A Novel Method for Safety Analysis of Cyber-Physical Systems—Application to a Ship Exhaust Gas Scrubber System


 ,
,  , and
, and
Abstract
:1. Introduction
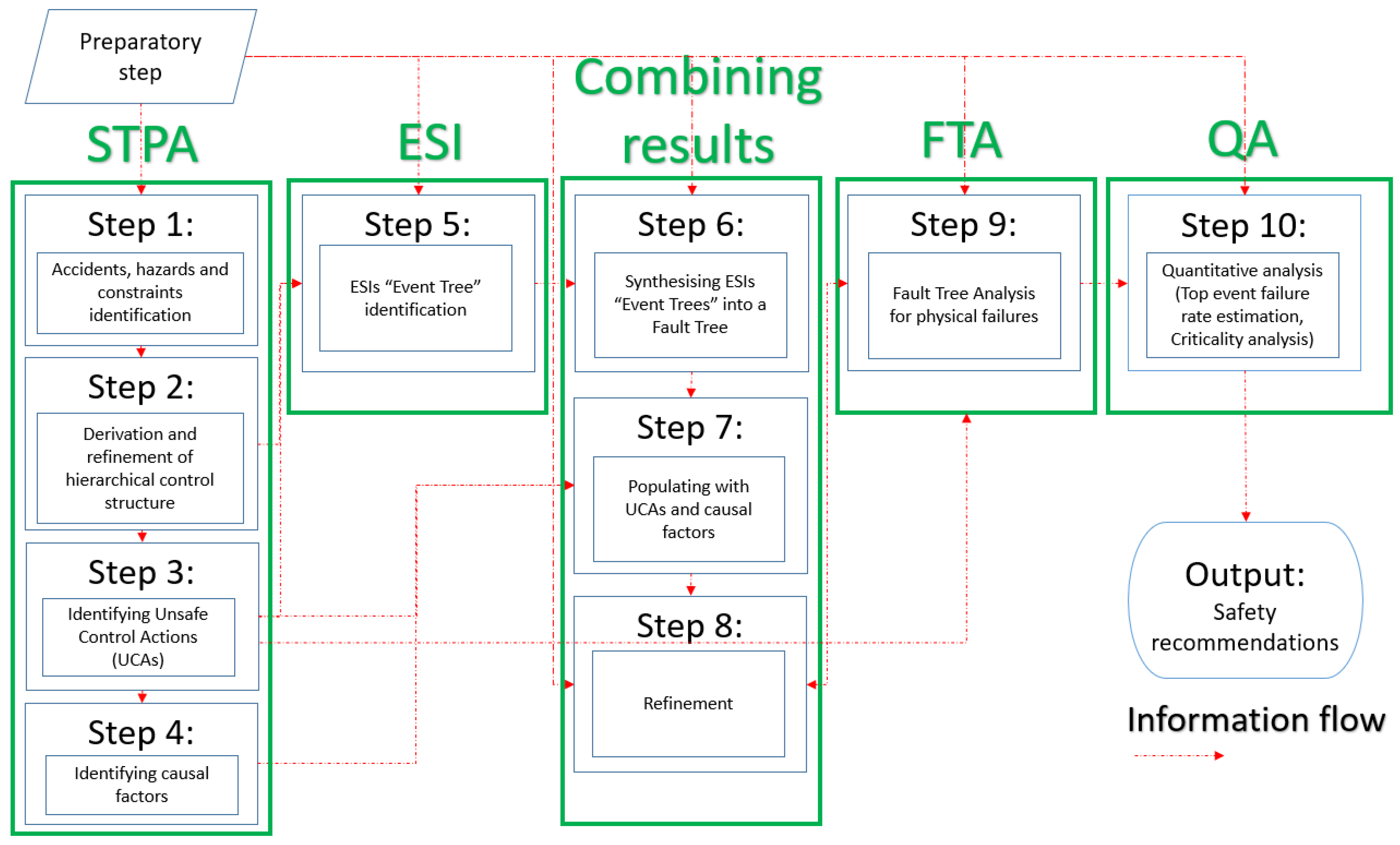
2. CASA Method Rationale and Description
2.1. Preparatory Step (Step 0)
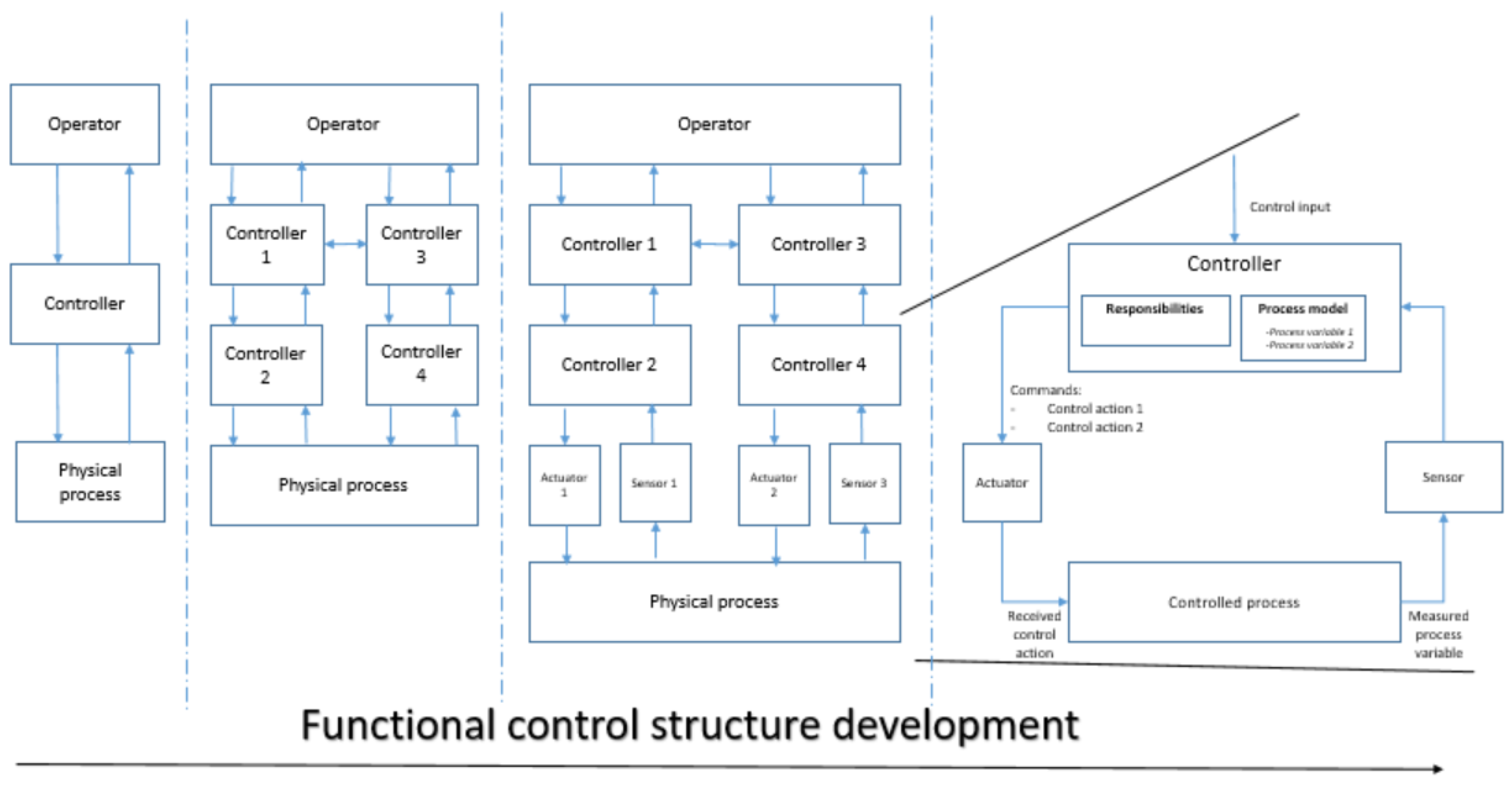
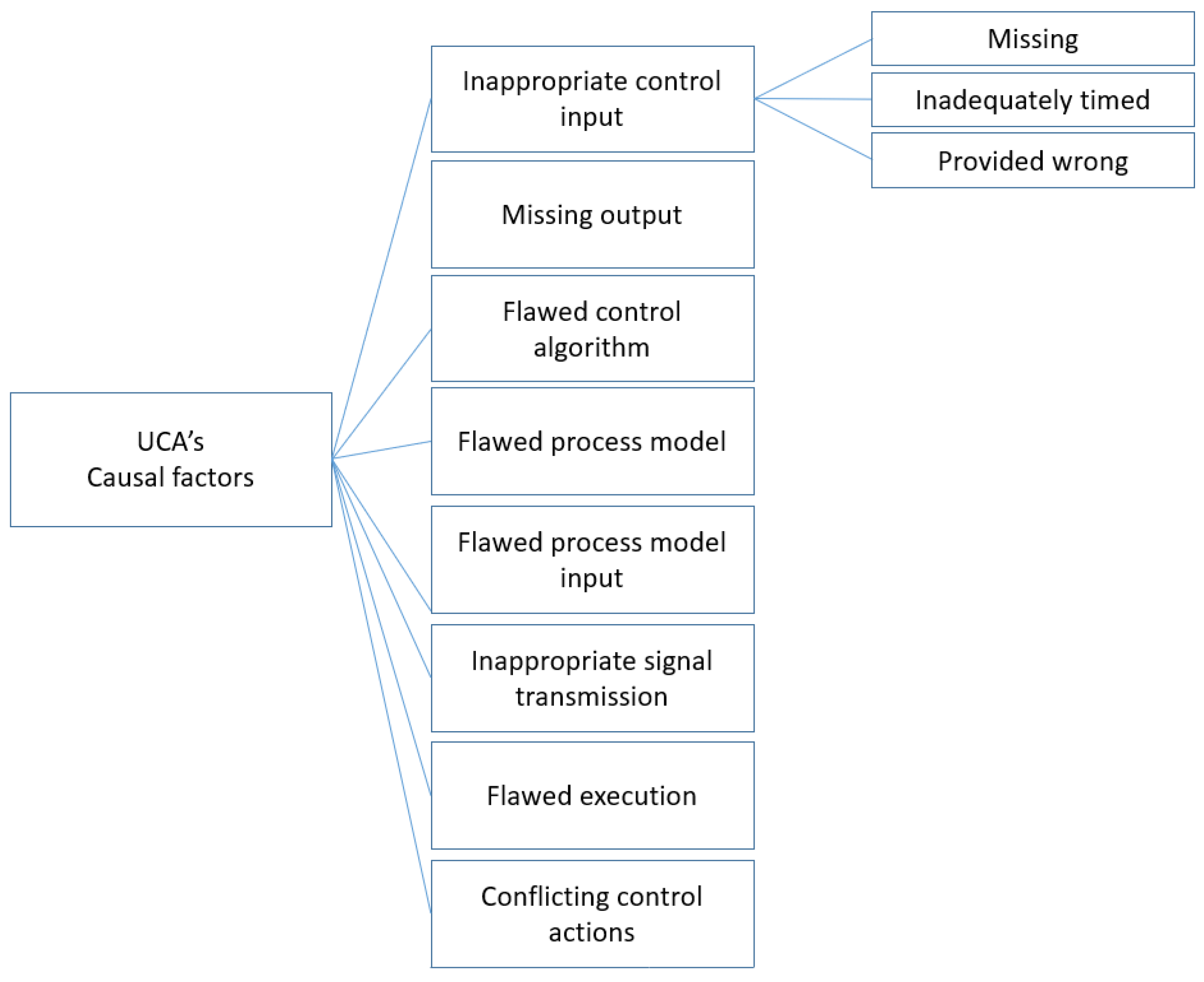
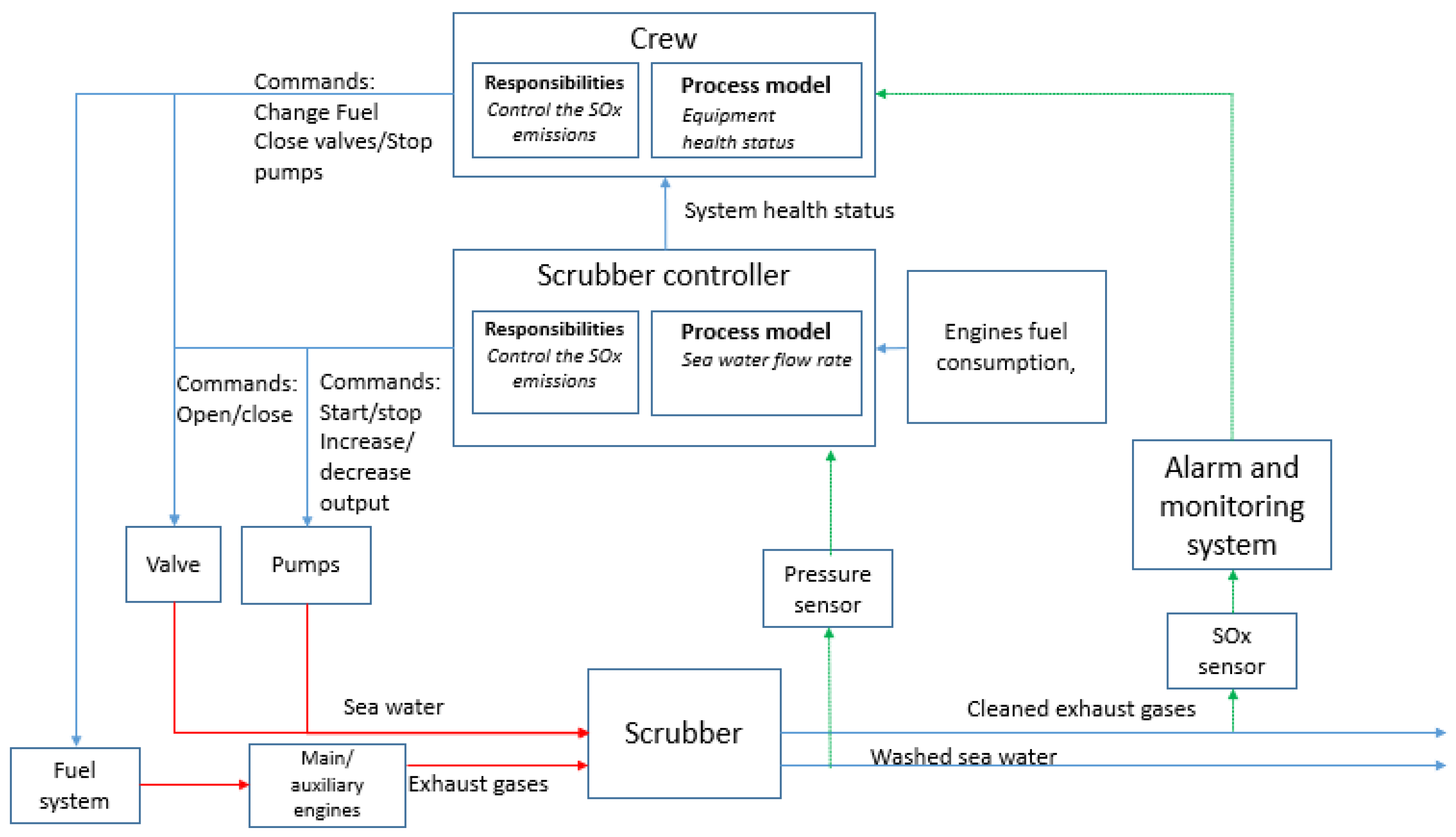
2.2. STPA (Steps 1–4)
- Type 1: Not providing the control action that leads to a hazard.
- Type 2: Providing a control action that leads to a hazard.
- Type 3: A control action is untimely provided (too late, too early or out of sequence).
- Type 4: A control action duration is not adequate (stopped too soon or applied for too long).
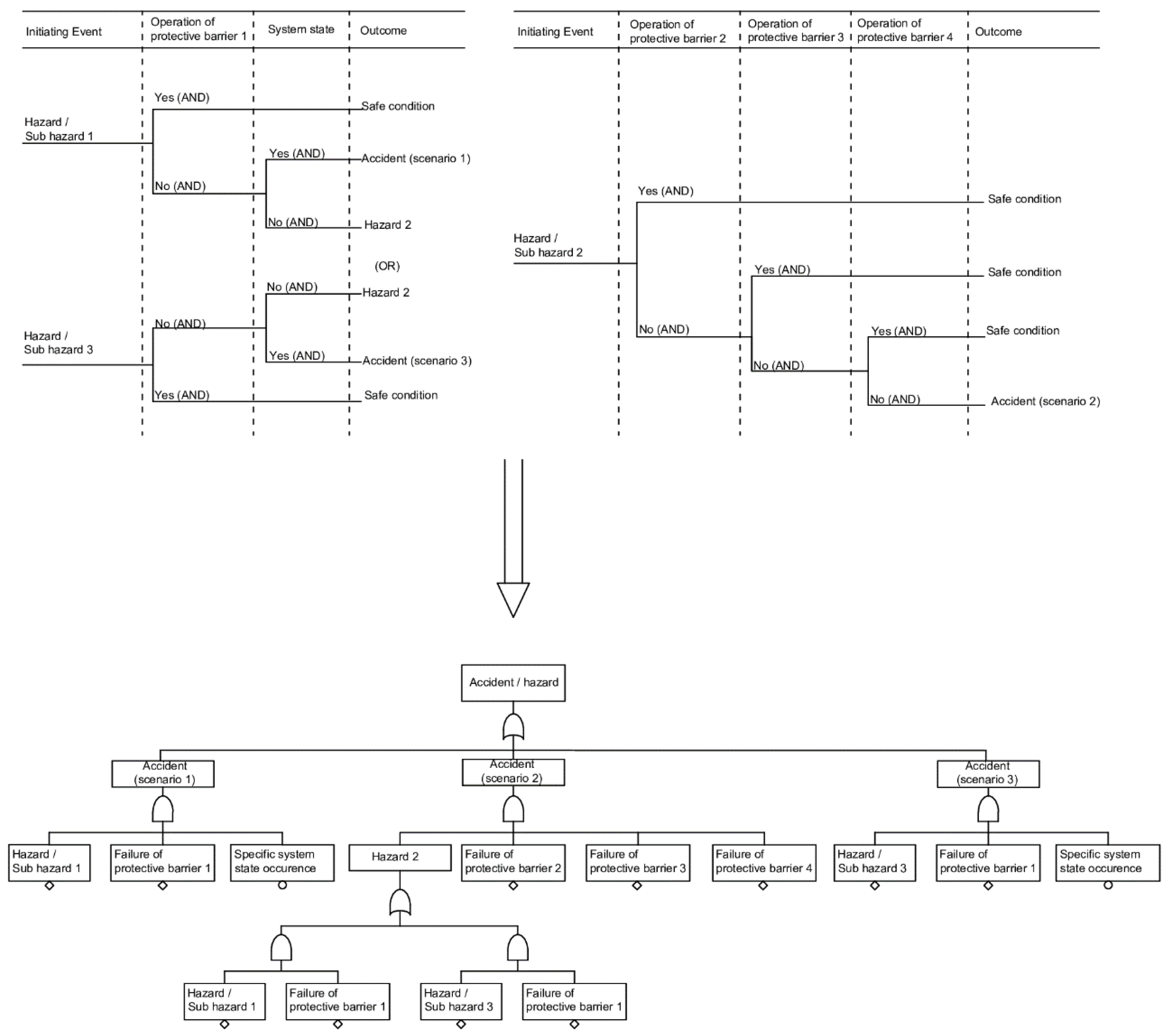
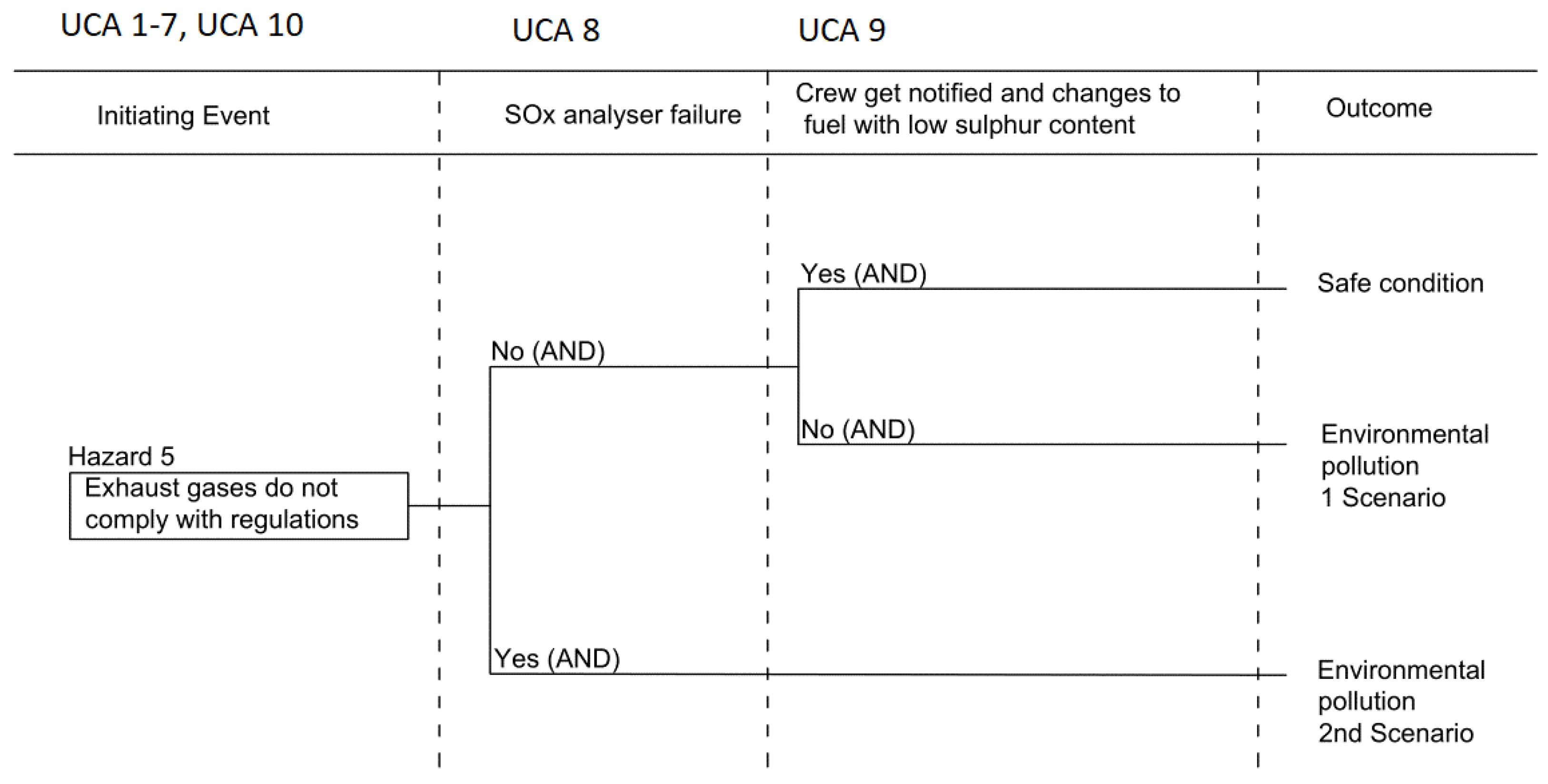
2.3. ESI (Step 5)
2.4. STPA and ESI Results’ Integration (Steps 6–8)
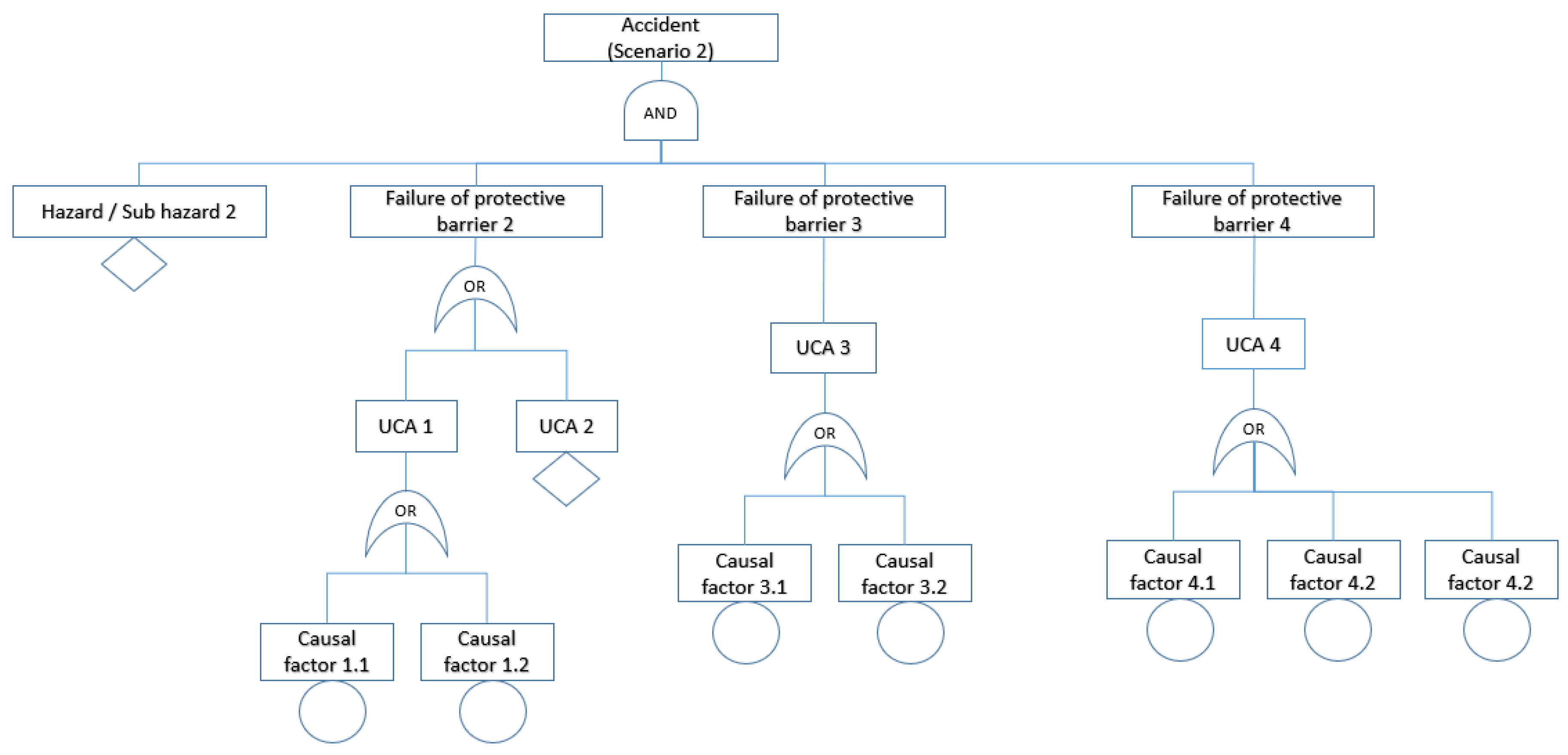
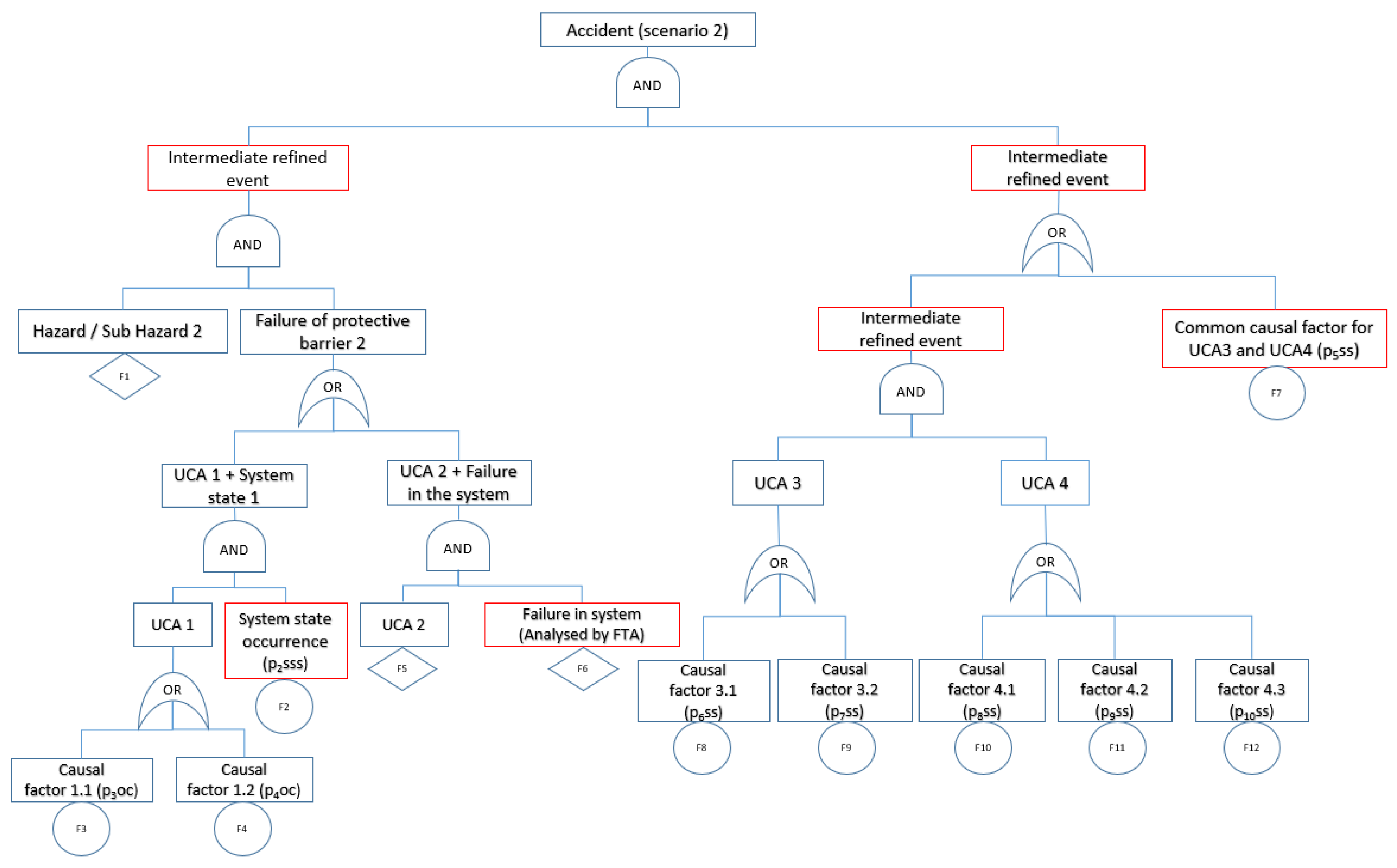
2.5. FTA (Step 9)
2.6. Quantitative Analysis (Step 10)
- The basic events in the Fault Tree can be grouped to three categories: (a) the operating system components failures (); (b) the safety systems failures () (it must be noted that the safety systems function is to control and handle the operating system components failures); and (c) specific system states, for example overloading of the generation sets ().
- The considered systems components’ failure rates follow an Exponential failure probability distribution.
- The inspection of the system components is performed according to the manufacturers’ guidelines and can effectively detect the system components’ condition including their failures and degradation level.
- The implemented maintenance practice for the systems components is according to the manufacture guidelines and restores the system components to the best possible condition (repairing their detected faults and mitigating their degradation). The maintenance intervals of the system components are considered to be timely as proposed by the respective manufacturers.
- The duration of testing and duration of repairs of faults detected during testing have negligible impact on the availability of the standby components or the components implementing safety functions.
- The top event probability differential can be adequately approximated by employing the respective difference considering a relatively small time interval, which was taken as 1 h.
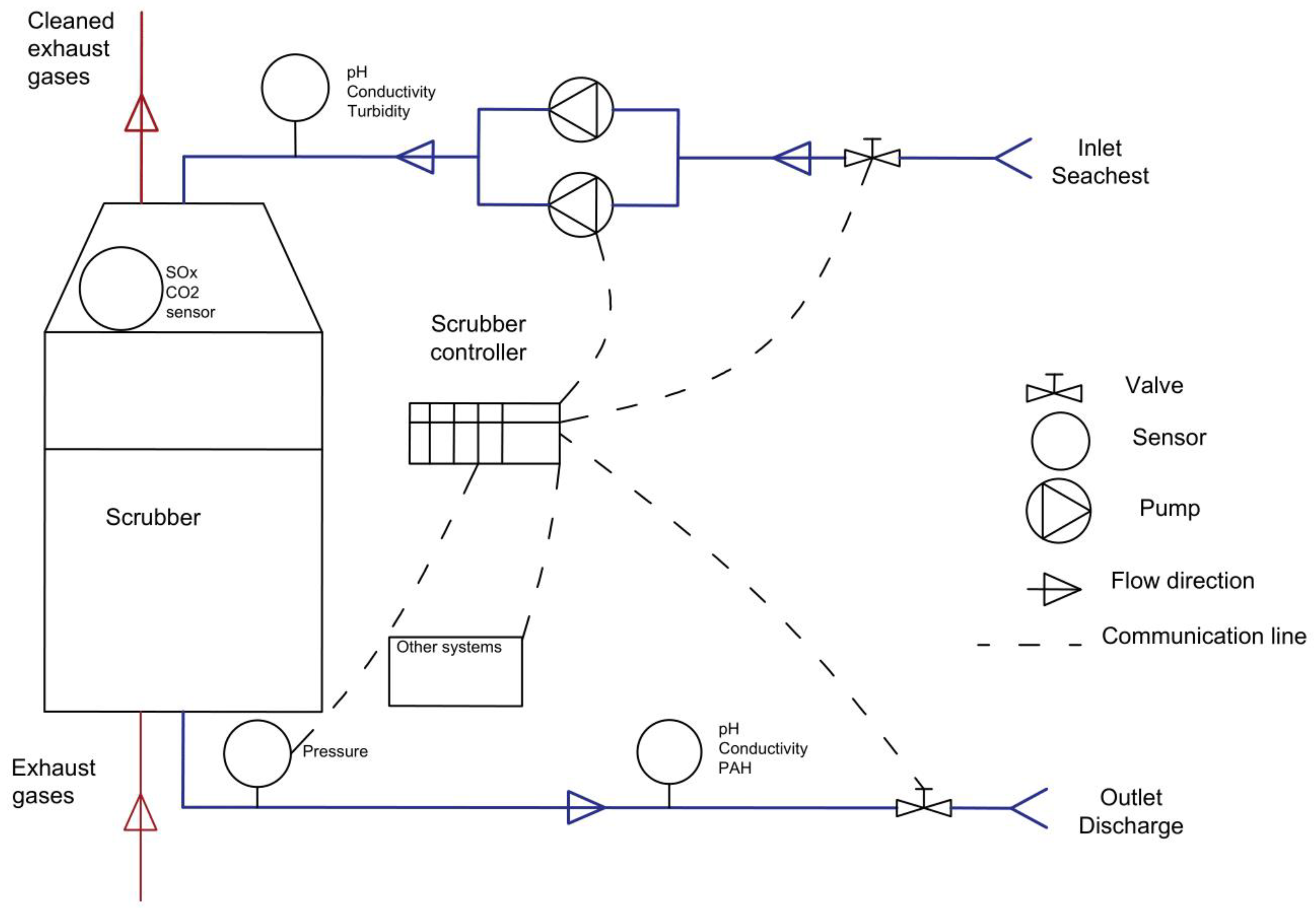
3. System Description and Analysis Input
4. Results and Discussion
4.1. STPA Results (Steps 1–4)
4.2. ESI Results (Step 5)
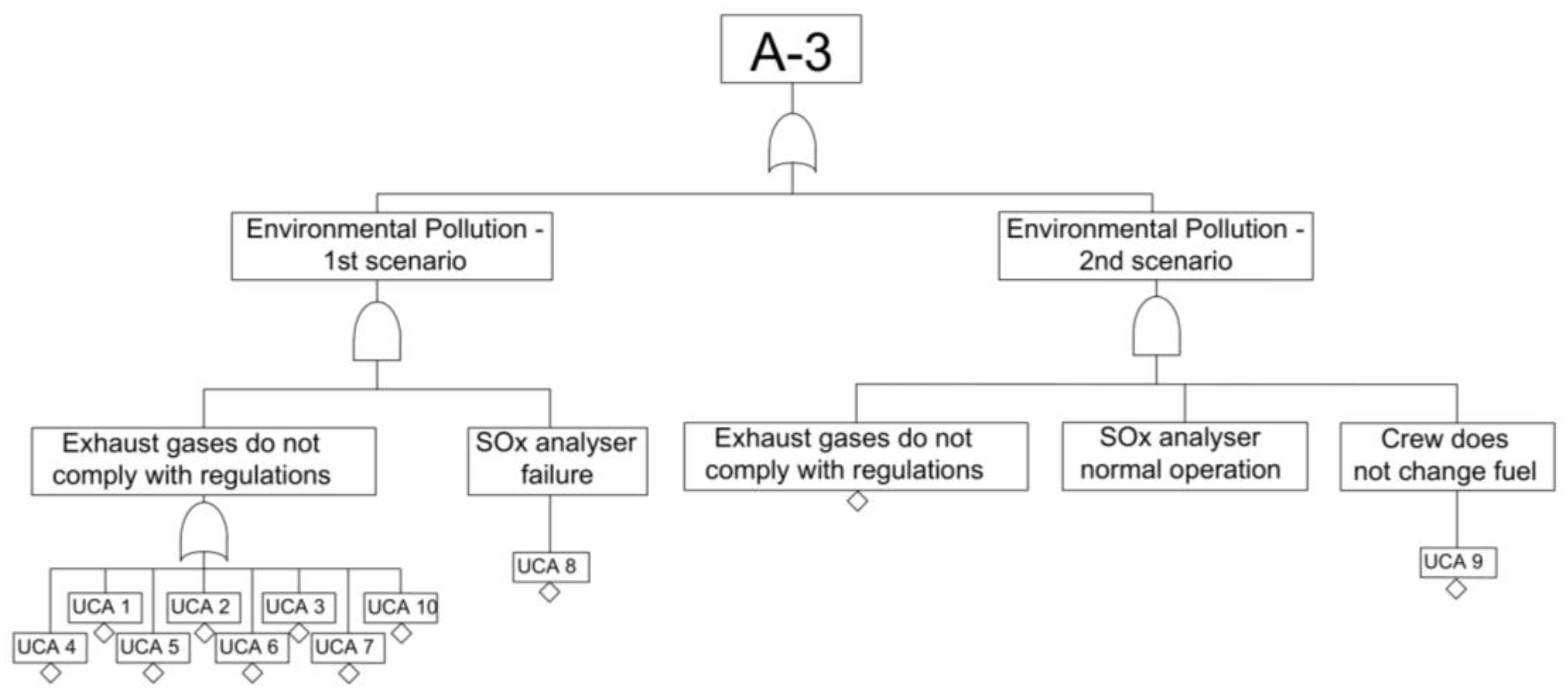
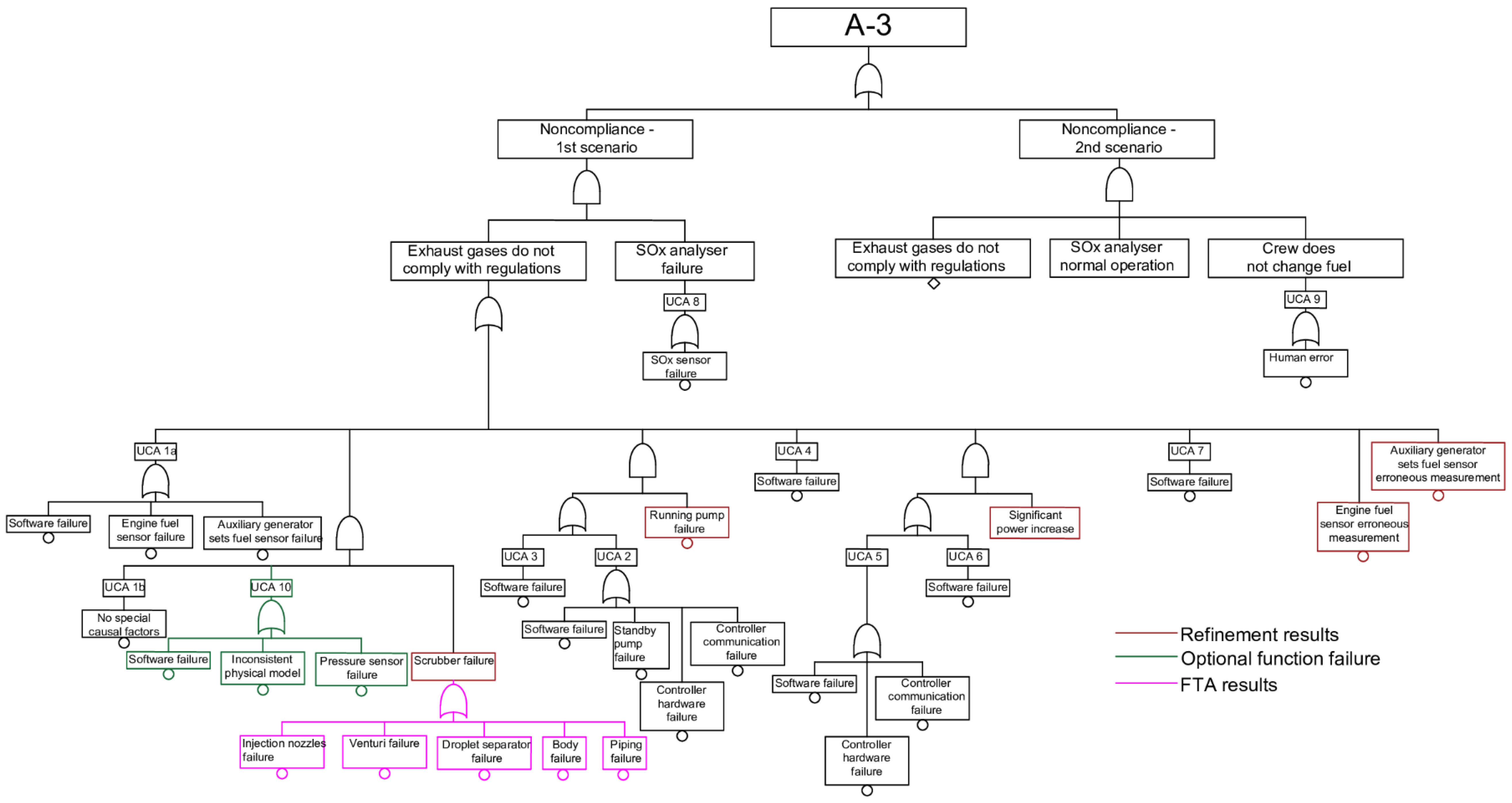
4.3. STPA and ESI Results Integration (Steps 6–8), FTA Results (Step 9)
4.4. Quantitative Analysis (Step 10)
4.5. Discussion on the Method
5. Conclusions
- The straightforward application of FTA to CPSs may result in inaccurate representation of the top event.
- The CASA method guided and resulted in a more accurate safety analysis, compared with previous FTAs for the same system by incorporating the system software failures represented by UCAs, considering the system states’ probabilities, multi-point failures, and temporal relationships in the system.
- The CASA method also allowed for the investigation and quantitative estimation of the system behaviour for cases where new functions are added to the system, as was demonstrated with the monitoring techniques applied to the SOx sensor and scrubber unit.
- The proposed method allowed for the estimation of the safety-related event failure rate and the identification of the most important factors and failures affecting the safety-related event guiding the safety enhancement of the investigated system.
- The implementation of monitoring techniques for the SOx sensor failures or two SOx sensors’ installation is expected to reduce significantly the system noncompliance failure rate (an order of magnitude) with regulations. Implementation of advanced monitoring techniques for the scrubber unit failures is expected to improve system safety, but to a lesser extent.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation and Nomenclature
| BBN | Bayesian Belief Networks |
| CPS | Cyber-Physical System |
| ESI | Events Sequence Identification |
| ETA | Event Tree Analysis |
| FMEA | Failure Modes and Effects Analysis |
| FTA | Fault Tree Analysis |
| HFO | Heavy Fuel Oil |
| ICS | Industrial Automation and Control Systems |
| PHA | Preliminary Hazard Analysis |
| PID | Proportional Integral Derivative |
| QA | Quantitative Analysis |
| STPA | System-Theoretic Process Analysis |
| UCA | Unsafe Control Action |
| Basic event in Fault Tree | |
| Fussell–Vesely importance measure | |
| Birnbaum’s importance measure | |
| Probability of failure for operating component | |
| Probability of failure of safety system | |
| Probability of specific system states | |
| The probability of failure on demand [-] | |
| Inspection or maintenance interval [hours] | |
| t | Time [hours] |
| Subscripts | |
| Component | |
| j | Basic event in Fault Tree |
| Greek symbols | |
| Failure rate for component [hours−1] | |
| The top event failure rate | |
| Repair rate for component [hours−1] |
Appendix A. The Causal Factors for UCAs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scenario Description | Causal Factors |
|---|---|
| Inappropriate control input | Missing control input |
| Inadequately timed control input | |
| Provided wrong control input | |
| Missing output (Flawed hardware) | Undiagnosed or on-demand hardware failure |
| Undiagnosed or on-demand power supply failure | |
| Flawed control algorithm (Flawed software) | Missing rules |
| Wrong rules | |
| Wrong clock and time schedule | |
| Flawed process model | Missing process variables |
| Inconsistency of the process model with the system due to system deterioration | |
| Inconsistency of the process model with the system due to system modification | |
| Inconsistency of the process model with the system due to environmental disturbances | |
| Inconsistency of process model with the system due to the improper representation of mode changes | |
| Flawed process model input | Delays due to measurement delays |
| Delays due to communication delays | |
| Delays due to inadequate integration with other controllers | |
| Inadequate information transmission due to interferences | |
| Inadequate information transmission due to noise in sensors | |
| Inadequate information transmission due to inaccurate measurements | |
| Inadequate information transmission due to incorrect installation of sensors | |
| Inadequate information due to communication with other controllers | |
| Missing information transmission due to communication failures (Hardware open, short circuits, sensor failure and failure in power supply to sensors, failure of other controllers) | |
| Missing information transmission due to errors in design (Communication bus errors, intermittent faults, incorrect installation of sensors, errors in other controllers) |
| Scenario Description | Causal Factors |
|---|---|
| Inappropriate signal transmission | Faulty transmission (Hardware open, short circuit, interferences) |
| Communication bus error | |
| Incorrect connection | |
| Inadequately timed | |
| Flawed execution (Faults in the physical process) | No execution, delayed execution, wrong execution due to actuator failure |
| No execution, wrong execution due to incorrect mounting of the actuator | |
| Failure in power supply to actuator | |
| Flawed execution due to inappropriate process input (missing, wrong, delayed) | |
| Control action not followed by the lower controller | |
| Conflicting control actions | Different data available to controllers or priorities are not appropriately set |
References
- DNV GL. Technology Outlook 2025; DNV GL: Arnhem, The Netherlands, 2015. [Google Scholar]
- Calantropio, A. The use of UAVs for performing safety-related tasks at post-disaster and non-critical construction sites. Safety 2019, 5, 64. [Google Scholar] [CrossRef] [Green Version]
- Eloranta, S.; Whitehead, A. Safety aspects of autonomous ships. In Proceedings of the 6th International Maritime Conference, Hamburg, Germany, 14–16 February 2015; pp. 168–175. [Google Scholar]
- Bolbot, V.; Theotokatos, G.; Bujorianu, L.M.; Boulougouris, E.; Vassalos, D. Vulnerabilities and safety assurance methods in Cyber-Physical Systems: A comprehensive review. Reliab. Eng. Syst. Saf. 2019, 182, 179–193. [Google Scholar] [CrossRef] [Green Version]
- Zio, E. Challenges in the vulnerability and risk analysis of critical infrastructures. Reliab. Eng. Syst. Saf. 2016, 152, 137–150. [Google Scholar] [CrossRef]
- Perrow, C. Normal Accidents: Living with High Risk Technologies; Princeton University Press: Princeton, NJ, USA, 1999. [Google Scholar]
- Sinha, K. Structural Complexity and Its Implications for Design of Cyber-Physical Systems; Massachusetts Institute of Technology: Cambridge, MA, USA, 2014. [Google Scholar]
- Wolf, M.; Serpanos, D. Safety and security in Cyber-Physical Systems and Internet-of-Things systems. Proc. IEEE 2018, 106, 9–20. [Google Scholar] [CrossRef]
- Kriaa, S.; Pietre-Cambacedes, L.; Bouissou, M.; Halgand, Y. A survey of approaches combining safety and security for industrial control systems. Reliab. Eng. Syst. Saf. 2015, 139, 156–178. [Google Scholar] [CrossRef]
- Aizpurua, J.I.; Muxika, E.; Papadopoulos, Y.; Chiacchio, F.; Manno, G. Application of the D3H2 methodology for the cost-effective design of dependable systems. Safety 2016, 2, 9. [Google Scholar] [CrossRef] [Green Version]
- Dolgov, I. Establishing training and certification criteria for visual observers of unmanned aircraft systems. Safety 2018, 4, 15. [Google Scholar] [CrossRef] [Green Version]
- Puisa, R.; Lin, L.; Bolbot, V.; Vassalos, D. Unravelling causal factors of maritime incidents and accidents. Saf. Sci. 2018, 110, 124–141. [Google Scholar] [CrossRef] [Green Version]
- Nævestad, T.-O.; Laiou, A.; Phillips, R.O.; Bjørnskau, T.; Yannis, G. Safety culture among private and professional drivers in norway and greece: Examining the influence of national road safety culture. Safety 2019, 5, 20. [Google Scholar] [CrossRef] [Green Version]
- Transportasi, K.N.K. Aircraft Accident Investigation Report; Ministry of Transportation: Jakarta, Indonesia, 2019.
- Ullah, Z.; Waldrop, T.; Chavez, N. Helicopters Sent to Rescue 1300 Passengers from Cruise Ship off Norway. Volume 2019. Available online: https://edition.cnn.com/2019/03/23/europe/norway-cruise-ship-evacuation/index.html (accessed on 1 January 2019).
- Leveson, N. Engineering a Safer World: Systems Thinking Applied to Safety; MIT press: Cambridge, MA, USA, 2011. [Google Scholar]
- Thomas, J. Extending and Automating a Systems-Theoretic Hazard Analysis for Requirements Generation and Analysis; Massachusetts Institute of Technology: Cambridge, MA, USA, 2013. [Google Scholar]
- Sulaman, S.M.; Beer, A.; Felderer, M.; Höst, M. Comparison of the FMEA and STPA safety analysis methods—A case study. Softw. Qual. J. 2019, 27, 349–387. [Google Scholar] [CrossRef] [Green Version]
- Rokseth, B.; Utne, I.B.; Vinnem, J.E. A systems approach to risk analysis of maritime operations. Proc. Inst. Mech. Eng. Part O J. Risk Reliab. 2017, 231, 53–68. [Google Scholar] [CrossRef]
- Zhang, J.; Kim, H.; Liu, Y.; Lundteigen, M.A. Combining system-theoretic process analysis and availability assessment: A subsea case study. Proc. Inst. Mech. Eng. Part O J. Risk Reliab. 2019, 233, 520–536. [Google Scholar] [CrossRef]
- Abdulkhaleq, A.; Wagner, S. Integrating State Machine Analysis with System-Theoretic Process Analysis; Gesellschaft fur Informatik: Bonn, Germany, 2013; pp. 501–514. [Google Scholar]
- Bjerga, T.; Aven, T.; Zio, E. Uncertainty treatment in risk analysis of complex systems: The cases of STAMP and FRAM. Reliab. Eng. Syst. Saf. 2016, 156, 203–209. [Google Scholar] [CrossRef]
- Asare, P.; Lach, J.; Stankovic, J.A. FSTPA-I: A formal approach to hazard identification via system theoretic process analysis. In Proceedings of the ACM/IEEE 4th International Conference on Cyber-Physical Systems, Philadelphia, PA, USA, 8–11 April 2013; pp. 150–159. [Google Scholar]
- Rabin, M.O.; Scott, D. Finite automata and their decision problems. IBM J. Res. Dev. 1959, 3, 114–125. [Google Scholar] [CrossRef]
- Zhong, D.; Wu, N.; Wang, Q.; Sun, R. A multi-view extended software control structure modeling and safety analysis method. In Proceedings of the 2015 Prognostics and System Health Management Conference (PHM), Beijing, China, 21–23 October 2015; pp. 1–5. [Google Scholar]
- Procter, S.; Hatcliff, J. An architecturally-integrated, systems-based hazard analysis for medical applications. In Proceedings of the 2014 Twelfth ACM/IEEE Conference on Formal Methods and Models for Codesign (MEMOCODE), Lausanne, Switzerland, 19–21 October 2014; pp. 124–133. [Google Scholar]
- Wang, R.; Zheng, W.; Liang, C.; Tang, T. An integrated hazard identification method based on the hierarchical Colored Petri Net. Saf. Sci. 2016, 88, 166–179. [Google Scholar] [CrossRef]
- Liu, J.T.; Tang, T.; Zhu, J.B.; Zhao, L. An extended system-theoretic hazard analysis method for the safety of high-speed railway train control systems. Proc. Inst. Mech. Eng. Part F J. Rail Rapid Transit 2016, 231, 821–834. [Google Scholar] [CrossRef]
- Faiella, G.; Parand, A.; Franklin, B.D.; Chana, P.; Cesarelli, M.; Stanton, N.A.; Sevdalis, N. Expanding healthcare failure mode and effect analysis: A composite proactive risk analysis approach. Reliab. Eng. Syst. Saf. 2018, 169, 117–126. [Google Scholar] [CrossRef] [Green Version]
- Wheeler, T.A.; Williams, A.D.; Turner, P.L.; Muna, A.B.; Schulz, P.V. A New Look at Cyber Security for Nuclear Power Plants: The Cyber Hazards Analysis Risk Methodology (CHARM)-Slides; Sandia National Lab.(SNL-NM): Albuquerque, NM, USA, 2016.
- Clark, A.J.; Williams, A.D.; Muna, A.; Gibson, M. Hazard and Consequence Analysis for Digital Systems–A New Approach to Risk Analysis in the Digital Era for Nuclear Power Plants; Transactions of the American Nuclear Society: Orlando, FL, USA, 2018. [Google Scholar]
- Utne, I.B.; Rokseth, B.; Sørensen, A.J.; Vinnem, J.E. Towards supervisory risk control of autonomous ships. Reliab. Eng. Syst. Saf. 2020, 196, 106757. [Google Scholar] [CrossRef]
- Rokseth, B.; Utne, I.B.; Vinnem, J.E. Deriving verification objectives and scenarios for maritime systems using the systems-theoretic process analysis. Reliab. Eng. Syst. Saf. 2018, 169, 18–31. [Google Scholar] [CrossRef]
- Puisa, R.; Bolbot, V.; Ihle, I. Development of functional safety requirements for DP-driven servicing of wind turbines. In Proceedings of the European STAMP Workshop & Conference 2019, Helsinki, Finland, 17–20 September 2019. [Google Scholar]
- Bolbot, V.; Puisa, R.; Theotokatos, G.; Boulougouris, E.; Vassalos, D. A comparative safety assessment for DC and DC with hybrid power systems in a windfarm SOV using STPA. In Proceedings of the European STAMP Workshop & Conference, Helsinki, Finland, 17–20 September 2019. [Google Scholar]
- Wróbel, K.; Montewka, J.; Kujala, P. Towards the development of a system-theoretic model for safety assessment of autonomous merchant vessels. Reliab. Eng. Syst. Saf. 2018, 178, 209–224. [Google Scholar] [CrossRef]
- Valdez Banda, O.A.; Kannos, S.; Goerlandt, F.; van Gelder, P.H.A.J.M.; Bergström, M.; Kujala, P. A systemic hazard analysis and management process for the concept design phase of an autonomous vessel. Reliab. Eng. Syst. Saf. 2019, 191, 106584. [Google Scholar] [CrossRef]
- Bolbot, V.; Theotokatos, G.; Boulougouris, E.; Vassalos, D. Comparison of diesel-electric with hybrid-electric propulsion system safety using System-Theoretic Process Analysis. In Proceedings of the Propulsion and Power Alternatives, London, UK, 22–23 January 2019; pp. 55–61. [Google Scholar]
- Panasiuk, I.; Turkina, L. The evaluation of investments efficiency of SOx scrubber installation. Transp. Res. Part D Transp. Environ. 2015, 40, 87–96. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. IARC: Diesel Engine Exhaust Carcinogenic; International Agency for Research on Cancer: Lyon, France, 2012; Volume 213. [Google Scholar]
- United States Environmental Protection Agency. What is Acid Rain? Available online: https://www.epa.gov/acidrain/what-acid-rain (accessed on 1 February 2020).
- Pavlidis, A. Techno-Economic and Safety Analysis of Installation of a Scrubber in Oil Tankers. Bachelor’s Thesis, University of Strathclyde, Glasgow, UK, 2018. [Google Scholar]
- Andersen, M.L. Formal Safety Assessment of an Open Loop System. Master’s Thesis, Norwegian University of Science and Technology, Trondheim, Norway, 2015. [Google Scholar]
- Young, W.; Leveson, N.G. An integrated approach to safety and security based on systems theory. Commun. ACM 2014, 57, 31–35. [Google Scholar] [CrossRef]
- Kabir, S.; Papadopoulos, Y.; Walker, M.; Parker, D.; Aizpurua, J.I.; Lampe, J.; Rüde, E. A model-based extension to hip-hops for dynamic fault propagation studies. In International Symposium on Model-Based Safety and Assessment; Springer: Cham, Switzerland, 2017; pp. 163–178. [Google Scholar]
- ISO. Risk Management—Risk assessment techniques. In ISO 31010; International Organization for Standardization: Switzerland, Geneva, 2009; p. 92. [Google Scholar]
- Ramos, M.A.; Thieme, C.A.; Utne, I.B.; Mosleh, A. Human-system concurrent task analysis for maritime autonomous surface ship operation and safety. Reliab. Eng. Syst. Saf. 2020, 195, 106697. [Google Scholar] [CrossRef]
- Bolbot, V.; Theotokatos, G.; Vassalos, D. Using system-theoretic process analysis and event tree analysis for creation of a fault tree of blackout in the Diesel-Electric Propulsion system of a cruise ship. In Proceedings of the International Marine Design Conference XIII, Helsinki, Finland, 10–14 June 2018; pp. 691–699. [Google Scholar]
- Leveson, N.; Thomas, J. STPA Handbook; MIT: Cambridge, MA, USA, 2018. [Google Scholar]
- Blandine, A. System theoretic hazard analysis applied to the risk review of complex systems: An example from the medical device industry. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2013. [Google Scholar]
- Becker, C.; Van Eikema Hommes, Q. Transportation Systems Safety Hazard Analysis Tool (SafetyHAT) User Guide (Version 1.0); John, A., Ed.; Volpe National Transportation Systems Center: Cambridge, MA, USA, 2014.
- Hamann, R.; Papanikolaou, A.; Eliopoulou, E.; Golyshev, P. Assessment of safety performance of container ships. In Proceedings of the IDFS 2013, Shanghai, China, 25–27 November 2013; pp. 18–26. [Google Scholar]
- Goerlandt, F.; Khakzad, N.; Reniers, G. Validity and validation of safety-related quantitative risk analysis: A review. Saf. Sci. 2016, 99, 127–139. [Google Scholar] [CrossRef]
- Johansen, I.L.; Rausand, M. Foundations and choice of risk metrics. Saf. Sci. 2014, 62, 386–399. [Google Scholar] [CrossRef]
- Schüller, J.; Brinkman, J.; Van Gestel, P.J.; Van Otterloo, R. Methods for Determining and Processing Probabilities: Red Book; Committee for the Prevention of Disasters: Hague, Netherlands, 1997. [Google Scholar]
- Verma, A.K.; Srividya, A.; Karanki, D.R. Reliability and Safety Engineering; Springer: Berlin/Heidelberg, Germany, 2010; Volume 43. [Google Scholar]
- Fricks, R.M.; Trivedi, K.S. Importance analysis with Markov chains. In Proceedings of the Annual Reliability and Maintainability Symposium, Tampa, FL, USA, 27–30 January 2003; pp. 89–95. [Google Scholar]
- Gomez, C. Importance Measures; Workshop on PSA applications: Sofia, Bulgaria, 1997.
- Chybowski, L.; Idziaszczyk, D.; Wiśnicki, B. A comparative components importance analysis of a complex technical system with the use of different importance measures. Syst. Wspomagania w Inżynierii Prod. 2014, 23–33. [Google Scholar]
- Laval, A. PureSOx Design Guide; Alfa Laval: Lund, Sweden, 2017. [Google Scholar]
- Laval, A. Maintenance Manual; Alfa Laval: Lund, Sweden, 2017. [Google Scholar]
- SINTEF. Reliability Data for Safety Instrumented Systems PDS Data Handbook; SINTEF: Trondheim, Norway, 2006; p. 85. [Google Scholar]
- Aldemir, T.; Stovsky, M.; Kirschenbaum, J.; Mandelli, D.; Bucci, P.; Mangan, L.; Miller, D.; Sun, X.; Ekici, E.; Guarro, S. Dynamic reliability modeling of digital instrumentation and control systems for nuclear reactor probabilistic risk assessments. In NUREG0CR-6942; US Nuclear Regulatory Commission: Washington, DC, USA, 2007. [Google Scholar]
- Chai, M.; Reddy, D.B.; Sobrayen, L.; Panda, K.S.; Die, W.; Xiaoqing, C. Improvement in efficiency and reliability for diesel- electric propulsion based marine vessels using genetic algorithm. In Proceedings of the 2016 IEEE Transportation Electrification Conference and Expo, Asia-Pacific (ITEC Asia-Pacific), Busan, Korea, 1–4 June 2016; pp. 180–184. [Google Scholar]
- OREDA. Offshore Reliability Data Handbook; OREDA: Trondheim, Norway, 2015. [Google Scholar]
- BSI. Functional safety—Safety instrumented systems for the process industry sector. In Part 3: Guidance for Determination of the Required Safety Integrity Levels; BSI: London, UK, 2004; Volume IEC-61511. [Google Scholar]
- Bolbot, V.; Trivyza, N.L.; Theotokatos, G.; Boulougouris, E.; Rentizelas, A.; Vassalos, D. Cruise ships power plant optimisation and comparative analysis. Energy 2020, 196, 117061. [Google Scholar] [CrossRef]
- Roskilly, T. INOMANS2HIP Final Publishable Report; University of Newcastle Upon Tyne: Tyne and Wear, UK, 2016. [Google Scholar]











| Steps | Step Description | Employed Technique | Justification | Required Resources | Output | Output to Steps | |
|---|---|---|---|---|---|---|---|
| Initiation | Step 0: Preparation | Accumulating system data: accidents investigations reports, previous hazards analyses, components failure rates, system simulations, etc. | Publications and accident investigation reports analysis | Good understanding of system problems required for analysis | Access to data | Good understanding of the system | All other steps |
| STPA | Step 1: Defining the scope of analysis | Identification/selection of accident, system hazards, sub hazards and safety constraints for the system | Hazard review/Brainstorming | Setting the boundaries of analysis | Good understanding of the system, potentially team of experts | List of accidents, hazards and safety constraints, hierarchical control structure | Steps 2, 3, 5 |
| Step 2: Hierarchical control structure | Development of the system control structure | Following the STPA guidelines | Developing system model for the STPA | Access to the manuals and the drawings | Hierarchical control structure | Steps 3, 4 | |
| Step 3: UCAs identification | UCAs are identified | Following the STPA guidelines | To identify control failures | List of the control actions and the context variables | List of UCAs in tabular format | Steps 4, 5 and 9 | |
| Step 4: Causal factors analysis | For each of the UCAs causal factors are identified | Using a developed checklist | Identification of the causal factors for the UCAs | List of the UCAs, control structure, checklist | List of the causal factors for the UCAs | Step 7 | |
| ESI | Step 5: Developing event sequences | ESI using hazards/sub hazards as Initiating Events following logic similar to Event Tree Analysis | ESI | Connecting UCAs, sub hazards and hazards | List of the hazards, safety constraints and UCAs | ESI results for each of the hazards | Step 6 |
| Integration of STPA and ESI results | Step 6: Synthesis of ESI results | Unification of the ESI results | Applying a number of logic rules | To connect different ESI results | ESI results from the previous step | Combined Fault Tree | Step 7 |
| Step 7: Populating the Fault Tree | Enriching the Fault Tree with results of the STPA | Manually | Connecting the UCAs, hazards and accidents | Results of STPA and initial Fault Tree | More detailed Fault Tree | Step 8 | |
| Step 8: Refinement | Refinement of already developed Fault Tree | Applying a number of logic rules | Correcting inconsistencies | Fault Tree from the previous step | Refined Fault Tree | Step 9 | |
| FTA | Step 9: Fault Tree Analysis | Fault Tree Analysis | Fault Tree Analysis | Analysis of the physical failures | Access to the manuals and the drawings | Final Fault Tree | Step 10 |
| QA | Step 10: Quantitative analysis | Estimation of the frequency of the top event, criticality analysis, importance analysis, etc. | Fault Tree and equations calculations | Critical components identification and performance prediction | Failure rates, operational data, inspection and maintenance intervals | Safety recommendations | Risk estimation |
| Rule Number | Condition | Refinement Action |
|---|---|---|
| 1 | An UCA is hazardous in a specific context and this is not captured by the ESI “Event Tree” | An UCA is split into control action and the context variable, representing context connected using AND gate |
| 2 | An UCA is a causal factor of another UCA | Grouping is applied, the UCA is connected to the other one using OR gate |
| 3 | UCAs have identical causal factors and are located in the same position of the ESI “Event Tree”/Fault Tree | Merging of these UCAs is applied |
| 4 | A common causal factor for the UCAs at different points of “Event Tree”/Fault Tree | Causal factors are promoted to a higher level of the Fault Tree |
| 5 | A contradiction in a sequence of events occurs | Elimination of the contradictory events |
| 6 | An UCA is caused by a complex physical failure, which is refined by a Fault Tree | Subcases are defined for each physical failure |
| 7 | Common cause failures leading to complex physical failure | Subcase is defined for the common cause failure in Fault Tree |
| Component | Function |
|---|---|
| Scrubber controller | Control of the sea water flow to the scrubber unit, monitoring of scrubber unit health status (provisional function) |
| Inlet sea chest valve | Sea water flow control (can be either open or closed) |
| Outlet sea chest valve | Sea water flow control (can be either open or closed) |
| Sea Water Pump | Increasing/Decreasing sea water flow |
| Scrubber Unit (Scrubber body, piping, droplet, venturi, injection nozzles) | Exhaust gases spraying |
| Sensors (SOx emissions, pressure, pH, conductivity, CO2 emissions) | Measuring operating parameters |
| Failure Rate Description | PFD/Failure Rate |
|---|---|
| Commission errors for software functions [h−1] [62] | 1.00 × 10−5 |
| Omission errors for software functions (probability of failure on demand (PFD)) [62] | 5.00 × 10−5 |
| Proportional Integral Derivative (PID) controller failure to react/overreaction to changes in system configuration due to software errors [h−1] [63] | 1.00 × 10−6 |
| Controller hardware failure rate [h−1] [62] | 1.50 × 10−5 |
| Communication lines failure rate [h−1] [64] | 2.50 × 10−8 |
| Fuel sensor failure rate (for engines and auxiliary generating sets) [h−1] [65] | 2.00 × 10−6 |
| Human error probability of failure on demand [66] | 1.00 × 10−3 |
| Pump failure rate [h−1] [65] | 3.02 × 10−5 |
| Injection nozzles failure rate [h−1] [42,43] | 4.58 × 10−6 |
| Venturi failure rate [h−1] [42,43] | 1.53 × 10−6 |
| Droplet separator failure rate [h−1] [42,43] | 1.53 × 10−6 |
| Body failure rate [h−1] [42,43] | 1.53 × 10−6 |
| Piping failure rate [h−1] [42,43] | 7.88 × 10−6 |
| Significant power increase in engine/auxiliary engines load [h−1] Approximation of operating profile, based on cruise ship vessel [67] | 1.00 × 10−1 |
| SOx sensor failure rate [h−1] [42] | 1.38 × 10−5 |
| Pressure sensors failure rate [65] [h−1] | 2.00 × 10−6 |
| Sensors maintenance rate—Assumption [h−1]—it considered that, under continuous monitoring of sensor failures, their correction is implemented almost immediately | 1 |
| Inconsistent diagnostic/prognostics model resulting in false negatives (test indicates that no failure is observed in the system whilst it is present)—Assumption (PFD) Rather conservative | 0.1 |
| Accident | Exhaust Gas Open Loop Scrubber Hazard | Safety Constraints |
|---|---|---|
| [A-1] Human loss or injury | [H-1] Operating personnel touching hot surfaces [H-2] Exhaust gases leakage depriving the engine room from oxygen | Protective surfaces, personnel training, oxygen level monitoring in engine room |
| [A-2] Damage to ship/ship systems | [H-3] Overpressure in scrubber unit [H-4] Water ingression through scrubber system | Diagnosis of system failures Use of non-return valves |
| [A-3] Environmental pollution | [H-5] Exhaust gas not complying with regulatory requirements. [H-6] Disposed sea water not complying with regulations. | SOx sensor Sea water analysers |
| Control Action | Type of UCA | UCA No. | Description |
|---|---|---|---|
| Close valves | Providing | 1 | Closing valves during normal operation/faulty conditions will restrict the scrubber functionality [H-5] |
| Start pump | Not providing | 2 | Not starting standby sea water pump when other pump is faulty/insufficient will inhibit the scrubber operation due to lack of sea water flow [H-5] |
| Providing with delay | 3 | Starting sea water pumps with delay will inhibit the scrubber operation due to the lack of sea water flow [H-5] | |
| Stop pump | Providing | 4 | Stopping pump during normal operation will cause unavailability of sea water in scrubber [H-5] |
| Increase sea water flow | Not providing | 5 | Not providing sea water flow increase when the auxiliary/engines output increase may lead to noncompliance with regulations [H-5] |
| Providing with delay | 6 | Providing sea water flow increase with delay when the auxiliary/engines output increase may lead to noncompliance with regulations [H-5] | |
| Decrease sea water flow | Providing | 7 | Decreasing sea water flow when the auxiliary/engines output increase/stable may lead to noncompliance with regulations [H-5] |
| Issue alarm | Not providing | 8 | Not issuing alarm, when the system SOx emissions are not in compliance will lead to noncompliance with regulations [H-5] |
| Implement fuel change over | Not providing | 9 | Not changing fuel during faulty operation of the scrubber will lead to noncompliance with regulations [H-5] |
| Diagnose and predict scrubber failures | Not providing | 10 | Not diagnosing and predicting failures in scrubber may lead to operation with faulty scrubber system [H-5] |
| UCA No. | Causal Factors |
|---|---|
| 1 | Software failure, engine and auxiliary generator sets fuel sensors failure |
| 2 | Pump failure, controller hardware failure, communication failure, software failure, controller hardware failure |
| 3 | Software failure (Wrong software implementation on controller) |
| 4 | Software failure, engine and auxiliary gets load/fuel sensors erroneous measurement |
| 5 | Software failure, controller hardware failure, communication failure, engine and auxiliary gets fuel sensors erroneous measurement |
| 6 | Software failure |
| 7 | Software failure, engine and auxiliary generator sets load sensors erroneous measurement |
| 8 | SOx sensor failure |
| 9 | Human error |
| 10 | Software failure, inconsistent physical model, pressure sensor errors |
| Case (a) | Case (b) | Case (c) | Case (d) |
|---|---|---|---|
| With regular testing of SOx sensor (without continuous monitoring) | With continuous monitoring of SOx sensor failures | With application of diagnosis/prognosis for scrubber unit failures and with regular testing of SOx sensor | With two SOx sensors installed |
| 1.99 10−6 [h−1] | 5.68 10−8 [h−1] | 1.44 10−6 [h−1] | 1.23 10−7 |
| No. | With Regular Testing of SOx Sensor (without Continuous Monitoring) | With Continuous Monitoring of SOx Sensor Failures | With Application of Diagnosis/Prognosis for Scrubber Unit Failures and with Regular Testing of the SOx Sensor | With Two SOx Sensors Installed | ||||
|---|---|---|---|---|---|---|---|---|
| Birnbaum [-] | Fussell–Vesely [-] | Birnbaum [-] | Fussell–Vesely [-] | Birnbaum [-] | Fussell–Vesely [-] | Birnbaum [-] | Fussell–Vesely [-] | |
| 1 | Injection nozzles failure 0.070 | SOx sensor failure 0.972 | Injection nozzles failure 0.002 | Human error 0.986 | Injection nozzles failure 0.039 | SOx sensor failure 0.972 | Injection nozzles failure 0.004 | SOx sensor failure 0.543 |
| 2 | Venturi failure 0.070 | Controller software closing valves 0.178 | Venturi failure 0.002 | Controller software closing valves 0.178 | Venturi failure 0.039 | Controller software closing valves 0.247 | Venturi failure 0.004 | Human error 0.457 |
| 3 | Controller software closing valves 0.035 | Controller software stopping pump 0.178 | Controller software closing valves 0.001 | Controller software stopping pump 0.178 | Controller software closing valves 0.035 | Controller software stopping pump 0.247 | Controller software closing valves 0.002 | Controller software closing valves 0.178 |
| 4 | Controller software stopping pump 0.035 | Injection nozzles failure 0.163 | Controller software stopping pump 0.001 | Piping failure 0.140 | Controller software stopping pump 0.035 | Injection nozzles failure 0.124 | Controller software stopping pump 0.002 | Controller software stopping pump 0.178 |
| 5 | Piping failure 0.035 | Piping failure 0.140 | Piping failure 0.001 | Venturi failure 0.054 | Auxiliary engine fuel sensor failure 0.035 | Auxiliary engine fuel sensor failure 0.074 | Piping failure 0.002 | Injection nozzles failure 0.163 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolbot, V.; Theotokatos, G.; Boulougouris, E.; Psarros, G.; Hamann, R. A Novel Method for Safety Analysis of Cyber-Physical Systems—Application to a Ship Exhaust Gas Scrubber System. Safety 2020, 6, 26. https://doi.org/10.3390/safety6020026
Bolbot V, Theotokatos G, Boulougouris E, Psarros G, Hamann R. A Novel Method for Safety Analysis of Cyber-Physical Systems—Application to a Ship Exhaust Gas Scrubber System. Safety. 2020; 6(2):26. https://doi.org/10.3390/safety6020026
Chicago/Turabian StyleBolbot, Victor, Gerasimos Theotokatos, Evangelos Boulougouris, George Psarros, and Rainer Hamann. 2020. "A Novel Method for Safety Analysis of Cyber-Physical Systems—Application to a Ship Exhaust Gas Scrubber System" Safety 6, no. 2: 26. https://doi.org/10.3390/safety6020026
APA StyleBolbot, V., Theotokatos, G., Boulougouris, E., Psarros, G., & Hamann, R. (2020). A Novel Method for Safety Analysis of Cyber-Physical Systems—Application to a Ship Exhaust Gas Scrubber System. Safety, 6(2), 26. https://doi.org/10.3390/safety6020026