
Navigating the New Reality: A Review of the Epidemiological, Clinical, and Microbiological Characteristics of Candida auris, with a Focus on Children

Abstract
:1. Introduction
2. The Epidemiology of C. auris
2.1. Global Increase in Infections Caused by Non-Albicans Candida Species
2.2. Emergence of Various Clones of C. auris
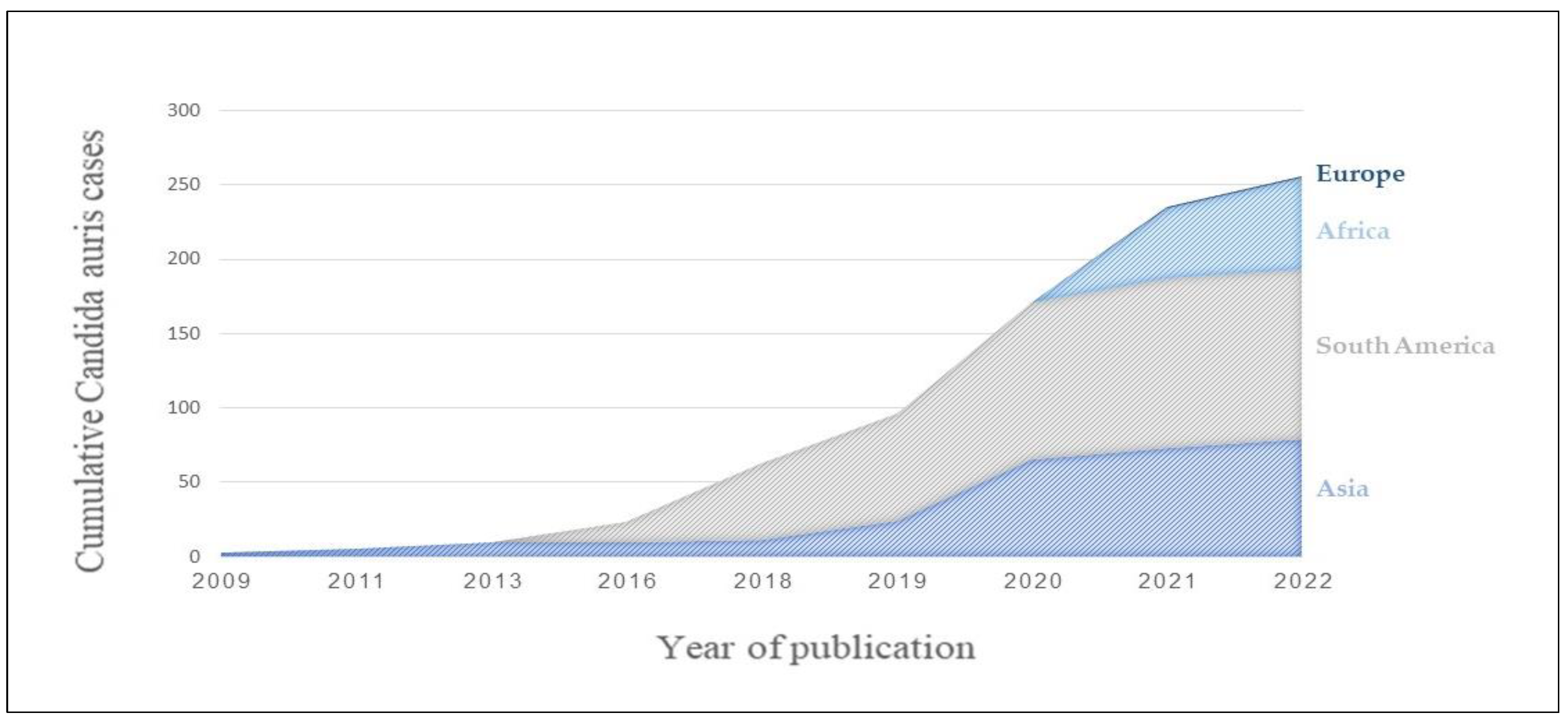
2.3. Timeline of C. auris Incidences
3. C. auris Microbiologic Identification
3.1. Phenotypic Characteristics
3.2. Diagnostic Biochemical Assays
3.3. Recommended Diagnostic Methods for C. auris
4. Clinical Spectrum of C. auris Infection
4.1. General Clinical Characteristics of C. auris Infection, with a Focus on Children
4.2. Clinical Characteristics of C. auris Infection Compared to Other Candida Species
5. C. auris Antifungal Resistance and Therapeutic Options
5.1. C. auris Susceptibility Profile
5.2. Recommendations for Treatment of C. auris
5.3. Recommendations for Prophylaxis
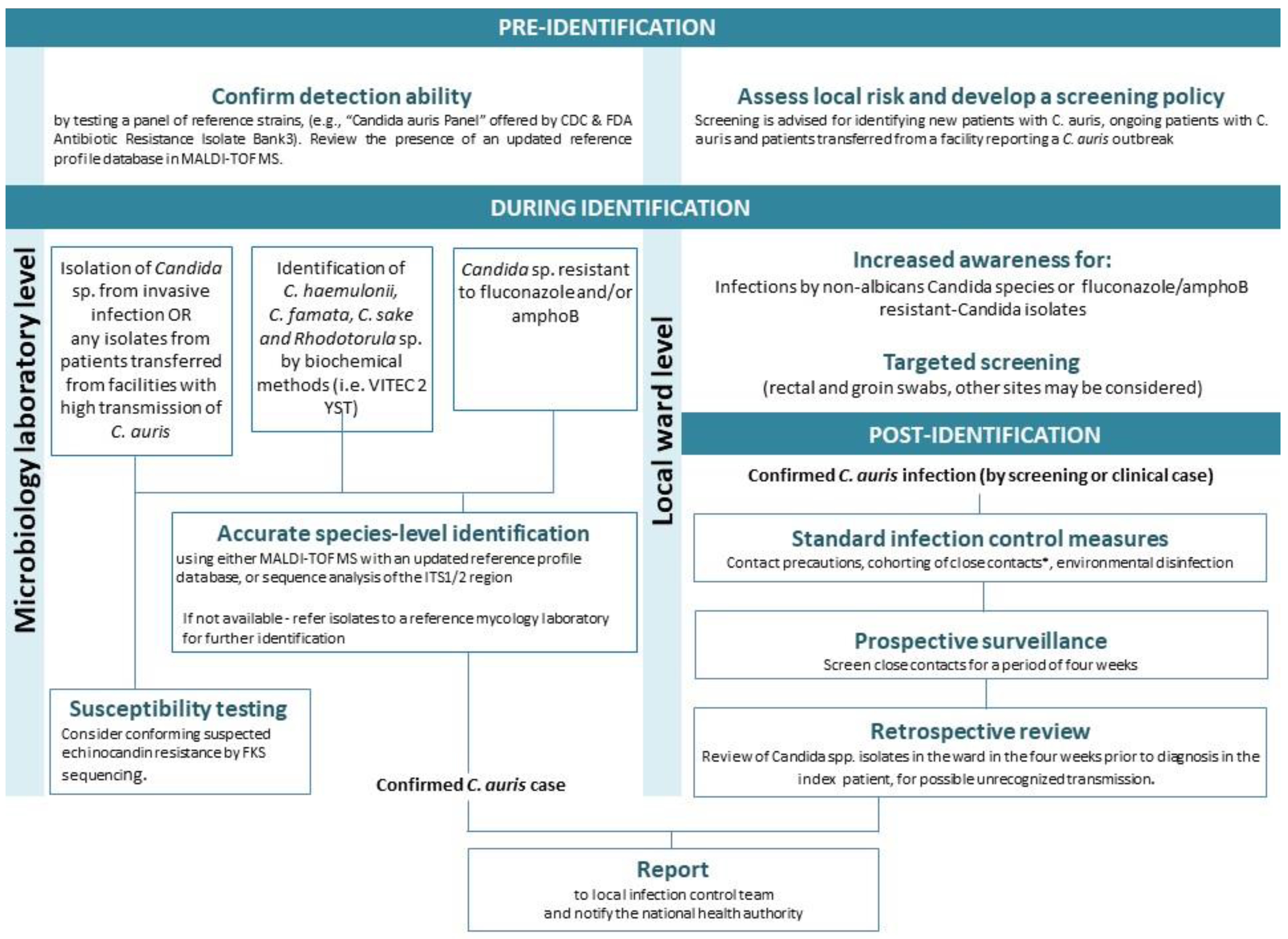
6. Infection Control Measures against C. auris
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centre for Disease Control. Antibiotic Resistance Threats in the United States (2019 AR Threats Report); U.S. Department of Health and Human Services, CDC: Washington, DC, USA, 2019. [Google Scholar]
- Ben-Ami, R.; Berman, J.; Novikov, A.; Bash, E.; Shachor-Meyouhas, Y.; Zakin, S.; Maor, Y.; Tarabia, J.; Schechner, V.; Adler, A.; et al. Multidrug-Resistant Candida haemulonii and C. auris, Tel Aviv, Israel. Emerg. Infect. Dis. 2017, 23, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous Emergence of Multidrug-Resistant Candida auris on 3 Continents Confirmed by Whole-Genome Sequencing and Epidemiological Analyses. Clin. Infect. Dis. 2017, 64, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Gaitán, A.; Moret, A.M.; Tasias-Pitarch, M.; Aleixandre-López, A.I.; Martínez-Morel, H.; Calabuig, E.; Salavert-Lletí, M.; Ramírez, P.; López-Hontangas, J.L.; Hagen, F.; et al. An outbreak due to Candida auris with prolonged colonisation and candidaemia in a tertiary care European hospital. Mycoses 2018, 61, 498–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schelenz, S.; Hagen, F.; Rhodes, J.L.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackleton, J.; Trimlett, R.; Meis, J.F.; et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob. Resist. Infect. Control 2016, 5, 35. [Google Scholar] [CrossRef] [Green Version]
- Vallabhaneni, S.; Kallen, A.; Tsay, S.; Chow, N.; Welsh, R.; Kerins, J.; Kemble, S.K.; Pacilli, M.; Black, S.R.; Landon, E.; et al. Investigation of the First Seven Reported Cases of Candida auris, a Globally Emerging Invasive, Multidrug-Resistant Fungus-United States, May 2013-August 2016. Am. J. Transplant. 2017, 17, 296–299. [Google Scholar] [CrossRef]
- Cadnum, J.L.; Shaikh, A.A.; Piedrahita, C.T.; Sankar, T.; Jencson, A.L.; Larkin, E.L.; Ghannoum, M.A.; Donskey, C.J. Effectiveness of Disinfectants Against Candida auris and Other Candida Species. Infect. Control Hosp. Epidemiol. 2017, 38, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- de Cássia Orlandi Sardi, J.; Silva, D.R.; Soares Mendes-Giannini, M.J.; Rosalen, P.L. Candida auris: Epidemiology, risk factors, virulence, resistance, and therapeutic options. Microb. Pathog. 2018, 125, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Du, H.; Bing, J.; Hu, T.; Ennis, C.L.; Nobile, C.J.; Huang, G. Candida auris: Epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog. 2020, 16, e1008921. [Google Scholar] [CrossRef]
- Clinical Alert to U.S. Healthcare Facilities—June 2016|Candida auris|Fungal Diseases|CDC. Available online: https://www.cdc.gov/fungal/candida-auris/candida-auris-alert.html (accessed on 4 December 2022).
- 3 October 2016: “Candida auris” Outbreaks in Health Care Services—Epidemiological Alert—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/documents/3-october-2016-candida-auris-outbreaks-health-care-services-epidemiological-alert (accessed on 6 December 2022).
- Epidemiological Alert: Candida auris Outbreaks in Health Care Services in the Context of the COVID-19 Pandemic—6 February 2021–PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/documents/epidemiological-alert-candida-auris-outbreaks-health-care-services-context-covid-19 (accessed on 6 December 2022).
- Candida auris: Laboratory Investigation, Management and Infection Prevention and Control—GOV.UK. Available online: https://www.gov.uk/government/publications/candida-auris-laboratory-investigation-management-and-infection-prevention-and-control (accessed on 6 December 2022).
- Available online: www.ecdc.europa.eu/sites/default/files/documents/RRA-Candida-auris-European-Union-countries.pdf (accessed on 6 December 2022).
- Abastabar, M.; Haghani, I.; Ahangarkani, F.; Rezai, M.S.; Taghizadeh Armaki, M.; Roodgari, S.; Kiakojuri, K.; Al-Hatmi, A.M.S.; Meis, J.F.; Badali, H. Candida auris otomycosis in Iran and review of recent literature. Mycoses 2019, 62, 101–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarado-Socarras, J.L.; Vargas-Soler, J.A.; Franco-Paredes, C.; Villegas-Lamus, K.C.; Rojas-Torres, J.P.; Rodriguez-Morales, A.J. A Cluster of Neonatal Infections Caused by Candida auris at a Large Referral Center in Colombia. J. Pediatr. Infect. Dis. Soc. 2021, 10, 549–555. [Google Scholar] [CrossRef]
- Escandón, P.; Cáceres, D.H.; Espinosa-Bode, A.; Rivera, S.; Armstrong, P.; Vallabhaneni, S.; Berkow, E.L.; Lockhart, S.R.; Chiller, T.; Jackson, B.R.; et al. Notes from the Field: Surveillance for Candida auris–Colombia, September 2016-May 2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 459–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, H.; Singh, S.; Rudramurthy, S.M.; Jayashree, M.; Peters, N.J.; Ray, P.; Samujh, R.; Ghosh, A.; Chakrabarti, A. Fungaemia due to rare yeasts in paediatric intensive care units: A prospective study. Mycoses 2021, 64, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-N.; Shin, J.H.; Sung, H.; Lee, K.; Kim, E.-C.; Ryoo, N.; Lee, J.-S.; Jung, S.-I.; Park, K.H.; Kee, S.J.; et al. Candida haemulonii and closely related species at 5 university hospitals in Korea: Identification, antifungal susceptibility, and clinical features. Clin. Infect. Dis. 2009, 48, e57–e61. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.G.; Shin, J.H.; Uh, Y.; Kang, M.G.; Kim, S.H.; Park, K.H.; Jang, H.-C. First three reported cases of nosocomial fungemia caused by Candida auris. J. Clin. Microbiol. 2011, 49, 3139–3142. [Google Scholar] [CrossRef] [Green Version]
- Mesini, A.; Saffioti, C.; Mariani, M.; Florio, A.; Medici, C.; Moscatelli, A.; Castagnola, E. First Case of Candida auris Colonization in a Preterm, Extremely Low-Birth-Weight Newborn after Vaginal Delivery. J. Fungi 2021, 7, 649. [Google Scholar] [CrossRef]
- Mirhendi, H.; Charsizadeh, A.; Aboutalebian, S.; Mohammadpour, M.; Nikmanesh, B.; de Groot, T.; Meis, J.F.; Badali, H. South Asian (Clade I) Candida auris meningitis in a paediatric patient in Iran with a review of the literature. Mycoses 2022, 65, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Mohsin, J.; Weerakoon, S.; Ahmed, S.; Puts, Y.; Al Balushi, Z.; Meis, J.F.; Al-Hatmi, A.M.S. A Cluster of Candida auris Blood Stream Infections in a Tertiary Care Hospital in Oman from 2016 to 2019. Antibiotics 2020, 9, 638. [Google Scholar] [CrossRef]
- Moin, S.; Farooqi, J.; Rattani, S.; Nasir, N.; Zaka, S.; Jabeen, K. C. auris and non-C. auris candidemia in hospitalized adult and pediatric COVID-19 patients; single center data from Pakistan. Med. Mycol. 2021, 59, 1238–1242. [Google Scholar] [CrossRef]
- Ramya, G.M.; Balakrishnan, U.; Chandrasekaran, A.; Abiramalatha, T.; Amboiram, P.; Sekar, U.; UshaDevi, R. Candida auris, an emerging pathogen–Challenge in the survival of microprimies. Indian J. Med. Microbiol. 2021, 39, 367–369. [Google Scholar] [CrossRef]
- Rodriguez, J.Y.; Le Pape, P.; Lopez, O.; Esquea, K.; Labiosa, A.L.; Alvarez-Moreno, C. Candida auris: A Latent Threat to Critically Ill Patients With Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 73, e2836–e2837. [Google Scholar] [CrossRef]
- Armstrong, P.A.; Rivera, S.M.; Escandon, P.; Caceres, D.H.; Chow, N.; Stuckey, M.J.; Díaz, J.; Gomez, A.; Vélez, N.; Espinosa-Bode, A.; et al. Hospital-Associated Multicenter Outbreak of Emerging Fungus Candida auris, Colombia, 2016. Emerg. Infect. Dis. 2019, 25, 1339–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathi, F.A.; Paul, S.K.; Ahmed, S.; Alam, M.M.; Nasreen, S.A.; Haque, N.; Islam, A.; Nila, S.S.; Afrin, S.Z.; Aung, M.S.; et al. Prevalence and Antifungal Susceptibility of Clinically Relevant Candida Species, Identification of Candida auris and Kodamaea ohmeri in Bangladesh. Trop. Med. Infect. Dis. 2022, 7, 211. [Google Scholar] [CrossRef] [PubMed]
- Shuping, L.; Mpembe, R.; Mhlanga, M.; Naicker, S.D.; Maphanga, T.G.; Tsotetsi, E.; Wadula, J.; Velaphi, S.; Nakwa, F.; Chibabhai, V.; et al. Epidemiology of Culture-confirmed Candidemia Among Hospitalized Children in South Africa, 2012–2017. Pediatr. Infect. Dis. J. 2021, 40, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Mukhopadhyay, S. 585 Changing trends of candida sepsis and its impact on neonates admitted in nicu: A prospective study from a tertiary centre in India. In British Association of Perinatal Medicine and Neonatal Society; BMJ Publishing Group Ltd.: London, UK; Royal College of Paediatrics and Child Health: London, UK, 2022; pp. A149.2–A150. [Google Scholar]
- Berrio, I.; Caceres, D.H.; Coronell, R.W.; Salcedo, S.; Mora, L.; Marin, A.; Varón, C.; Lockhart, S.R.; Escandón, P.; Berkow, E.L.; et al. Bloodstream Infections With Candida auris Among Children in Colombia: Clinical Characteristics and Outcomes of 34 Cases. J. Pediatr. Infect. Dis. Soc. 2021, 10, 151–154. [Google Scholar] [CrossRef]
- Calvo, B.; Melo, A.S.A.; Perozo-Mena, A.; Hernandez, M.; Francisco, E.C.; Hagen, F.; Meis, J.F.; Colombo, A.L. First report of Candida auris in America: Clinical and microbiological aspects of 18 episodes of candidemia. J. Infect. 2016, 73, 369–374. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Sood, P.; Rudramurthy, S.M.; Chen, S.; Jillwin, J.; Iyer, R.; Sharma, A.; Harish, B.N.; Roy, I.; Kindo, A.J.; et al. Characteristics, outcome and risk factors for mortality of paediatric patients with ICU-acquired candidemia in India: A multicentre prospective study. Mycoses 2020, 63, 1149–1163. [Google Scholar] [CrossRef] [PubMed]
- Chandramati, J.; Sadanandan, L.; Kumar, A.; Ponthenkandath, S. Neonatal Candida auris infection: Management and prevention strategies—A single centre experience. J. Paediatr. Child Health 2020, 56, 1565–1569. [Google Scholar] [CrossRef]
- Chibabhai, V. Incidence of candidemia and prevalence of azole-resistant candidemia at a tertiary South African hospital—A retrospective laboratory analysis 2016–2020. S. Afr. J. Infect. Dis. 2022, 37, 326. [Google Scholar] [CrossRef]
- Chowdhary, A.; Sharma, C.; Duggal, S.; Agarwal, K.; Prakash, A.; Singh, P.K.; Jain, S.; Kathuria, S.; Randhawa, H.S.; Hagen, F.; et al. New clonal strain of Candida auris, Delhi, India. Emerg. Infect. Dis. 2013, 19, 1670–1673. [Google Scholar] [CrossRef] [Green Version]
- Dutta, S.; Rahman, M.H.; Hossain, K.S.; Haq, J.A. Detection of Candida auris and its antifungal susceptibility: First report from Bangladesh. IMC J. Med. Sci. 2020, 13, 18–22. [Google Scholar] [CrossRef]
- Falagas, M.E.; Roussos, N.; Vardakas, K.Z. Relative frequency of albicans and the various non-albicans Candida spp among candidemia isolates from inpatients in various parts of the world: A systematic review. Int. J. Infect. Dis. 2010, 14, e954–e966. [Google Scholar] [CrossRef] [Green Version]
- Fu, J.; Ding, Y.; Wei, B.; Wang, L.; Xu, S.; Qin, P.; Wei, L.; Jiang, L. Epidemiology of Candida albicans and non-C.albicans of neonatal candidemia at a tertiary care hospital in western China. BMC Infect. Dis. 2017, 17, 329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvester, E.J.; Watanabe, M.M.Y.; Pittet, L.F.; Boast, A.; Bryant, P.A.; Haeusler, G.M.; Daley, A.J.; Curtis, N.; Gwee, A. Candidemia in Children: A 16-year Longitudinal Epidemiologic Study. Pediatr. Infect. Dis. J. 2021, 40, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Kullberg, B.J.; Arendrup, M.C. Invasive Candidiasis. N. Engl. J. Med. 2015, 373, 1445–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfaller, M.A.; Jones, R.N.; Castanheira, M. Regional data analysis of Candida non-albicans strains collected in United States medical sites over a 6-year period, 2006–2011. Mycoses 2014, 57, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Guinea, J. Global trends in the distribution of Candida species causing candidemia. Clin. Microbiol. Infect. 2014, 20 (Suppl. 6), 5–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfaller, M.A.; Andes, D.R.; Diekema, D.J.; Horn, D.L.; Reboli, A.C.; Rotstein, C.; Franks, B.; Azie, N.E. Epidemiology and outcomes of invasive candidiasis due to non-albicans species of Candida in 2496 patients: Data from the Prospective Antifungal Therapy (PATH) registry 2004–2008. PLoS ONE 2014, 9, e101510. [Google Scholar] [CrossRef] [Green Version]
- Arendrup, M.C.; Dzajic, E.; Jensen, R.H.; Johansen, H.K.; Kjaeldgaard, P.; Knudsen, J.D.; Kristensen, L.; Leitz, C.; Lemming, L.E.; Nielsen, L.; et al. Epidemiological changes with potential implication for antifungal prescription recommendations for fungaemia: Data from a nationwide fungaemia surveillance programme. Clin. Microbiol. Infect. 2013, 19, E343–E353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrington, R.; Kindermann, S.L.; Hou, Q.; Taylor, R.J.; Azie, N.; Horn, D.L. Candidemia and invasive candidiasis among hospitalized neonates and pediatric patients. Curr. Med. Res. Opin. 2017, 33, 1803–1812. [Google Scholar] [CrossRef]
- Warris, A.; Pana, Z.-D.; Oletto, A.; Lundin, R.; Castagnola, E.; Lehrnbecher, T.; Groll, A.H.; Roilides, E.; EUROCANDY Study Group. Etiology and Outcome of Candidemia in Neonates and Children in Europe: An 11-year Multinational Retrospective Study. Pediatr. Infect. Dis. J. 2020, 39, 114–120. [Google Scholar] [CrossRef]
- Chow, N.A.; de Groot, T.; Badali, H.; Abastabar, M.; Chiller, T.M.; Meis, J.F. Potential Fifth Clade of Candida auris, Iran, 2018. Emerg. Infect. Dis. 2019, 25, 1780–1781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szekely, A.; Borman, A.M.; Johnson, E.M. Candida auris Isolates of the Southern Asian and South African Lineages Exhibit Different Phenotypic and Antifungal Susceptibility Profiles In Vitro. J. Clin. Microbiol. 2019, 57, e02055-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsh, R.M.; Sexton, D.J.; Forsberg, K.; Vallabhaneni, S.; Litvintseva, A. Insights into the Unique Nature of the East Asian Clade of the Emerging Pathogenic Yeast Candida auris. J. Clin. Microbiol. 2019, 57, e00007-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhary, A.; Prakash, A.; Sharma, C.; Kordalewska, M.; Kumar, A.; Sarma, S.; Tarai, B.; Singh, A.; Upadhyaya, G.; Upadhyay, S.; et al. A multicentre study of antifungal susceptibility patterns among 350 Candida auris isolates (2009–17) in India: Role of the ERG11 and FKS1 genes in azole and echinocandin resistance. J. Antimicrob. Chemother. 2018, 73, 891–899. [Google Scholar] [CrossRef]
- Kordalewska, M.; Lee, A.; Park, S.; Berrio, I.; Chowdhary, A.; Zhao, Y.; Perlin, D.S. Understanding Echinocandin Resistance in the Emerging Pathogen Candida auris. Antimicrob. Agents Chemother. 2018, 62, e00238-18. [Google Scholar] [CrossRef] [Green Version]
- Kordalewska, M.; Perlin, D.S. Identification of Drug Resistant Candida auris. Front. Microbiol. 2019, 10, 1918. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Diekema, D.J.; Turnidge, J.D.; Castanheira, M.; Jones, R.N. Twenty Years of the SENTRY Antifungal Surveillance Program: Results for Candida Species From 1997–2016. Open Forum Infect. Dis. 2019, 6, S79–S94. [Google Scholar] [CrossRef] [Green Version]
- Berger, S.; El Chazli, Y.; Babu, A.F.; Coste, A.T. Azole Resistance in Aspergillus fumigatus: A Consequence of Antifungal Use in Agriculture? Front. Microbiol. 2017, 8, 1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deorukhkar, S.C.; Saini, S.; Mathew, S. Non-albicans Candida Infection: An Emerging Threat. Interdiscip. Perspect. Infect. Dis. 2014, 2014, 615958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlin, D.S.; Rautemaa-Richardson, R.; Alastruey-Izquierdo, A. The global problem of antifungal resistance: Prevalence, mechanisms, and management. Lancet Infect. Dis. 2017, 17, e383–e392. [Google Scholar] [CrossRef]
- Clancy, C.J.; Nguyen, M.H. Emergence of Candida auris: An International Call to Arms. Clin. Infect. Dis. 2017, 64, 141–143. [Google Scholar] [CrossRef] [Green Version]
- Emara, M.; Ahmad, S.; Khan, Z.; Joseph, L.; Al-Obaid, I.; Purohit, P.; Bafna, R. Candida auris candidemia in Kuwait, 2014. Emerg. Infect. Dis. 2015, 21, 1091–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Solache, M.A.; Casadevall, A. Global warming will bring new fungal diseases for mammals. MBio 2010, 1, e00061-10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, B.R.; Chow, N.; Forsberg, K.; Litvintseva, A.P.; Lockhart, S.R.; Welsh, R.; Vallabhaneni, S.; Chiller, T. On the Origins of a Species: What Might Explain the Rise of Candida auris? J. Fungi 2019, 5, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tedersoo, L.; Bahram, M.; Põlme, S.; Kõljalg, U.; Yorou, N.S.; Wijesundera, R.; Villarreal Ruiz, L.; Vasco-Palacios, A.M.; Thu, P.Q.; Suija, A.; et al. Fungal biogeography. Global diversity and geography of soil fungi. Science 2014, 346, 1256688. [Google Scholar] [CrossRef] [Green Version]
- Satoh, K.; Makimura, K.; Hasumi, Y.; Nishiyama, Y.; Uchida, K.; Yamaguchi, H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol. Immunol. 2009, 53, 41–44. [Google Scholar] [CrossRef]
- Thatchanamoorthy, N.; Rukumani Devi, V.; Chandramathi, S.; Tay, S.T. Candida auris: A Mini Review on Epidemiology in Healthcare Facilities in Asia. J. Fungi 2022, 8, 1126. [Google Scholar] [CrossRef]
- Govender, N.P.; Magobo, R.E.; Mpembe, R.; Mhlanga, M.; Matlapeng, P.; Corcoran, C.; Govind, C.; Lowman, W.; Senekal, M.; Thomas, J. Candida auris in South Africa, 2012–2016. Emerg. Infect. Dis. 2018, 24, 2036–2040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lane, C.R.; Seemann, T.; Worth, L.J.; Easton, M.; Pitchers, W.; Wong, J.; Cameron, D.; Azzato, F.; Bartolo, R.; Mateevici, C.; et al. Incursions of Candida auris into Australia, 2018. Emerg. Infect. Dis. 2020, 26, 1326–1328. [Google Scholar] [CrossRef]
- Worth, L.J.; Harrison, S.J.; Dickinson, M.; van Diemen, A.; Breen, J.; Harper, S.; Marshall, C.; Williamson, D.A.; Thursky, K.A.; Slavin, M.A. Candida auris in an Australian health care facility: Importance of screening high risk patients. Med. J. Aust. 2020, 212, 510–511.e1. [Google Scholar] [CrossRef]
- Rhodes, J.; Fisher, M.C. Global epidemiology of emerging Candida auris. Curr. Opin. Microbiol. 2019, 52, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Tracking. Candida auris|Fungal Diseases|CDC. Available online: https://www.cdc.gov/fungal/candida-auris/tracking-c-auris.html (accessed on 6 December 2022).
- Plachouras, D.; Lötsch, F.; Kohlenberg, A.; Monnet, D.L.; Candida auris survey collaborative group. Candida auris: Epidemiological situation, laboratory capacity and preparedness in the European Union and European Economic Area*, January 2018 to May 2019. Euro Surveill. 2020, 25, 2000240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buil, J.B.; van der Lee, H.A.L.; Curfs-Breuker, I.; Verweij, P.E.; Meis, J.F. External Quality Assessment Evaluating the Ability of Dutch Clinical Microbiological Laboratories to Identify Candida auris. J. Fungi 2019, 5, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewaele, K.; Lagrou, K.; Frans, J.; Hayette, M.-P.; Vernelen, K. Hospital Laboratory Survey for Identification of Candida auris in Belgium. J. Fungi 2019, 5, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keighley, C.; Garnham, K.; Harch, S.A.J.; Robertson, M.; Chaw, K.; Teng, J.C.; Chen, S.C.A. Candida auris: Diagnostic Challenges and Emerging Opportunities for the Clinical Microbiology Laboratory. Curr. Fungal Infect. Rep. 2021, 15, 116–126. [Google Scholar] [CrossRef] [PubMed]
- de Jong, A.W.; Dieleman, C.; Carbia, M.; Mohd Tap, R.; Hagen, F. Performance of Two Novel Chromogenic Media for the Identification of Multidrug-Resistant Candida auris Compared with Other Commercially Available Formulations. J. Clin. Microbiol. 2021, 59, e03220-20. [Google Scholar] [CrossRef]
- Kumar, A.; Sachu, A.; Mohan, K.; Vinod, V.; Dinesh, K.; Karim, S. Simple low cost differentiation of Candida auris from Candida haemulonii complex using CHROMagar Candida medium supplemented with Pal’s medium. Rev. Iberoam. Micol. 2017, 34, 109–111. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Berkow, E.L.; Chow, N.; Welsh, R.M. Candida auris for the clinical microbiology laboratory: Not your grandfather’s Candida species. Clin. Microbiol. Newsl. 2017, 39, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Mizusawa, M.; Miller, H.; Green, R.; Lee, R.; Durante, M.; Perkins, R.; Hewitt, C.; Simner, P.J.; Carroll, K.C.; Hayden, R.T.; et al. Can Multidrug-Resistant Candida auris Be Reliably Identified in Clinical Microbiology Laboratories? J. Clin. Microbiol. 2017, 55, 638–640. [Google Scholar] [CrossRef] [Green Version]
- Kathuria, S.; Singh, P.K.; Sharma, C.; Prakash, A.; Masih, A.; Kumar, A.; Meis, J.F.; Chowdhary, A. Multidrug-Resistant Candida auris Misidentified as Candida haemulonii: Characterization by Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry and DNA Sequencing and Its Antifungal Susceptibility Profile Variability by Vitek 2, CLSI Broth Microdilution, and Etest Method. J. Clin. Microbiol. 2015, 53, 1823–1830. [Google Scholar] [CrossRef]
- Morales-López, S.E.; Parra-Giraldo, C.M.; Ceballos-Garzón, A.; Martínez, H.P.; Rodríguez, G.J.; Álvarez-Moreno, C.A.; Rodríguez, J.Y. Invasive Infections with Multidrug-Resistant Yeast Candida auris, Colombia. Emerg. Infect. Dis. 2017, 23, 162–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz Gaitán, A.C.; Moret, A.; López Hontangas, J.L.; Molina, J.M.; Aleixandre López, A.I.; Cabezas, A.H.; Mollar Maseres, J.; Arcas, R.C.; Gómez Ruiz, M.D.; Chiveli, M.Á.; et al. Nosocomial fungemia by Candida auris: First four reported cases in continental Europe. Rev. Iberoam. Micol. 2017, 34, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Forsberg, K.; Woodworth, K.; Walters, M.; Berkow, E.L.; Jackson, B.; Chiller, T.; Vallabhaneni, S. Candida auris: The recent emergence of a multidrug-resistant fungal pathogen. Med. Mycol. 2019, 57, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Antifungal Susceptibility Testing and Interpretation|Candida auris|Fungal Diseases|CDC. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html (accessed on 7 December 2022).
- Arendrup, M.C.; Prakash, A.; Meletiadis, J.; Sharma, C.; Chowdhary, A. Comparison of EUCAST and CLSI Reference Microdilution MICs of Eight Antifungal Compounds for Candida auris and Associated Tentative Epidemiological Cutoff Values. Antimicrob. Agents Chemother. 2017, 61, 00485-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeffery-Smith, A.; Taori, S.K.; Schelenz, S.; Jeffery, K.; Johnson, E.M.; Borman, A.; Candida auris Incident Management Team; Manuel, R.; Brown, C.S. Candida auris: A Review of the Literature. Clin. Microbiol. Rev. 2018, 31, e00029-17. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.-H.; Kweon, O.J.; Kim, H.R.; Lee, M.-K. Identification of uncommon candida species using commercial identification systems. J. Microbiol. Biotechnol. 2016, 26, 2206–2213. [Google Scholar] [CrossRef]
- Wattal, C.; Oberoi, J.K.; Goel, N.; Raveendran, R.; Khanna, S. Matrix-assisted laser desorption ionization time of flight mass spectrometry (MALDI-TOF MS) for rapid identification of micro-organisms in the routine clinical microbiology laboratory. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Kordalewska, M.; Zhao, Y.; Lockhart, S.R.; Chowdhary, A.; Berrio, I.; Perlin, D.S. Rapid and Accurate Molecular Identification of the Emerging Multidrug-Resistant Pathogen Candida auris. J. Clin. Microbiol. 2017, 55, 2445–2452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- T2Candida Panel. Available online: https://www.t2biosystems.com/products-technology/t2candida-panel/ (accessed on 7 December 2022).
- Arastehfar, A.; Fang, W.; Pan, W.; Lackner, M.; Liao, W.; Badiee, P.; Zomorodian, K.; Badali, H.; Hagen, F.; Lass-Flörl, C.; et al. YEAST PANEL multiplex PCR for identification of clinically important yeast species: Stepwise diagnostic strategy, useful for developing countries. Diagn. Microbiol. Infect. Dis. 2019, 93, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Sexton, D.J.; Bentz, M.L.; Welsh, R.M.; Litvintseva, A.P. Evaluation of a new T2 Magnetic Resonance assay for rapid detection of emergent fungal pathogen Candida auris on clinical skin swab samples. Mycoses 2018, 61, 786–790. [Google Scholar] [CrossRef]
- Yamamoto, M.; Alshahni, M.M.; Tamura, T.; Satoh, K.; Iguchi, S.; Kikuchi, K.; Mimaki, M.; Makimura, K. Rapid Detection of Candida auris Based on Loop-Mediated Isothermal Amplification (LAMP). J. Clin. Microbiol. 2018, 56, 00591-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borman, A.M.; Szekely, A.; Johnson, E.M. Isolates of the emerging pathogen Candida auris present in the UK have several geographic origins. Med. Mycol. 2017, 55, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Briano, F.; Magnasco, L.; Sepulcri, C.; Dettori, S.; Dentone, C.; Mikulska, M.; Ball, L.; Vena, A.; Robba, C.; Patroniti, N.; et al. Candida auris Candidemia in Critically Ill, Colonized Patients: Cumulative Incidence and Risk Factors. Infect. Dis. Ther. 2022, 11, 1149–1160. [Google Scholar] [CrossRef]
- Southwick, K.; Adams, E.H.; Greenko, J.; Ostrowsky, B.; Fernandez, R.; Patel, R.; Quinn, M.; Vallabhaneni, S.; Denis, R.J.; Erazo, R.; et al. 2039. New York State 2016–2018: Progression from Candida auris Colonization to Bloodstream Infection. Open Forum Infect. Dis. 2018, 5, S594–S595. [Google Scholar] [CrossRef] [Green Version]
- Escandón, P.; Chow, N.A.; Caceres, D.H.; Gade, L.; Berkow, E.L.; Armstrong, P.; Rivera, S.; Misas, E.; Duarte, C.; Moulton-Meissner, H.; et al. Molecular Epidemiology of Candida auris in Colombia Reveals a Highly Related, Countrywide Colonization With Regional Patterns in Amphotericin B Resistance. Clin. Infect. Dis. 2019, 68, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Tsay, S.; Kallen, A.; Jackson, B.R.; Chiller, T.M.; Vallabhaneni, S. Approach to the Investigation and Management of Patients with Candida auris, an Emerging Multidrug-Resistant Yeast. Clin. Infect. Dis. 2018, 66, 306–311. [Google Scholar] [CrossRef] [Green Version]
- McPherson, T.D.; Walblay, K.A.; Roop, E.; Soglin, D.; Valley, A.; Logan, L.K.; Vallabhaneni, S.; Black, S.R.; Pacilli, M. Notes from the Field: Candida auris and Carbapenemase-Producing Organism Prevalence in a Pediatric Hospital Providing Long-Term Transitional Care—Chicago, Illinois, 2019. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1180–1181. [Google Scholar] [CrossRef]
- Pasternak, Y.; Rubin, S.; Bilavsky, E.; Mozer-Glassberg, Y.; Levy, I.; Nahum, E.; Rom, E.; Gurevich, M.; Ben-Zvi, H.; Ashkenazi-Hoffnung, L. Risk factors for early invasive fungal infections in paediatric liver transplant recipients. Mycoses 2018, 61, 639–645. [Google Scholar] [CrossRef]
- Gokcebay, D.G.; Yarali, N.; Isik, P.; Bayram, C.; Ozkaya-Parlakay, A.; Kara, A.; Tunc, B. Candida associated bloodstream infections in pediatric hematology patients: A single center experience. Mediterr. J. Hematol. Infect. Dis. 2016, 8, e2016018. [Google Scholar] [CrossRef] [Green Version]
- Sutcu, M.; Salman, N.; Akturk, H.; Dalgıc, N.; Turel, O.; Kuzdan, C.; Kadayifci, E.K.; Sener, D.; Karbuz, A.; Erturan, Z.; et al. Epidemiologic and microbiologic evaluation of nosocomial infections associated with Candida spp in children: A multicenter study from Istanbul, Turkey. Am. J. Infect. Control 2016, 44, 1139–1143. [Google Scholar] [CrossRef]
- Guo, W.; Gu, H.F.; Zhang, H.G.; Chen, S.B.; Wang, J.Q.; Geng, S.X.; Li, L.; Liu, P.; Liu, X.; Ji, Y.R.; et al. An outbreak of Candida parapsilosis fungemia among preterm infants. Genet. Mol. Res. 2015, 14, 18259–18267. [Google Scholar] [CrossRef] [PubMed]
- Magobo, R.E.; Naicker, S.D.; Wadula, J.; Nchabeleng, M.; Coovadia, Y.; Hoosen, A.; Lockhart, S.R.; Govender, N.P.; TRAC-South Africa group. Detection of neonatal unit clusters of Candida parapsilosis fungaemia by microsatellite genotyping: Results from laboratory-based sentinel surveillance, South Africa, 2009–2010. Mycoses 2017, 60, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Pinhati, H.M.S.; Casulari, L.A.; Souza, A.C.R.; Siqueira, R.A.; Damasceno, C.M.G.; Colombo, A.L. Outbreak of candidemia caused by fluconazole resistant Candida parapsilosis strains in an intensive care unit. BMC Infect. Dis. 2016, 16, 433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magobo, R.E.; Corcoran, C.; Seetharam, S.; Govender, N.P. Candida auris-associated candidemia, South Africa. Emerg. Infect. Dis. 2014, 20, 1250–1251. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Bradley, N.; Brooks, S.; Burney, S.; Wassner, C. Management of Patients with Candida auris Fungemia at Community Hospital, Brooklyn, New York, USA, 2016–2018. Emerg. Infect. Dis. 2019, 25, 601–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, J.; Abdolrasouli, A.; Farrer, R.A.; Cuomo, C.A.; Aanensen, D.M.; Armstrong-James, D.; Fisher, M.C.; Schelenz, S. Genomic epidemiology of the UK outbreak of the emerging human fungal pathogen Candida auris. Emerg. Microbes Infect. 2018, 7, 43. [Google Scholar] [CrossRef] [Green Version]
- Sharma, C.; Kumar, N.; Pandey, R.; Meis, J.F.; Chowdhary, A. Whole genome sequencing of emerging multidrug resistant Candida auris isolates in India demonstrates low genetic variation. New Microbes New Infect. 2016, 13, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Chowdhary, A.; Anil Kumar, V.; Sharma, C.; Prakash, A.; Agarwal, K.; Babu, R.; Dinesh, K.R.; Karim, S.; Singh, S.K.; Hagen, F.; et al. Multidrug-resistant endemic clonal strain of Candida auris in India. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 919–926. [Google Scholar] [CrossRef]
- Ostrowsky, B.; Greenko, J.; Adams, E.; Quinn, M.; O’Brien, B.; Chaturvedi, V.; Berkow, E.; Vallabhaneni, S.; Forsberg, K.; Chaturvedi, S.; et al. Candida auris Isolates Resistant to Three Classes of Antifungal Medications—New York, 2019. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 6–9. [Google Scholar] [CrossRef] [Green Version]
- Kilburn, S.; Innes, G.; Quinn, M.; Southwick, K.; Ostrowsky, B.; Greenko, J.A.; Lutterloh, E.; Greeley, R.; Magleby, R.; Chaturvedi, V.; et al. Antifungal Resistance Trends of Candida auris Clinical Isolates in New York and New Jersey from 2016 to 2020. Antimicrob. Agents Chemother. 2022, 66, e0224221. [Google Scholar] [CrossRef]
- Treatment and Management of Infections and Colonization|Candida auris|Fungal Diseases|CDC. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-treatment.html (accessed on 7 December 2022).
- Zhu, Y.; O’Brien, B.; Leach, L.; Clarke, A.; Bates, M.; Adams, E.; Ostrowsky, B.; Quinn, M.; Dufort, E.; Southwick, K.; et al. Laboratory Analysis of an Outbreak of Candida auris in New York from 2016 to 2018: Impact and Lessons Learned. J. Clin. Microbiol. 2020, 58, e01503-19. [Google Scholar] [CrossRef] [Green Version]
- Lyman, M.; Forsberg, K.; Reuben, J.; Dang, T.; Free, R.; Seagle, E.E.; Sexton, D.J.; Soda, E.; Jones, H.; Hawkins, D.; et al. Notes from the Field: Transmission of Pan-Resistant and Echinocandin-Resistant Candida auris in Health Care Facilities—Texas and the District of Columbia, January-April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1022–1023. [Google Scholar] [CrossRef] [PubMed]
- Healey, K.R.; Kordalewska, M.; Jiménez Ortigosa, C.; Singh, A.; Berrío, I.; Chowdhary, A.; Perlin, D.S. Limited ERG11 Mutations Identified in Isolates of Candida auris Directly Contribute to Reduced Azole Susceptibility. Antimicrob. Agents Chemother. 2018, 62, e01427-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, S.E.; Jacobs, J.L.; Dennis, E.K.; Taimur, S.; Rana, M.; Patel, D.; Gitman, M.; Patel, G.; Schaefer, S.; Iyer, K.; et al. Candida auris Pan-Drug-Resistant to Four Classes of Antifungal Agents. Antimicrob. Agents Chemother. 2022, 66, e0005322. [Google Scholar] [CrossRef] [PubMed]
- Biagi, M.J.; Wiederhold, N.P.; Gibas, C.; Wickes, B.L.; Lozano, V.; Bleasdale, S.C.; Danziger, L. Development of High-Level Echinocandin Resistance in a Patient With Recurrent Candida auris Candidemia Secondary to Chronic Candiduria. Open Forum Infect. Dis. 2019, 6, ofz262. [Google Scholar] [CrossRef]
- Chow, N.A.; Muñoz, J.F.; Gade, L.; Berkow, E.L.; Li, X.; Welsh, R.M.; Forsberg, K.; Lockhart, S.R.; Adam, R.; Alanio, A.; et al. Tracing the Evolutionary History and Global Expansion of Candida auris Using Population Genomic Analyses. MBio 2020, 11, e03364-19. [Google Scholar] [CrossRef]
- O’Brien, B.; Liang, J.; Chaturvedi, S.; Jacobs, J.L.; Chaturvedi, V. Pan-resistant Candida auris: New York subcluster susceptible to antifungal combinations. Lancet Microbe 2020, 1, e193–e194. [Google Scholar] [CrossRef]
- Hou, X.; Lee, A.; Jiménez-Ortigosa, C.; Kordalewska, M.; Perlin, D.S.; Zhao, Y. Rapid Detection of ERG11-Associated Azole Resistance and FKS-Associated Echinocandin Resistance in Candida auris. Antimicrob. Agents Chemother. 2019, 63, e01811-18. [Google Scholar] [CrossRef] [Green Version]
- Rybak, J.M.; Sharma, C.; Doorley, L.A.; Barker, K.S.; Palmer, G.E.; Rogers, P.D. Delineation of the Direct Contribution of Candida auris ERG11 Mutations to Clinical Triazole Resistance. Microbiol. Spectr. 2021, 9, e0158521. [Google Scholar] [CrossRef]
- Rudramurthy, S.M.; Chakrabarti, A.; Paul, R.A.; Sood, P.; Kaur, H.; Capoor, M.R.; Kindo, A.J.; Marak, R.S.K.; Arora, A.; Sardana, R.; et al. Candida auris candidaemia in Indian ICUs: Analysis of risk factors. J. Antimicrob. Chemother. 2017, 72, 1794–1801. [Google Scholar] [CrossRef] [PubMed]
- Candida auris Clinical Update—September 2017|Candida auris|Fungal Diseases|CDC. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-alert-09-17.html (accessed on 7 December 2022).
- Ben-Ami, R.; Ashkenazi, L.; Berman, J.; Korolker, N.; Novikov, A. Assessment of Candida auris Response to Antifungal Drugs Using Time–Kill Assays and an Animal Model. Open Forum Infect. Dis. 2017, 4, S73. [Google Scholar] [CrossRef] [Green Version]
- Auriti, C.; Falcone, M.; Ronchetti, M.P.; Goffredo, B.M.; Cairoli, S.; Crisafulli, R.; Piersigilli, F.; Corsetti, T.; Dotta, A.; Pai, M.P. High-Dose Micafungin for Preterm Neonates and Infants with Invasive and Central Nervous System Candidiasis. Antimicrob. Agents Chemother. 2016, 60, 7333–7339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasmann, R.E.; Muilwijk, E.W.; Burger, D.M.; Verweij, P.E.; Knibbe, C.A.; Brüggemann, R.J. Clinical pharmacokinetics and pharmacodynamics of micafungin. Clin. Pharmacokinet. 2018, 57, 267–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bochennek, K.; Balan, A.; Müller-Scholden, L.; Becker, M.; Farowski, F.; Müller, C.; Groll, A.H.; Lehrnbecher, T. Micafungin twice weekly as antifungal prophylaxis in paediatric patients at high risk for invasive fungal disease. J. Antimicrob. Chemother. 2015, 70, 1527–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. Mycamine (R). Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/mycamine-epar-product-information_en.pdf (accessed on 26 December 2022).
- Durand, C.; Maubon, D.; Cornet, M.; Wang, Y.; Aldebert, D.; Garnaud, C. Can we improve antifungal susceptibility testing? Front. Cell Infect. Microbiol. 2021, 11, 720609. [Google Scholar] [CrossRef]
- Knoll, M.A.; Ulmer, H.; Lass-Flörl, C. Rapid Antifungal Susceptibility Testing of Yeasts and Molds by MALDI-TOF MS: A Systematic Review and Meta-Analysis. J. Fungi 2021, 7, 63. [Google Scholar] [CrossRef]
- Vatanshenassan, M.; Boekhout, T.; Meis, J.F.; Berman, J.; Chowdhary, A.; Ben-Ami, R.; Sparbier, K.; Kostrzewa, M. Candida auris Identification and Rapid Antifungal Susceptibility Testing Against Echinocandins by MALDI-TOF MS. Front. Cell Infect. Microbiol. 2019, 9, 20. [Google Scholar] [CrossRef] [Green Version]
- Brennan-Krohn, T.; Friar, L.; Ditelberg, S.; Kirby, J.E. Evaluation of the Synergistic Activity of Antibacterial and Antifungal Drugs against Candida auris Using an Inkjet Printer-Assisted Method. Antimicrob. Agents Chemother. 2021, 65, e0026821. [Google Scholar] [CrossRef] [PubMed]
- Caballero, U.; Eraso, E.; Quindós, G.; Jauregizar, N. In Vitro Interaction and Killing-Kinetics of Amphotericin B Combined with Anidulafungin or Caspofungin against Candida auris. Pharmaceutics 2021, 13, 1333. [Google Scholar] [CrossRef]
- Caballero, U.; Kim, S.; Eraso, E.; Quindós, G.; Vozmediano, V.; Schmidt, S.; Jauregizar, N. In Vitro Synergistic Interactions of Isavuconazole and Echinocandins against Candida auris. Antibiotics 2021, 10, 355. [Google Scholar] [CrossRef] [PubMed]
- Jaggavarapu, S.; Burd, E.M.; Weiss, D.S. Micafungin and amphotericin B synergy against Candida auris. Lancet Microbe 2020, 1, e314–e315. [Google Scholar] [CrossRef]
- O’Brien, B.; Chaturvedi, S.; Chaturvedi, V. In Vitro Evaluation of Antifungal Drug Combinations against Multidrug-Resistant Candida auris Isolates from New York Outbreak. Antimicrob. Agents Chemother. 2020, 64, e02195-19. [Google Scholar] [CrossRef] [PubMed]
- Bidaud, A.L.; Botterel, F.; Chowdhary, A.; Dannaoui, E. In vitro antifungal combination of flucytosine with amphotericin B, voriconazole, or micafungin against Candida auris shows no antagonism. Antimicrob. Agents Chemother. 2019, 63, e01393-19. [Google Scholar] [CrossRef]
- Ghannoum, M.; Isham, N.; Angulo, D.; Borroto-Esoda, K.; Barat, S.; Long, L. Efficacy of Ibrexafungerp (SCY-078) against Candida auris in an In Vivo Guinea Pig Cutaneous Infection Model. Antimicrob. Agents Chemother. 2020, 64, e00854-20. [Google Scholar] [CrossRef]
- Larkin, E.; Hager, C.; Chandra, J.; Mukherjee, P.K.; Retuerto, M.; Salem, I.; Long, L.; Isham, N.; Kovanda, L.; Borroto-Esoda, K.; et al. The Emerging Pathogen Candida auris: Growth Phenotype, Virulence Factors, Activity of Antifungals, and Effect of SCY-078, a Novel Glucan Synthesis Inhibitor, on Growth Morphology and Biofilm Formation. Antimicrob. Agents Chemother. 2017, 61, e02396-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schell, W.A.; Jones, A.M.; Borroto-Esoda, K.; Alexander, B.D. Antifungal Activity of SCY-078 and Standard Antifungal Agents against 178 Clinical Isolates of Resistant and Susceptible Candida Species. Antimicrob. Agents Chemother. 2017, 61, e01102-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pipeline: SCYNEXIS, Inc. (SCYX). Available online: https://www.scynexis.com/pipeline (accessed on 8 December 2022).
- Arendrup, M.C.; Chowdhary, A.; Jørgensen, K.M.; Meletiadis, J. Manogepix (APX001A) In Vitro Activity against Candida auris: Head-to-Head Comparison of EUCAST and CLSI MICs. Antimicrob. Agents Chemother. 2020, 64, e00656-20. [Google Scholar] [CrossRef]
- Berkow, E.L.; Lockhart, S.R. Activity of novel antifungal compound APX001A against a large collection of Candida auris. J. Antimicrob. Chemother. 2018, 73, 3060–3062. [Google Scholar] [CrossRef]
- Hager, C.L.; Larkin, E.L.; Long, L.; Zohra Abidi, F.; Shaw, K.J.; Ghannoum, M.A. In Vitro and In Vivo Evaluation of the Antifungal Activity of APX001A/APX001 against Candida auris. Antimicrob. Agents Chemother. 2018, 62, e02319-17. [Google Scholar] [CrossRef] [Green Version]
- Wiederhold, N.P.; Najvar, L.K.; Shaw, K.J.; Jaramillo, R.; Patterson, H.; Olivo, M.; Catano, G.; Patterson, T.F. Efficacy of Delayed Therapy with Fosmanogepix (APX001) in a Murine Model of Candida auris Invasive Candidiasis. Antimicrob. Agents Chemother. 2019, 63, e01120-19. [Google Scholar] [CrossRef]
- Hope, W.W.; Castagnola, E.; Groll, A.H.; Roilides, E.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; Bassetti, M.; Bille, J.; Cornely, O.A.; et al. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: Prevention and management of invasive infections in neonates and children caused by Candida spp. Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 38–52. [Google Scholar] [CrossRef] [Green Version]
- Maede, Y.; Ibara, S.; Nagasaki, H.; Inoue, T.; Tokuhisa, T.; Torikai, M.; Ishihara, C.; Matsui, T.; Kodaira, Y. Micafungin versus fluconazole for prophylaxis against fungal infections in premature infants. Pediatr. Int. 2013, 55, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Ascher, S.; Smith, P.B.; Benjamin, D.K. Safety of micafungin in infants: Insights into optimal dosing. Expert Opin Drug Saf. 2011, 10, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Vena, A.; Esposito, S. An overview of micafungin as a treatment option for invasive candidiasis in pediatric patients younger than 4 months old. Expert Opin. Pharmacother. 2022, 23, 1987–1993. [Google Scholar] [CrossRef] [PubMed]
- Manzoni, P.; Wu, C.; Tweddle, L.; Roilides, E. Micafungin in premature and non-premature infants: A systematic review of 9 clinical trials. Pediatr. Infect. Dis. J. 2014, 33, e291–e298. [Google Scholar] [CrossRef] [Green Version]
- Sexton, D.J.; Bentz, M.L.; Welsh, R.M.; Derado, G.; Furin, W.; Rose, L.J.; Noble-Wang, J.; Pacilli, M.; McPherson, T.D.; Black, S.; et al. Positive Correlation Between Candida auris Skin-Colonization Burden and Environmental Contamination at a Ventilator-Capable Skilled Nursing Facility in Chicago. Clin. Infect. Dis. 2021, 73, 1142–1148. [Google Scholar] [CrossRef]
- Welsh, R.M.; Bentz, M.L.; Shams, A.; Houston, H.; Lyons, A.; Rose, L.J.; Litvintseva, A.P. Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida auris on a Plastic Health Care Surface. J. Clin. Microbiol. 2017, 55, 2996–3005. [Google Scholar] [CrossRef] [Green Version]
- Chowdhary, A.; Tarai, B.; Singh, A.; Sharma, A. Multidrug-Resistant Candida auris Infections in Critically Ill Coronavirus Disease Patients, India, April–July 2020. Emerg. Infect. Dis. 2020, 26, 2694–2696. [Google Scholar] [CrossRef]
- Magnasco, L.; Mikulska, M.; Giacobbe, D.R.; Taramasso, L.; Vena, A.; Dentone, C.; Dettori, S.; Tutino, S.; Labate, L.; Di Pilato, V.; et al. Spread of Carbapenem-Resistant Gram-Negatives and Candida auris during the COVID-19 Pandemic in Critically Ill Patients: One Step Back in Antimicrobial Stewardship? Microorganisms 2021, 9, 95. [Google Scholar] [CrossRef]
- Prestel, C.; Anderson, E.; Forsberg, K.; Lyman, M.; de Perio, M.A.; Kuhar, D.; Edwards, K.; Rivera, M.; Shugart, A.; Walters, M.; et al. Candida auris Outbreak in a COVID-19 Specialty Care Unit—Florida, July-August 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 56–57. [Google Scholar] [CrossRef]
- Villanueva-Lozano, H.; Treviño-Rangel, R.d.J.; González, G.M.; Ramírez-Elizondo, M.T.; Lara-Medrano, R.; Aleman-Bocanegra, M.C.; Guajardo-Lara, C.E.; Gaona-Chávez, N.; Castilleja-Leal, F.; Torre-Amione, G.; et al. Outbreak of Candida auris infection in a COVID-19 hospital in Mexico. Clin. Microbiol. Infect. 2021, 27, 813–816. [Google Scholar] [CrossRef] [PubMed]
- Infection Prevention and Control for Candida auris|Fungal Diseases|CDC. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-infection-control.html (accessed on 8 December 2022).
- Sharp, A.; Muller-Pebody, B.; Charlett, A.; Patel, B.; Gorton, R.; Lambourne, J.; Cummins, M.; Alcolea-Medina, A.; Wilks, M.; Smith, R.; et al. Screening for Candida auris in patients admitted to eight intensive care units in England, 2017 to 2018. Euro Surveill. 2021, 26, 1900730. [Google Scholar] [CrossRef]
- Kenters, N.; Kiernan, M.; Chowdhary, A.; Denning, D.W.; Pemán, J.; Saris, K.; Schelenz, S.; Tartari, E.; Widmer, A.; Meis, J.F.; et al. Control of Candida auris in healthcare institutions: Outcome of an International Society for Antimicrobial Chemotherapy expert meeting. Int. J. Antimicrob. Agents 2019, 54, 400–406. [Google Scholar] [CrossRef]
- Adams, E.; Quinn, M.; Tsay, S.; Poirot, E.; Chaturvedi, S.; Southwick, K.; Greenko, J.; Fernandez, R.; Kallen, A.; Vallabhaneni, S.; et al. Candida auris in Healthcare Facilities, New York, USA, 2013–2017. Emerg. Infect. Dis. 2018, 24, 1816–1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacilli, M.; Kerins, J.L.; Clegg, W.J.; Walblay, K.A.; Adil, H.; Kemble, S.K.; Xydis, S.; McPherson, T.D.; Lin, M.Y.; Hayden, M.K.; et al. Regional Emergence of Candida auris in Chicago and Lessons Learned From Intensive Follow-up at 1 Ventilator-Capable Skilled Nursing Facility. Clin. Infect. Dis. 2020, 71, e718–e725. [Google Scholar] [CrossRef] [PubMed]
- Sexton, D.J.; Welsh, R.M.; Bentz, M.L.; Forsberg, K.; Jackson, B.; Berkow, E.L.; Litvintseva, A.P. Evaluation of nine surface disinfectants against Candida auris using a quantitative disk carrier method: EPA SOP-MB-35. Infect. Control Hosp. Epidemiol. 2020, 41, 1219–1221. [Google Scholar] [CrossRef]
- Texas Department of State Health Services. Infectious Disease Control. Candida auris (C. auris). Emerging and Acute Infectious Disease Guidelines. 2022. Available online: https://www.dshs.state.tx.us/IDCU/investigation/electronic/EAIDG/Candida-auris-C-auris.pdf (accessed on 28 November 2022).
- Brown, C.S.; Guy, R. National Public Health Response to Candida auris in England. J. Fungi 2019, 5, 93. [Google Scholar] [CrossRef] [Green Version]
- Lockhart, S.R.; Jackson, B.R.; Vallabhaneni, S.; Ostrosky-Zeichner, L.; Pappas, P.G.; Chiller, T. Thinking beyond the Common Candida Species: Need for Species-Level Identification of Candida Due to the Emergence of Multidrug-Resistant Candida auris. J. Clin. Microbiol. 2017, 55, 3324–3327. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Method of Identification | Potential Misidentification [77] |
|---|---|
| VITEK® 2 YST (bioMerieux) | C. haemulonii, C. lusitaniae [80], C. famata [78], C. pelliculosa [16] |
| BD Phoenix™ (Becton Dickinson) | C. haemulonii, C. catenulata |
| API® 20C AUX (bioMerieux) | C. sake, Rhodotorula glutinis |
| API® Candida | C. famata [79] |
| MicroScan (Beckman Coulter) | C. famata, C. guilliermondii, C. lusitaniae, C. parapsilosis, C. tropicalis [79], C. albicans [79] |
| (a) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Country | Number of Cases | Method of Reliable Identification | Initial Misidentification | Method of Misidentification | Reference | |||
| Colombia | 34 | MALDI-TOF MS | C. haemulonii, C. guilliermondii, C. albicans, C. parapsilosis, Rhodotorula rubra | BD Phoenix, microscan | Berrio et al. [31] | |||
| Colombia | 39 | MALDI-TOF MS | C. haemulonii, C. albicans, C. guilliermondii, C. parapsilosis, R. rubra | NA | Escandon et al. [17] | |||
| Colombia | 8 | 50% MALDI-TOF MS 50% presumed C. auris due to susceptibility profile | C. haemulonii, C. pelliculosae | VITEK2 | Alvarado-Socarras et al. [16] | |||
| Venezuela | 13 | ITS sequencing | C. haemulonii | VITEK2 | Calvo et al. [32] | |||
| Iran | 1 | MALDI-TOF MS, rDNA sequencing, WGS | non-albicans Candida | Phenotypic characterization | Abastabar et al. [15] | |||
| Iran | 1 | MALDI-TOF MS, ITS sequencing | none | none | Mirhendi et al. [22] | |||
| India | 17 | Sequencing (2016), VITEK with ID system software version 8.01 software update (2017) | C. haemulonii, C. duobushaemulonii | VITEK | Chandramati et al. [34] * | |||
| India | 5 | VITEK2 MALDI-TOF (VITEK MS) and PCR | NA | NA | Ramya et al. [25] | |||
| India | 5 | ITS and D1/D2 region sequencing | C. haemulonii, C. famata, C. sake | VITEK2, API20C | Chowdhary et al. [36] | |||
| India | 1 | MALDI-TOF and ITS or D1/D2 region sequencing | NA | NA | Kaur et al. [18] | |||
| India | 22 | ITS sequencing | NA | NA | Chakrabarti et al. [33] | |||
| Bangladesh | 3 | ITS sequencing | NA | NA | Sathi et al. [28] | |||
| Pakistan | 1 | Profile numbers 2,000,130, 2,000,173, 2,102,173, 6,102,173 on API 20C AUX in conjunction with phenotypic characteristics and susceptibility profile | NA | NA | Moin et al. [44] | |||
| North Korea | 3 | ITS and D1/D2 region sequencing | C. haemulonii, R. glutinis | VITEK2 YST and API 20C, respectively | Kim et al. [45] | |||
| Republic of Korea | 2 | ITS sequencing | C. haemulonii, R. glutinis | VITEK2 and API20C | Lee et al. [34] | |||
| Oman | 2 | MALDI-TOF MS ITS sequencing | C. haemulonii, C. famata, R. glutinis | BD Phoenix and API AUX 20C | Mohsin et al. [23] | |||
| Italy | 1 | MALDI-TOF MS | NA | NA | Mesini et al. [43] | |||
| Gauteng province | 47 | NA | NA | NA | Shuping et al. [29] | |||
| (b) | ||||||||
| Country | Number of Cases | Susceptibility Profile % of Resistance (available MIC data, μg/mL) | Reference | |||||
| FLC | VRC | CAS | MFG | AFG | AMB | |||
| Colombia | 34 | 15% | NA | 0% | 0% | 8% | 54% | Berrio et al. [31] |
| Colombia | 39 | 30% | NA | NA | NA | 1% | 22% | Escandon et al. [17] |
| Colombia | 8 | 16.7% (MIC range <2–≥64) | 0% (MIC range ≤ 0.12–1) | 0% (MIC range ≤ 0.25) | 0% (MIC range < 0.12) | NA | 100% (MIC range 8–≥64) | Alvarado-Socarras et al. [16] |
| Venezuela | 13 | 100% (MIC range > 64) | 100% (MIC 4) | NA | NA | 0% (MIC range 0.06–0.125) | NA (MIC range 1–2) | Calvo et al. [32] |
| Iran | 1 | 0% (MIC 16) | 0% (MIC 0.125) | NA | 0% (MIC 0.031) | 0% (MIC 0.016) | 0% (MIC 0.5) | Abastabar et al. [15] |
| Iran | 1 | 100% (MIC > 64) | 0% (MIC 0.25) | 0% (MIC 0.5) | NA | 0% (MIC 1) | 0% (MIC 1) | Mirhendi et al. [22] |
| India | 17 | 100% | 0% | NA | 0% | NA | NA | Chandramati et al. [34] * |
| India | 5 | NA | 0% | NA | 0% | 0% | NA | Ramya et al. [25] |
| India | 5 | 100% (MIC range 16–64) | 0% (MIC range 0.125–1) | 0% (MIC range 0.125–0.25) | 0% (MIC range 0.06–0.125) | 0% (MIC range 0.125–0.5) | 0% (MIC range 0.25–1) | Chowdhary et al. [36] |
| India | 1 | 100% (MIC 64) | 0% (MIC 0.5) | 0% (MIC 0.5) | NA | 0% (MIC-2) | 100% (MIC-4) | Kaur et al. [18] |
| India | 22 | 55% (MIC50-8–64) | 5% (MIC50-0.38–1) | 5% (MIC50- 0.5–0.75) | 0% (MIC50- 0.09–1) | 0% (MIC50- 0.12–0.25) | 5% ** (MIC50-0.12–0.5) | Chakrabarti et al. [33] |
| Bangladesh | 3 | 100% (MIC 64) | 33% | NA | NA | NA | 100% (MIC 4) | Sathi et al. [28] |
| Pakistan | 1 | 100% | NA | 0% | NA | 0% | NA | Moin et al. [44] |
| North Korea | 3 | 47% (MIC range 2–128) | NA | 0% (MIC range 0.125–0.25) | 0% (MIC 0.03) | NA | 33% (MIC range 0.38–1.5) | Kim et al. [45] |
| Republic of Korea | 2 | 33% (MIC range 2–128) | 33% (MIC range 0.03–1) | 0% (MIC 0.06) | 0% (MIC 0.03) | NA | 0% (MIC range 0.5–1) | Lee et al. [34] |
| Oman | 2 | 100% (MIC 64) | 0% (MIC 0.5) | NA | 0% (MIC range 0.125–0.25) | 0% (MIC range 0.125–0.5) | 50% (MIC range 1–2) | Mohsin et al. [23] |
| Italy | 1 | 100% (MIC > 256) | NA | 0% (MIC 0.12) | 0% (MIC 0.12) | 0% (MIC 0.25) | 0% (MIC 1) | Mesini et al. [43] |
| Gauteng province | 47 | 90% (MIC range 16–256) | NA | NA | 0% (MIC range 0.03–1) | 0% (MIC range 0.06–0.5) | 0% (MIC range 0.003–1) | Shuping et al. [29] |
| Continent | Country | Number of Cases | Age, Mean | Male Sex | BSI | Underlying Conditions | Treatment | Mortality | Reference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Preterm | CVC | TPN | Surgery | Immunodeficiency 1 | Azole | Echinocandin | AmphoB | ||||||||
| South America | Colombia | 34 | NA | 64% | 100% | 26% | 82% | 56% | 15% | 44% | 29% | 21% | 47% | 41% | Berrio et al. [31] |
| Colombia | 39 | NA (19%) aged < 1 yr) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | Escandon et al. [33] | |
| Colombia | 8 2 | 16 d | NA | 50% | 13% | 38% | NA | 75% | NA | 38% | 88% | 0% | 38% | Alvarado-Socarras et al. [30] | |
| Colombia | 12 3 | 34 d (median) | 75% | 100% | 50% | 100% | 92% | 75% | 33% | NA | NA | NA | 42% | Armstrong et al. [27] | |
| Venezuela | 13 | <2 m, one aged 14 yr | 46% | 100% | 61% | 100% | NA | 46% | NA | 85% | 69% | 23% | 31% | Calvo et al. [32] | |
| Asia | Iran | 1 | 14 yr | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | Abastabar et al. [22] |
| Iran | 1 | 2.5 yr | 100% | 0% | 0% | NA | NA | NA | 100% | 100% | 0% | 100% | NA | Mirhendi et al. [29] | |
| India | 17 | 19 d | 70% | 88% | 88% | 100% | 94% | 47% | NA | 71% | 41% | 53% | 41% | Chandramati et al. [42] | |
| India | 1 | NA | NA | 100% | NA | NA | NA | NA | NA | NA | NA | NA | NA | Kaur et al. [18] | |
| India | 5 | 9 d | 60% | 100% | 100% | 100% | 1000% | NA | NA | 60% | 100% | 0% | 80% | Ramya et al. [41] | |
| India | 5 | 2 yr | 20% | 100% | 40% | 80% | NA | 20% | 80% | 0% | 20% | 60% | 40% | Chowdhary et al. [79] | |
| India | 3 | <1 m | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 67% | Singh et al. [30] | |
| India | 22 | NA (27% < 1 m) | NA | 100% | 18% | 44% | NA | 25% 4 | NA | NA | NA | NA | 41% | Chakrabarti et al. [33] | |
| Bangladesh | 13 | <1 m | NA | 100% | NA | NA | NA | NA | NA | NA | NA | NA | NA | Dutta et al. [37] | |
| Bangladesh | 3 | 10 d | 100% | 100% | NA | NA | NA | NA | NA | 100% | 0% | 0% | 67% | Sathi et al. [28] | |
| Pakistan | 1 | NA | 100% | 100% | NA | 100% | NA | NA | NA | NA | NA | NA | 0% | Moin et al. [44] | |
| North Korea | 3 | NA | NA | 0% | NA | NA | NA | NA | NA | NA | NA | NA | NA | Kim et al. [45] | |
| Republic of Korea | 2 | 1 yr | 50% | 100% | 0% | 50% | 100% | 50% | 50% | 100% | 0% | 100% | 50% | Lee et al. [34] | |
| Oman | 2 | 1 yr | 100% | 100% | NA | NA | NA | NA | 50% | NA | NA | NA | NA | Mohsin et al. [23] | |
| Europe | Italy | 1 | 1 d | 0% | 0% | 100% | NA | NA | NA | NA | 0% | 0% | 0% | 100% 5 | Mesini et al. [43] |
| South Africa | Gauteng province | 47 | NA (15% < 1 m) | NA | 100% | NA | NA | NA | NA | NA | NA | NA | NA | NA | Shuping et al. [29] |
| Gauteng province | 15 | NA (93% < 1 m) | NA | 100% | NA | NA | NA | NA | NA | NA | NA | NA | NA | Chibabhai et al. [35] | |
| Age Group | Preferred Treatment Regimen | Dosing | Alternate Regimen 1 | Dosing |
|---|---|---|---|---|
| Neonates and infants aged < 2 months | Amphotericin B deoxycholate | 1 mg/kg once daily | L-AmB | 5 mg/kg once daily |
| Caspofungin | 25 mg/m2 once daily | |||
| Micafungin | 10 mg/kg once daily | |||
| Children aged ≥ 2 months | Caspofungin | 70 mg/m2 once daily on day 1, followed by 50 mg/m2 once daily, (Max dose 70 mg) | L-AmB | 5 mg/kg once daily |
| Micafungin | 2mg/kg once daily, in children ≥40 kg option to increase to 4 mg/kg once daily (Max dose 100 mg) | |||
| Age group | Prophylaxis in outbreak setting | Dosing | ||
| Neonates in NICUs <1000 g or who have risk factors for invasive candidiasis | Micafungin | 3–4 mg/kg twice weekly or 2 mg/kg/day |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashkenazi-Hoffnung, L.; Rosenberg Danziger, C. Navigating the New Reality: A Review of the Epidemiological, Clinical, and Microbiological Characteristics of Candida auris, with a Focus on Children. J. Fungi 2023, 9, 176. https://doi.org/10.3390/jof9020176
Ashkenazi-Hoffnung L, Rosenberg Danziger C. Navigating the New Reality: A Review of the Epidemiological, Clinical, and Microbiological Characteristics of Candida auris, with a Focus on Children. Journal of Fungi. 2023; 9(2):176. https://doi.org/10.3390/jof9020176
Chicago/Turabian StyleAshkenazi-Hoffnung, Liat, and Chen Rosenberg Danziger. 2023. "Navigating the New Reality: A Review of the Epidemiological, Clinical, and Microbiological Characteristics of Candida auris, with a Focus on Children" Journal of Fungi 9, no. 2: 176. https://doi.org/10.3390/jof9020176
APA StyleAshkenazi-Hoffnung, L., & Rosenberg Danziger, C. (2023). Navigating the New Reality: A Review of the Epidemiological, Clinical, and Microbiological Characteristics of Candida auris, with a Focus on Children. Journal of Fungi, 9(2), 176. https://doi.org/10.3390/jof9020176