
Evaluation of Five Non-Culture-Based Methods for the Diagnosis of Meningeal Sporotrichosis

 , ,
, ,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Location, Design, and Samples
2.2. Definitions
2.3. Routine CSF Analysis
2.4. DNA Extraction and Quality Controls
2.5. Diagnostic Methods
2.5.1. DNA-Based Methods
Nested PCR
Species-Specific PCR
Multiplex qPCR
2.5.2. Limits of Detection (LOD)
2.5.3. Immunoassays
ELISA for IgG detection
ELISA for IgM detection
2.6. Data Analysis
3. Results
3.1. Patients
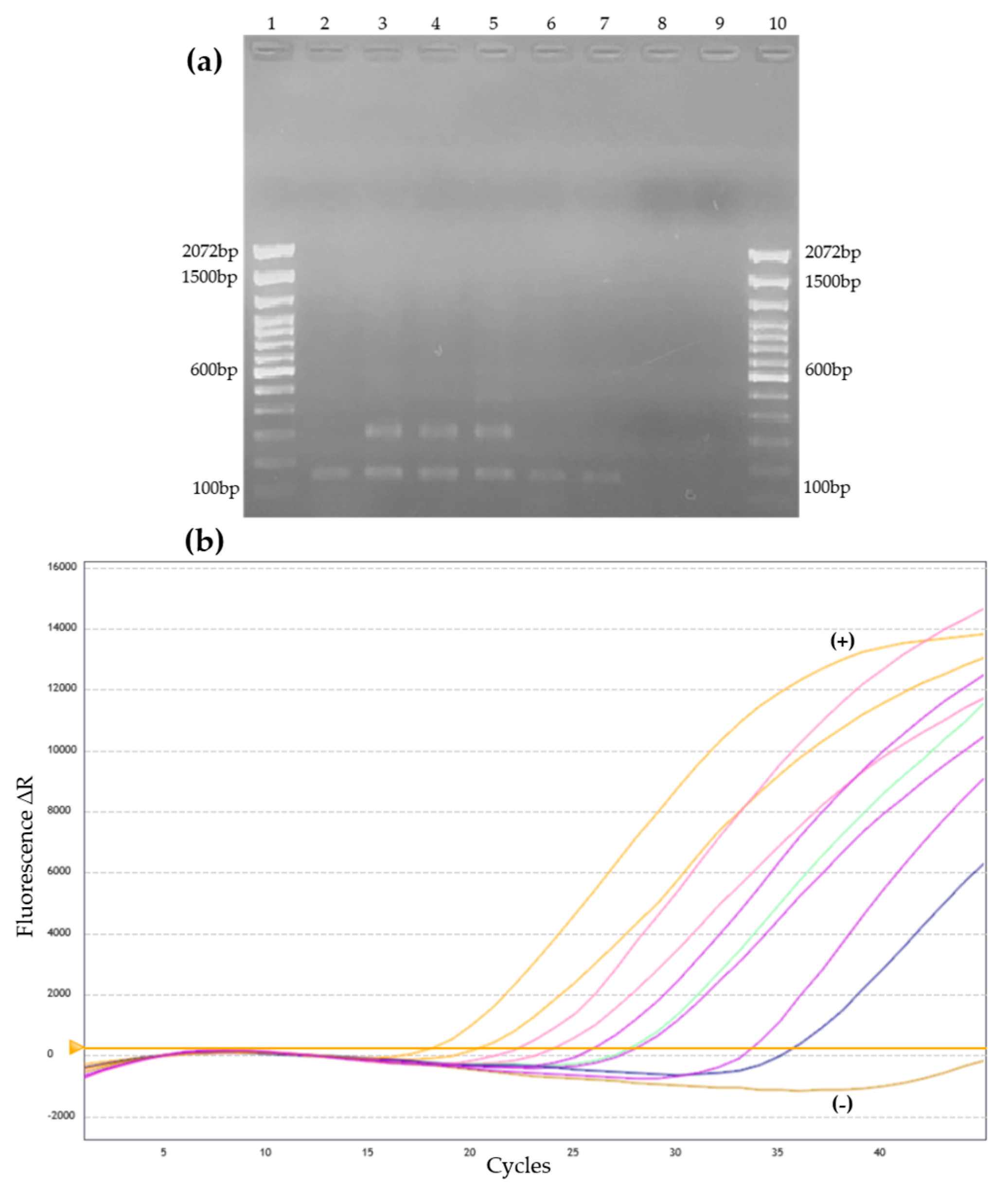
3.2. DNA-Based Methods
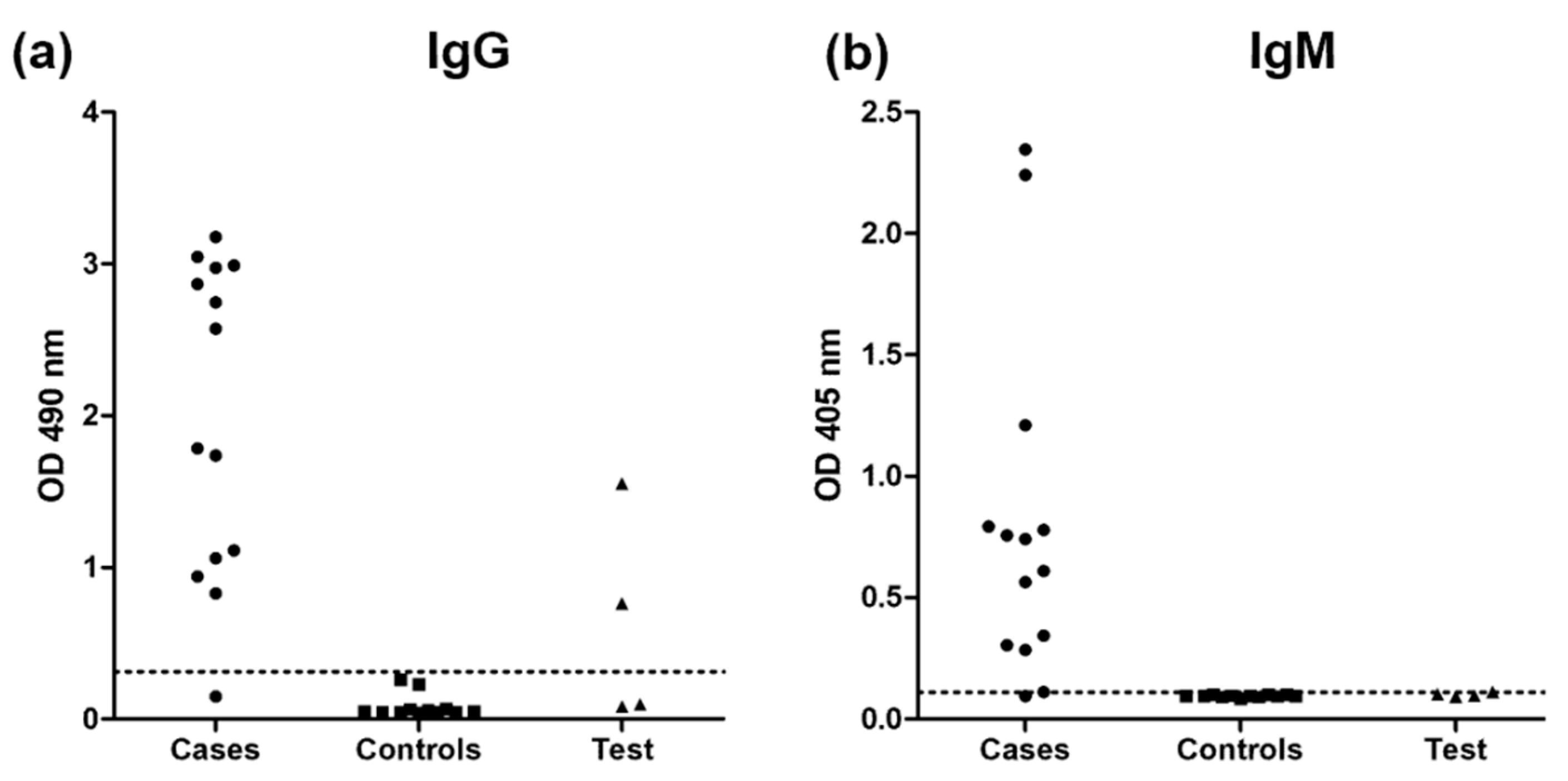
3.3. Immunoassays
3.4. Diagnostic Performance of the Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Góralska, K.; Blaszkowska, J.; Dzikowiec, M. Neuroinfections caused by fungi. Infection 2018, 46, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Saullo, J.L.; Miller, R.A. Updates on histoplasmosis in solid organ transplantation. Curr. Fungal Infect. Rep. 2022, 16, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Jackson, N.R.; Blair, J.E.; Ampel, N.M. Central nervous system infections due to coccidioidomycosis. J. Fungi 2019, 5, 54. [Google Scholar] [CrossRef] [PubMed]
- De Macedo, P.M.; Falcão, E.M.M.; Freitas, D.F.S.; Freitas, A.d.; Coutinho, Z.F.; Muniz, M.d.M.; Zancopé-Oliveira, R.M.; Almeida-Paes, R.; da Silva, M.T.T.; do Valle, A.C.F. Neuroparacoccidioidomycosis: A 13-Year cohort study, Rio de Janeiro, Brazil. J. Fungi 2020, 6, 303. [Google Scholar] [CrossRef] [PubMed]
- Gremião, I.D.F.; Miranda, L.H.M.; Reis, E.G.; Rodrigues, A.M.; Pereira, S.A. Zoonotic Epidemic of Sporotrichosis: Cat to Human Transmission. PLoS Pathog. 2017, 13, e1006077. [Google Scholar] [CrossRef] [PubMed]
- Fichman, V.; Freitas, D.F.S.; do Valle, A.C.F.; de Souza, R.V.; Curi, A.L.L.; Valete-Rosalino, C.M.; de Macedo, P.M.; Varon, A.G.; Figueiredo-Carvalho, M.H.G.; Almeida-Silva, F.; et al. Severe sporotrichosis Treated with Amphotericin B: A 20-Year cohort study in an endemic area of zoonotic transmission. J. Fungi 2022, 8, 469. [Google Scholar] [CrossRef]
- Lima, M.A.; Freitas, D.F.S.; Oliveira, R.V.C.; Fichman, V.; Varon, A.G.; Freitas, A.D.; Lamas, C.C.; Andrade, H.B.; Veloso, V.G.; Almeida-Paes, R.; et al. Meningeal Sporotrichosis due to Sporothrix brasiliensis: A 21-Year Cohort Study from a Brazilian Reference Center. J. Fungi 2022, 9, 17. [Google Scholar] [CrossRef]
- Freitas, D.F.S.; Lima, M.A.; de Almeida-Paes, R.; Lamas, C.C.; do Valle, A.C.F.; Oliveira, M.M.E.; Zancopé-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporotrichosis in the Central Nervous System Caused by Sporothrix brasiliensis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 61, 663–664. [Google Scholar] [CrossRef]
- Orofino-Costa, R.; Freitas, D.F.S.; Bernardes-Engemann, A.R.; Rodrigues, A.M.; Talhari, C.; Ferraz, C.E.; Veasey, J.V.; Quintella, L.; Sousa, M.S.L.A.d.; Vettorato, R.; et al. Human Sporotrichosis: Recommendations from the Brazilian Society of Dermatology for the Clinical, Diagnostic and Therapeutic Management. An. Bras. Dermatol. 2022, 97, 757–777. [Google Scholar] [CrossRef]
- Oliveira, L.C.d.; Almeida-Paes, R.; Pizzini, C.V.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S.; Zancopé-Oliveira, R.M. Diagnostic performance of mycologic and serologic methods in a cohort of patients with suspected sporotrichosis. Rev. Iberoam. Micol. 2019, 36, 61–65. [Google Scholar] [CrossRef]
- Wickes, B.L.; Wiederhold, N.P. Molecular diagnostics in medical mycology. Nat. Commun. 2018, 9, 5135. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, V.K. Sporotrichosis: An overview and therapeutic options. Dermatol. Res. Pract. 2014, 2014, 272376. [Google Scholar] [CrossRef]
- Parreiras de Jesus, A.C.; Grossi de Oliveira, A.L.; Sernizon Guimarães, N.; Mendoza, L.; Toshio Fujiwara, R.; Alves da Silva Menezes, C.; Rocha Vilela, R.V. Serological tests using Sporothrix species antigens for the accurate diagnosis of sporotrichosis: A Meta-Analysis. Diagn. Microbiol. Infect. Dis. 2020, 98, 115131. [Google Scholar] [CrossRef] [PubMed]
- Scott, E.N.; Kaufman, L.; Brown, A.C.; Muchmore, H.G. Serologic studies in the diagnosis and management of meningitis due to Sporothrix schenckii. N. Engl. J. Med. 1987, 317, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Gomes, Y.; Caterino-de-Araujo, A.; Campos, K.; Gonçalves, M.G.; Leite, A.C.; Lima, M.A.; Araújo, A.; Silva, M.T.; Espíndola, O. Loop-Mediated isothermal amplification (LAMP) assay for rapid and accurate confirmatory diagnosis of HTLV-1/2 infection. Viruses 2020, 12, 981. [Google Scholar] [CrossRef]
- Almeida-Silva, F.; de Melo Teixeira, M.; Matute, D.R.; de Faria Ferreira, M.; Barker, B.M.; Almeida-Paes, R.; Guimarães, A.J.; Zancopé-Oliveira, R.M. Genomic Diversity Analysis Reveals a Strong Population Structure in Histoplasma capsulatum LAmA (Histoplasma suramericanum). J. Fungi 2021, 7, 865. [Google Scholar] [CrossRef]
- Hu, S.; Chung, W.-H.; Hung, S.-I.; Ho, H.-C.; Wang, Z.-W.; Chen, C.-H.; Lu, S.-C.; Kuo, T.-T.; Hong, H.-S. Detection of Sporothrix schenckii in clinical samples by a Nested PCR assay. J. Clin. Microbiol. 2003, 41, 1414–1418. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; de Hoog, G.S.; de Camargo, Z.P. Molecular diagnosis of pathogenic Sporothrix species. PLoS Negl. Trop. Dis. 2015, 9, e0004190. [Google Scholar] [CrossRef]
- Zhang, M.; Li, F.; Li, R.; Gong, J.; Zhao, F. Fast diagnosis of sporotrichosis caused by Sporothrix globosa, Sporothrix schenckii, and Sporothrix brasiliensis based on multiplex Real-Time PCR. PLoS Negl. Trop. Dis. 2019, 13, e0007219. [Google Scholar] [CrossRef]
- Almeida-Paes, R.; Pimenta, M.A.; Pizzini, C.V.; Monteiro, P.C.F.; Peralta, J.M.; Nosanchuk, J.D.; Zancopé-Oliveira, R.M. Use of mycelial-phase Sporothrix schenckii exoantigens in an enzyme-linked immunosorbent assay for diagnosis of sporotrichosis by antibody detection. Clin. Vaccine Immunol. CVI 2007, 14, 244–249. [Google Scholar] [CrossRef]
- Galhardo, M.C.; Silva, M.T.; Lima, M.A.; Nunes, E.P.; Schettini, L.E.; de Freitas, R.F.; Paes, R.d.A.; Neves, E.d.S.; do Valle, A.C. Sporothrix schenckii meningitis in AIDS during immune reconstitution syndrome. J. Neurol. Neurosurg. Psychiatry 2010, 81, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.M.E.; Muniz, M.d.M.; Almeida-Paes, R.; Zancope-Oliveira, R.M.; Freitas, A.D.; Lima, M.A.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S. Cerebrospinal fluid PCR: A new approach for the diagnosis of CNS sporotrichosis. PLoS Negl. Trop. Dis. 2020, 14, e0008196. [Google Scholar] [CrossRef] [PubMed]
- Otašević, S.; Momčilović, S.; Stojanović, N.M.; Skvarč, M.; Rajković, K.; Arsić-Arsenijević, V. Non-culture based assays for the detection of fungal pathogens. J. Mycol. Medicale 2018, 28, 236–248. [Google Scholar] [CrossRef] [PubMed]
- Vasconcellos, I.C.d.S.; Dalla Lana, D.F.; Pasqualotto, A.C. The role of molecular tests in the diagnosis of disseminated histoplasmosis. J. Fungi 2019, 6, 1. [Google Scholar] [CrossRef]
- Almeida-Paes, R.; Almeida, M.d.A.; de Macedo, P.M.; Caceres, D.H.; Zancopé-Oliveira, R.M. Performance of two commercial assays for the detection of serum Aspergillus galactomannan in non-neutropenic patients. J. Fungi 2022, 8, 741. [Google Scholar] [CrossRef]
- Almeida-Silva, F.; Damasceno, L.S.; Serna, M.J.B.; Valero, C.; Quintella, L.P.; Almeida-Paes, R.; Muniz, M.d.M.; Zancope-Oliveira, R.M. Multiple opportunistic fungal infections in an individual with severe HIV disease: A case report. Rev. Iberoam. Micol. 2016, 33, 118–121. [Google Scholar] [CrossRef]
- Almeida-Silva, F.; Rabello, V.B.d.S.; Scramignon-Costa, B.d.S.; Zancopé-Oliveira, R.M.; de Macedo, P.M.; Almeida-Paes, R. Beyond domestic cats: Environmental detection of Sporothrix brasiliensis DNA in a hyperendemic area of sporotrichosis in Rio de Janeiro state, Brazil. J. Fungi 2022, 8, 604. [Google Scholar] [CrossRef]
- Valero, C.; de la Cruz-Villar, L.; Zaragoza, Ó.; Buitrago, M.J. New panfungal Real-Time PCR assay for diagnosis of invasive fungal infections. J. Clin. Microbiol. 2016, 54, 2910–2918. [Google Scholar] [CrossRef]
- Khare, V.R.; Gupta, M.K.; Kumar, N.; Bhattnagar, R.; Tilak, R.; Kumar, K.; Kumar, C.; Rana, A. Utility of Nested polymerase chain reaction for fungus in detecting clinically suspected patients of invasive fungal infections and its clinical correlation and comparison with fungal culture. J. Fam. Med. Prim. Care 2020, 9, 4992–4997. [Google Scholar] [CrossRef]
- De Carvalho, J.A.; Monteiro, R.C.; Hagen, F.; Camargo, Z.P.d.; Rodrigues, A.M. Trends in molecular diagnostics and genotyping tools applied for emerging Sporothrix species. J. Fungi 2022, 8, 809. [Google Scholar] [CrossRef]
- Rachman, R.; Ligaj, M.; Chinthapalli, S.; Serafino Wani, R. Zoonotic acquisition of cutaneous Sporothrix brasiliensis infection in the UK. BMJ Case Rep. 2022, 15, e248418. [Google Scholar] [CrossRef] [PubMed]
- Khot, P.D.; Fredricks, D.N. PCR-Based diagnosis of human fungal infections. Expert Rev. Anti Infect. Ther. 2009, 7, 1201–1221. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Paes, R.; Pimenta, M.A.; Monteiro, P.C.F.; Nosanchuk, J.D.; Zancopé-Oliveira, R.M. Immunoglobulins G, M, and A against Sporothrix schenckii exoantigens in patients with sporotrichosis before and during treatment with itraconazole. Clin. Vaccine Immunol. 2007, 14, 1149–1157. [Google Scholar] [CrossRef]
- Bernardes-Engemann, A.R.; Costa, R.C.O.; Miguens, B.R.; Penha, C.V.L.; Neves, E.; Pereira, B.a.S.; Dias, C.M.P.; Mattos, M.; Gutierrez, M.C.; Schubach, A.; et al. Development of an enzyme-linked immunosorbent assay for the serodiagnosis of several clinical forms of sporotrichosis. Med. Mycol. 2005, 43, 487–493. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Sample (CSF) | Diagnosis and Comorbidity/Immunosuppression | Routine Findings | Nested PCR | qPCR | ELISA | ||
|---|---|---|---|---|---|---|---|
| IgG | IgM | ||||||
| a Case group | 1a | Disseminated sporotrichosis/HIV/AIDS/Past of seizures (childhood) | Pleocytosis, low glucose and high protein | + | + | + | + |
| 1b | Pleocytosis and low glucose | + | + | + | + | ||
| 1c | Normal | + | + | + | + | ||
| 2a | Disseminated sporotrichosis/HIV/AIDS/Depression | Pleocytosis, low glucose, high protein and Sporothrix sp. in culture | − | + | + | + | |
| 2b | Pleocytosis, low glucose, high protein and Sporothrix sp. in culture | + | + | + | + | ||
| 3a | Disseminated sporotrichosis/HIV/AIDS/Previous pulmonary TB | Pleocytosis, low glucose and high protein | + | − | + | + | |
| 3b | Pleocytosis and high protein | + | − | + | + | ||
| 3c | Pleocytosis, low glucose and high protein | + | + | + | + | ||
| 4a | Disseminated sporotrichosis/HIV/AIDS/Previous syphilis | Pleocytosis, low glucose and high protein | + | + | + | + | |
| 4b | Pleocytosis, low glucose and high protein | + | + | + | + | ||
| 4c | Pleocytosis, low glucose and high protein | + | − | + | + | ||
| 5 | Disseminated sporotrichosis/HIV/AIDS/Disseminated TB/Alcohol abuse | Sporothrix sp. in culture | + | + | − | − | |
| 6a | Disseminated sporotrichosis/HIV/AIDS/Asthma | Pleocytosis and high protein | + | + | + | + | |
| 6b | High protein | + | + | + | + | ||
| Control group | 7 | Previous disseminated sporotrichosis/Meningeal TB/HIV/AIDS | High protein/ Mycobacterium tuberculosis | − | − | − | − |
| 8 | Spinal syndrome/HIV/AIDS/Pulmonary TB/Syphilis/Disseminated histoplasmosis | Pleocytosis, EBV | − | − | − | − | |
| 9 | Posterior uveitis, optic disc edema | Normal | + | + | − | − | |
| 10 | Investigation of headaches | Normal | − | − | − | − | |
| 11 | Paracoccidioidomycosis/HIV/AIDS | Normal | − | − | − | − | |
| 12 | Disseminated histoplasmosis/Facial herpes zoster/HIV/AIDS | High protein/VZV | − | − | − | − | |
| 13 | Pansinusitis/HIV/AIDS | Normal | − | − | − | − | |
| 14 | PML/Disseminated TB/HIV/AIDS | HSV-2, CMV | − | − | − | − | |
| 15 | Neuroparacoccidioidomycosis | Normal | − | − | − | − | |
| 16 | COVID-19 and Pneumocystis jirovecii pneumonia/HIV/AIDS | Normal | + | − | − | − | |
| 17 | PML/HIV/AIDS | Normal | + | − | − | − | |
| 18 | Cryptococcal meningitis/Disseminated histoplasmosis/HIV/AIDS | Cryptococcal antigen positive | − | − | − | − | |
| a Test group | 19 | Disseminated sporotrichosis/DM | Normal | − | − | + | − |
| 20 | Disseminated sporotrichosis/HIV/AIDS | Normal | + | − | − | − | |
| 21 | Disseminated sporotrichosis/Latent syphilis/Pulmonary TB/HIV/AIDS | Normal | + | + | + | − | |
| 22 | Disseminated sporotrichosis/Facial palsy and neuromotor impairment since birthday/HIV/AIDS | High protein | + | − | − | + | |
| Parameter | Nested PCR | qPCR | IgG ELISA | IgM ELISA |
|---|---|---|---|---|
| Sensitivity | 92.9% (66.1–99.8) | 78.6% (49.2–95.3) | 92.9% (66.1–99.8) | 92.9% (66.1–99.8) |
| Specificity | 75.0% (42.8–94.5) | 91.7% (61.5–99.8) | 100% (73.5–100) | 100% (73.5–100) |
| Accuracy | 84.6% (65.1–95.6) | 84.6% (65.1–95.6) | 96.2% (80.4–99.9) | 96.2% (80.4–99.9) |
| Positive likelihood ratio | 3.71 (1.38–10.00) | 9.43 (1.42–62.81) | ∞ | ∞ |
| Negative likelihood ratio | 0.10 (0.01–0.65) | 0.23 (0.08–0.65) | 0.07 (0.01–0.47) | 0.07 (0.01–0.47) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida-Silva, F.; Almeida, M.d.A.; Rabello, V.B.d.S.; Zancopé-Oliveira, R.M.; Baeza, L.C.; Lamas, C.d.C.; Lima, M.A.; de Macedo, P.M.; Gutierrez-Galhardo, M.C.; Almeida-Paes, R.; et al. Evaluation of Five Non-Culture-Based Methods for the Diagnosis of Meningeal Sporotrichosis. J. Fungi 2023, 9, 535. https://doi.org/10.3390/jof9050535
Almeida-Silva F, Almeida MdA, Rabello VBdS, Zancopé-Oliveira RM, Baeza LC, Lamas CdC, Lima MA, de Macedo PM, Gutierrez-Galhardo MC, Almeida-Paes R, et al. Evaluation of Five Non-Culture-Based Methods for the Diagnosis of Meningeal Sporotrichosis. Journal of Fungi. 2023; 9(5):535. https://doi.org/10.3390/jof9050535
Chicago/Turabian StyleAlmeida-Silva, Fernando, Marcos de Abreu Almeida, Vanessa Brito de Souza Rabello, Rosely Maria Zancopé-Oliveira, Lilian Cristiane Baeza, Cristiane da Cruz Lamas, Marco Antonio Lima, Priscila Marques de Macedo, Maria Clara Gutierrez-Galhardo, Rodrigo Almeida-Paes, and et al. 2023. "Evaluation of Five Non-Culture-Based Methods for the Diagnosis of Meningeal Sporotrichosis" Journal of Fungi 9, no. 5: 535. https://doi.org/10.3390/jof9050535
APA StyleAlmeida-Silva, F., Almeida, M. d. A., Rabello, V. B. d. S., Zancopé-Oliveira, R. M., Baeza, L. C., Lamas, C. d. C., Lima, M. A., de Macedo, P. M., Gutierrez-Galhardo, M. C., Almeida-Paes, R., & Freitas, D. F. S. (2023). Evaluation of Five Non-Culture-Based Methods for the Diagnosis of Meningeal Sporotrichosis. Journal of Fungi, 9(5), 535. https://doi.org/10.3390/jof9050535