1. Introduction
Notable progress has been made, since the turn of the century, in the field of medical image enhancement, segmentation, quantification, and registration [
1]. While the generation of a three-dimensional (3D) segmentation from a set of medical images is almost commmonplace, the question of its accuracy in representing the patient’s health status sufficiently well to inform prognosis and treatment remains one which still requires significant attention. The process of validating the image processing algorithms is therefore of crucial importance. To this end, several options are available: in order of decreasing financial and temporal cost, these are human clinical trials, in vivo animal models, ex vivo human or animal models, physical phantoms and, finally, digital phantoms (DP).
Digital phantoms consist of algorithmically generated data which, in the context of medical imaging, are used to generate synthetic yet realistic images that can be valuable for the calibration of imaging devices, the standardisation of imaging protocols, or the comparison of devices. In addition to cost, the significant advantage of DPs is that they allow potentially unlimited customisation and personalisation, with error-free knowledge of the object of interest. Examples of their use include the dependency of brain tissue perfusion estimates on tracer delay in computed tomography imaging [
2], the creation of a digital population spanning several organs for the optimisation of imaging protocols in the context of myocardial perfusion SPECT [
3], the study of the effect of noise in the validation of the kurtosis model for estimations of brain perfusions using diffusion-weighted imaging in MRI [
4], and the comparison of complication probability when using different modes of radiotherapy on lung tissue [
5]. To our knowledge, no digital phantoms exist of the coronary arteries and/or of the heart.
The use of cardiac DPs, both static and dynamic, for the assessment of imaging modalities has accelerated over the last decade [
6], along with similarly conceived cardiac atlases [
7,
8], to which we return below. Here, we present a static DP that our group has created for the assessment of derived haemodynamic modalities. Our tool represents the main vessels composing the left and right coronary arterial trees, and we demonstrate its use in the validation of our process in (i) the 3D geometry reconstruction and (ii) our computation of virtual fractional flow reserve (vFFR), both of which are embedded in our software suite VIRTUheart
TM. The detailed workflow of the software is described elsewhere (see [
9,
10]). However, our method and the associated DP tool are readily transferable to other clinically oriented workflows.
Briefly, the VIRTUheart
TM software takes as input a pair of coronary angiograms obtained from different viewing angles and allows users to define the vessel endpoints of the segment of interest (typically within the vicinity of a local stenosis in the vessel). The software then reconstructs the 3D geometry of the selected segment. This is then meshed and, after the application of appropriate boundary conditions, computational fluid dynamics (CFD) analysis is carried out using ANSYS Fluent
TM software to obtain the vFFR, i.e., the predicted ratio between the pressure distal to the stenosis and the aortic pressure. This software has been validated in both a clinical setting [
9] and using a physical, 3D-printed phantom [
10]. In this work we report the use of a DP to perform a more thorough and controlled error propagation study in order to provide insight on the effect of view selection, stenosis severity, and stenosis eccentricity on the accuracy of the 3D geometry reconstruction and hence on the computation of vFFR.
Our digital phantom is a minimally parameterised description, based upon a Cartesian grid, of vessel lumens of the most clinically important coronary arteries, and it interacts with CFD transparently. Its intended purpose is not to provide a “passive” cardiac statistical shape model (SSM), a novel cardiac atlas or, indeed, cardiac bioinformatics [
11]. Indeed, more extensively parameterised SSMs and cardiac atlases have been applied in several ways: directly to visualise coronary arteries in 3D (a form of reconstruction), to parameterize epicardial surface geometry (myocardial shape), and to quantify its physiological, pathophysiological, and dynamical variation (especially the consequences of an infarct) by a number of workers [
7,
12]. We return to this matter in the Discussion section.
4. Discussion
In this study, we have developed a DP to allow the assessment of the accuracy of 3D geometry reconstruction and the subsequent computation of vFFR, using the VIRTUheartTM software framework. Although we present a specific instance of use of this digital phantom as an exemplar, this approach could be used in any other software framework dealing with medical image processing and/or CFD analysis on arterial geometries. We have considered the implications of imaging stenoses located in both the LCX and LAD vessels, using several image pairs in each case, with a stenosis severity that represents (and is indeed larger than) the range expected to be observed in clinical practice.
A comparison of the accuracy of the VIRTUheart
TM vessel reconstructions is reported in
Table 2 and
Table 3 of the Results section. These data demonstrate the overall accuracy of the reconstruction of the vessel centreline, with the magnitude of the Hausdorff distance between 3D-DP and 3D-IP reconstructions being less than 1 mm in all cases. The Hausdorff distance was less for the LCX (all values < 0.3 mm) compared with the LAD (all values < 0.85 mm). The ability of the 3D-IP reconstruction to capture the radius of the vessel was good for LCX reconstruction, with the error in absolute average value being < 0.12 mm in all cases, and the
-norm of the pointwise difference along the vessel length being < 0.17 mm. The error increased for the reconstruction of the LAD, with an error in absolute average value of < 0.31 mm and a
-norm of the pointwise difference of < 0.38 mm. The reduced accuracy in LAD reconstruction compared to the LCX is most likely due to the foreshortening of the former vessel at its distal end in all views. Indeed, while it was possible to reconstruct the LCX artery almost entirely, i.e., with the distal endpoint being very close to the endpoint of the vessel, in the case of the LAD, the distal endpoint of the segmentation had to be selected a small distance before the actual vessel endpoint due to significant foreshortening. When computing the Hausdorff distance, the two centerlines (3D-DP and 3D-IP) are registered so that either the distal or the proximal end coincide. The larger discrepancy between 3D-DP and 3D-IP endpoints for the LAD artery then results in a larger Hausdorff distance between the two centrelines.
There was relatively little variation in any of the error metrics with choice of image pairs or with stenosis severity, as they all represent the ability of the reconstruction to capture the overall form of vessel anatomy, rather than the detail of the stenosis itself. As a result, these error metrics are expected to have small influence on the computed vFFR values.
The accuracy of the reconstruction of the vessel radius at the stenosis location was expected to be closely related to the accuracy of the computed vFFR. Greater variation of this metric was observed with choice of image pairs with a range of maximum absolute error from 0.07 mm to 0.20 mm for the LCX and 0.15 mm to 0.24 mm for the LAD. There was no clear relation between absolute error and the stenosis severity; as a result, the percentage error in the stenosis radius tended to increase for larger-percentage diameter reductions. The error in stenosis reconstruction was typically larger for cases with eccentric stenosis, as expected, due to the different views showing different vessel radii depending on the orientation of the eccentricity. Indeed, as visible in
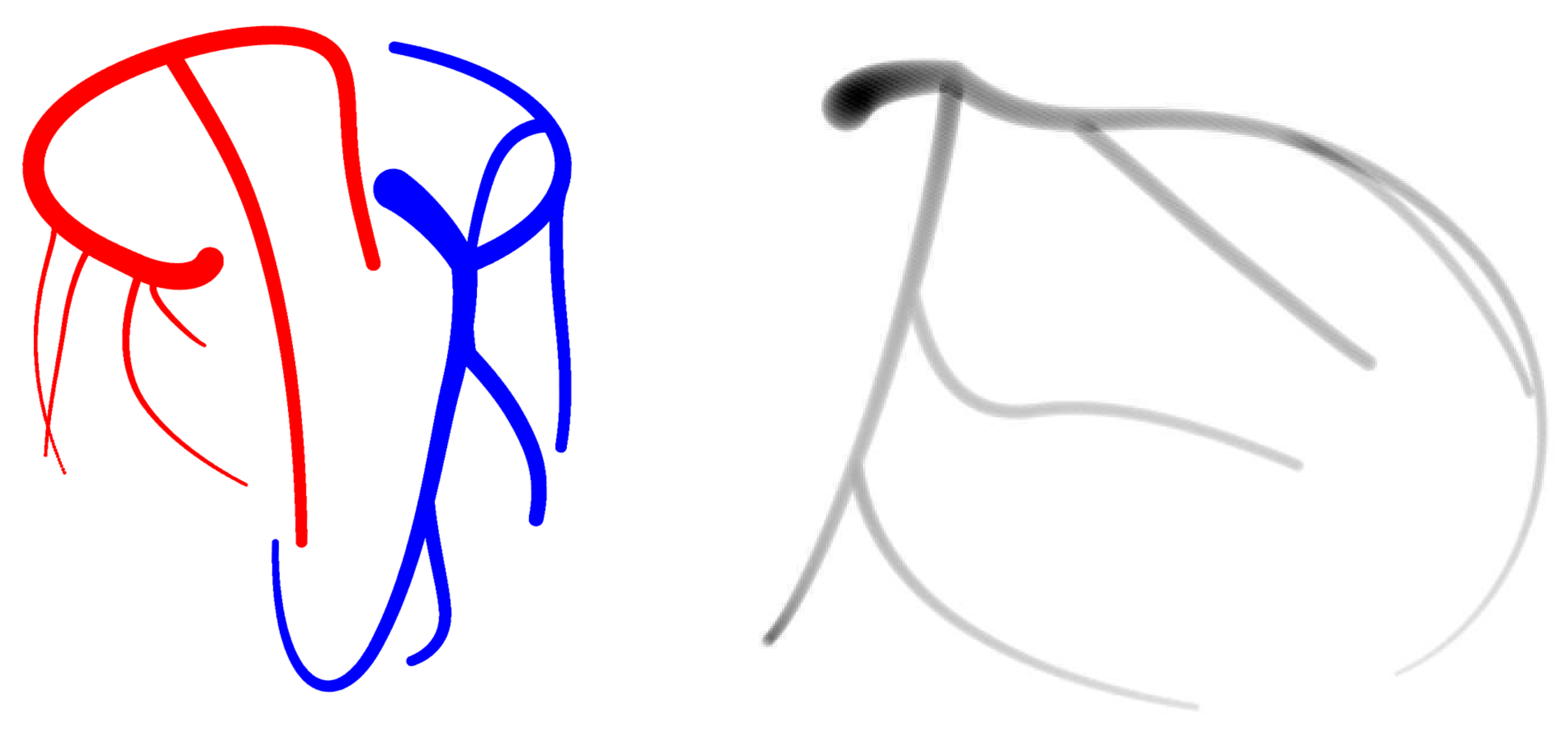
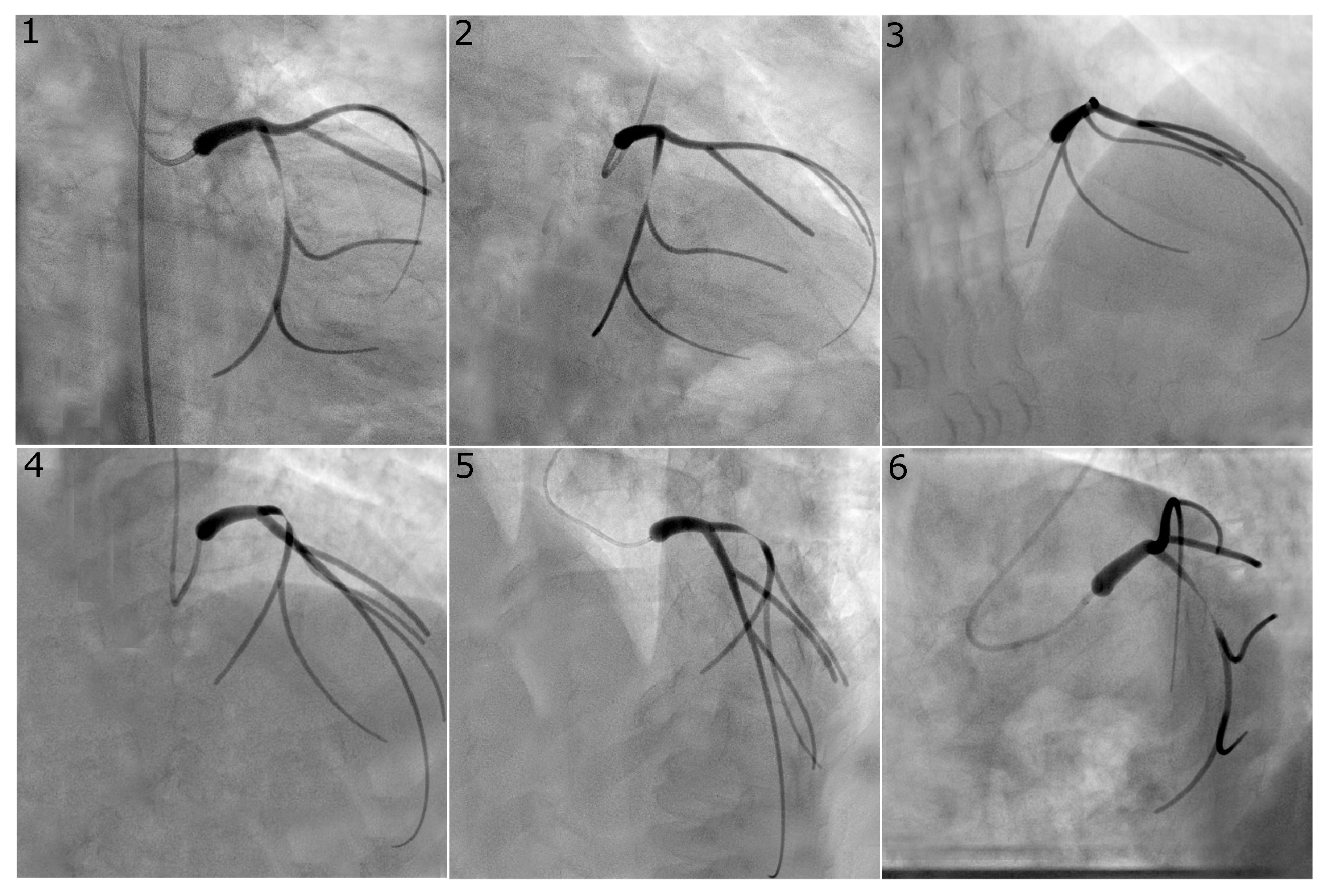
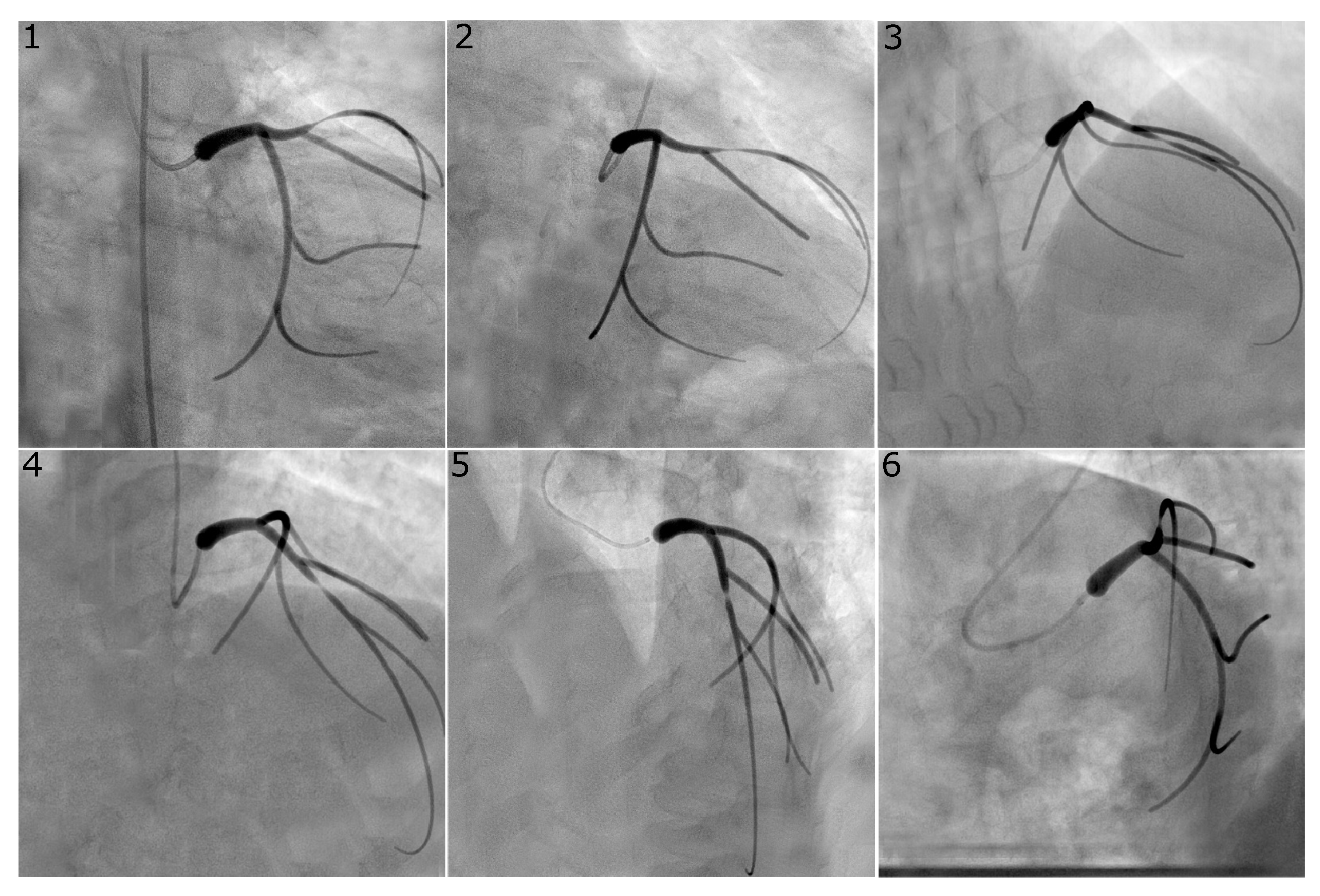
Figure 3, which reports a case of eccentric stenosis in the LAD, the vessel radius appears significantly larger in views 4 and 5, compared to, for example, views 1 and 2. Our software estimates the vessel radius from each of the two angiographic views and averages the two values; the reconstructed local lumen will have a circular shape with a radius equal to that averaged value. It is possible for two views to simultaneously fail to capture the peak value of stenosis, thus obtaining a larger error in the radius estimation and therefore in the vFFR.
A comparison of the vFFR values computed using the 3D-DP geometry and the 3D-IP geometry is reported in
Table 4 and
Table 5. This data demonstrates similar outcomes when reconstructing stenoses in both the LCX and LAD vessels. For the cases 0000, 4040, 4060, and 6040, the error in the computed vFFR is <0.05, and all vFFR values are above the typical threshold of 0.8 that is used to determine if intervention is required. For the 6060 case, the error in the computed vFFR remains less than 0.05, and for the LAD, the vFFR values remain above the threshold for intervention. For the LCX, the hyperaemic vFFR computed using the 3D-DP geometry is 0.77, and the error in vFFR is sufficient to raise this above 0.8 for image pairs 0102 and 0206, but not for image pair 0106. The error becomes more pronounced for all cases involving an
diameter reduction on at least one axis of the stenosis. The only exception to this is the 6080 case in the LAD, where all vFFR errors < 0.05 and all values agree in terms of relation to the 0.8 threshold. This increased error results in disagreement between the 3D-DP data and the 3D-IP data, in terms of the relation to the 0.8 threshold for the 4080, 8040, and 8060 cases across both the baseline and hyperaemic simulations. It is notable that there is variation in agreement with the choice of image pair used. For the 8080 case, although the error in vFFR is large, there is no disagreement between the 3D-DP and 3D-IP values in terms of their relation to the threshold, due to the low values of vFFR for all image pairs.
Less reassuringly, this study also shows that care must be taken in the catheterisation laboratory when selecting an optimal view that highlights the stenosis. Indeed, especially in the case of eccentric stenosis, it is possible for both views to not show maximum stenosis and, thus, overestimate the FFR, in turn underestimating the severity of the disease.
Our software encountered some difficulties when processing cases with very severe stenoses. All cases of or area reduction (i.e., “6080”, “8060”, and “8080”) required increased contrast between the phantom projection and the added background in the digital angiographies. This was due to the fact that the number of voxels traversed by the light (and, thus, the resulting shade of gray in the projection) in the area of peak stenosis was very low; thus, the vessel (the diameter of which spanned 1 to 2 pixels in the projection) was indistinguishable from the background to our image processing algorithm. This problem was overcome by slightly increasing the contrast between the projected phantom vessel and the background.
The CFD analysis also encountered convergence issues for all cases of and one case of area reduction. Although the pressure converged, the residual in the continuity equation displayed non-convergent oscillatory behaviour that might indicate the absence of a steady-state solution. This is not a consequence of using the DP methodology, and both the above issues are not unexpected. We have indeed considered a range of stenosis severity that exceeds that of clinical significance, but remains of interest from the theoretical perspective of CFD analysis. Our software is designed to deal with cases that are of clinical interest and, in particular, to help inform treatment decisions for cases that are close to the treatment decision boundary, which is generally taken at an FFR value of . Accordingly, cases of such high vessel diameter reduction are outside the scope of our software and, in real life, are likely to be severe enough that treatment is deemed necessary, with all estimations or measurements of FFR considered to be superfluous.
Fractional flow reserve is the gold-standard method of assessing lesion severity in coronary artery disease and is recommended in international guidelines. However, due to the increased cost and patient time on the table, its use is not yet as widespread as would be desirable [
18]. In recent years, several software suites that aim to estimate FFR from coronary angiographies have emerged [
9,
19,
20,
21]. All software packages were validated against invasive measurements of FFR via pressure wires, and one was additionally validated against an in vitro model of the coronary circulation [
19]. A systematic review and meta-analysis of the clinical validation studies confirms the good accuracy of the software packages, with small differences between them [
22], although no comparison has been made to date on a shared set of cases. A variation of this software that computes absolute flow within a coronary artery has been validated both clinically and against an in vitro model [
23]. The methodology of the digital phantom could be adopted by any of these software packages, not only as a method for software validation, but also as a tool to identify sources of error to address with software improvements. The widespread adoption of such software has the potential to significantly improve patient care in the context of coronary artery disease, as it bypasses the obstacles presented by the invasive measurement of FFR [
24]. For this reason, it is highly desirable that these softwares continually improve their accuracy and computational efficiency: The digital phantom could be a valuable tool in facilitating this progress.
Recent years have seen growing interest in the development of cardiac atlases [
7,
25], i.e., libraries of patient-specific medical images of cardiac anatomy and associated clinical data. These atlases can be used to inform statistical shape models (SSMs), i.e., mathematically defined geometries parametrised so as to allow the spanning of population-wide possible geometries by varying shape-defining parameters. Some libraries include time-dependent data and are, therefore, also capable of generating
models, which allow the study of heart motion over the cardiac cycle [
12,
26]. SSMs are also valuable tools for the study of population-wide variability in cardiac anatomy, (patho-)physiology, and bioinformatics. For our purposes, however, these tools include complexity and parametrisation requirements that are outside the scope of this work. As we state from the outset, the objective of our DP is to create geometries that are mathematically defined and realistic, but computationally tractable with the minimum number of parameters that would allow reasonable customisation, without adding unnecessary complexity that would hinder the identifiability of error sources and modes of error propagation. However, their use is a possible research direction for our work, following the workflow of Catalano et al. in [
27], for example. In the above, a statistical shape model of the aortic arch is constructed from a library of
patients, an average “template” shape is identified, and principal component analysis is performed to identify modes of variation of the geometry across the population. A set of representative geometries is then generated by varying each mode by
and 3 standard deviations, and finally, CFD analysis is performed on the generated set. The application of a similar workflow to coronary artery disease would validate the use of the digital phantom against real patient-specific data, and could potentially reveal the anatomical features that have the greatest impact on haemodynamic metrics of interest and, thus, help assess lesion severity.
The CFD analysis tool used in our software solves the Navier–Stokes equations as standard practice, but the application of the digital phantom presented in this work is not limited to this case. Indeed, it is defined on a Cartesian grid, which is the native coordinate system for a majority of medical image standards. The definition of the geometrically complex luminal boundary on such a grid is very convenient for more novel CFD tools, such as lattice Boltzmann simulations, which may have a larger role to play in CFD workflows in the future.
The DP presented in this work is generated as a cloud of points, and we attach the coordinates of the constitutive points to this manuscript for both the complete phantom and for individual vessels, with the hope that it can be used and shared in the community or motivate the use of similar methodologies.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}



