
Dental MRI of Oral Soft-Tissue Tumors—Optimized Use of Black Bone MRI Sequences and a 15-Channel Mandibular Coil

 ,
,
Abstract
:1. Introduction
2. Material and Methods
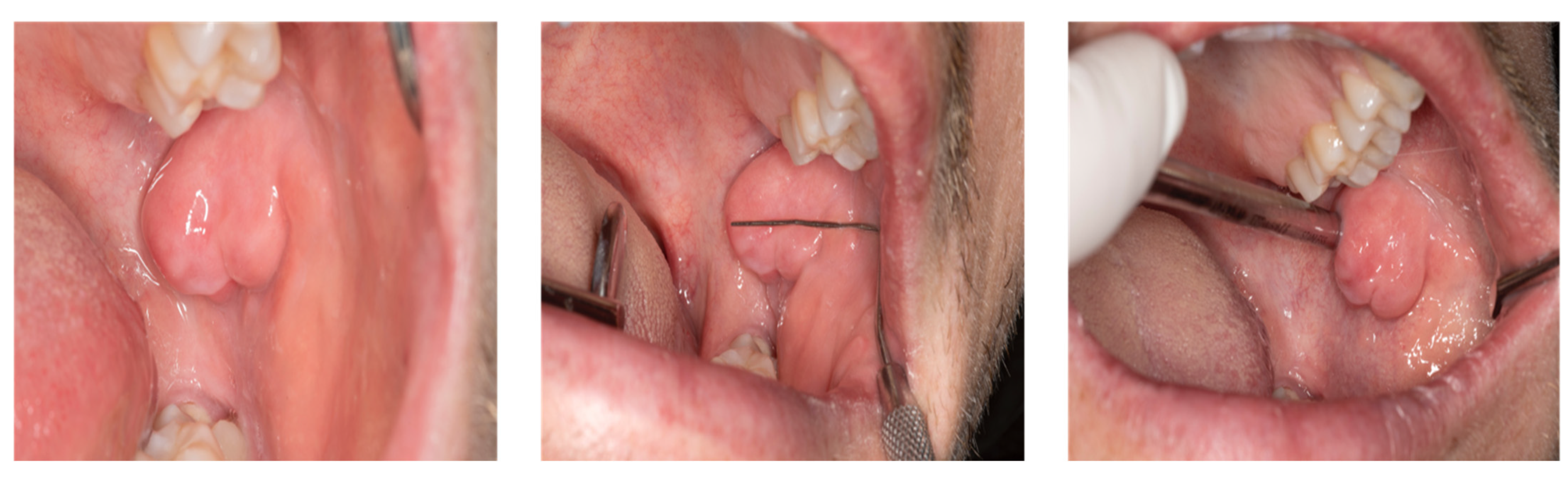
2.1. Case Presentation
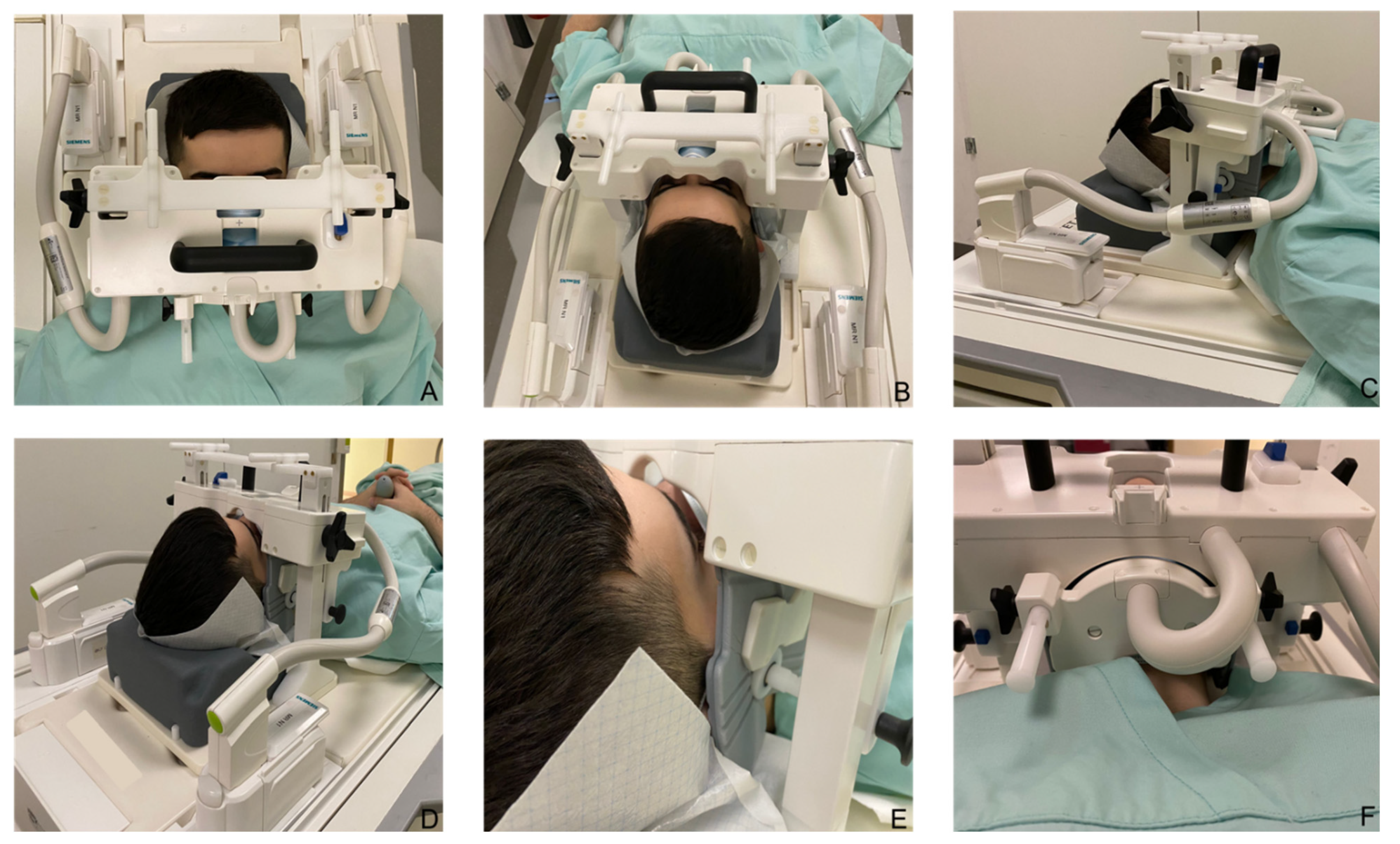
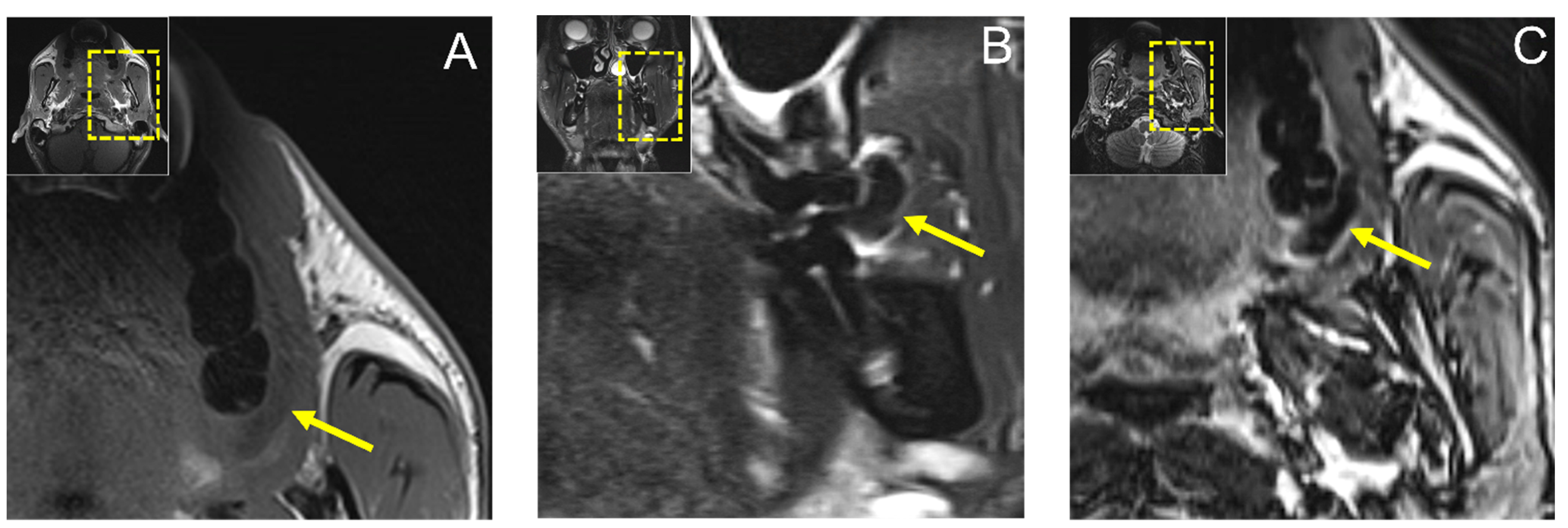
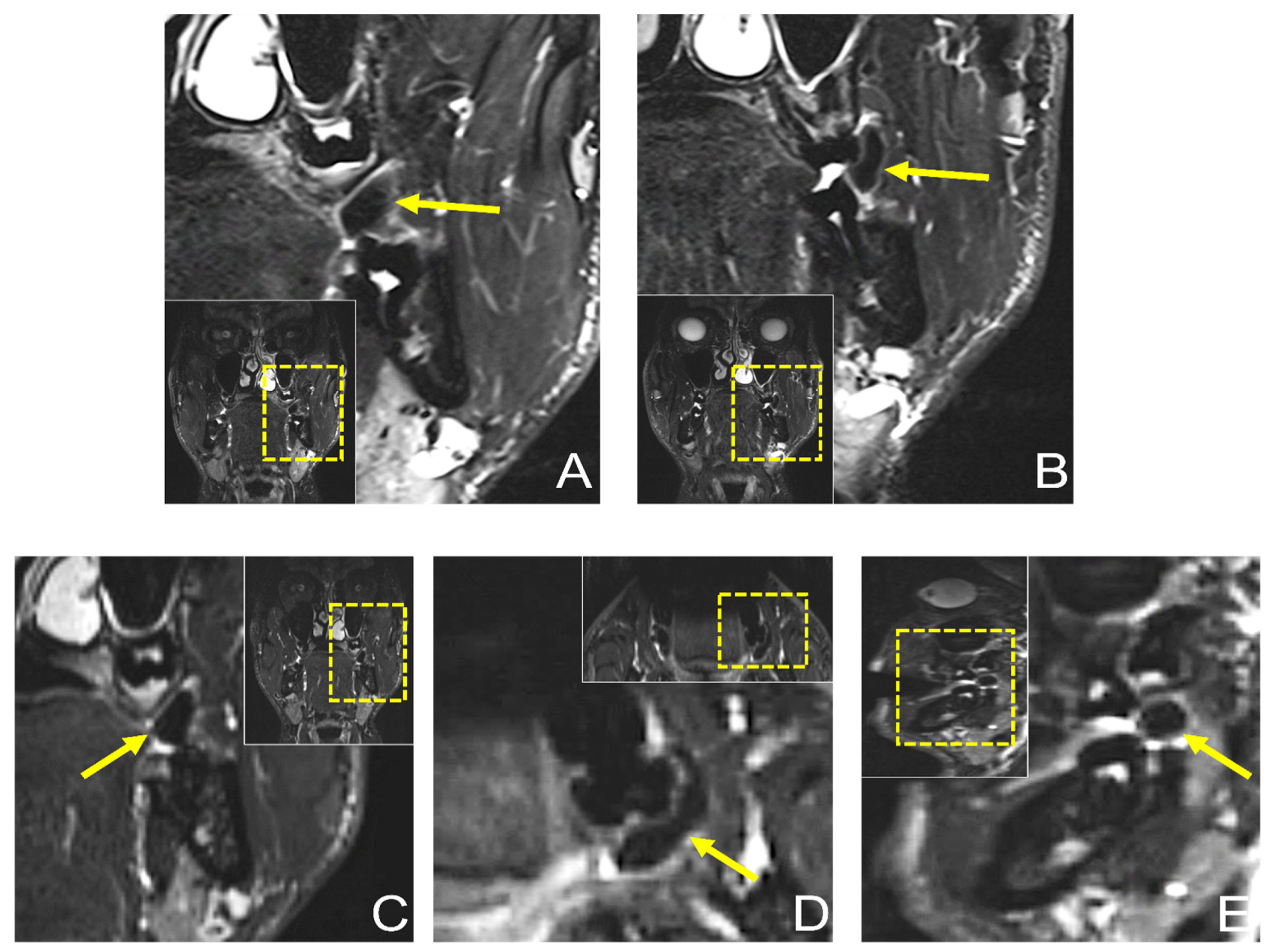
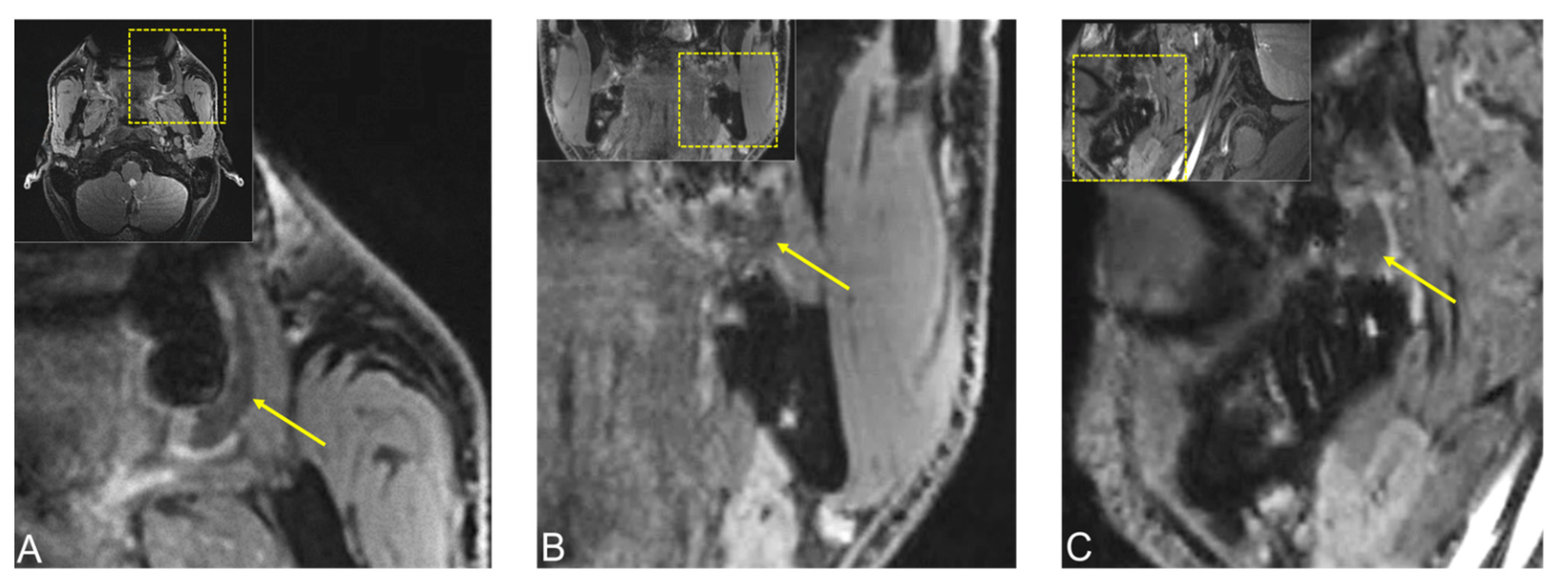
2.2. Dental Magnetic Resonance Imaging—Data Acquisition
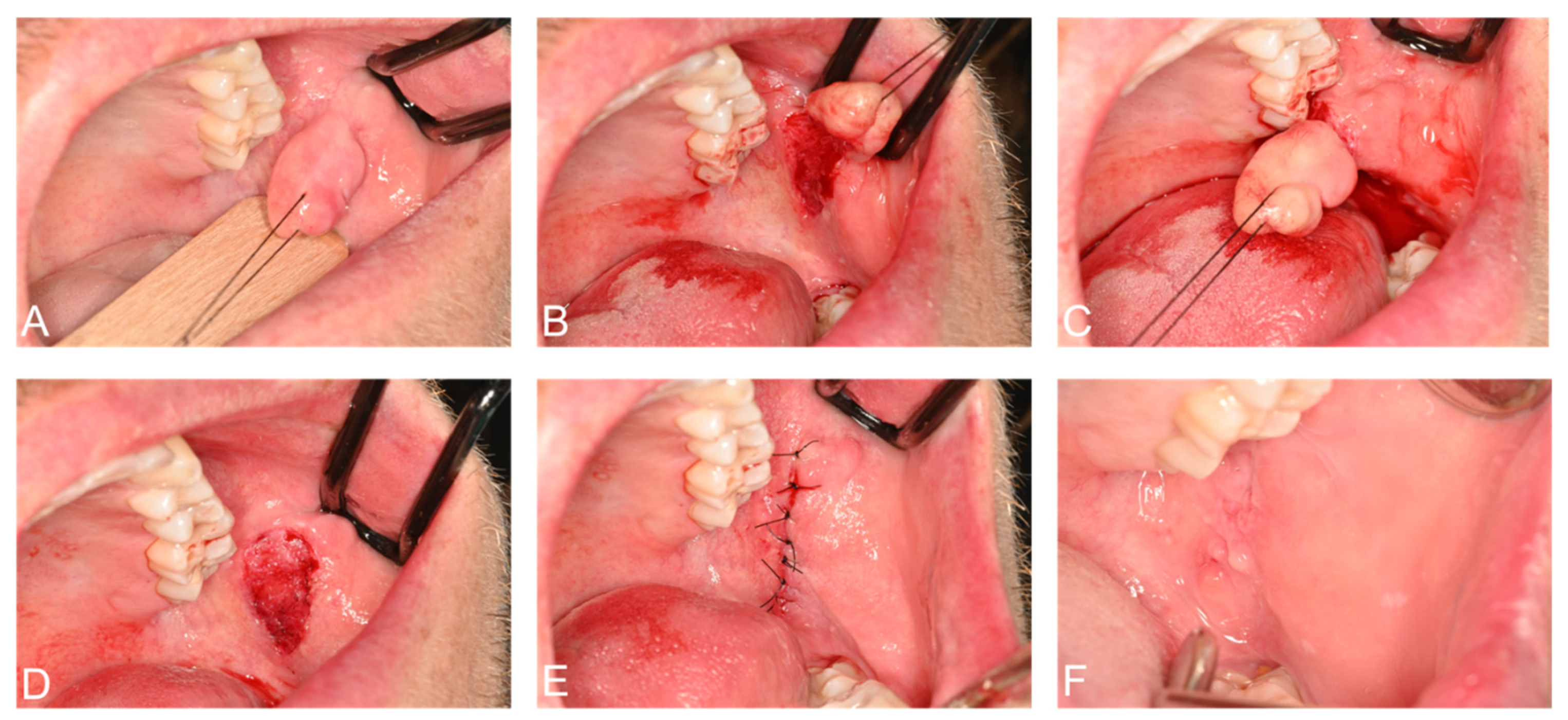
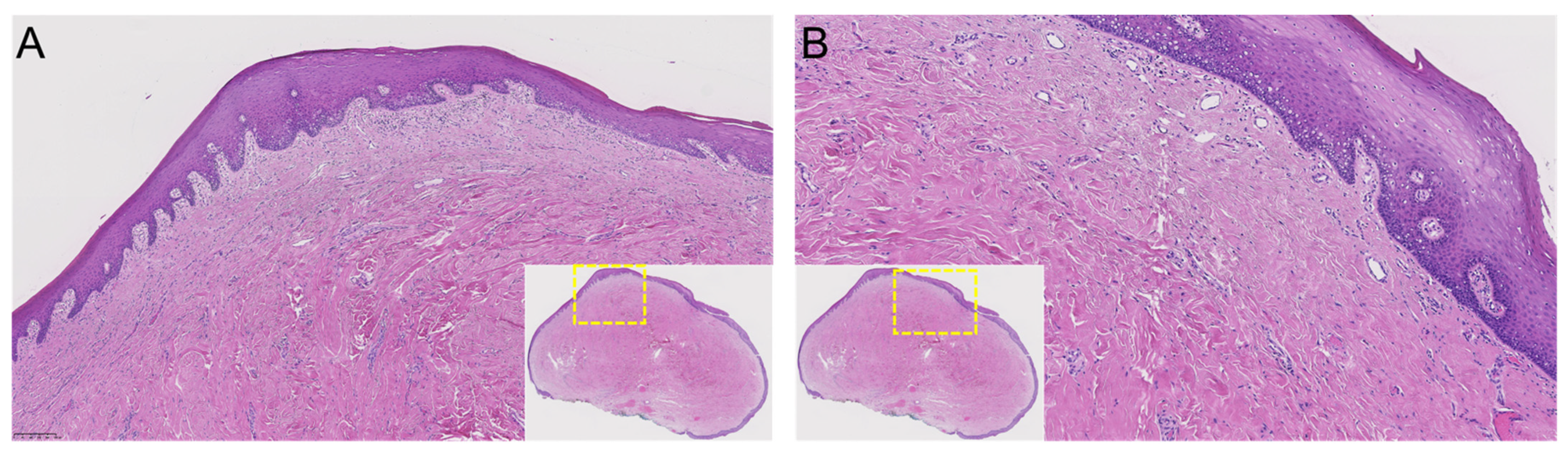
2.3. Surgery and Histopathology
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peker, E.; Öğütlü, F.; Karaca, İ.; Gültekin, E.S.; Çakır, M. A 5 year retrospective study of biopsied jaw lesions with the assessment of concordance between clinical and histopathological diagnoses. J. Oral Maxillofac. Pathol. 2016, 20, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guedes, M.M.; Albuquerque, R.; Monteiro, M.; Lopes, C.A.; do Amaral, J.B.; Pacheco, J.J.; Monteiro, L.S. Oral soft tissue biopsies in Oporto, Portugal: An eight year retrospective analysis. J. Clin. Exp. Dent. 2015, 7, e640–e648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Błochowiak, K.; Farynowska, J.; Sokalski, J.; Wyganowska-Świątkowska, M.; Witmanowski, H. Benign tumours and tumour-like lesions in the oral cavity: A retrospective analysis. Postepy Dermatol. Alergol. 2019, 36, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Naderi, N.J.; Eshghyar, N.; Esfehanian, H. Reactive lesions of the oral cavity: A retrospective study on 2068 cases. Dent. Res. J. 2012, 9, 251–255. [Google Scholar]
- Kfir, Y.; Buchner, A.; Hansen, L.S. Reactive lesions of the gingiva. A clinicopathological study of 741 cases. J. Periodontol. 1980, 51, 655–661. [Google Scholar] [CrossRef]
- Barker, D.S.; Lucas, R.B. Localised fibrous overgrowths of the oral mucosa. Br. J. Oral Surg. 1967, 5, 86–92. [Google Scholar] [CrossRef]
- Greenberg, M.S.; Glick, M. Burket’s Oral Medicine Diagnosis & Treatment, 10th ed.; Decker Inc.: Hamilton, ON, Canada, 2003; pp. 138–141. [Google Scholar]
- Wood, N.K.; Goaz, P.W. Differential Diagnosis of Oral and Maxillofacial Lesions, 5th ed.; Mosby: St. Louis, MO, USA, 2006; pp. 136–138. [Google Scholar]
- Valério, R.A.; de Queiroz, A.M.; Romualdo, P.C.; Brentegani, L.G.; de Paula-Silva, F.W. Mucocele and fibroma: Treatment and clinical features for differential diagnosis. Braz. Dent. J. 2013, 24, 537–541. [Google Scholar] [CrossRef] [Green Version]
- Toida, M.; Murakami, T.; Kato, K.; Kusunoki, Y.; Yasuda, S.; Fujitsuka, H.; Ichihara, H.; Watanabe, F.; Shimokawa, K.; Tatematsu, N. Irritation Fibroma of the Oral Mucosa: A clinicopathological study of 129 lesions in 124 cases. Oral Med. Pathol. 2001, 6, 91–94. [Google Scholar] [CrossRef] [Green Version]
- Wippold, F.J. Head and neck imaging: The role of CT and MRI. J. Magn. Reson. Imaging 2007, 25, 453–465. [Google Scholar] [CrossRef]
- Al-Haj Husain, A.; Solomons, M.; Stadlinger, B.; Pejicic, R.; Winklhofer, S.; Piccirelli, M.; Valdec, S. Visualization of the Inferior Alveolar Nerve and Lingual Nerve Using MRI in Oral and Maxillofacial Surgery: A Systematic Review. Diagnostics 2021, 11, 1657. [Google Scholar] [CrossRef]
- Reda, R.; Zanza, A.; Mazzoni, A.; Cicconetti, A.; Testarelli, L.; Di Nardo, D. An Update of the Possible Applications of Magnetic Resonance Imaging (MRI) in Dentistry: A Literature Review. J. Imaging 2021, 7, 75. [Google Scholar] [CrossRef] [PubMed]
- Valdec, S.; Al-Haj Husain, A.; Winklhofer, S.; Müller, M.; Piccirelli, M.; Stadlinger, B. Comparison of Preoperative Cone-Beam Computed Tomography and 3D-Double Echo Steady-State MRI in Third Molar Surgery. J. Clin. Med. 2021, 10, 4768. [Google Scholar] [CrossRef] [PubMed]
- Burian, E.; Sollmann, N.; Ritschl, L.M.; Palla, B.; Maier, L.; Zimmer, C.; Probst, F.; Fichter, A.; Miloro, M.; Probst, M. High resolution MRI for quantitative assessment of inferior alveolar nerve impairment in course of mandible fractures: An imaging feasibility study. Sci. Rep. 2020, 10, 11566. [Google Scholar] [CrossRef] [PubMed]
- Fujii, H.; Fujita, A.; Yang, A.; Kanazawa, H.; Buch, K.; Sakai, O.; Sugimoto, H. Visualization of the Peripheral Branches of the Mandibular Division of the Trigeminal Nerve on 3D Double-Echo Steady-State with Water Excitation Sequence. AJNR Am. J. Neuroradiol. 2015, 36, 1333–1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Haj Husain, A.; Valdec, S.; Stadlinger, B.; Rücker, M.; Piccirelli, M.; Winklhofer, S. Preoperative visualization of the lingual nerve by 3D double-echo steady-state MRI in surgical third molar extraction treatment. Clin. Oral Investig. 2022, 26, 2043–2053. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T. Dental MRI: A road beyond CBCT. Eur. Radiol. 2020, 30, 6389–6391. [Google Scholar] [CrossRef]
- Al-Haj Husain, A.; Schönegg, D.; Valdec, S.; Stadlinger, B.; Gander, T.; Essig, H.; Piccirelli, M.; Winklhofer, S. Visualization of Inferior Alveolar and Lingual Nerve Pathology by 3D Double-Echo Steady-State MRI: Two Case Reports with Literature Review. J. Imaging 2022, 8, 75. [Google Scholar] [CrossRef]
- Al-Haj Husain, A.; Stadlinger, B.; Winklhofer, S.; Piccirelli, M.; Valdec, S. Magnetic resonance imaging for preoperative diagnosis in third molar surgery: A systematic review. Oral Radiol. 2022. [Google Scholar] [CrossRef]
- Probst, M.; Burian, E.; Robl, T.; Weidlich, D.; Karampinos, D.; Brunner, T.; Zimmer, C.; Probst, F.A.; Folwaczny, M. Magnetic Resonance Imaging as a Diagnostic Tool for Periodontal Disease: A prospective study with correlation to standard clinical findings—Is there added value? J. Clin. Periodontol. 2021, 48, 929–948. [Google Scholar] [CrossRef]
- Gray, C.F.; Redpath, T.W.; Smith, F.W.; Staff, R.T. Advanced imaging: Magnetic resonance imaging in implant dentistry. Clin. Oral Implant Res. 2003, 14, 18–27. [Google Scholar] [CrossRef]
- Prager, M.; Heiland, S.; Gareis, D.; Hilgenfeld, T.; Bendszus, M.; Gaudino, C. Dental MRI using a dedicated RF-coil at 3 Tesla. J. Craniomaxillofac. Surg. 2015, 43, 2175–2182. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, U.; Eisenbeiss, A.K.; Scheifele, C.; Nelson, K.; Bock, M.; Hennig, J.; von Elverfeldt, D.; Herdt, O.; Flügge, T.; Hövener, J.B. Dental MRI using wireless intraoral coils. Sci. Rep. 2016, 6, 23301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sedlacik, J.; Kutzner, D.; Khokale, A.; Schulze, D.; Fiehler, J.; Celik, T.; Gareis, D.; Smeets, R.; Friedrich, R.E.; Heiland, M.; et al. Optimized 14 + 1 receive coil array and position system for 3D high-resolution MRI of dental and maxillomandibular structures. Dentomaxillofac. Radiol. 2016, 45, 20150177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolte, A.P.; Kolte, R.A.; Shrirao, T.S. Focal fibrous overgrowths: A case series and review of literature. Contemp. Clin. Dent. 2010, 1, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, H.; Ogasawara, T.; Toya, T.; Makihara, R.; Hirai, R.; Kawahara, E. Slow-Growing Large Irritation Fibroma of the Anterior Hard Palate: A Case Report Using Immunohistochemical Analysis. J. Maxillofac. Oral Surg. 2016, 15, 253–257. [Google Scholar] [CrossRef] [Green Version]
- Esmeili, T.; Lozada-Nur, F.; Epstein, J. Common benign oral soft tissue masses. Dent. Clin. N. Am. 2005, 49, 223–240. [Google Scholar] [CrossRef]
- Al-Haj Husain, A.; Stadlinger, B.; Winklhofer, S.; Müller, M.; Piccirelli, M.; Valdec, S. Mandibular Third Molar Surgery: Intraosseous Localization of the Inferior Alveolar Nerve Using 3D Double-Echo Steady-State MRI (3D-DESS). Diagnostics 2021, 11, 1245. [Google Scholar] [CrossRef]
- Probst, F.A.; Schweiger, J.; Stumbaum, M.J.; Karampinos, D.; Burian, E.; Probst, M. Magnetic resonance imaging based computer-guided dental implant surgery-A clinical pilot study. Clin. Implant Dent. Relat. Res. 2020, 22, 612–621. [Google Scholar] [CrossRef]
- Gradl, J.; Höreth, M.; Pfefferle, T.; Prager, M.; Hilgenfeld, T.; Gareis, D.; Bäumer, P.; Heiland, S.; Bendszus, M.; Hähnel, S. Application of a Dedicated Surface Coil in Dental MRI Provides Superior Image Quality in Comparison with a Standard Coil. Clin. Neuroradiol. 2017, 27, 371–378. [Google Scholar] [CrossRef]
- Bracher, A.K.; Hofmann, C.; Bornstedt, A.; Boujraf, S.; Hell, E.; Ulrici, J.; Spahr, A.; Haller, B.; Rasche, V. Feasibility of ultra-short echo time (UTE) magnetic resonance imaging for identification of carious lesions. Magn. Reson. Med. 2011, 66, 538–545. [Google Scholar] [CrossRef]
- Burian, E.; Probst, F.A.; Weidlich, D.; Cornelius, C.P.; Maier, L.; Robl, T.; Zimmer, C.; Karampinos, D.C.; Ritschl, L.M.; Probst, M. MRI of the inferior alveolar nerve and lingual nerve-anatomical variation and morphometric benchmark values of nerve diameters in healthy subjects. Clin. Oral Investig. 2020, 24, 2625–2634. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Wu, F.; Liu, D.; Zheng, C.; Kong, X.; Shu, S.; Li, D.; Wang, L. Visualization of the morphology and pathology of the peripheral branches of the cranial nerves using three-dimensional high-resolution high-contrast magnetic resonance neurography. Eur. J. Radiol. 2020, 132, 109137. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Black Bone MRI | 3D Double-Echo Steady-State (DESS) | 3D Short-Tau Inversion Recovery (STIR) |
|---|---|---|
| Acquisition time | 12:24 min:s | 7:04 min:s |
| FOV | 242 × 242 × 78 mm3 | 210 × 242 × 78 mm3 |
| Acquisition matrix | 320 × 320 × 78 | 256 × 243 × 64 |
| Acquisition voxel | 0.75 × 0.75 × 0.75 mm3 | 0.82 × 0.86 × 1.0 mm3 |
| Number of signal averages | 1 | 1.4 |
| TR | 11.16 ms | 3300 ms |
| TE1 | 4.21 ms | 197 ms |
| TE2 | 7.7 ms | – |
| TI | – | 220 ms |
| WFS (pix)/bandwidth (Hz) | 1/355 | 1/630 |
| Fat suppression | Selective water excitation | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Haj Husain, A.; Sekerci, E.; Schönegg, D.; Bosshard, F.A.; Stadlinger, B.; Winklhofer, S.; Piccirelli, M.; Valdec, S. Dental MRI of Oral Soft-Tissue Tumors—Optimized Use of Black Bone MRI Sequences and a 15-Channel Mandibular Coil. J. Imaging 2022, 8, 146. https://doi.org/10.3390/jimaging8050146
Al-Haj Husain A, Sekerci E, Schönegg D, Bosshard FA, Stadlinger B, Winklhofer S, Piccirelli M, Valdec S. Dental MRI of Oral Soft-Tissue Tumors—Optimized Use of Black Bone MRI Sequences and a 15-Channel Mandibular Coil. Journal of Imaging. 2022; 8(5):146. https://doi.org/10.3390/jimaging8050146
Chicago/Turabian StyleAl-Haj Husain, Adib, Esra Sekerci, Daphne Schönegg, Fabienne A. Bosshard, Bernd Stadlinger, Sebastian Winklhofer, Marco Piccirelli, and Silvio Valdec. 2022. "Dental MRI of Oral Soft-Tissue Tumors—Optimized Use of Black Bone MRI Sequences and a 15-Channel Mandibular Coil" Journal of Imaging 8, no. 5: 146. https://doi.org/10.3390/jimaging8050146
APA StyleAl-Haj Husain, A., Sekerci, E., Schönegg, D., Bosshard, F. A., Stadlinger, B., Winklhofer, S., Piccirelli, M., & Valdec, S. (2022). Dental MRI of Oral Soft-Tissue Tumors—Optimized Use of Black Bone MRI Sequences and a 15-Channel Mandibular Coil. Journal of Imaging, 8(5), 146. https://doi.org/10.3390/jimaging8050146