
A Bottom-Up Review of Image Analysis Methods for Suspicious Region Detection in Mammograms



Abstract
:1. Introduction
1.1. Motivation and Study Criteria
- Which are various techniques to extract low-level image features from mammograms?
- What machine learning approaches tackle the detection of a mistrustful region in breast images?
- What are the various supervised and unsupervised deep learning approaches used for breast image analysis to detect and/or classify a suspicious region from a mammography image?
- What are the most commonly cited and publicly available mammogram datasets?
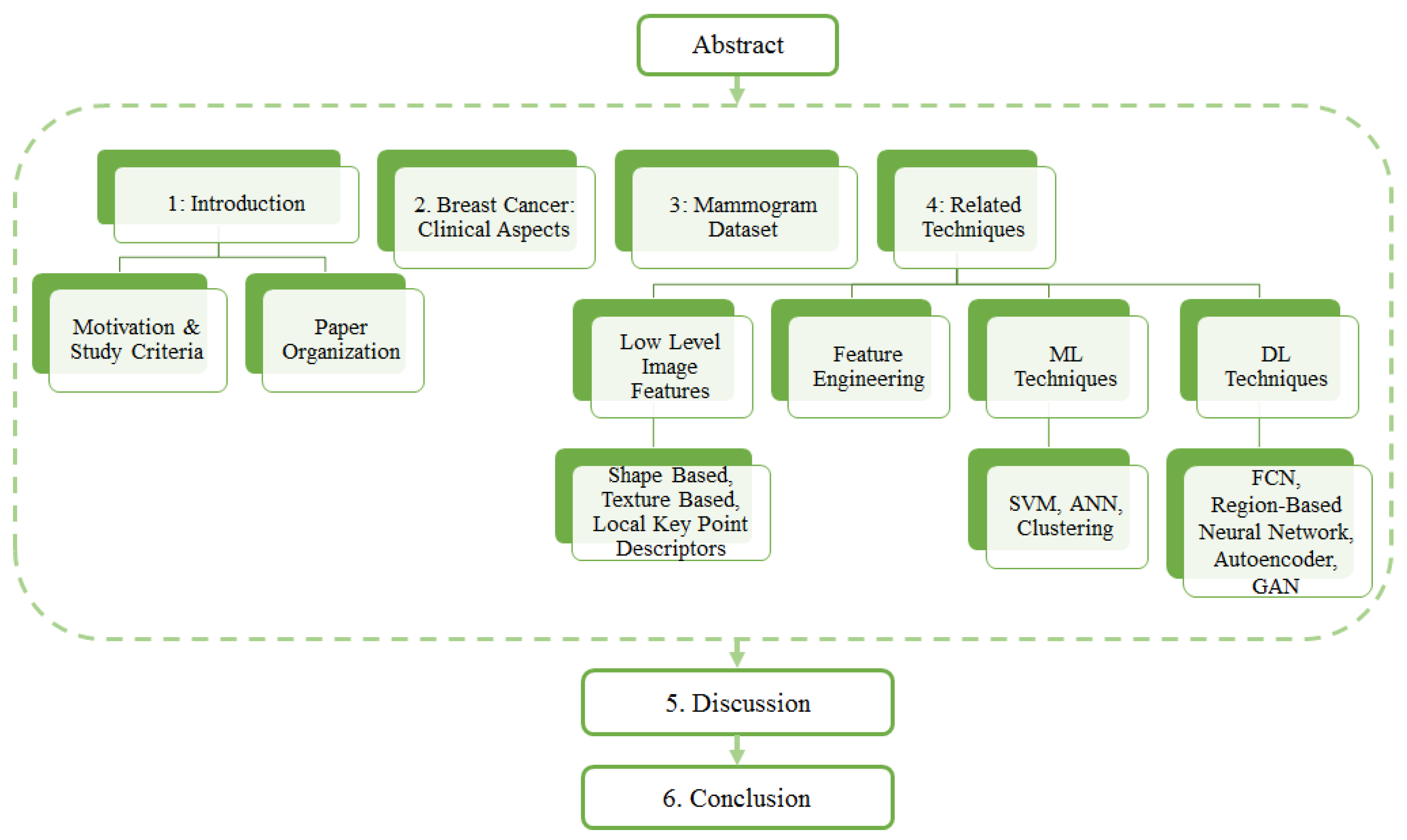
1.2. Paper Organization
2. Breast Cancer: Clinical Aspects
2.1. Breast Positioning and Projection View
2.2. Various Forms of Breast Abnormalities
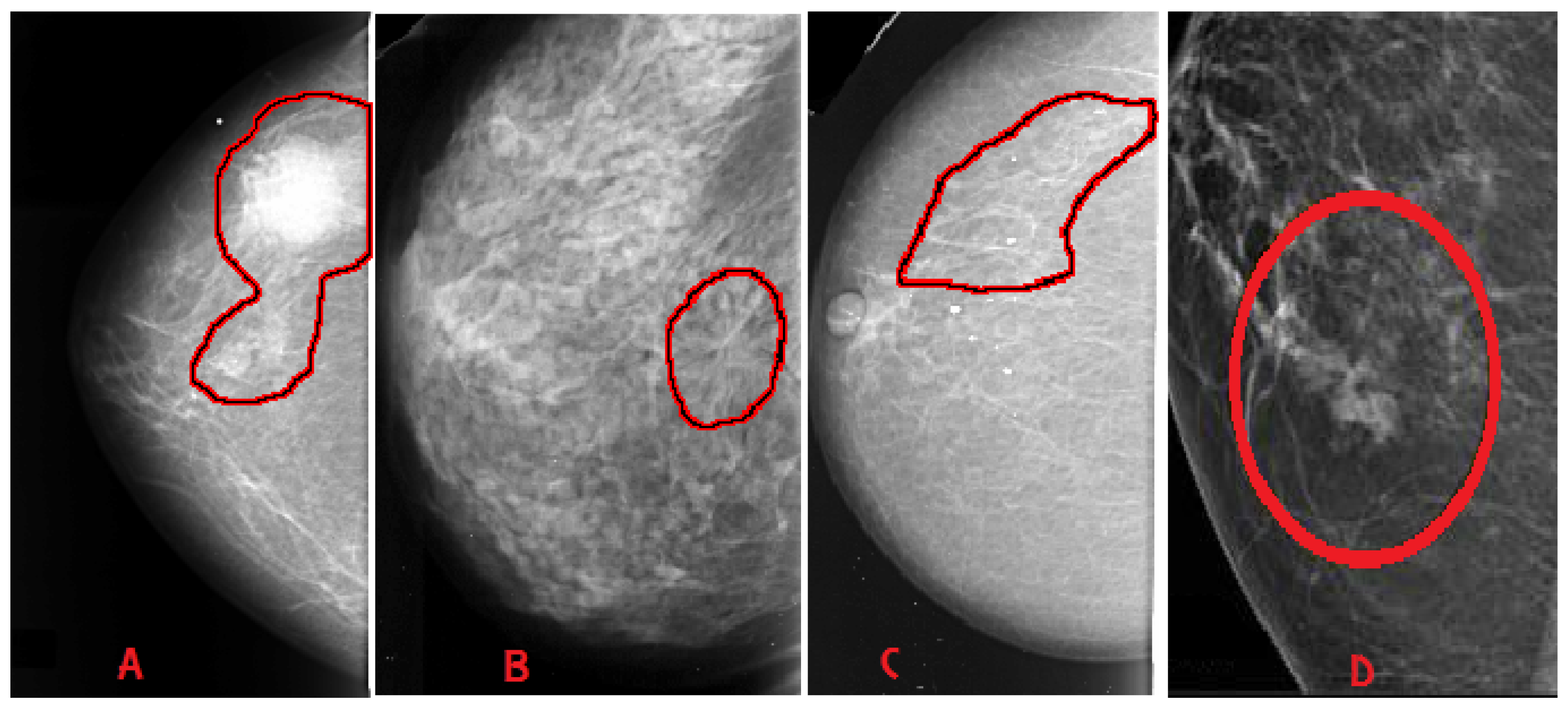
- Mass: A mass is a 3D lesion that can be seen in various projections. Morphological features, such as shape, margin and density, are used for mass characterisation. The shape can be round, oval or irregular. The margin can be not well defined, microlobulated, speculated, indistinct or circumscribed. Figure 4 shows the graphical representation of these morphological features (shape and margin) of a mass along with their subcategories. When superimposed breast tissues hide margins, that is called obscured or partially obscured. Microlobulated infers a suspicious finding. Spiculated margin with radiating lines is also a suspicious finding. Indistinct, also termed as ill-defined, is a suspicious finding too. Circumscribed is a well-defined mass that is a benign finding. Density can be high, low or fat-containing. The density of a mass is related to the expected attenuation of an equal volume of a fibroglandular tissue [6,20]. High density is associated with malignancy.
- Architectural distortion: This abnormality is found when normal architecture is distorted without certain mass visibility. Architectural distortion may include straight thin lines, speculated radiating lines, or focal retraction [6,20]. This abnormality can be seen as an additional feature. If there is a mass with distortion, it is likely to be malignant.
- Calcification: Calcifications are tiny spots of calcium that develop in the breast tissues. Arrangement of calcifications can be diffuse, regional, cluster, linear or segmental [6,20]. There are two types; macrocalcification and microcalcification. Macrocalcifications are large dots of white colour and often spread randomly within the breast area. Microcalcifications are small deposits of calcium, usually non-cancerous, but if visualised as particular patterns and clustered, they may reveal an early sign of malignancy.
- BI-RADS 0 (Assessment Incomplete)—Need further assistance.
- BI-RADS 1 (Normal)—No evidence of lesion.
- BI-RADS 2 (Benign)—Non-cancerous lesion (calcified lesion with high density).
- BI-RADS 3 (Probably benign) —Non-calcified circumscribed mass/obscured mass.
- BI-RADS 4 (Suspicious abnormality)—Microlubulated mass.
- BI-RADS 5 (High probability of malignancy)—Indistinct and spiculated mass.
- BI-RADS 6 (Proven malignancy)—Biopsy-proven malignancy (to check the extent and presence in the opposite breast).
3. Mammogram Datasets

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Origin and Year | Total Cases | Total Images (Approx) | View Type | Image Type | Annotation | Reference Link for the Dataset | |
|---|---|---|---|---|---|---|---|
| SureMaPP | UK, 2020 | 145 | 343 | MLO | DICOM | Centre and radious of circle enclosing the abnormality | https://mega.nz/#F!Ly5g0agB!%E2%80%91QL9uBEvoP8rNig8JBuYfw (accessed on 27 October 2020) |
| DDSM | USA, 1999 | 2620 | 10000 | MLO, CC | LJPEG | Pixel level boundary around abnormality | http://www.eng.usf.edu/cvprg/Mammography/Database.html (accessed on 31 May 2021) |
| CBIS-DDSM | USA, 1999 | 6775 | 10239 | MLO, CC | DICOM | Pixel level boundary around abnormality | https://wiki.cancerimagingarchive.net/display/Public/CBIS-DDSM (accessed on 31 May 2021) |
| INBreast | Portugal, 2011 | 115 | 422 | MLO, CC | DICOM | Pixel level boundary around abnormality | http://medicalresearch.inescporto.pt/breastresearch/GetINbreastDatabase.html (Link is taken from the base paper. Accessed on 31 May 2021) |
| MIAS | 161 | 322 | MLO | PGM | Centre and radious of circle enclosing the abnormality | https://www.repository.cam.ac.uk/handle/1810/250394 (accessed on 31 May 2021) | |
| BCDR | Portugal, 2012 | 1734 | 7315 | MLO, CC | TIFF | Unknown | https://bcdr.eu/information/about (accessed on 31 May 2021) |
| IRMA | Germany, 2008 | Unknown | 10509 | MLO, CC | Several | Several | https://www.spiedigitallibrary.org/conference-proceedings-of-spie/6915/1/Toward-a-standard-reference-database-for-computer-aided-mammography/10.1117/12.770325.short?SSO=1 (accessed on 31 May 2021) |
| BancoWeb LAPIMO | Brazil, 2010 | 320 | 1473 | MLO, CC | TIFF | ROI for few images | http://lapimo.sel.eesc.usp.br/bancoweb (assessed on 31 May 2021) |
3.1. SureMaPP
3.2. DDSM
3.3. CBIS-DDSM
3.4. INBreast
3.5. MIAS
3.6. BCDR
3.7. IRMA
3.8. BancoWeb LAPIMO
4. Related Techniques
4.1. Low Level Image Features
4.1.1. Shape Based Features
Shape Descriptor Analysis Approaches
Shape Descriptors for Classification Systems
Pros and Cons
4.1.2. Texture-Based Features
Texture Descriptors’ Analysis
Texture Descriptors for Classification Systems
Pros and Cons
4.1.3. Local Keypoint Descriptors
Local Keypoint Descriptor Analysis
Local Keypoint Descriptors for Classification Systems
Pros and Cons
| Reference | Technique | Task Performed | Dataset | Performances |
|---|---|---|---|---|
| [39] | Fractal Analysis | Mass Classification | Local Dataset San Paolo Hospital, Bari, Italy | Area under ROC: 0.97 |
| [44] | Local contour features, +SVM | Mass Classification | DDSM | Accuracy: 99.6% |
| [45] | Multiple instance learning: textural and shape features + K-means | Mass Classification | DDSM and MIAS | Sensitivity: 95.6% on DDSM 94.78% on MIAS |
| [46] | Spatial and Morphology domain features | Microcalcification clusters’ detection | USUHS | Sensitivity: 97.6% |
| [47] | Multiwavelet, wavelet, Haralick, and shape features | Microcalcification classification | Nijmegen Database | Area under ROC: 0.89 |
| [48] | Zernike moments | Classification of mammographic mass lesions | Local dataset | Precision: 80% Recall: 20% |
| [41] | Spiculation Index, Fractional Concavity, Compactness | Mass Classification | MIAS | Area under ROC: 0.82 Accuracy: 80% |
| [42] | Average Gradient and Shape Based Feature | Pectoral Muscle Detection | MIAS a local database | False Positives (FP) and False Negatives (FN): FP on MIAS 4.22%, FN on MIAS 3.93%; |
| [49] | Shape features and Haralick features. | Microcalcification classification | Nijmegen Database | Area under ROC: Shape Features 0.82; Haralick Features 0.72 |
| [50] | Swarm optimisation (PSO) algorithm and k-nearest classifier | Microcalcification cluster detection | MIAS and a local dataset from the Bronson Methodist hospital | Accuracy: 96% on MIAS, 94% on BMH |
| [51] | Texture and Morphological Features | Mass Classification | local database | Area under ROC: 0.91 ± 0.02 |
| [40] | Morphological Features | Mass Detection | DDSM | Sensitivity: 92% |
| [52] | Geostatistical and concave geometry (Alpha Shapes) | Mass Detection | MIAS and DDSM | Detection rate: 97.30% on MIAS and 91.63% on DDSM |
| [53] | Co-occurrence matrices, wavelet and ridgelet transforms | Mass Classification | Local Database | AUC = 0.90 |
| [58] | Local Binary Pattern | Breast Mass Recognition | MIAS | Sensitivity 99.65% Specificity 99.24% |
| [54] | Local texture feature and KL Transform | Enhancing texture irregularities | Inbreast | True Positive 96% False Positive 65% False Negative 4% |
| [59] | GLCM and GLRLM features | Mass Classification | DDSM | Accuracy 93.6% |
| [43] | Pixel intensity and Morphological Features | Nipple detection | 144 Mammograms (Local Dataset) | Detection Rate 97.92% |
| Reference | Technique | Task Performed | Dataset | Performances |
|---|---|---|---|---|
| [55] | Texture Feature and Lattice Points | Mammographic Percent Density | Local Database | Area under Curve: 0.60–0.74 |
| [60] | local patterns | Mass Classification | INBreast and MIAS | Accuracy: 82.50% on INBreat 80.30% on MIAS |
| [61] | morphological Top-Hat transform | mass and microcalcification detection | MIAS | Sensitivity and Specificity: 99.02% 99.94% |
| [62] | Texture Features analysis with GPU | Texture analysis in mammograms | DDSM and MIAS | CPU and GPU time on each picture |
| [56] | GLCM features and optical density features | Mass Detection | DDSM | Sensitivity 99% |
| [57] | Density Slicing and Texture Flow-Field Analysis | Mass Detection | MIAS | Area under Curve: 0.79 |
| [63] | Mixture of Gaussian distribution for texture analysis in mammograms | Architectural Distortion Detection in Mammograms | MIAS and DDSM | MIAS Sensitivity 85.5% Specificity 81.0% DDSM Sensitivity 89.2% Specificity 86.7% |
| [70] | FC-VGG16 + SIFT, SURF, ORB, BRISK, and KAZE | Mass Classification | MIAS | SIFT + FC MobileNetV2 Specificity 100%; Sensitivity 100%; |
| [67] | SIFT features, Vocabulary Tree and Contextual Information | Mass Classification | Local dataset of 11553 ROIs from Mammograms | Accuracy 90.8% |
| [68] | SIFT features | Segmentation of Microcalcifications | MIAS | - |
| [71] | Scale-Invariant Feature and K-means clustering | ROI (Region of Interest) detection in mammograms | 4 mammograms from MIAS | - |
| [72] | Local Descriptors and (pLSA) | Parenchymal Tissue Classification | MIAS and DDSM | Accuracy on MIAS 95.42%; DDSM 84.75% |
| [73] | SIFT, LBP and Texton Histograms and SVM | Breast Density Classification | MIAS | Accuracy 93% |
| [74] | Bag of Features (BoF) and SVM | Mass Classification | DDSM | Sensitivity 100% Specificity 99.24% |
| [69] | Histogram Specification and SURF features | Mass Detection | MIAS | Sensitivity 0.89 |
| [75] | Optimised SURF | Mass Classification | MIAS and DDSM | MIAS Accuracy 92.30% DDSM Accuracy 96.87% |
| [76] | LBP plus classifiers (KNN, SVM, Gp, AB) | Abnormality Classification | DDSM | Precision 94.60% Recall 95% |
4.2. Feature Engineering
4.3. Machine Learning
4.3.1. Artificial Neural Networks
Artificial Neural Networks for Mammogram Analysis
4.3.2. Clustering Techniques
Clustering Techniques for Mammogram Analysis
4.3.3. Support Vector Machine (SVM)
SVM for Mammogram Analysis
| Reference | Technique | Task Performed | Dataset | Model Performace |
|---|---|---|---|---|
| [101] | Clustering | Mass Segmentation | MIAS | K-means: 91.18% Fuzzy c-means: 94.12% |
| [102] | Clustering | Mass Detection | DDSM | Accuracy: 90% |
| [103] | Clustering | Suspicious Lesion Segmentation | MIAS | Accuracy: 84.32% |
| [109] | SVM | Microcalcification Detection | InBreast | ROC: 0.8676 Sensitivity: 92% FPR: 2.3 clusters/image |
| [110] | SVM | Mass Detection, Mass Classification | DDSM | Sensitivity: 92.31% Specificity: 82.2% Accuracy: 83.53% ROC: 0.8033. |
| [111] | SVM | Tumor Detection | USFDM, MIAS | Precision:0.98 Sensitivity: 0.73 Specificity: 0.99 Accuracy: 0.81 Score: 0.758 |
| [112] | SVM | Segmentation, Classification | MIAS | Accuracy: 96.55% |
| [113] | SVM | Abnormality Detection | IRMA, DDSM | IRMA: Sensitivity: 99% Specificity: 99% DDSM: Sensitivity: 97% Specificity: 96% |
| [114] | SVM | Mammogram Classification | MIAS | Accuracy: 94% |
| [89] | ANN | Lesion Classification | Mammography Atlas | ROC: 0.95 |
| [90] | ANN | Mammogram Feature Analysis | Private | ROC: 0.91 Specificity: 62% Sensitivity: 95%. |
| [91] | MLP, RBFNN | Microcalcification Detection | MIAS | Positive detection rate: 94.7% False positives per image: 0.2% |
| [94] | SVM, ANN | Microcalcification Characterization | MIAS | SVM: Original feature set, Az: 0.81 Enhanced feature set, Az: 0.80 ANN: Original feature set, Az: 0.73 Enhanced feature set, Az: 0.78 |
| [95] | ANN | Detect and Classify Masses | DDSM | AUC = 0.925 |
| [96] | ANN | Detection of Mass and Architectural Distortion | Private | TPF: 0.620 |
| [97] | ANN | Detection of Breast Cancer | Private | AUC = 0.779 ± 0.025 |
| [98] | ANN | Mass Detection | MIAS | Recognition Rate = 97.08% |
Pros and Cons of Machine Learning Approaches
4.4. Deep Learning Approaches
4.4.1. Supervised Deep Learning
Fully Convolutional Network (FCN)
| Reference | Technique | Task Performed | Dataset | Model Performace |
|---|---|---|---|---|
| [116] | FCN | Breast Density Estimation | Private | Pearson’s rho values: CC View: 0.81 MLO View: 0.79 |
| [117] | FCN | Mass Segmentation | DDSM, INBreast | DDSM: Dice similarity coefficient: 0.915 ± 0.031 Hausdorff distance: 6.257 ± 3.380 INBreast: Dice similarity coefficient: 0.918 ± 0.038 Hausdorff distance: 2.572 ± 0.956 |
| [118] | FC-Densenet | Tumor Segmentation | Private | Dice Index: 0.7697 Pixel Accuracy: 0.7983 Intersection Over Union: 0.6041 |
| [119] | Unet | Mass and Calcification Detection | CBIS-DDSM, INBreast | MassDice score: 67.3% Sensitivity: 70.3% |
| [120] | Attention Dense—Unet | Mass Segmetation | DDSM | F1 Score: 82.24 ± 0.06 Sensitivity: 77.89 ± 0.08 Specificity: 84.69 ± 0.09 Accuracy: 78.38 ± 0.04 |
| [121] | Dense-Unet | Calcification Detection | CBIS-DDSM | Accuracy: 91.47% Sensitivity: 91.22% Specificity: 92.01% F1 Score: 92.19% |
| [122] | CSA Block, Cascade RCNN | Mass Detection | Private, CBIS-DDSM | Average precision: 0.822 Average recall: 0.949 |
| [123] | Faster RCNN | Mass Detection | INBreast, Private | TPR—0.88 FPs/I—0.85 |
| [124] | Faster RCNN | Mass Detection | OMI, INBreast | TPR at FPI: OMI-H: 0.93 at 0.78 OMI-H OMI-G: 0.91 ± 0.06 at 1.70 Inbreast: 0.92 ± 0.08 at 0.30 0.85 ± 0.08 at 1.0 0.95 ± 0.03 at 1.14 |
| [125] | RCNN | Architecturak Distrotion Detection | DDSM | Sensitivity and specificity: 80% FPI: 0.46, TPR: 83% |
| [126] | Faster RCNN | Mass Detection | DDSM | Average Precision: Inception ResNet V2: 0.85 |
| [127] | Mask RCNN-FPN | Multi Detection and Segmentation of Breast Lesions | DDSM, INBreast | Overall Accuracy: 91% |
| [128] | Faster RCNN | Mass Detection | Private | AUC: 0.96 |
| [129] | Faster RCNN | Detection and Classification of Mammogram Lesions | INBreast | AUC: 85% |
| [130] | GAN, ResNet | Data Augmentation, Mammogram Classification | DDSM | AUC: 0.896 |
| [131] | GAN, U-Net | Data Augmentation, Classification | OMID | AUC: 0.846 |
| [132] | GAN | Mass Image Synthesis | DDSM, Private | AUC DDSM: 0.172 Private: 0.144 |
| [133] | CycleGAN | Mass Image Synthesis | BCDR, INBreast | - |
| [134] | GAN | Mammogram Synthesis | Private | - |
| [135] | Sparse Autoencoder | Breast Density Segmentation | Private | PMD scores on AUC: 0.59 |
| [136] | Sparse Autoencoder | Breast Asymmetry Analysis | Private | Sensitivity: 0.97 |
| [137] | Denoising Autoencoders | Breast Density Scoring | Private | AUC: 0.68 |
| [138] | Stacked Autoencoders | Mammogram Classification | MIAS | 98.50% |
| [139] | Sparse Autoencoder, ML classifiers | Mass Classification | MIAS | Accuracy by Random forest: 98.89% |
| [140] | Autoencoder | Mammography Classification | INBreast, IRMA | Accuracy: 98.45% |
FCN for Mammogram Segmentation
Region Based Neural Networks
Region Based Convolutional Neural Networks (R-CNN)
- The approach is not suitable for real-time applications because of its computational cost.
- Selective search approach is not flexible; no learning takes place in it.
- Training happens in three phases; CNN fine-tuning, SVM training and bounding box regressor on thousands of candidate proposals.
- For all region proposals, it is necessary to save feature maps that need a large amount of memory space during training.
Fast RCNN
- The CNN architecture takes image (size = for VGG-16) and its region proposal and outputs the convolution feature map (size = for VGG-16).
- Last pooling layer (layer before fully connected layer) is replaced with a region of interest pooling layer.
- Final fully connected layer and softmax layer are replaced by twin softmax layers and a bounding box regressor.
Faster R-CNN
Region Based Neural Networks for Mammogram Analysis
4.4.2. Unsupervised Deep Learning
Autoencoders
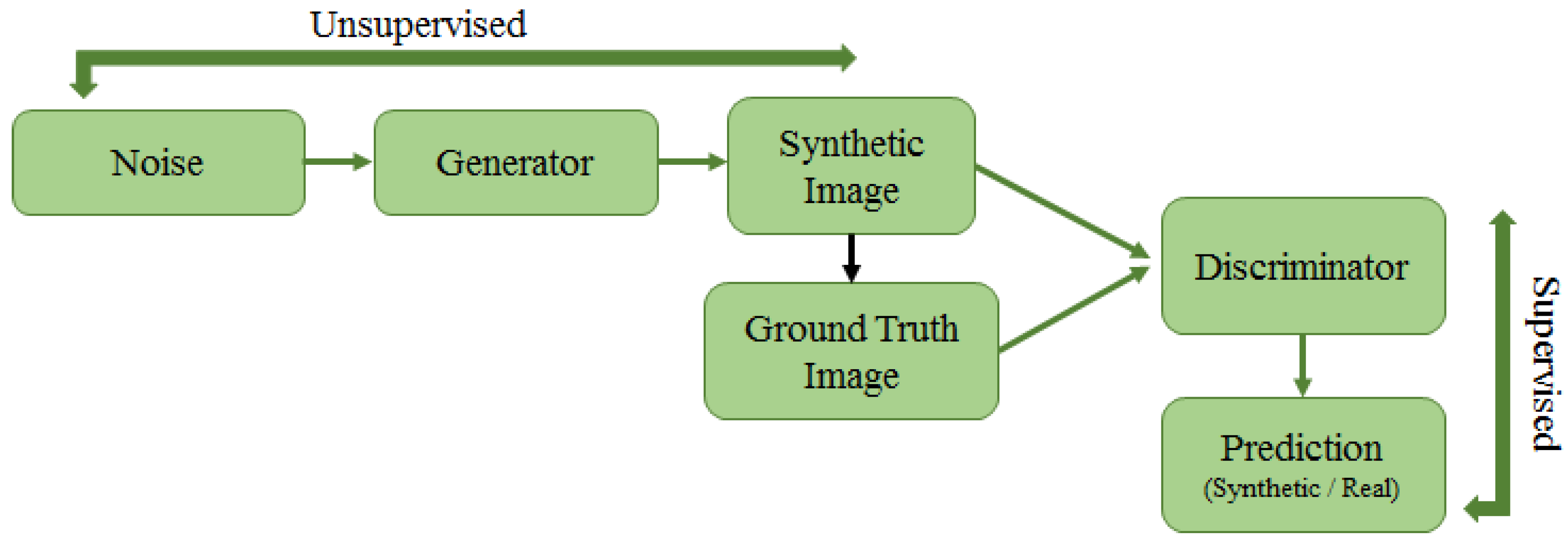
Generative Adversarial Networks (GAN)
4.4.3. Pros and Cons of Deep Learning Approaches
5. Discussion
Final Points
- This paper surveys methods and techniques tackling the detection of suspicious regions in mammograms. The narrative of this work is bottom-up, spanning low-level image feature-based approaches to deep learning architectures. The paper provides summaries of different approaches in tables. In Table 2, Table 3, Table 4 and Table 5, a thorough description of features, performed tasks, datasets, performances is given for the aforementioned methods. Most approaches tackle mass detection and classification, while others address mammogram enhancement, microcalcification detection, and mammogram image generation with unsupervised deep learning architectures. Missing rates on datasets do not allow comparing some methods’ performances. Both MIAS and DDSM datasets stand out in the tables because their employment is far higher than others.
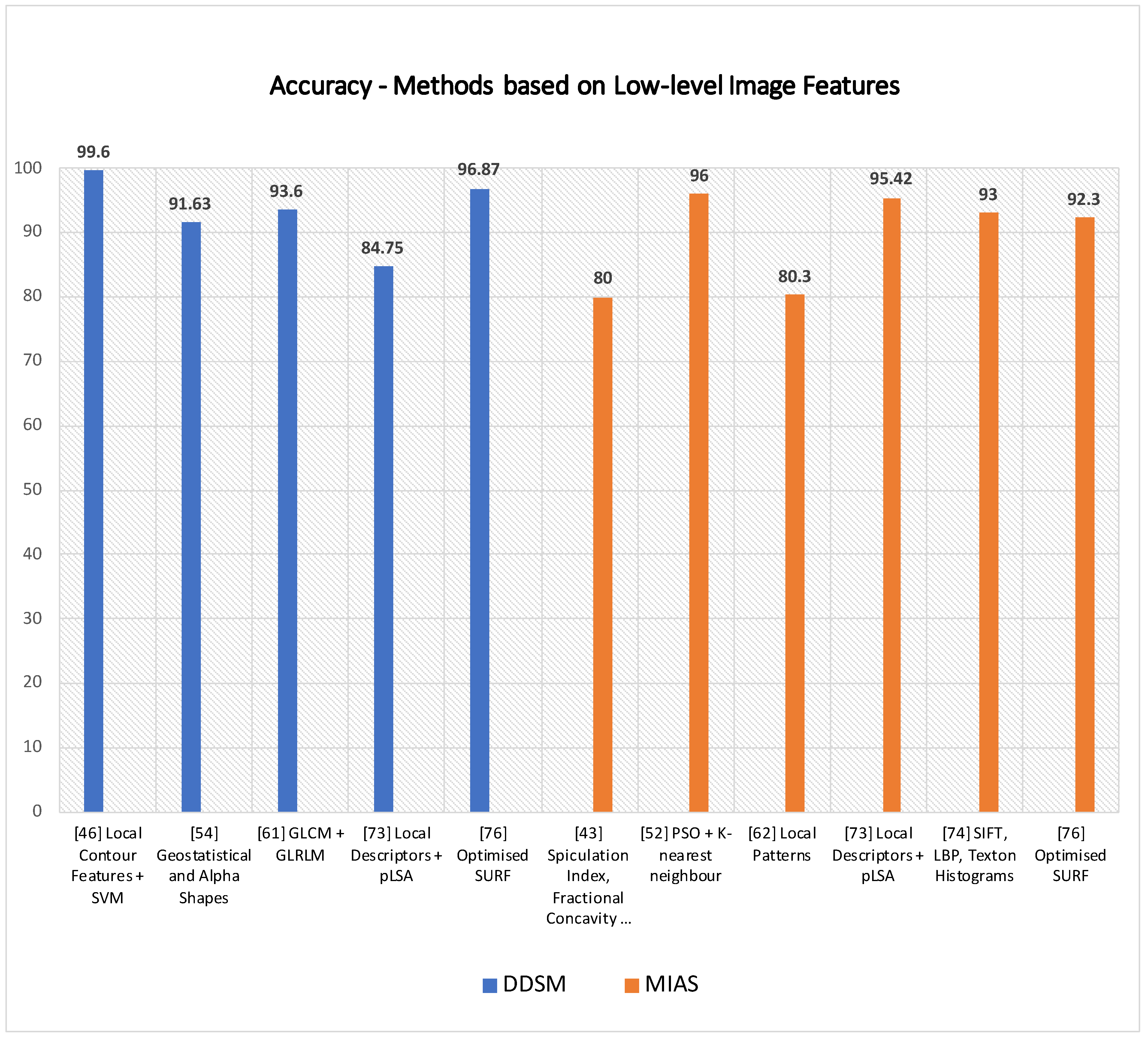
- Machine learning methods are reliable on most datasets. A method based on textural and shape features and K-means [45] achieves sensitivity rates higher than 94% on both datasets; a technique [44] relying on local contour features, 1D signature contour subsection and SVM shows an accuracy rate of 99.6% on a subset of DDSM. Elmoufidi et al. [50] obtained 96% of accuracy on MIAS using a swarm optimisation algorithm for heuristic parameter selection. The method in [40] adopts morphological features for mass detection in mammograms and achieves 92% of sensitivity, but no performance metrics are given about false positives. Geostatistical and concave geometry (alpha shapes) features [52] allow achieving high detection rates on MIAS (97.30%) and DDSM (91.63%). An LBP (local binary pattern) based method [58] turns out to be quite reliable for mass classification in MIAS (99.65% sensitivity and 99.24% specificity). A morphological top-hat transform method [61] is successful in mass and microcalcification detection on MIAS with around 99% specificity and sensitivity rates (Table 2). As highlighted in the pros and cons sections, when low-level image feature descriptors feed into deep neural networks, as in the method by Utomo et al. [70], they can achieve remarkably well (100% specificity and sensitivity rates) on MIAS. The same is true for methods relying on BoF (Bag of Features) and SVM, meaning they are discriminative features for mass classification in mammograms (DDSM). Accuracy rates are achieved by Deshmuk and Bhosle [75] on MIAS (92.3% accuracy) and DDSM (96.8% accuracy) by using an optimised SURF descriptor.
- As listed in Table 4, machine learning methods show some remarkable differences with methods in Table 2 and Table 3. Clustering-based methods by Kamil et al. [101] and Ketabi et al. [102] cannot achieve accuracy rates higher than 94% on MIAS and 90% on DDSM. Sharma et al. [113] achieved high performances in mass detection and classification on IRMA (specificity 99% and sensitivity 99%) and DDSM (specificity 96% and sensitivity 97%) using SVM. The ANN method proposed by Mahersia et al. [98] achieved an average mass recognition rates of 97.08% on MIAS.
- Deep learning methods (Table 5) raise the bar, exploiting their inference knowledge capabilities on more than a single dataset. The autoencoder-based method by Taghanaki et al. [140] performed mammography classification with 98.45% accuracy on INBreast and IRMA. The methods of Selvathi et al. [138,139] scored around 99% accuracy on MIAS by leveraging stacked autencoders, and sparse autoencoder plus random forest.
- Bruno et al. [29] highlighted how convolutional neural networks’ performance could be affected with noise and bias embedded with training dataset images. The availability of larger sized datasets might fully unleash the inference knowledge capabilities of deep learning architectures. Furthermore, it would enable a training-from-scratch process for neural networks. Further comparisons could be then carried out with pre-existing DL models that are fine-tuned over a limited sized mammogram dataset using transfer learning. It is necessary to highlight that most deep learning methods in the biomedical imaging field currently adopt the above-mentioned pipeline laying on data augmentation plus transfer learning, due to the lack of publicly available and manually annotated datasets.
6. Conclusions
- (1)
- Shape-based, texture-based and local keypoint descriptors are the most common techniques used to extract low-level image features from mammograms;
- (2)
- Machine learning approaches such as SVM, ANN, and various clustering techniques are also quite successful over various medical imaging tasks, especially to detect/classify abnormality from mammograms;
- (3)
- Both supervised and unsupervised DL approaches have proven to be best for various mammogram analysis tasks;
- (4)
- As listed in Table 1, researchers in the community of biomedical imaging ran experiments on different publicly available and commonly cited datasets such as SureMaPP, DDSM, INBreast, BCDR, IRMA, BancoWeb LAPIMO etc. Each dataset features images with several properties, due to different acquiring device properties.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CAD | Computer-Aided Diagnosis |
| BI-RADS | Breast Imaging Reporting and Database System |
| AI | Artificial Intelligence |
| ML | Machine Learning |
| DL | Deep Learning |
| SVM | Support Vector Machine |
| ANN | Artificial Neural Network |
| CNN | Convolutional Neural Network |
| SIFT | Scale Invariant Feature Transform |
| SURF | Speed Up Robust Feature |
| FCN | Fully Convolutional Network |
| RCNNN | Region-Based Convolutional Neural Network |
| GAN | Generative Adversarial Network |
| MLO | Mediolateral Oblique |
| CC | Craniocaudal |
| ROI | Region of Interest |
| kNN | k-Nearest Neighbour |
| MC | Microcalcification |
| MCL | Multiple Concentric Layers |
| MRE | Mean Squared Reconstruction Error |
| MSE | Mean Squared Error |
| GLCM | Gray-Level Co-occurrence Matrix |
| GLRLM | Gray-Level Run-Length Matrix |
| LBP | Local Binary Patterns |
| LQP | Local Quinary Patterns |
| CLAHE | Contrast Limited Adaptive Histogram Equalization |
| BRIEF | Binary Robust Independent Elementary Features |
| SOM | Self Organising Maps |
| GA | Genetic Algorithms |
| PFCM | Possibilistic Fuzzy C-Means |
| MIAS | Mammographic Image Analysis Society |
| DDSM | Digital Database of Screening Mammography |
| CBIS-DDSM | Curated Breast Imaging Subset-DDSM |
| BCDR | Breast Cancer Digital Repository |
References
- Society, A.C. Breast cancer facts & figures 2019–2020. Am. Cancer Soc. 2019, 1–44. [Google Scholar]
- Hamidinekoo, A.; Denton, E.; Rampun, A.; Honnor, K.; Zwiggelaar, R. Deep learning in mammography and breast histology, an overview and future trends. Med. Image Anal. 2018, 47, 45–67. [Google Scholar] [CrossRef] [Green Version]
- Yassin, N.I.; Omran, S.; El Houby, E.M.; Allam, H. Machine learning techniques for breast cancer computer aided diagnosis using different image modalities: A systematic review. Comput. Methods Programs Biomed. 2018, 156, 25–45. [Google Scholar] [CrossRef]
- Comelli, A.; Bruno, A.; Di Vittorio, M.L.; Ienzi, F.; Lagalla, R.; Vitabile, S.; Ardizzone, E. Automatic multi-seed detection for MR breast image segmentation. In International Conference on Image Analysis and Processing; Springer: Cham, Switzerland, 2017; pp. 706–717. [Google Scholar]
- Sickles, E.; d’Orsi, C.; Bassett, L.; Appleton, C.; Berg, W.; Burnside, E.; Feig, S.; Gavenonis, S.; Newell, M.; Trinh, M. Acr bi-rads® mammography. ACR BI-RADS® Atlas Breast Imaging Report. Data Syst. 2013, 5, 2013. [Google Scholar]
- Surendiran, B.; Vadivel, A. Mammogram mass classification using various geometric shape and margin features for early detection of breast cancer. Int. J. Med. Eng. Inform. 2012, 4, 36–54. [Google Scholar] [CrossRef]
- Ardizzone, E.; Bruno, A.; Mazzola, G. Scale detection via keypoint density maps in regular or near-regular textures. Pattern Recognit. Lett. 2013, 34, 2071–2078. [Google Scholar] [CrossRef] [Green Version]
- Lowe, D.G. Distinctive image features from scale-invariant keypoints. Int. J. Comput. Vis. 2004, 60, 91–110. [Google Scholar] [CrossRef]
- Pillai, R.; Oza, P.; Sharma, P. Review of machine learning techniques in health care. In Proceedings of the ICRIC 2019, Jammu, India, 8–9 March 2019; Springer: Cham, Switzerland, 2020; pp. 103–111. [Google Scholar]
- Oza, P.; Sharma, P.; Patel, S. Machine Learning Applications for Computer-Aided Medical Diagnostics. In Proceedings of the Second International Conference on Computing, Communications, and Cyber-Security, Ghaziabad, India, 3–4 October; Springer: Singapore, 2021; pp. 377–392. [Google Scholar]
- Oza, P.; Shah, Y.; Vegda, M. A Comprehensive Study of Mammogram Classification Techniques. In Tracking and Preventing Diseases with Artificial Intelligence; Springer: Berlin/Heidelberg, Germany, 2021; pp. 217–238. [Google Scholar]
- Saxena, S.; Gyanchandani, M. Machine learning methods for computer-aided breast cancer diagnosis using histopathology: A narrative review. J. Med. Imaging Radiat. Sci. 2020, 51, 182–193. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Sechopoulos, I.; Teuwen, J.; Mann, R. Artificial intelligence for breast cancer detection in mammography and digital breast tomosynthesis: State of the art. In Seminars in Cancer Biology; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Baldi, P. Autoencoders, unsupervised learning, and deep architectures. In Proceedings of the ICML Workshop on Unsupervised and Transfer Learning, Bellevue, WA, USA, 2 July 2011; pp. 37–49. [Google Scholar]
- Sadoughi, F.; Kazemy, Z.; Hamedan, F.; Owji, L.; Rahmanikatigari, M.; Azadboni, T.T. Artificial intelligence methods for the diagnosis of breast cancer by image processing: A review. Breast Cancer Targets Ther. 2018, 10, 219. [Google Scholar] [CrossRef] [Green Version]
- Moran, M.B.; Conci, A.; de JF Rêgo, S.; Fontes, C.A.; Faria, M.D.B.; Bastos, L.F.; Giraldi, G.A. On Using Image Processing Techniques for Evaluation of Mammography Acquisition Errors. In Anais do XIX Simpósio Brasileiro de Computação Aplicada à Saúde; SBC: Porto Alegre, Brazil, 2019; pp. 330–335. [Google Scholar]
- Andersson, I.; Hildell, J.; Muhlow, A.; Pettersson, H. Number of projections in mammography: Influence on detection of breast disease. Am. J. Roentgenol. 1978, 130, 349–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popli, M.B.; Teotia, R.; Narang, M.; Krishna, H. Breast positioning during mammography: Mistakes to be avoided. Breast Cancer Basic Clin. Res. 2014, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mammography—Breast Imaging Lexicon. Available online: https://radiologyassistant.nl/breast/bi-rads/bi-rads-for-mammography-and-ultrasound-2013#mammography-breast-imaging-lexicon (accessed on 30 September 2010).
- Gemignani, M.L. Breast diseases. Clin. Gynecol. Oncol. 2012, 369–403. [Google Scholar]
- Kamal, R.M.; Helal, M.H.; Mansour, S.M.; Haggag, M.A.; Nada, O.M.; Farahat, I.G.; Alieldin, N.H. Can we apply the MRI BI-RADS lexicon morphology descriptors on contrast-enhanced spectral mammography? Br. J. Radiol. 2016, 89, 20160157. [Google Scholar] [CrossRef] [Green Version]
- Wedegärtner, U.; Bick, U.; Wörtler, K.; Rummeny, E.; Bongartz, G. Differentiation between benign and malignant findings on MR-mammography: Usefulness of morphological criteria. Eur. Radiol. 2001, 11, 1645–1650. [Google Scholar] [CrossRef]
- Breast Imaging-Reporting and Data System (BI-RADS). Available online: https://radiopaedia.org/articles/breast-imaging-reporting-and-data-system-bi-rads (accessed on 20 July 2021).
- Obenauer, S.; Hermann, K.; Grabbe, E. Applications and literature review of the BI-RADS classification. Eur. Radiol. 2005, 15, 1027–1036. [Google Scholar] [CrossRef]
- Beam, C.A.; Layde, P.M.; Sullivan, D.C. Variability in the interpretation of screening mammograms by US radiologists: Findings from a national sample. Arch. Intern. Med. 1996, 156, 209–213. [Google Scholar] [CrossRef]
- Berg, W.A.; Campassi, C.; Langenberg, P.; Sexton, M.J. Breast Imaging Reporting and Data System: Inter-and intraobserver variability in feature analysis and final assessment. Am. J. Roentgenol. 2000, 174, 1769–1777. [Google Scholar] [CrossRef] [Green Version]
- Geller, B.M.; Barlow, W.E.; Ballard-Barbash, R.; Ernster, V.L.; Yankaskas, B.C.; Sickles, E.A.; Carney, P.A.; Dignan, M.B.; Rosenberg, R.D.; Urban, N.; et al. Use of the American College of Radiology BI-RADS to report on the mammographic evaluation of women with signs and symptoms of breast disease. Radiology 2002, 222, 536–542. [Google Scholar] [CrossRef] [Green Version]
- Bruno, A.; Ardizzone, E.; Vitabile, S.; Midiri, M. A novel solution based on scale invariant feature transform descriptors and deep learning for the detection of suspicious regions in mammogram images. J. Med. Signals Sens. 2020, 10, 158. [Google Scholar]
- Heath, M.; Bowyer, K.; Kopans, D.; Kegelmeyer, P.; Moore, R.; Chang, K.; Munishkumaran, S. Current status of the digital database for screening mammography. In Digital Mammography; Springer: Dordrecht, The Netherlands, 1998; pp. 457–460. [Google Scholar]
- Lee, R.S.; Gimenez, F.; Hoogi, A.; Miyake, K.K.; Gorovoy, M.; Rubin, D.L. A curated mammography data set for use in computer-aided detection and diagnosis research. Sci. Data 2017, 4, 1–9. [Google Scholar] [CrossRef]
- Moreira, I.C.; Amaral, I.; Domingues, I.; Cardoso, A.; Cardoso, M.J.; Cardoso, J.S. Inbreast: Toward a full-field digital mammographic database. Acad. Radiol. 2012, 19, 236–248. [Google Scholar] [CrossRef] [Green Version]
- Suckling, J.; Parker, J.; Dance, D.; Astley, S.; Hutt, I.; Boggis, C.; Ricketts, I.; Stamatakis, E.; Cerneaz, N.; Kok, S.; et al. Mammographic Image Analysis Society (mias) Database v1. 21. Available online: https://www.repository.cam.ac.uk/handle/1810/250394 (accessed on 18 September 2021).
- Lopez, M.; Posada, N.; Moura, D.C.; Pollán, R.R.; Valiente, J.M.F.; Ortega, C.S.; Solar, M.; Diaz-Herrero, G.; Ramos, I.; Loureiro, J.; et al. BCDR: A breast cancer digital repository. In Proceedings of the 15th International Conference on Experimental Mechanics, Porto, Portugal, 22 July 2012; Volume 1215. [Google Scholar]
- Oliveira, J.E.; Gueld, M.O.; Araújo, A.d.A.; Ott, B.; Deserno, T.M. Toward a standard reference database for computer-aided mammography. In Medical Imaging 2008: Computer-Aided Diagnosis; International Society for Optics and Photonics: Bellingham, WA, USA, 2008; Volume 6915, p. 69151Y. [Google Scholar]
- Matheus, B.R.N.; Schiabel, H. Online mammographic images database for development and comparison of CAD schemes. J. Digit. Imaging 2011, 24, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Nemoto, M.; Masutani, Y.; Nomura, Y.; Hanaoka, S.; Miki, S.; Yoshikawa, T.; Hayashi, N.; Ootomo, K. Machine Learning for Computer-aided Diagnosis. Igaku Butsuri Nihon Igaku Butsuri Gakkai Kikanshi Jpn. J. Med. Phys. Off. J. Jpn. Soc. Med. Phys. 2016, 36, 29–34. [Google Scholar]
- Sampat, M.P.; Markey, M.K.; Bovik, A.C. Computer-aided detection and diagnosis in mammography. Handb. Image Video Process. 2005, 2, 1195–1217. [Google Scholar]
- Raguso, G.; Ancona, A.; Chieppa, L.; L’Abbate, S.; Pepe, M.L.; Mangieri, F.; De Palo, M.; Rangayyan, R.M. Application of fractal analysis to mammography. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 3182–3185. [Google Scholar] [CrossRef]
- Eltonsy, N.H.; Tourassi, G.D.; Elmaghraby, A.S. A Concentric Morphology Model for the Detection of Masses in Mammography. IEEE Trans. Med. Imaging 2007, 26, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Rangayyan, R.M.; Mudigonda, N.R.; Desautels, J.L. Boundary modelling and shape analysis methods for classification of mammographic masses. Med. Biol. Eng. Comput. 2000, 38, 487–496. [Google Scholar] [CrossRef]
- Chakraborty, J.; Mukhopadhyay, S.; Singla, V.; Khandelwal, N.; Bhattacharyya, P. Automatic detection of pectoral muscle using average gradient and shape based feature. J. Digit. Imaging 2012, 25, 387–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustra, M.; Bozek, J.; Grgic, M. Nipple detection in craniocaudal digital mammograms. In Proceedings of the 2009 International Symposium ELMAR, Zadar, Croatia, 28–30 September 2009; pp. 15–18. [Google Scholar]
- Li, H.; Meng, X.; Wang, T.; Tang, Y.; Yin, Y. Breast masses in mammography classification with local contour features. Biomed. Eng. Online 2017, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Elmoufidi, A.; El Fahssi, K.; Jai-Andaloussi, S.; Sekkaki, A.; Gwenole, Q.; Lamard, M. Anomaly classification in digital mammography based on multiple-instance learning. IET Image Process. 2017, 12, 320–328. [Google Scholar] [CrossRef]
- Zhang, L.; Qian, W.; Sankar, R.; Song, D.; Clark, R. A new false positive reduction method for MCCs detection in digital mammography. In Proceedings of the 2001 IEEE International Conference on Acoustics, Speech, and Signal Processing, Proceedings (Cat. No.01CH37221), Salt Lake City, UT, USA, 7–11 May 2001; Volume 2, pp. 1033–1036. [Google Scholar] [CrossRef]
- Soltanian-Zadeh, H.; Rafiee-Rad, F.; Pourabdollah-Nejad, D.S. Comparison of multiwavelet, wavelet, Haralick, and shape features for microcalcification classification in mammograms. Pattern Recognit. 2004, 37, 1973–1986. [Google Scholar] [CrossRef]
- Felipe, J.C.; Ribeiro, M.X.; Sousa, E.P.; Traina, A.J.; Traina, C.J. Effective shape-based retrieval and classification of mammograms. In Proceedings of the 2006 ACM Symposium on Applied Computing, Dijon, France, 23–27 April 2006; pp. 250–255. [Google Scholar]
- Soltanian-Zadeh, H.; Pourabdollah-Nezhad, S.; Rad, F.R. Shape-based and texture-based feature extraction for classification of microcalcifications in mammograms. In Medical Imaging 2001: Image Processing; International Society for Optics and Photonics: San Diego, CA, USA, 2001; Volume 4322, pp. 301–310. [Google Scholar]
- Zyout, I.; Abdel-Qader, I.; Jacobs, C. Embedded feature selection using PSO-kNN: Shape-based diagnosis of microcalcification clusters in mammography. J. Ubiquitous Syst. Pervasive Netw. 2011, 3, 7–11. [Google Scholar] [CrossRef]
- Sahiner, B.; Chan, H.P.; Petrick, N.; Helvie, M.A.; Hadjiiski, L.M. Improvement of mammographic mass characterization using spiculation measures and morphological features. Med. Phys. 2001, 28, 1455–1465. [Google Scholar] [CrossRef]
- Junior, G.B.; da Rocha, S.V.; de Almeida, J.D.; de Paiva, A.C.; Silva, A.C.; Gattass, M. Breast cancer detection in mammography using spatial diversity, geostatistics, and concave geometry. Multimed. Tools Appl. 2019, 78, 13005–13031. [Google Scholar] [CrossRef]
- Ramos, R.P.; do Nascimento, M.Z.; Pereira, D.C. Texture extraction: An evaluation of ridgelet, wavelet and co-occurrence based methods applied to mammograms. Expert Syst. Appl. 2012, 39, 11036–11047. [Google Scholar] [CrossRef]
- Haindl, M.; Remeš, V. Pseudocolor enhancement of mammogram texture abnormalities. Mach. Vis. Appl. 2019, 30, 785–794. [Google Scholar] [CrossRef]
- Zheng, Y.; Keller, B.M.; Ray, S.; Wang, Y.; Conant, E.F.; Gee, J.C.; Kontos, D. Parenchymal texture analysis in digital mammography: A fully automated pipeline for breast cancer risk assessment. Med. Phys. 2015, 42, 4149–4160. [Google Scholar] [CrossRef] [Green Version]
- Tai, S.C.; Chen, Z.S.; Tsai, W.T. An automatic mass detection system in mammograms based on complex texture features. IEEE J. Biomed. Health Inform. 2013, 18, 618–627. [Google Scholar]
- Mudigonda, N.R.; Rangayyan, R.M.; Desautels, J.L. Detection of breast masses in mammograms by density slicing and texture flow-field analysis. IEEE Trans. Med. Imaging 2001, 20, 1215–1227. [Google Scholar] [CrossRef] [PubMed]
- Farhan, A.H.; Kamil, M.Y. Texture Analysis of Mammogram Using Local Binary Pattern Method. In Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2020; Volume 1530, p. 012091. [Google Scholar]
- Mohanty, A.K.; Senapati, M.R.; Beberta, S.; Lenka, S.K. Texture-based features for classification of mammograms using decision tree. Neural Comput. Appl. 2013, 23, 1011–1017. [Google Scholar] [CrossRef]
- Li, H.; Mukundan, R.; Boyd, S. Robust Texture Features for Breast Density Classification in Mammograms. In Proceedings of the 2020 16th IEEE International Conference on Control, Automation, Robotics and Vision (ICARCV), Shenzhen, China, 13–15 December 2020; pp. 454–459. [Google Scholar]
- Quintanilla-Domínguez, J.; Barrón-Adame, J.M.; Gordillo-Sosa, J.A.; Lozano-Garcia, J.M.; Estrada-García, H.; Guzmán-Cabrera, R. Analysis of Mammograms Using Texture Segmentation. Adv. Lang. Knowl. Eng. 2016, 119. [Google Scholar] [CrossRef]
- Hung, C.L.; Lin, C.Y. GPU-Based Texture Analysis approach for Mammograms Institute of Biomedical Informatics. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Korea, 16–19 December 2020; pp. 2183–2186. [Google Scholar]
- Biswas, S.K.; Mukherjee, D.P. Recognizing architectural distortion in mammogram: A multiscale texture modeling approach with GMM. IEEE Trans. Biomed. Eng. 2011, 58, 2023–2030. [Google Scholar] [CrossRef] [PubMed]
- Lowe, D. Object recognition from local scale-invariant features. In Proceedings of the Seventh IEEE International Conference on Computer Vision, Kerkyra, Greece, 20–27 September 1999; Volume 2, pp. 1150–1157. [Google Scholar] [CrossRef]
- Bay, H.; Tuytelaars, T.; Van Gool, L. SURF: Speeded Up Robust Features. In Computer Vision—ECCV 2006; Leonardis, A., Bischof, H., Pinz, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2006; pp. 404–417. [Google Scholar] [CrossRef]
- Li, J.; Allinson, N.M. A comprehensive review of current local features for computer vision. Neurocomputing 2008, 71, 1771–1787. [Google Scholar] [CrossRef]
- Jiang, M.; Zhang, S.; Li, H.; Metaxas, D.N. Computer-Aided Diagnosis of Mammographic Masses Using Scalable Image Retrieval. IEEE Trans. Biomed. Eng. 2015, 62, 783–792. [Google Scholar] [CrossRef]
- Guan, Q.; Zhang, J.; Chen, S.; Todd-Pokropek, A. Automatic segmentation of micro-calcification based on sift in mammograms. In Proceedings of the 2008 IEEE International Conference on BioMedical Engineering and Informatics, Sanya, China, 27–30 May 2008; Volume 2, pp. 13–17. [Google Scholar]
- Insalaco, M.; Bruno, A.; Farruggia, A.; Vitabile, S.; Ardizzone, E. An Unsupervised Method for Suspicious Regions Detection in Mammogram Images. In ICPRAM (2); SCITEPRESS Digital Library: Setúbal, Portugal, 2015; pp. 302–308. [Google Scholar]
- Utomo, A.; Juniawan, E.F.; Lioe, V.; Santika, D.D. Local Features Based Deep Learning for Mammographic Image Classification: In Comparison to CNN Models. Procedia Comput. Sci. 2021, 179, 169–176. [Google Scholar] [CrossRef]
- Salazar-Licea, L.A.; Mendoza, C.; Aceves, M.A.; Pedraza, J.C.; Pastrana-Palma, A. Automatic segmentation of mammograms using a Scale-Invariant Feature Transform and K-means clustering algorithm. In Proceedings of the 2014 11th International Conference on Electrical Engineering, Computing Science and Automatic Control (CCE), Campeche, Mexico, 29 September–3 October 2014; pp. 1–6. [Google Scholar] [CrossRef]
- Bosch, A.; Munoz, X.; Oliver, A.; Marti, J. Modeling and Classifying Breast Tissue Density in Mammograms. In Proceedings of the 2006 IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR’06), New York, NY, USA, 17–22 June 2006; Volume 2, pp. 1552–1558. [Google Scholar] [CrossRef] [Green Version]
- Liasis, G.; Pattichis, C.; Petroudi, S. Combination of different texture features for mammographic breast density classification. In Proceedings of the 2012 IEEE 12th International Conference on Bioinformatics Bioengineering (BIBE), Larnaca, Cyprus, 11–13 November 2012; pp. 732–737. [Google Scholar] [CrossRef]
- Matos, C.E.F.; Souza, J.C.; Diniz, J.O.B.; Junior, G.B.; de Paiva, A.C.; de Almeida, J.D.S.; da Rocha, S.V.; Silva, A.C. Diagnosis of breast tissue in mammography images based local feature descriptors. Multimed. Tools Appl. 2019, 78, 12961–12986. [Google Scholar] [CrossRef]
- Deshmukh, J.; Bhosle, U. SURF features based classifiers for mammogram classification. In Proceedings of the 2017 International Conference on Wireless Communications, Signal Processing and Networking (WiSPNET), Chennai, India, 22–24 March 2017; pp. 134–139. [Google Scholar] [CrossRef]
- Abudawood, T.; Al-Qunaieer, F.; Alrshoud, S. An Efficient Abnormality Classification for Mammogram Images. In Proceedings of the 2018 21st Saudi Computer Society National Computer Conference (NCC), Riyadh, Saudi Arabia, 25–26 April 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Chandakkar, P.; Ragav, V.; Li, B. Feature Extraction and Learning for Visual Data. In Feature Engineering for Machine Learning and Data Analytics; Dong, G., Liu, H., Eds.; CRC Press: Oxford, UK, 2018; Chapter 3; pp. 55–79. [Google Scholar]
- Moura, D.C.; López, M.A.G. An evaluation of image descriptors combined with clinical data for breast cancer diagnosis. Int. J. Comput. Assist. Radiol. Surg. 2013, 8, 561–574. [Google Scholar] [CrossRef]
- Pérez, N.P.; López, M.A.G.; Silva, A.; Ramos, I. Improving the Mann–Whitney statistical test for feature selection: An approach in breast cancer diagnosis on mammography. Artif. Intell. Med. 2015, 63, 19–31. [Google Scholar] [CrossRef]
- Arefan, D.; Mohamed, A.A.; Berg, W.A.; Zuley, M.L.; Sumkin, J.H.; Wu, S. Deep learning modeling using normal mammograms for predicting breast cancer risk. Med. Phys. 2020, 47, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Roth, H.R.; Lu, L.; Liu, J.; Yao, J.; Seff, A.; Cherry, K.; Kim, L.; Summers, R.M. Improving computer-aided detection using convolutional neural networks and random view aggregation. IEEE Trans. Med. Imaging 2015, 35, 1170–1181. [Google Scholar] [CrossRef] [Green Version]
- Dou, Q.; Chen, H.; Yu, L.; Zhao, L.; Qin, J.; Wang, D.; Mok, V.C.; Shi, L.; Heng, P.A. Automatic detection of cerebral microbleeds from MR images via 3D convolutional neural networks. IEEE Trans. Med. Imaging 2016, 35, 1182–1195. [Google Scholar] [CrossRef]
- Sirinukunwattana, K.; Raza, S.E.A.; Tsang, Y.W.; Snead, D.R.; Cree, I.A.; Rajpoot, N.M. Locality sensitive deep learning for detection and classification of nuclei in routine colon cancer histology images. IEEE Trans. Med. Imaging 2016, 35, 1196–1206. [Google Scholar] [CrossRef] [Green Version]
- Dhungel, N.; Carneiro, G.; Bradley, A.P. The automated learning of deep features for breast mass classification from mammograms. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2016; pp. 106–114. [Google Scholar]
- Ridhi, A.; Rai, P.K.; Balasubramanian, R. Deep feature–based automatic classification of mammograms. Med. Biol. Eng. Comput. 2020, 58, 1199–1211. [Google Scholar]
- Parisi, G.I.; Kemker, R.; Part, J.L.; Kanan, C.; Wermter, S. Continual lifelong learning with neural networks: A review. Neural Netw. 2019, 113, 54–71. [Google Scholar] [CrossRef]
- Houssein, E.H.; Emam, M.M.; Ali, A.A.; Suganthan, P.N. Deep and machine learning techniques for medical imaging-based breast cancer: A comprehensive review. Expert Syst. Appl. 2020, 114161. [Google Scholar] [CrossRef]
- Mehdy, M.; Ng, P.; Shair, E.; Saleh, N.; Gomes, C. Artificial neural networks in image processing for early detection of breast cancer. Comput. Math. Methods Med. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Giger, M.L.; Doi, K.; Vyborny, C.J.; Schmidt, R.A.; Metz, C.E. Artificial neural networks in mammography: Application to decision making in the diagnosis of breast cancer. Radiology 1993, 187, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Fogel, D.B.; Wasson, E.C., III; Boughton, E.M.; Porto, V.W. Evolving artificial neural networks for screening features from mammograms. Artif. Intell. Med. 1998, 14, 317–326. [Google Scholar] [CrossRef]
- Halkiotis, S.; Botsis, T.; Rangoussi, M. Automatic detection of clustered microcalcifications in digital mammograms using mathematical morphology and neural networks. Signal Process. 2007, 87, 1559–1568. [Google Scholar] [CrossRef]
- Ayer, T.; Chen, Q.; Burnside, E.S. Artificial neural networks in mammography interpretation and diagnostic decision making. Comput. Math. Methods Med. 2013, 2013. [Google Scholar] [CrossRef] [Green Version]
- Quintanilla-Domínguez, J.; Cortina-Januchs, M.; Jevtić, A.; Andina, D.; Barrón-Adame, J.; Vega-Corona, A. Combination of nonlinear filters and ANN for detection of microcalcifications in digitized mammography. In Proceedings of the 2009 IEEE International Conference on Systems, Man and Cybernetics, San Antonio, TX, USA, 11–14 October 2009; pp. 1516–1520. [Google Scholar]
- Papadopoulos, A.; Fotiadis, D.I.; Likas, A. Characterization of clustered microcalcifications in digitized mammograms using neural networks and support vector machines. Artif. Intell. Med. 2005, 34, 141–150. [Google Scholar] [CrossRef]
- García-Manso, A.; García-Orellana, C.J.; González-Velasco, H.; Gallardo-Caballero, R.; Macías, M.M. Consistent performance measurement of a system to detect masses in mammograms based on blind feature extraction. Biomed. Eng. Online 2013, 12, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hupse, R.; Samulski, M.; Lobbes, M.; Den Heeten, A.; Imhof-Tas, M.W.; Beijerinck, D.; Pijnappel, R.; Boetes, C.; Karssemeijer, N. Standalone computer-aided detection compared to radiologists’ performance for the detection of mammographic masses. Eur. Radiol. 2013, 23, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Qian, W.; Pu, J.; Liu, H.; Zheng, B. A new approach to develop computer-aided detection schemes of digital mammograms. Phys. Med. Biol. 2015, 60, 4413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahersia, H.; Boulehmi, H.; Hamrouni, K. Development of intelligent systems based on Bayesian regularization network and neuro-fuzzy models for mass detection in mammograms: A comparative analysis. Comput. Methods Programs Biomed. 2016, 126, 46–62. [Google Scholar] [CrossRef] [PubMed]
- Ng, H.; Ong, S.; Foong, K.; Goh, P.S.; Nowinski, W. Medical image segmentation using k-means clustering and improved watershed algorithm. In Proceedings of the 2006 IEEE Southwest Symposium on Image Analysis and Interpretation, Denver, CO, USA, 26–28 March 2006; pp. 61–65. [Google Scholar]
- Chen, C.W.; Luo, J.; Parker, K.J. Image segmentation via adaptive K-mean clustering and knowledge-based morphological operations with biomedical applications. IEEE Trans. Image Process. 1998, 7, 1673–1683. [Google Scholar] [CrossRef] [Green Version]
- Kamil, M.Y.; Salih, A.M. Mammography Images Segmentation via Fuzzy C-mean and K-mean. Int. J. Intell. Eng. Syst. 2019, 12, 22–29. [Google Scholar] [CrossRef]
- Ketabi, H.; Ekhlasi, A.; Ahmadi, H. A computer-aided approach for automatic detection of breast masses in digital mammogram via spectral clustering and support vector machine. Phys. Eng. Sci. Med. 2021, 44, 277–290. [Google Scholar] [CrossRef]
- Kumar, S.N.; Fred, A.L.; Varghese, P.S. Suspicious lesion segmentation on brain, mammograms and breast MR images using new optimized spatial feature based super-pixel fuzzy c-means clustering. J. Digit. Imaging 2019, 32, 322–335. [Google Scholar] [CrossRef]
- Chowdhary, C.L.; Acharjya, D. Segmentation of mammograms using a novel intuitionistic possibilistic fuzzy c-mean clustering algorithm. In Nature Inspired Computing; Springer: Singapore, 2018; pp. 75–82. [Google Scholar]
- Boser, B.E.; Guyon, I.M.; Vapnik, V.N. A training algorithm for optimal margin classifiers. In Proceedings of the 5th Annual ACM Workshop on Computational Learning Theory, Pittsburgh, PA, USA, 27–29 July 1992; pp. 144–152. [Google Scholar]
- Cristianini, N.; Shawe-Taylor, J. An Introduction to Support Vector Machines and OTHER Kernel-Based Learning Methods; Cambridge University Press: Cambridge, UK, 2000. [Google Scholar]
- Ak, M.F. A comparative analysis of breast cancer detection and diagnosis using data visualization and machine learning applications. Healthcare 2020, 8, 111. [Google Scholar] [CrossRef]
- Tharwat, A.; Hassanien, A.E.; Elnaghi, B.E. A BA-based algorithm for parameter optimization of support vector machine. Pattern Recognit. Lett. 2017, 93, 13–22. [Google Scholar] [CrossRef]
- Liu, X.; Mei, M.; Liu, J.; Hu, W. Microcalcification detection in full-field digital mammograms with PFCM clustering and weighted SVM-based method. EURASIP J. Adv. Signal Process. 2015, 2015, 1–13. [Google Scholar] [CrossRef] [Green Version]
- de Nazaré Silva, J.; de Carvalho Filho, A.O.; Silva, A.C.; De Paiva, A.C.; Gattass, M. Automatic detection of masses in mammograms using quality threshold clustering, correlogram function, and SVM. J. Digit. Imaging 2015, 28, 323–337. [Google Scholar] [CrossRef] [Green Version]
- Ancy, C.; Nair, L.S. An efficient CAD for detection of tumour in mammograms using SVM. In Proceedings of the 2017 IEEE International Conference on Communication and Signal Processing (ICCSP), Chennai, India, 6–8 April 2017; pp. 1431–1435. [Google Scholar]
- Qayyum, A.; Basit, A. Automatic breast segmentation and cancer detection via SVM in mammograms. In Proceedings of the 2016 IEEE International Conference on Emerging Technologies (ICET), Islamabad, Pakistan, 18–19 October 2016; pp. 1–6. [Google Scholar]
- Sharma, S.; Khanna, P. Computer-aided diagnosis of malignant mammograms using Zernike moments and SVM. J. Digit. Imaging 2015, 28, 77–90. [Google Scholar] [CrossRef]
- Vijayarajeswari, R.; Parthasarathy, P.; Vivekanandan, S.; Basha, A.A. Classification of mammogram for early detection of breast cancer using SVM classifier and Hough transform. Measurement 2019, 146, 800–805. [Google Scholar] [CrossRef]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar]
- Lee, J.; Nishikawa, R.M. Automated mammographic breast density estimation using a fully convolutional network. Med. Phys. 2018, 45, 1178–1190. [Google Scholar] [CrossRef]
- Xu, S.; Adeli, E.; Cheng, J.Z.; Xiang, L.; Li, Y.; Lee, S.W.; Shen, D. Mammographic mass segmentation using multichannel and multiscale fully convolutional networks. Int. J. Imaging Syst. Technol. 2020, 30, 1095–1107. [Google Scholar] [CrossRef]
- Hai, J.; Qiao, K.; Chen, J.; Tan, H.; Xu, J.; Zeng, L.; Shi, D.; Yan, B. Fully convolutional densenet with multiscale context for automated breast tumor segmentation. J. Healthc. Eng. 2019, 2019. [Google Scholar] [CrossRef] [Green Version]
- Sathyan, A.; Martis, D.; Cohen, K. Mass and Calcification Detection from Digital Mammograms Using UNets. In Proceedings of the 2020 7th IEEE International Conference on Soft Computing & Machine Intelligence (ISCMI), Stockholm, Sweden, 14–15 November 2020; pp. 229–232. [Google Scholar]
- Li, S.; Dong, M.; Du, G.; Mu, X. Attention dense-u-net for automatic breast mass segmentation in digital mammogram. IEEE Access 2019, 7, 59037–59047. [Google Scholar] [CrossRef]
- AlGhamdi, M.; Abdel-Mottaleb, M.; Collado-Mesa, F. Du-net: Convolutional network for the detection of arterial calcifications in mammograms. IEEE Trans. Med. Imaging 2020, 39, 3240–3249. [Google Scholar] [CrossRef]
- Xiao, H.; Wang, Q.; Liu, Z.; Huang, J.; Zhou, Y.; Zhou, Y.; Xu, W. CSABlock-based Cascade RCNN for Breast Mass Detection in Mammogram. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Korea, 16–19 December 2020; pp. 2120–2124. [Google Scholar]
- Zhang, L.; Li, Y.; Chen, H.; Cheng, L. Mammographic Mass Detection by Bilateral Analysis Based on Convolution Neural Network. In Proceedings of the 2019 IEEE International Conference on Image Processing (ICIP), Taipei, Taiwan, 22–25 September 2019; pp. 784–788. [Google Scholar]
- Agarwal, R.; Díaz, O.; Yap, M.H.; Lladó, X.; Martí, R. Deep learning for mass detection in Full Field Digital Mammograms. Comput. Biol. Med. 2020, 121, 103774. [Google Scholar] [CrossRef]
- Ben-Ari, R.; Akselrod-Ballin, A.; Karlinsky, L.; Hashoul, S. Domain specific convolutional neural nets for detection of architectural distortion in mammograms. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 552–556. [Google Scholar]
- Zhang, Z.; Wang, Y.; Zhang, J.; Mu, X. Comparison of multiple feature extractors on Faster RCNN for breast tumor detection. In Proceedings of the 2019 8th IEEE International Symposium on Next Generation Electronics (ISNE), Zhengzhou, China, 9–10 October 2019; pp. 1–4. [Google Scholar]
- Bhatti, H.M.A.; Li, J.; Siddeeq, S.; Rehman, A.; Manzoor, A. Multi-detection and Segmentation of Breast Lesions Based on Mask RCNN-FPN. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, Korea, 16–19 December 2020; pp. 2698–2704. [Google Scholar]
- Fan, M.; Li, Y.; Zheng, S.; Peng, W.; Tang, W.; Li, L. Computer-aided detection of mass in digital breast tomosynthesis using a faster region-based convolutional neural network. Methods 2019, 166, 103–111. [Google Scholar] [CrossRef]
- Ribli, D.; Horváth, A.; Unger, Z.; Pollner, P.; Csabai, I. Detecting and classifying lesions in mammograms with deep learning. Sci. Rep. 2018, 8, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Wu, E.; Wu, K.; Cox, D.; Lotter, W. Conditional infilling GANs for data augmentation in mammogram classification. In Image Analysis for Moving Organ, Breast, and Thoracic Images; Springer: Berlin/Heidelberg, Germany, 2018; pp. 98–106. [Google Scholar]
- Wu, E.; Wu, K.; Lotter, W. Synthesizing lesions using contextual GANs improves breast cancer classification on mammograms. arXiv 2020, arXiv:2006.00086. [Google Scholar]
- Shen, T.; Hao, K.; Gou, C.; Wang, F.Y. Mass Image Synthesis in Mammogram with Contextual Information Based on GANs. Comput. Methods Programs Biomed. 2021, 106019. [Google Scholar] [CrossRef]
- Becker, A.S.; Jendele, L.; Skopek, O.; Berger, N.; Ghafoor, S.; Marcon, M.; Konukoglu, E. Injecting and removing malignant features in mammography with CycleGAN: Investigation of an automated adversarial attack using neural networks. arXiv 2018, arXiv:1811.07767. [Google Scholar]
- Korkinof, D.; Rijken, T.; O’Neill, M.; Yearsley, J.; Harvey, H.; Glocker, B. High-resolution mammogram synthesis using progressive generative adversarial networks. arXiv 2018, arXiv:1807.03401. [Google Scholar]
- Kallenberg, M.; Petersen, K.; Nielsen, M.; Ng, A.Y.; Diao, P.; Igel, C.; Vachon, C.M.; Holland, K.; Winkel, R.R.; Karssemeijer, N.; et al. Unsupervised deep learning applied to breast density segmentation and mammographic risk scoring. IEEE Trans. Med. Imaging 2016, 35, 1322–1331. [Google Scholar] [CrossRef]
- Yang, D.; Wang, Y.; Jiao, Z. Asymmetry Analysis with sparse autoencoder in mammography. In Proceedings of the International Conference on Internet Multimedia Computing and Service, Xi’an, China, 19–21 August 2016; pp. 287–291. [Google Scholar]
- Petersen, K.; Chernoff, K.; Nielsen, M.; Ng, A.Y. Breast density scoring with multiscale denoising autoencoders. In Proceedings of the STMI Workshop at 15th Int. Conf. Medical Image Computing and Computer Assisted Intervention (MICCAI), Nice, Italy, 5 October 2012. [Google Scholar]
- Selvathi, D.; Poornila, A.A. Breast cancer detection in mammogram images using deep learning technique. Middle-East J. Sci. Res. 2017, 25, 417–426. [Google Scholar]
- Selvathi, D.; AarthyPoornila, A. Performance analysis of various classifiers on deep learning network for breast cancer detection. In Proceedings of the 2017 IEEE International Conference on Signal Processing and Communication (ICSPC), Coimbatore, India, 28–29 July 2017; pp. 359–363. [Google Scholar]
- Taghanaki, S.A.; Kawahara, J.; Miles, B.; Hamarneh, G. Pareto-optimal multi-objective dimensionality reduction deep auto-encoder for mammography classification. Comput. Methods Programs Biomed. 2017, 145, 85–93. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Girshick, R.; Donahue, J.; Darrell, T.; Malik, J. Rich feature hierarchies for accurate object detection and semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 580–587. [Google Scholar]
- Girshick, R. Fast r-cnn. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 7–13 December 2015; pp. 1440–1448. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster r-cnn: Towards real-time object detection with region proposal networks. arXiv 2015, arXiv:1506.01497. [Google Scholar] [CrossRef] [Green Version]
- Russell, S.J.; Norvig, P. Artificial Intelligence: A Modern Approach, 4th ed.; Alan Apt: Madrid, Spain, 2020. [Google Scholar]
- Samala, R.K.; Chan, H.P.; Hadjiiski, L.M.; Helvie, M.A.; Cha, K.H.; Richter, C.D. Multi-task transfer learning deep convolutional neural network: Application to computer-aided diagnosis of breast cancer on mammograms. Phys. Med. Biol. 2017, 62, 8894. [Google Scholar] [CrossRef]
- Murtaza, G.; Shuib, L.; Wahab, A.W.A.; Mujtaba, G.; Nweke, H.F.; Al-garadi, M.A.; Zulfiqar, F.; Raza, G.; Azmi, N.A. Deep learning-based breast cancer classification through medical imaging modalities: State of the art and research challenges. Artif. Intell. Rev. 2020, 53, 1655–1720. [Google Scholar] [CrossRef]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. Adv. Neural Inf. Process. Syst. 2014, 27. [Google Scholar]
- Ratner, A.J.; Ehrenberg, H.R.; Hussain, Z.; Dunnmon, J.; Ré, C. Learning to compose domain-specific transformations for data augmentation. Adv. Neural Inf. Process. Syst. 2017, 30, 3239. [Google Scholar]
- Hussain, Z.; Gimenez, F.; Yi, D.; Rubin, D. Differential data augmentation techniques for medical imaging classification tasks. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Bethesda, MD, USA, 2017; Volume 2017, p. 979. [Google Scholar]
- Radford, A.; Metz, L.; Chintala, S. Unsupervised representation learning with deep convolutional generative adversarial networks. arXiv 2015, arXiv:1511.06434. [Google Scholar]
- Singh, V.K.; Romani, S.; Rashwan, H.A.; Akram, F.; Pandey, N.; Sarker, M.M.K.; Abdulwahab, S.; Torrents-Barrena, J.; Saleh, A.; Arquez, M.; et al. Conditional generative adversarial and convolutional networks for X-ray breast mass segmentation and shape classification. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 833–840. [Google Scholar]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oza, P.; Sharma, P.; Patel, S.; Bruno, A. A Bottom-Up Review of Image Analysis Methods for Suspicious Region Detection in Mammograms. J. Imaging 2021, 7, 190. https://doi.org/10.3390/jimaging7090190
Oza P, Sharma P, Patel S, Bruno A. A Bottom-Up Review of Image Analysis Methods for Suspicious Region Detection in Mammograms. Journal of Imaging. 2021; 7(9):190. https://doi.org/10.3390/jimaging7090190
Chicago/Turabian StyleOza, Parita, Paawan Sharma, Samir Patel, and Alessandro Bruno. 2021. "A Bottom-Up Review of Image Analysis Methods for Suspicious Region Detection in Mammograms" Journal of Imaging 7, no. 9: 190. https://doi.org/10.3390/jimaging7090190
APA StyleOza, P., Sharma, P., Patel, S., & Bruno, A. (2021). A Bottom-Up Review of Image Analysis Methods for Suspicious Region Detection in Mammograms. Journal of Imaging, 7(9), 190. https://doi.org/10.3390/jimaging7090190