




Using an Ultrasound Tissue Phantom Model for Hybrid Training of Deep Learning Models for Shrapnel Detection


Abstract
:1. Introduction
2. Materials and Methods
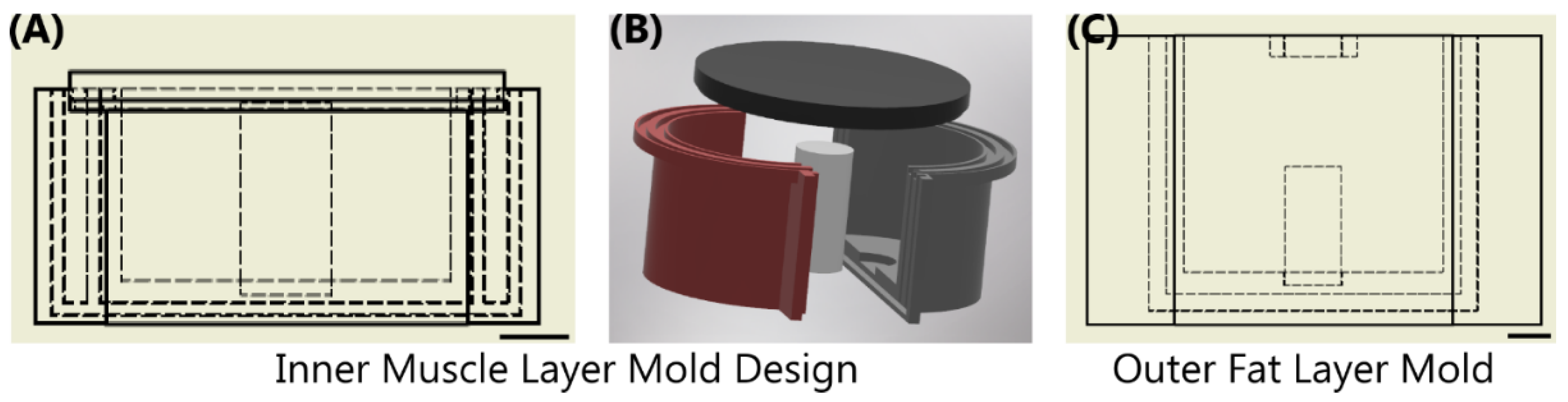
2.1. Fabrication of a Tissue Phantom Mold
2.2. Tissue Phantom Construction Using Gelatin
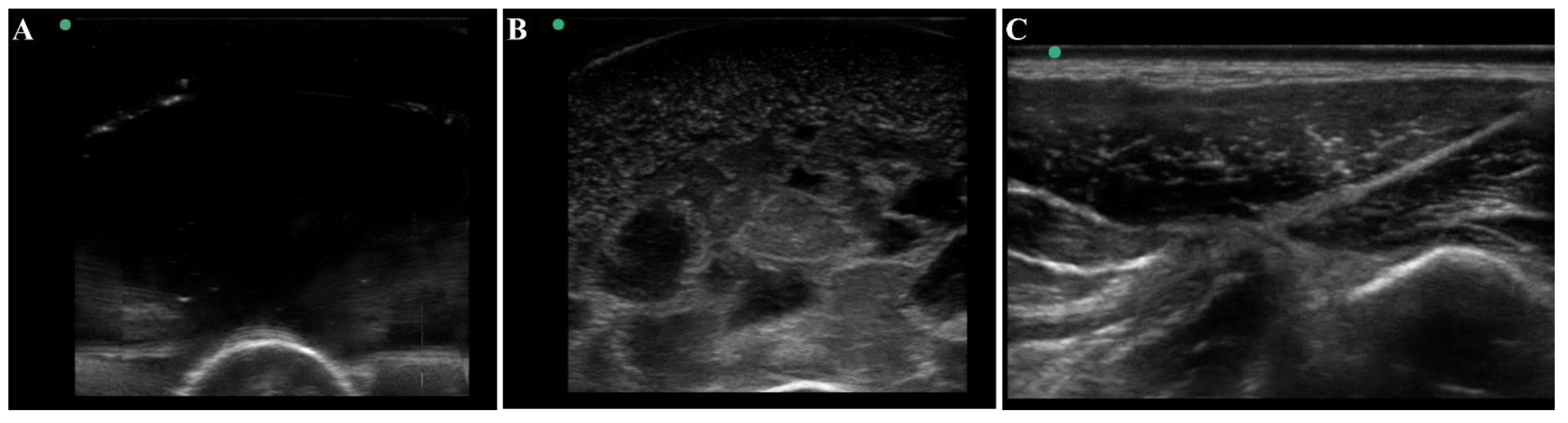
2.3. Ultrasound Shrapnel Imaging
2.4. Training Image Classification Algorithms for Shrapnel Detection
3. Results
3.1. Overview of the Tissue Phantom for Shrapnel Image Acquisition
3.2. Application for Automated Shrapnel Detection
3.3. Phantom and Swine Training Datasets for ShrapML
3.4. Ratio Comparison ShrapML vs. MobileNetv2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American College of Emergency Physicians Council. Resolution on Ultrasound. ACEP News 1990, 9, 1–15. [Google Scholar]
- Harper, H.; Myers, M. Military and Tactical Ultrasound. In Emergency Ultrasound; ACEP: Irving, TX, USA, 2008. [Google Scholar]
- Heegaard, W.G.; Walcher, F.; Brenner, F.; dell’Orto, M.C.; Kirschning, T.; Marzi, I.; Breitkreutz, R.; Zechner, P.M.; Aichinger, G.; Wildner, G.; et al. Chapter 4. Ultrasound in Prehospital and Austere Environments. In Ma and Mateer’s Emergency Ultrasound; Ma, O.J., Mateer, J.R., Reardon, R.F., Joing, S.A., Eds.; The McGraw-Hill Companies: New York, NY, USA, 2014. [Google Scholar]
- Russell, T.C.; Crawford, P.F. Ultrasound in the Austere Environment: A Review of the History, Indications, and Specifications. Mil. Med. 2013, 178, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zieleskiewicz, L.; Fresco, R.; Duclos, G.; Antonini, F.; Mathieu, C.; Medam, S.; Vigne, C.; Poirier, M.; Roche, P.-H.; Bouzat, P.; et al. Integrating Extended Focused Assessment with Sonography for Trauma (EFAST) in the Initial Assessment of Severe Trauma: Impact on the Management of 756 Patients. Injury 2018, 49, 1774–1780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakraborty, S.; Murali, B.; Mitra, A.K. An Efficient Deep Learning Model to Detect COVID-19 Using Chest X-ray Images. Int. J. Environ. Res. Public Health 2022, 19, 2013. [Google Scholar] [CrossRef]
- Guefrechi, S.; Jabra, M.B.; Ammar, A.; Koubaa, A.; Hamam, H. Deep Learning Based Detection of COVID-19 from Chest X-ray Images. Multimed. Tools Appl. 2021, 80, 31803–31820. [Google Scholar] [CrossRef]
- Keidar, D.; Yaron, D.; Goldstein, E.; Shachar, Y.; Blass, A.; Charbinsky, L.; Aharony, I.; Lifshitz, L.; Lumelsky, D.; Neeman, Z.; et al. COVID-19 Classification of X-ray Images Using Deep Neural Networks. Eur. Radiol. 2021, 31, 9654–9663. [Google Scholar] [CrossRef]
- Akkus, Z.; Galimzianova, A.; Hoogi, A.; Rubin, D.L.; Erickson, B.J. Deep Learning for Brain MRI Segmentation: State of the Art and Future Directions. J. Digit. Imaging 2017, 30, 449–459. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Zhang, J.; Liu, Q.; Wang, Y. Multimodal MRI-Based Classification of Migraine: Using Deep Learning Convolutional Neural Network. BioMed. Eng. OnLine 2018, 17, 138. [Google Scholar] [CrossRef] [Green Version]
- Noor, M.B.T.; Zenia, N.Z.; Kaiser, M.S.; Mamun, S.A.; Mahmud, M. Application of Deep Learning in Detecting Neurological Disorders from Magnetic Resonance Images: A Survey on the Detection of Alzheimer’s Disease, Parkinson’s Disease and Schizophrenia. Brain Inf. 2020, 7, 11. [Google Scholar] [CrossRef]
- Riquelme, D.; Akhloufi, M. Deep Learning for Lung Cancer Nodules Detection and Classification in CT Scans. AI 2020, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Xiao, J.; He, L.; Peng, X.; Yuan, X. The Tumor Target Segmentation of Nasopharyngeal Cancer in CT Images Based on Deep Learning Methods. Technol. Cancer Res. Treat. 2019, 18, 153303381988456. [Google Scholar] [CrossRef] [PubMed]
- Lakshmanaprabu, S.K.; Mohanty, S.N.; Shankar, K.; Arunkumar, N.; Ramirez, G. Optimal Deep Learning Model for Classification of Lung Cancer on CT Images. Future Gener. Comput. Syst. 2019, 92, 374–382. [Google Scholar] [CrossRef]
- Santosh, K.C.; Dhar, M.K.; Rajbhandari, R.; Neupane, A. Deep Neural Network for Foreign Object Detection in Chest X-rays. In Proceedings of the 2020 IEEE 33rd International Symposium on Computer-Based Medical Systems (CBMS), Rochester, MN, USA, 28–30 July 2020; IEEE: Pistacaway, NJ, USA, 2020; pp. 538–541. [Google Scholar]
- Deshpande, H.; Harder, T.; Saalbach, A.; Sawarkar, A.; Buelow, T. Detection of Foreign Objects in Chest Radiographs Using Deep Learning. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging Workshops (ISBI Workshops), Iowa City, IA, USA, 3–7 April 2020; IEEE: Pistacaway, NJ, USA, 2020; pp. 1–4. [Google Scholar]
- Liu, S.; Wang, Y.; Yang, X.; Lei, B.; Liu, L.; Li, S.X.; Ni, D.; Wang, T. Deep Learning in Medical Ultrasound Analysis: A Review. Engineering 2019, 5, 261–275. [Google Scholar] [CrossRef]
- Diaz-Escobar, J.; Ordóñez-Guillén, N.E.; Villarreal-Reyes, S.; Galaviz-Mosqueda, A.; Kober, V.; Rivera-Rodriguez, R.; Rizk, J.E.L. Deep-Learning Based Detection of COVID-19 Using Lung Ultrasound Imagery. PLoS ONE 2021, 16, e0255886. [Google Scholar] [CrossRef] [PubMed]
- Willemink, M.J.; Koszek, W.A.; Hardell, C.; Wu, J.; Fleischmann, D.; Harvey, H.; Folio, L.R.; Summers, R.M.; Rubin, D.L.; Lungren, M.P. Preparing Medical Imaging Data for Machine Learning. Radiology 2020, 295, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Culjat, M.O.; Goldenberg, D.; Tewari, P.; Singh, R.S. A Review of Tissue Substitutes for Ultrasound Imaging. Ultrasound Med. Biol. 2010, 36, 861–873. [Google Scholar] [CrossRef]
- McGarry, C.K.; Grattan, L.J.; Ivory, A.M.; Leek, F.; Liney, G.P.; Liu, Y.; Miloro, P.; Rai, R.; Robinson, A.P.; Shih, A.J. Tissue Mimicking Materials for Imaging and Therapy Phantoms: A Review. Phys. Med. Biol. 2020, 65, 23TR01. [Google Scholar] [CrossRef]
- Cao, Y.; Li, G.-Y.; Zhang, X.; Liu, Y.-L. Tissue-Mimicking Materials for Elastography Phantoms: A Review. Extrem. Mech. Lett. 2017, 17, 62–70. [Google Scholar] [CrossRef]
- Alves, N.; Kim, A.; Tan, J.; Hwang, G.; Javed, T.; Neagu, B.; Courtney, B.K. Cardiac Tissue-Mimicking Ballistic Gel Phantom for Ultrasound Imaging in Clinical and Research Applications. Ultrasound Med. Biol. 2020, 46, 2057–2069. [Google Scholar] [CrossRef]
- Anugrah, M.A.; Suryani, S.; Ilyas, S.; Mutmainna, I.; Fahri, A.N.; Jusmawang; Tahir, D. Composite Gelatin/Rhizophora SPP Particleboards/PVA for Soft Tissue Phantom Applications. Radiat. Phys. Chem. 2020, 173, 108878. [Google Scholar] [CrossRef]
- Yoon, K.-C.; Kim, K.G. Manufacturing of a Gelatin Phantom with Lymphedema for Ultrasonic Imaging Measurement. J. Eng. Sci. Med. Diagn. Ther. 2021, 4, 044502. [Google Scholar] [CrossRef]
- Amidi, E.; Yang, G.; Uddin, K.M.S.; Wahidi, R.; Zhu, Q. Low-Cost Ultrasound and Optical Gelatin-Based Phantoms. Photons Plus Ultrasound Imaging Sens. 2019, 10878, 330–336. [Google Scholar]
- Dahal, E.; Badal, A.; Zidan, A.; Alayoubi, A.; Hagio, T.; Glick, S.; Badano, A.; Ghammraoui, B. Stable Gelatin-Based Phantom Materials with Tunable X-ray Attenuation Properties and 3D Printability for X-ray Imaging. Phys. Med. Biol. 2018, 63, 09NT01. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, M.; Özdemir, G.; Eroğul, O. Investigating Ballistic Gelatin Based Phantom Properties for Ultrasound Training. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering 2018, Prague, Czech Republic, 3–8 June 2018; Lhotska, L., Sukupova, L., Lacković, I., Ibbott, G.S., Eds.; Springer: Singapore, 2019; pp. 789–793. [Google Scholar]
- Anderson, T. Small Rodent Cardiac Phantom for Preclinical Ultrasound Imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2017, 64, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hocking, G.; Hebard, S.; Mitchell, C.H. A Review of the Benefits and Pitfalls of Phantoms in Ultrasound-Guided Regional Anesthesia. Reg. Anesth. Pain. Med. 2011, 36, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Snider, E.J.; Hernandez-Torres, S.I.; Boice, E.N. An Image Classification Deep-Learning Algorithm for Shrapnel Detection from Ultrasound Images. Sci. Rep. 2022, 12, 8427. [Google Scholar] [CrossRef]
- Niimi, R.; Kono, T.; Nishihara, A.; Hasegawa, M.; Matsumine, A.; Kono, T.; Sudo, A. Cortical Thickness of the Femur and Long-Term Bisphosphonate Use. J. Bone Miner. Res. 2015, 30, 225–231. [Google Scholar] [CrossRef]
- Femur—OrthopaedicsOne Review—OrthopaedicsOne. Available online: https://www.orthopaedicsone.com/display/Review/Femur (accessed on 17 December 2021).
- Schindelin, J.; Rueden, C.T.; Hiner, M.C.; Eliceiri, K.W. The ImageJ Ecosystem: An Open Platform for Biomedical Image Analysis. Mol. Reprod. Dev. 2015, 82, 518–529. [Google Scholar] [CrossRef] [Green Version]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An Open-Source Platform for Biological-Image Analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Boice, E.N.; Hernandez-Torres, S.I.; Snider, E.J. Comparison of Ultrasound Image Classifier Deep Learning Algorithms for Shrapnel Detection. J. Imaging 2022, 8, 140. [Google Scholar] [CrossRef]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.-C. MobileNetV2: Inverted Residuals and Linear Bottlenecks. arXiv 2018, arXiv:1801.04381. [Google Scholar] [CrossRef]
- Snider, E.J.; Hernandez-Torres, S.I.; Avital, G.; Boice, E.N. Evaluation of an Object Detection Algorithm for Shrapnel and Development of a Triage Tool to Determine Injury Severity. J. Imaging 2022, 8, 252. [Google Scholar] [CrossRef] [PubMed]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You Only Look Once: Unified, Real-Time Object Detection. In Proceedings of the Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; IEEE: Pistacaway, NJ, USA, 2016; pp. 779–788. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-Cnn: Towards Real-Time Object Detection with Region Proposal Networks. In Advances in Neural Information Processing Systems; Neural Information Processing Systems Foundation, Inc.: San Diego, CA, USA, 2015; Volume 28. [Google Scholar]
- Flax, S.W.; Pelc, N.J.; Glover, G.H.; Gutmann, F.D.; McLachlan, M. Spectral Characterization and Attenuation Measurements in Ultrasound. Ultrason. Imaging 1983, 5, 95–116. [Google Scholar] [CrossRef]
- Patterson, B.; Miller, D.L. Experimental Measurements of Ultrasound Attenuation in Human Chest Wall and Assessment of the Mechanical Index for Lung Ultrasound. Ultrasound Med. Biol. 2020, 46, 1442–1454. [Google Scholar] [CrossRef] [PubMed]
- Treeby, B.E.; Zhang, E.Z.; Thomas, A.S.; Cox, B.T. Measurement of the Ultrasound Attenuation and Dispersion in Whole Human Blood and Its Components From 0–70 MHz. Ultrasound Med. Biol. 2011, 37, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.J.; Einhorn, T.A. Perspectives: Ultrasound Assessment of Bone. J. Bone Miner. Res. 1993, 8, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Boice, E.N.; Hernandez-Torres, S.I.; Knowlton, Z.J.; Berard, D.; Gonzalez, J.M.; Snider, E.J. Training Ultrasound Image Classification Deep-Learning Algorithms for Pneumothorax Detection Using a Synthetic Tissue Phantom. J. Imaging 2022, 8, 249. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter. | Value |
|---|---|
| Total # of trainable parameters | 17.17 million |
| Number of Sparsely Connected CNN Layers | 5 CNN Layers |
| Filters in Each CNN Layer | 16/32/64/128/256 |
| Number of Fully Connected Layers | 1 |
| Filters in Fully Connected Layer | 256 |
| Dropout Rate | 55% |
| Training Optimizer | RMSprop |
| Number of Epochs | 100 |
| Learning Rate | 0.001 |
| Batch Size | 32 |
| 1:0 Image Ratio (0% Phantom) | 1:1 Image Ratio (50% Phantom) | 1:3 Image Ratio (75% Phantom) | 1:9 Image Ratio (90% Phantom) | 0:1 Image Ratio (100% Phantom)) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Shrapnel | Baseline | Shrapnel | Baseline | Shrapnel | Baseline | Shrapnel | Baseline | Shrapnel | |
| Total | 443 | 467 | 428 | 480 | 422 | 486 | 418 | 490 | 415 | 493 |
| Swine | 443 | 467 | 221 | 234 | 111 | 117 | 45 | 47 | 0 | 0 |
| Phantom | 0 | 0 | 207 | 246 | 311 | 369 | 373 | 443 | 415 | 493 |
| Swine to Phantom Training Image Ratio for ShrapML Algorithm | |||||
|---|---|---|---|---|---|
| 1:0 (Swine Only) | 1:1 | 1:3 | 1:9 | 0:1 (Phantom Only) | |
| Accuracy | 0.990 | 0.950 | 0.960 | 0.870 | 0.610 |
| AUC | 0.990 | 0.990 | 0.990 | 0.970 | 0.620 |
| Precision | 0.990 | 0.930 | 0.970 | 0.870 | 0.690 |
| Recall | 0.990 | 0.990 | 0.950 | 0.910 | 0.520 |
| Specificity | 0.980 | 0.910 | 0.970 | 0.840 | 0.710 |
| F1 | 0.990 | 0.960 | 0.960 | 0.880 | 0.580 |
| Swine to Phantom Training Image Ratio for MobileNetv2 | |||||
|---|---|---|---|---|---|
| 1:0 (Swine Only) | 1:1 | 1:3 | 1:9 | 0:1 (Phantom Only) | |
| Accuracy | 0.982 | 0.991 | 0.908 | 0.693 | 0.509 |
| AUC | 1.000 | 0.998 | 0.987 | 0.871 | 0.499 |
| Precision | 0.964 | 0.982 | 0.829 | 0.414 | 0.901 |
| Recall | 1.000 | 1.000 | 0.979 | 0.902 | 0.498 |
| Specificity | 0.967 | 0.983 | 0.858 | 0.633 | 0.593 |
| F1 | 0.982 | 0.991 | 0.898 | 0.568 | 0.641 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernandez-Torres, S.I.; Boice, E.N.; Snider, E.J. Using an Ultrasound Tissue Phantom Model for Hybrid Training of Deep Learning Models for Shrapnel Detection. J. Imaging 2022, 8, 270. https://doi.org/10.3390/jimaging8100270
Hernandez-Torres SI, Boice EN, Snider EJ. Using an Ultrasound Tissue Phantom Model for Hybrid Training of Deep Learning Models for Shrapnel Detection. Journal of Imaging. 2022; 8(10):270. https://doi.org/10.3390/jimaging8100270
Chicago/Turabian StyleHernandez-Torres, Sofia I., Emily N. Boice, and Eric J. Snider. 2022. "Using an Ultrasound Tissue Phantom Model for Hybrid Training of Deep Learning Models for Shrapnel Detection" Journal of Imaging 8, no. 10: 270. https://doi.org/10.3390/jimaging8100270
APA StyleHernandez-Torres, S. I., Boice, E. N., & Snider, E. J. (2022). Using an Ultrasound Tissue Phantom Model for Hybrid Training of Deep Learning Models for Shrapnel Detection. Journal of Imaging, 8(10), 270. https://doi.org/10.3390/jimaging8100270