6) |
| Atrial fibrillation | 3/43 (7.0) | 3/43 (7.0) | |
| Coronary angioplasty | 1/43 (2.3) | 1/43 (2.3) | |
| Coronary disease | 5/43 (11.6) | 4/43 (9.3) | 1/43 (2.3) |
| Heart attack history | 5/43 (11.6) | 4/43 (9.3) | 1/43 (2.3) |
| Heart failure | 1/43 (2.3) | 1/43 (2.3) | |
| Giant cell arthritis | 1/43 (2.3) | 1/43 (2.3) | |
| Venous thrombosis | 3/43 (7.0) | 3/43 (7.0) | |
| Respiratory system | |||
| Bronchial asthma | 3/43 (7.0) | 2/43 (4.7) | 1/43 (2.3) |
| Emphysema | 1/43 (2.3) | 1/43 (2.3) | |
| Obstructive sleep apnoea | 2/43 (4.7) | 1/43 (2.3) | 1/43 (2.3) |
| Pulmonary embolism | 1/43 (2.3) | 1/43 (2.3) | |
| Chronic obstructive pulmonary disease | 2/43 (4.7) | 1/43 (2.3) | 1/43 (2.3) |
| Haematological/Ontological malignancies | |||
| Chronic lymphocytic leukaemia | 3/43 (7.0) | 1/43 (2.3) | 2/43 (4.7) |
| Multiple myeloma | 2/43 (4.7) | 1/43 (2.3) | 1/43 (2.3) |
| Malignancy | 1/43 (2.3) | 1/43 (2.3) | |
| Red blood cells dysplasia | 1/43 (2.3) | 1/43 (2.3) | |
| Spinal cord ependymoma | 1/43 (2.3) | 1/43 (2.3) | |
| Kidney diseases | |||
| Chronic renal failure | 1/43 (2.3) | 1/43 (2.3) | |
| Disorders of endocrine glands | |||
| Diabetes mellitus | 13/43 (30.2) | 8/43 (18.6) | 5/43 (11.6) |
| Hypothyroidism | 4/43 (9.3) | 2/43 (4.7) | 2/43 (4.7) |
| Dyslipidaemia | 13/43 (30.2) | 12/43 (27.9) | 1/43 (2.3) |
| Other diseases | |||
| HBV carrier | 4/43 (9.3) | 3/43 (7.0) | 1/43 (2.3) |
| Hyperuricemia | 1/43 (2.3) | 1/43 (2.3) | |
| Obesity | 14/43 (32.6) | 11/43 (25.6) | 3/43 (7.0) |
| Osteoporosis | 1/43 (2.3) | 1/43 (2.3) | |
| Polymyalgia rheumatica | 1/43 (2.3) | 1/43 (2.3) | |
| Pregnancy | 1/43 (2.3) | 1/43 (2.3) | |
| Rheumatoid arthritis | 1/43 (2.3) | 1/43 (2.3) | |
| Beta thalassemia trait | 1/43 (2.3) | 1/43 (2.3) | |
| Ankylosing spondylitis | 1/43 (2.3) | 1/43 (2.3) | |
| History of smoking or smoking | 4/43 (9.3) | 4/43 (9.3) |
| CAPA Patients * | Aspergillus Respiratory Tract Colonisation Patients * | Total % (n) | |
|---|---|---|---|
| Positive microscopic examination in BAL | 4/16 | 0/7 | 17.4 (4/23) |
| Positive microscopic examination in NBL | 8/12 | 0/3 | 53.3 (8/15) |
| Positive GM in BAL | 15/16 | 0/7 | 65.2 (15/23) |
| Positive GM in NBL | 12/12 | 3/3 | 100 (15/15) |
| Positive GM in serum | 6/26 | 0/10 | 16.7 (6/36) |
| Positive culture for Aspergillus species in BAL | 7/16 | 0/7 | 30.4 (7/23) |
| Positive culture for Aspergillus species in NBL | 16/17 | 0/3 | 80 (16/20) |
| Positive PCR for Aspergillus genus | 4/8 | 7/7 | 73.3 (11/15) |
| Sample | Species | Microscopy | GM | PCR | VOR MIC | IT MIC | CAS MIC | AP-B MIC | POS MIC | ISA MIC | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BAL | NBL | Serum | |||||||||||
| 1 | BAL | A. fumigatus | Pos | 4.16 | - | 0.36 | - | 0.25 | 0.75 | 0.125 | 0.047 | 0.19 | 0.19 |
| 2 | BAL | A. fumigatus A. niger | Neg | 4.6 | - | 0.54 | - | 0.094 | 0.38 | 0.19 | 1.0 | 0.094 | 0.19 |
| 0.064 | 0.25 | 0.19 | 0.25 | 0.094 | 0.064 | ||||||||
| 3 | BS | A. terreus and C. glabrata | Pos | - | 3.9 | 0.22 | - | 0.25 | 0.19 | 0.125 | 1.0 | 0.094 | 0.125 |
| 4 | BAL | A. fumigatus A. terreus | Neg | 2.52 | - | 0.05 | Pos | 0.094 | 1.0 | <0.5 | 0.094 | ||
| 0.023 | 0.016 | 0.094 | 8 | 0.094 | 0.012 | ||||||||
| 5 | BS | A. fumigatus A. flavus | Pos | - | 4.15 | - | - | 0.47 | 0.75 | 0.19 | 1.0 | 0.125 | 0.094 |
| 0.19 | 0.5 | 0.125 | 8 | 0.125 | 0.125 | ||||||||
| 6 | BAL | A. fumigatus | Neg | 1.16 | - | 0.20 | - | 0.125 | 0.5 | 0.19 | 1.5 | 0.19 | 0.125 |
| 7 | BAL | A. terreus, A. flavus and C. albicans | Neg | 2.92 | - | 0.17 | - | 0.19 | 0.25 | 0.19 | 4 | 0.125 | 0.125 |
| 8 | BS | A. niger | Pos | - | 2.89 | 0.43 | - | 0.016 | 0.094 | 0.094 | 0.032 | 0.094 | 0.094 |
| 9 | BS | A. terreus | Pos | - | 5 | 0.4 | - | 0.125 | 0.19 | 0.094 | 1.5 | 0.094 | 0.094 |
| 10 | BS | A. niger | Neg | - | 4.5 | 0.08 | - | 0.032 | 0.094 | 0.094 | 0.125 | 0.094 | 0.094 |
| 11 | CP (BS) | A. flavus | - | - | - | - | - | 0.125 | 0.5 | 0.125 | 2.0 | 0.125 | 0.19 |
| 12 | BS | A. flavus | Pos | - | 3.7 | 0.2 | - | 0.19 | 0.38 | 0.047 | 4 | 0.094 | 0.094 |
| 13 | CP (BS) | A. niger | - | - | - | - | - | Antifungal susceptibility test was not performed due to the patient’s death. | |||||
| 14 | BS | A. flavus | Neg | - | 4.5 | 4.21 | - | 0.094 | 0.38 | 0.125 | 3 | 0.19 | 0.094 |
| 15 | CP (BS) | A. terreus | - | - | - | - | - | 0.125 | 0.38 | 0.094 | 6 | 0.094 | 0.19 |
| 16 | BS | A. niger and C. albicans | Neg | - | 4.05 | 0.22 | - | 0.25 | 2 | 0.25 | 1 | 0.38 | 0.75 |
| 17 | BS | A. niger and C. albicans | Pos | - | 4.7 | 0.03 | - | 0.19 | 1.5 | 0.19 | 0.125 | 0.125 | 0.25 |
| 18 | BS | A. niger | Pos | - | 3.3 | 0.67 | - | 0.25 | 2 | 0.19 | 1 | 0.5 | 0.5 |
| 19 | CP (BS) | A. terreus | - | - | - | - | - | 0.064 | 0.125 | 0.094 | 0.25 | 0.064 | 0.125 |
| 20 | CP (BS) | A. fumigatus | - | - | - | - | - | 0.047 | 1 | 0.032 | 0.016 | 0.064 | 0.064 |
| 21 | BAL | A. niger | Pos | 3.09 | - | 0.58 | Pos | 0.047 | 1 | 0.19 | 0.25 | 0.25 | 0.125 |
| Fungi Isolated in Respiratory Sample * | Total % (n) |
|---|---|
| Aspergillus niger | 11.6 (5/43) |
| Aspergillus terreus | 7.0 (3/43) |
| Aspergillus flavus | 7.0 (3/43) |
| Aspergillus fumigatus | 7.0 (3/43) |
| Aspergillus fumigatus and flavus and terreus | 2.3 (1/43) |
| Aspergillus fumigatus and niger | 2.3 (1/43) |
| Aspergillus terreus and Candida glabrata | 2.3 (1/43) |
| Aspergillus fumigatus and terreus | 2.3 (1/43) |
| Aspergillus fumigatus and flavus | 2.3 (1/43) |
| Aspergillus terreus and flavus and Candida albicans | 2.3 (1/43) |
| Aspergillus niger and Candida albicans | 4.7 (2/43) |
| Aspergillus terreus and Candida albicans | 2.3 (1/43) |
| Candida parapsilosis | 2.3 (1/43) |
| Candida albicans | 7.0 (3/43) |
| Candida glabrata | 2.3 (1/43) |
| Negative | 34.9 (15/43) |
| EORTC/MSGERC | ECMM/ISHAM | Modified AspICU | Novel CAPA Definitions | |
|---|---|---|---|---|
| Putative | - | - | 20 | 43 |
| Probable | 3 | 16 | - | - |
| Possible | 4 | 17 | - | - |
| Colonisation | - | 10 | 13 | - |
| NA (not applicable) | 36 | - | 10 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siasios, P.; Arvaniti, K.; Zachrou, E.; Poulopoulou, A.; Pisanidou, P.; Vasileiadou, G.; Kaimakamis, E.; Georgopoulou, A.; Renta, F.; Lathyris, D.; et al. COVID-19-Associated Pulmonary Aspergillosis (CAPA) in Northern Greece during 2020–2022: A Comparative Study According to the Main Consensus Criteria and Definitions. J. Fungi 2023, 9, 81. https://doi.org/10.3390/jof9010081
Siasios P, Arvaniti K, Zachrou E, Poulopoulou A, Pisanidou P, Vasileiadou G, Kaimakamis E, Georgopoulou A, Renta F, Lathyris D, et al. COVID-19-Associated Pulmonary Aspergillosis (CAPA) in Northern Greece during 2020–2022: A Comparative Study According to the Main Consensus Criteria and Definitions. Journal of Fungi. 2023; 9(1):81. https://doi.org/10.3390/jof9010081
Chicago/Turabian StyleSiasios, Panagiotis, Kostoula Arvaniti, Evangelia Zachrou, Aikaterini Poulopoulou, Pinelopi Pisanidou, Georgia Vasileiadou, Evangelos Kaimakamis, Athina Georgopoulou, Foteini Renta, Dimitrios Lathyris, and et al. 2023. "COVID-19-Associated Pulmonary Aspergillosis (CAPA) in Northern Greece during 2020–2022: A Comparative Study According to the Main Consensus Criteria and Definitions" Journal of Fungi 9, no. 1: 81. https://doi.org/10.3390/jof9010081
APA StyleSiasios, P., Arvaniti, K., Zachrou, E., Poulopoulou, A., Pisanidou, P., Vasileiadou, G., Kaimakamis, E., Georgopoulou, A., Renta, F., Lathyris, D., Veroniki, F., Geka, E., Soultati, I., Argiriadou, E., Apostolidou, E., Amoiridou, P., Ioannou, K., Kouras, L., Mimitou, I., ... Vyzantiadis, T. -A. (2023). COVID-19-Associated Pulmonary Aspergillosis (CAPA) in Northern Greece during 2020–2022: A Comparative Study According to the Main Consensus Criteria and Definitions. Journal of Fungi, 9(1), 81. https://doi.org/10.3390/jof9010081