
An Investigation of the Fracture Loads Involved in the Framework of Removable Partial Dentures Using Two Types of All-Ceramic Restorations
 , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Model Fabrication
2.2. Crown Fabrication
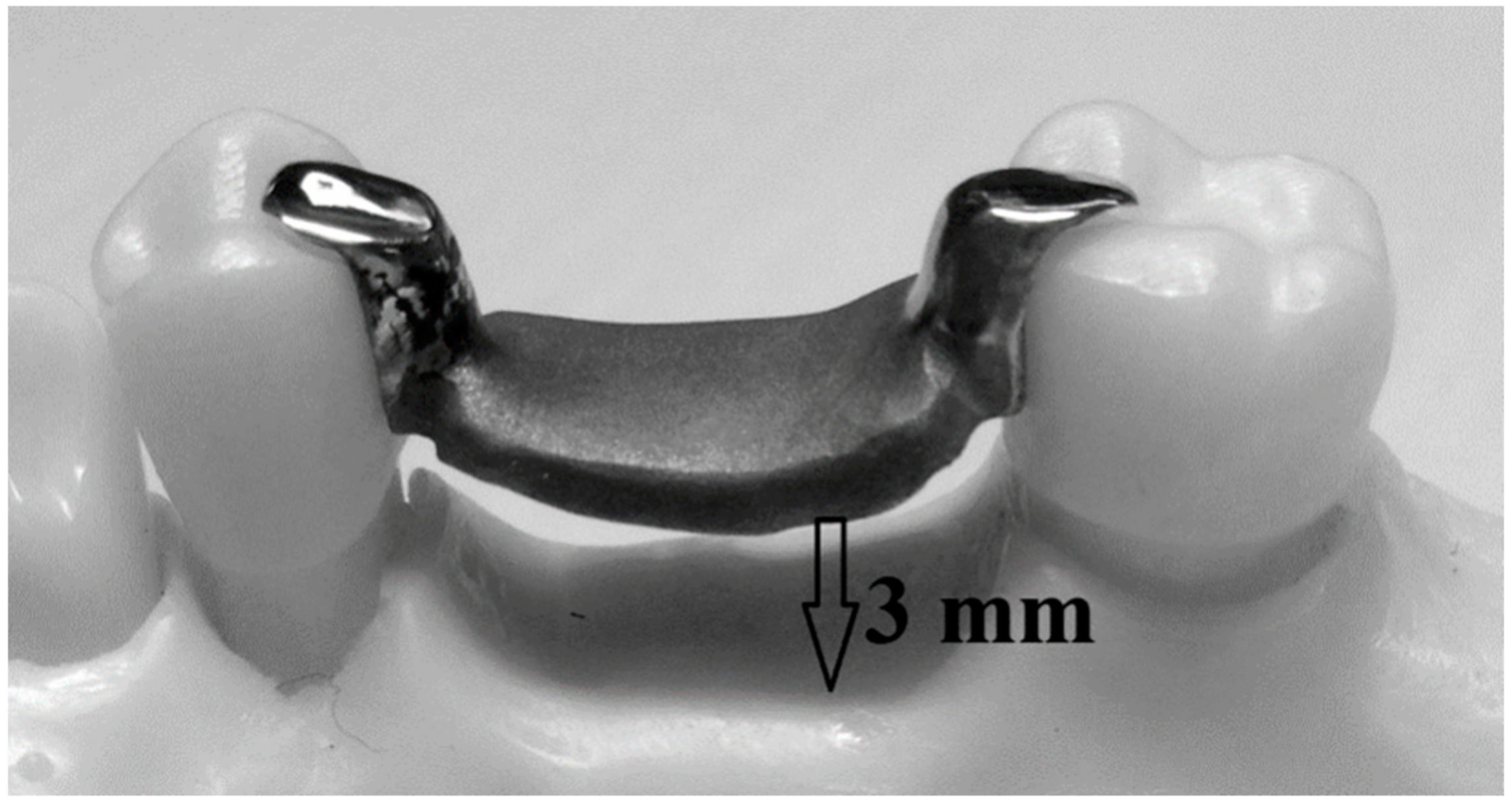
2.3. RPD Framework Fabrication
2.4. Samples Summery
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RPD | Removable partial Denture |
| N | Newtons |
| Co-Cr | Cobalt-chromium |
| CAD/CAM | Computer-aided design/computer-aided manufacturing |
| (PEEK) | Polyetheretherketone |
References
- Rekow, D.; Thompson, V.P. Engineering long term clinical success of advanced ceramic prostheses. J. Mater. Sci. Mater. Med. 2007, 18, 47–56. [Google Scholar] [CrossRef]
- Galeotti, A.; Uomo, R.; Spagnuolo, G.; Paduano, S.; Cimino, R.; Valletta, R.; D’Antò, V. Effect of pH on in vitro biocompatibility of orthodontic miniscrew implants. Prog Orthod. 2013, 14, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milward, P.; Katechia, D.; Morgan, M.Z. Knowledge of removable partial denture wearers on denture hygiene. Br. Dent. J. 2013, 215, E20. [Google Scholar] [CrossRef]
- Temelci, A.; Yılmaz, H.G.; Ünsal, G.; Uyanik, L.O.; Yazman, D.; Ayali, A.; Minervini, G. Investigation of the Wetting Properties of Thalassemia Patients’ Blood Samples on Grade 5 Titanium Implant Surfaces: A Pilot Study. Biomimetics 2023, 8, 25. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Basili, M.; Franco, R.; Bollero, P.; Mancini, M.; Gozzo, L.; Romano, G.L.; Marrapodi, M.M.; Gorassini, F.; D’Amico, C.; et al. Periodontal Disease and Pregnancy: Correlation with Underweight Birth. Eur. J. Dent. 2022. Available online: http://www.thieme-connect.de/DOI/DOI?10.1055/s-0042-1757906 (accessed on 31 January 2023).
- Bohnenkamp, D.M. Removable Partial Dentures: Clinical Concepts. Dent. Clin. North Am. 2014, 58, 69–89. [Google Scholar] [CrossRef]
- Wood, M.R.; Vermilyea, S.G. A review of selected dental literature on evidence-based treatment planning for dental implants: Report of the Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. J. Prosthet. Dent. 2004, 92, 447–462. [Google Scholar] [CrossRef]
- Ikebe, K.; Wada, M.; Kagawa, R.; Maeda, Y. Is old age a risk factor for dental implants? Jpn. Dent. Sci. Rev. 2009, 45, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Minervini, G.; del Mondo, D.; Russo, D.; Cervino, G.; D’Amico, C.; Fiorillo, L. Stem Cells in Temporomandibular Joint Engineering: State of Art and Future Persectives. J. Craniofacial Surg. 2022, 33, 2181–2187. Available online: https://journals.lww.com/10.1097/SCS.0000000000008771 (accessed on 31 January 2023). [CrossRef]
- August, M.; Chung, K.; Chang, Y.; Glowacki, J. Influence of estrogen status on endosseous implant osseointegration. J. Oral Maxillofac. Surg. 2001, 59, 1285–1289. [Google Scholar] [CrossRef]
- Sato, M.; Suzuki, Y.; Kurihara, D.; Shimpo, H.; Ohkubo, C. Effect of implant support on mandibular distal extension removable partial dentures: Relationship between denture supporting area and stress distribution. J. Prosthodont Res. 2013, 57, 109–112. [Google Scholar] [CrossRef]
- Gates, W.D.; Cooper, L.F.; Sanders, A.E.; Reside, G.J.; de Kok, I.J. The effect of implant-supported removable partial dentures on oral health quality of life. Clin. Oral Implant. Res. 2014, 25, 207–213. [Google Scholar] [CrossRef]
- Ganz, S.D. Combination natural tooth and implant-borne removable partial denture: A clinical report. J. Prosthet. Dent. 1991, 66, 1–5. [Google Scholar] [CrossRef]
- Marchack, B.W.; Chen, L.B.; Marchack, C.B.; Futatsuki, Y. Fabrication of an all-ceramic abutment crown under an existing removable partial denture using CAD/CAM technology. J. Prosthet. Dent. 2007, 98, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Cervino, G.; Chaturvedi, S.; Franco, R.; di Francesco, F.; Fiorillo, L.; Cicciù, M. Advanced method of rehabilitating edentulous Jaws: A review on telescopic denture. Technol. Health Care 2023, 3, 1–17. [Google Scholar] [CrossRef]
- Lee, H.; Shirakura, A. A technique to fabricate a cast metal crown for an existing removable partial denture using an acrylic resin template. J. Prosthet. Dent. 2007, 97, 181–182. [Google Scholar] [CrossRef] [PubMed]
- Carracho, J.F.; Razzoog, M.E. Removable partial denture abutments restored with all-ceramic surveyed crowns. Quintessence Int. 2006, 37, 283–288. Available online: https://pubmed.ncbi.nlm.nih.gov/16594359/ (accessed on 29 January 2023). [PubMed]
- Sailer, I.; Pjetursson, B.E.; Zwahlen, M.; Hämmerle, C.H.F. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin. Oral Implant. Res. 2007, 18, 86–96. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Sailer, I.; Zwahlen, M.; Hämmerle, C.H.F. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin. Oral Implant. Res. 2007, 18, 73–85. [Google Scholar] [CrossRef]
- Alshehri, S.A. An Investigation into the Role of Core Porcelain Thickness and Lamination in Determining the Flexural Strength of In-Ceram Dental Materials. J. Prosthodont. 2011, 20, 261–266. [Google Scholar] [CrossRef]
- Sorrentino, R.; De Simone, G.; Tetè, S.; Russo, S.; Zarone, F. Five-year prospective clinical study of posterior three-unit zirconia-based fixed dental prostheses. Clin. Oral Investig 2012, 16, 977–985. Available online: https://link.springer.com/article/10.1007/s00784-011-0575-2 (accessed on 31 January 2023). [CrossRef]
- Wang, X.; Fan, D.; Vincent Swain, M.; Zhao, K. A systematic review of all-ceramic crowns: Clinical fracture rates in relation to restored tooth type. Int. J. Prosthodont. 2012, 25, 441–450. Available online: https://pubmed.ncbi.nlm.nih.gov/22930765/ (accessed on 31 January 2023).
- Rathi, S.; Chaturvedi, S.; Abdullah, S.; Rajput, G.; Alqahtani, N.M.; Chaturvedi, M.; Gurumurthy, V.; Saini, R.; Bavabeedu, S.S.; Minervini, G. Clinical Trial to Assess Physiology and Activity of Masticatory Muscles of Complete Denture Wearer Following Vitamin D Intervention. Medicina 2023, 59, 410. [Google Scholar] [CrossRef] [PubMed]
- Sornsuwan, T.; Swain, M.V. Influence of occlusal geometry on ceramic crown fracture; role of cusp angle and fissure radius. J. Mech. Behav. Biomed. Mater. 2011, 4, 1057–1066. [Google Scholar] [CrossRef] [PubMed]
- Rekow, E.D.; Harsono, M.; Janal, M.; Thompson, V.P.; Zhang, G. Factorial analysis of variables influencing stress in all-ceramic crowns. Dent. Mater. 2006, 22, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Land, M.F.; Hopp, C.D. Survival Rates of All-Ceramic Systems Differ by Clinical Indication and Fabrication Method. J. Evid. Based Dent. Pract. 2010, 10, 37–38. [Google Scholar] [CrossRef] [PubMed]
- Nishigawa, K.; Bando, E.; Nakano, M. Quantitative study of bite force during sleep associated bruxism. J. Oral Rehabil. 2001, 28, 485–491. [Google Scholar] [CrossRef]
- Varga, S.; Spalj, S.; Lapter Varga, M.; Anic Milosevic, S.; Mestrovic, S.; Slaj, M. Maximum voluntary molar bite force in subjects with normal occlusion. Eur. J. Orthod. 2011, 33, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Braun, S.; Hnat, W.P.; Freudenthaler, J.W.; Marcotte, M.R.; Hönigle, K.; Johnson, B.E. A study of maximum bite force during growth and development. Angle Orthod. 1996, 66, 261–264. [Google Scholar]
- Helkimo, E.; Carlsson, G.E.; Helkimo, M. Chewing efficiency and state of dentition. Acta Odontol Scand 1978, 36, 33–41. Available online: http://www.tandfonline.com/doi/full/10.3109/00016357809026364 (accessed on 29 January 2023). [CrossRef]
- Miyaura, K.; Morita, M.; Matsuka, Y.; Yamashita, A.; Watanabe, T. Rehabilitation of biting abilities in patients with different types of dental prostheses. J. Oral Rehabil. 2000, 27, 1073–1076. [Google Scholar] [CrossRef]
- Rao, S.; Chowdhary, R. Comparison of Fracture Toughness of All-Ceramic and Metal–Ceramic Cement Retained Implant Crowns: An In Vitro Study. J. Indian Prosthodont. Soc. 2014, 14, 408–414. [Google Scholar] [CrossRef]
- Lundgren, D.; Laurell, L. Occlusal force pattern during chewing and biting in dentitions restored with fixed bridges of cross-arch extension. J. Oral Rehabil. 1986, 13, 191–203. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1365-2842.1986.tb00651.x (accessed on 31 January 2023). [CrossRef]
- Jang, G.W.; Kim, H.S.; Choe, H.C.; Son, M.K. Fracture Strength and Mechanism of Dental Ceramic Crown with Zirconia Thickness. Procedia Eng. 2011, 10, 1556–1560. [Google Scholar] [CrossRef] [Green Version]
- Cicciù, M.; Fiorillo, L.; D’Amico, C.; Gambino, D.; Amantia, E.M.; Laino, L.; Crimi, S.; Campagna, P.; Bianchi, A.; Herford, A.S.; et al. 3D digital impression systems compared with traditional techniques in dentistry: A recent data systematic review. Materials 2020, 13, 1982. [Google Scholar] [CrossRef] [PubMed]
- Skouridou, N.; Pollington, S.; Rosentritt, M.; Tsitrou, E. Fracture strength of minimally prepared all-ceramic CEREC crowns after simulating 5 years of service. Dent. Mater. 2013, 29, e70–e77. [Google Scholar] [CrossRef]
- Vaddamanu, S.K.; Alhamoudi, F.H.; Chaturvedi, S.; Alqahtani, N.M.; Addas, M.K.; Alfarsi, M.A.; Vyas, R.; Kanji, M.A.; Zarbah, M.A.; Alqahtani, W.M.; et al. Retentive Forces and Deformation of Fitting Surface in RPD Clasp Made of Polyether-Ether-Ketone (PEEK). Polymers 2023, 15, 956. [Google Scholar] [CrossRef]
- Nordahl, N.; von Steyern, P.V.; Larsson, C. Fracture strength of ceramic monolithic crown systems of different thickness. J. Oral Sci. 2015, 57, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z.; Kattadiyil, M.T. Comparison of denture base adaptation between CAD-CAM and conventional fabrication techniques. J. Prosthet Dent. 2016, 116, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Shindoi, N.; Koretake, K.; Hosokawa, R. The effect of occlusal rest size and shape on yield strength. J. Prosthet Dent. 2003, 89, 503–507. [Google Scholar] [CrossRef]
- Gapido, C.G.; Kobayashi, H.; Miyakawa, O.; Kohno, S. Fatigue resistance of cast occlusal rests using Co-Cr and Ag-Pd-Cu-Au alloys. J. Prosthet Dent. 2003, 90, 261–269. [Google Scholar] [CrossRef]
- Wu, J.C.; Latta, G.H.; Wicks, R.A.; Swords, R.L.; Scarbecz, M. In vitro deformation of acetyl resin and metal alloy removable partial denture direct retainers. J. Prosthet Dent. 2003, 90, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Swain, M.V. Unstable cracking (chipping) of veneering porcelain on all-ceramic dental crowns and fixed partial dentures. Acta Biomater. 2009, 5, 1668–1677. [Google Scholar] [CrossRef]
- Di Francesco, F.; Lanza, A.; Di Blasio, M.; Vaienti, B.; Cafferata, E.A.; Cervino, G.; Cicciù, M.; Minervini, G. Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs). Appl. Sci. 2022, 12, 12409. [Google Scholar] [CrossRef]
- Minervini, G.; D’Amico, C.; Cicciù, M.; Fiorillo, L. Temporomandibular Joint Disk Displacement: Etiology, Diagnosis, Imaging, and Therapeutic Approaches. J. Craniofac. Surg 2022. Nov 4. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciù, M.; Laino, L. Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis. Cranio 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Qazi, N.; Pawar, M.; Padhly, P.P.; Pawar, V.; Mehta, V.; D’Amico, C.; Nicita, F.; Fiorillo, L.; Alushi, A.; Minervini, G.; et al. Teledentistry: Evaluation of Instagram posts related to Bruxism. Technol. Health Care 2023, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Crescente, G.; Minervini, G.; Spagnuolo, C.; Moccia, S. Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain. Molecules 2022, 28, 106. [Google Scholar] [CrossRef]
- della Bona, A.; Kelly, J.R. The Clinical Success of All-Ceramic Restorations. J. Am. Dent. Assoc. 2008, 139 (Suppl. S9), S8–S13. [Google Scholar] [CrossRef] [Green Version]
- Burke, F.J.; Fleming, G.J.; Nathanson, D.; Marquis, P.M. Are adhesive technologies needed to support ceramics? An assessment of the current evidence. J. Adhes Dent. 2002, 4, 7–22. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Type of Material | Quantity |
|---|---|---|
| models | Model resin | 20 |
| crowns | 30 zirconia | 20 |
| crowns | 30 IPS e.max Press | 20 |
| RPD frameworks | Chrome-cobalt alloy | 20 |
| Sample No | RPD with Zirconia | RPD with IPS e.max Press |
|---|---|---|
| 1 | 335 N | 284 N |
| 2 | 305 N | 273 N |
| 3 | 386 N | 244 N |
| 4 | 313 N | 346 N |
| 5 | 400 N | 374 N |
| 6 | 367 N | 323 N |
| 7 | 376 N | 174 N |
| 8 | 206 N | 203 N |
| 9 | 312 N | 293 N |
| 10 | 304 N | 303 N |
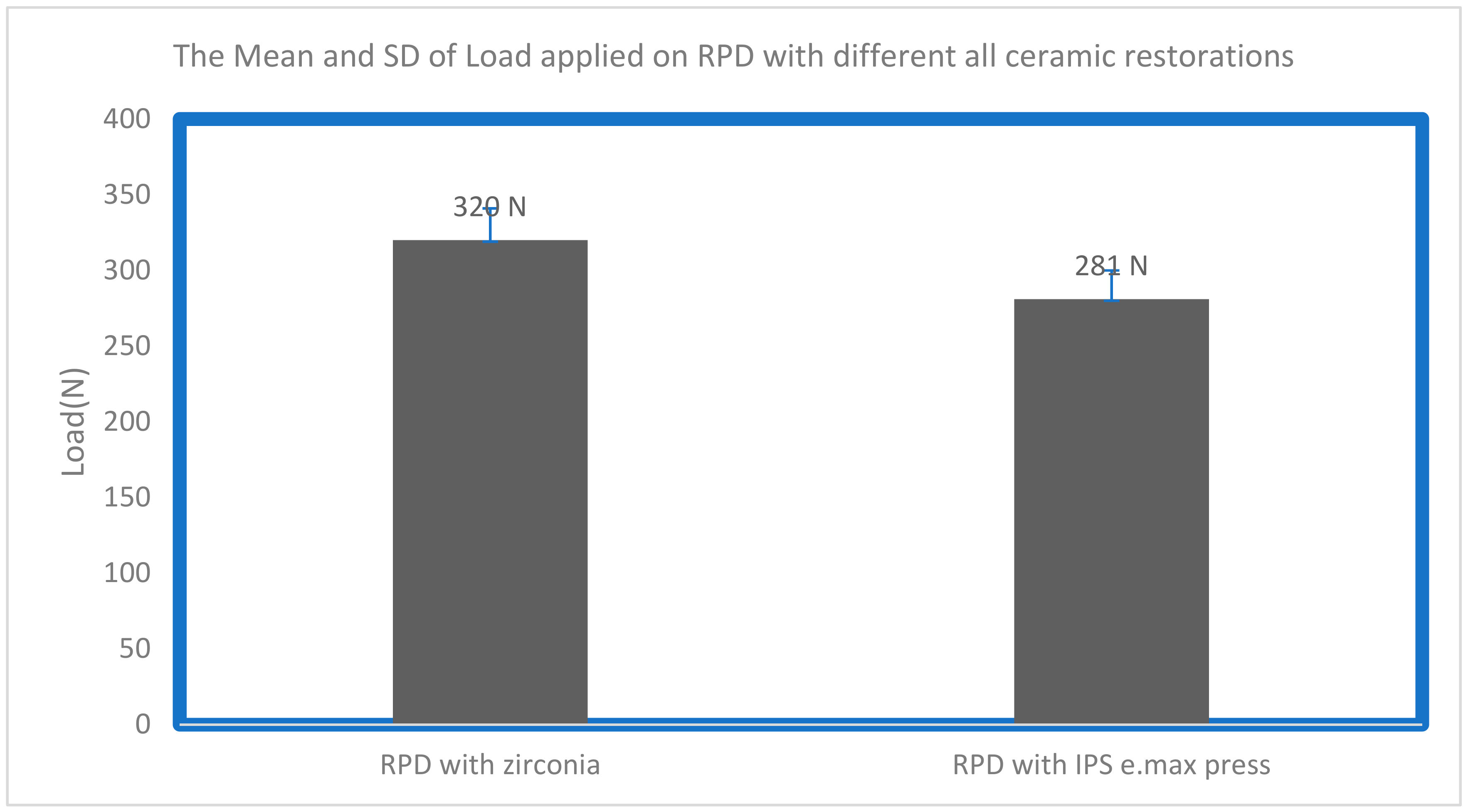
| mean | 320 N | 281 N |
| Standard deviation | ±21 N | ±19 N |
| Sample No | Zirconia | RPD with Zirconia |
|---|---|---|
| 1 | 3020 N | 335 N |
| 2 | 2949 N | 305 N |
| 3 | 3405 N | 386 N |
| 4 | 3353 N | 313 N |
| 5 | 3275 N | 400 N |
| 6 | 3277 N | 367 N |
| 7 | 2248 N | 376 N |
| 8 | 2402 N | 206 N |
| 9 | 2427 N | 312 N |
| 10 | 3184 N | 304 N |
| mean | 2954 N | 320 N |
| Standard deviation | ±320 N | ±21 N |
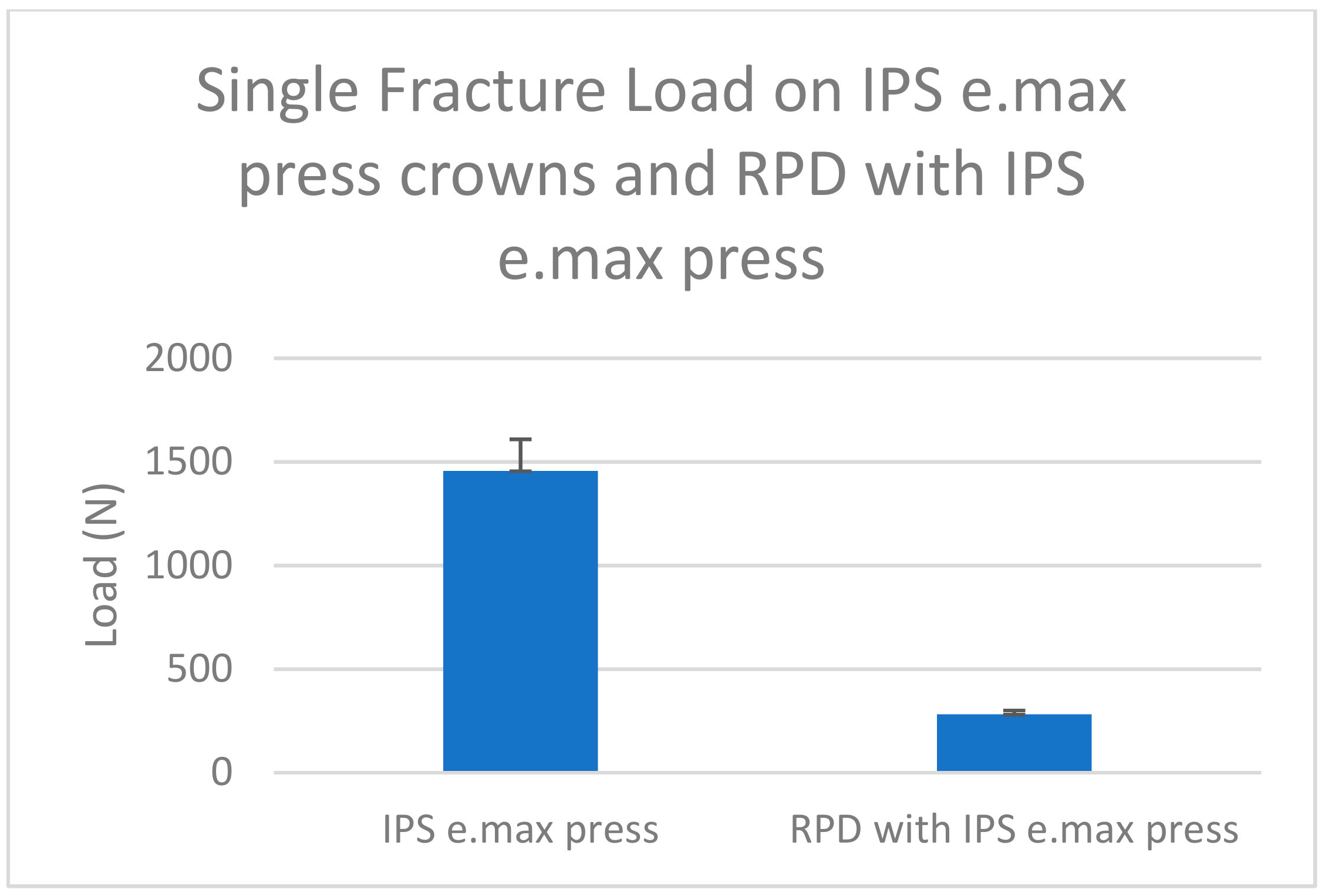
| Sample No | IPS e.max Press | RPD with IPS e.max Press |
|---|---|---|
| 1 | 1593 N | 284 N |
| 2 | 2080 N | 273 N |
| 3 | 1378 N | 244 N |
| 4 | 1350 N | 346 N |
| 5 | 730 N | 374 N |
| 6 | 2265 N | 323 N |
| 7 | 955 N | 174 N |
| 8 | 1295 N | 203 N |
| 9 | 1123 N | 293 N |
| 10 | 1788 N | 303 N |
| mean | 1456 N | 281 N |
| Standard deviation | ±153 N | ±19 N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhamoudi, F.H.; Aldosari, L.I.N.; Alshadidi, A.A.F.; Hassan, S.A.B.; Alwadi, M.A.M.; Vaddamanu, S.K.; Cicciù, M.; Minervini, G. An Investigation of the Fracture Loads Involved in the Framework of Removable Partial Dentures Using Two Types of All-Ceramic Restorations. Biomimetics 2023, 8, 113. https://doi.org/10.3390/biomimetics8010113
Alhamoudi FH, Aldosari LIN, Alshadidi AAF, Hassan SAB, Alwadi MAM, Vaddamanu SK, Cicciù M, Minervini G. An Investigation of the Fracture Loads Involved in the Framework of Removable Partial Dentures Using Two Types of All-Ceramic Restorations. Biomimetics. 2023; 8(1):113. https://doi.org/10.3390/biomimetics8010113
Chicago/Turabian StyleAlhamoudi, Fahad Hussain, Lujain Ibrahim N. Aldosari, Abdulkhaliq Ali F. Alshadidi, Saeed Awod Bin Hassan, Maram Ali M. Alwadi, Sunil Kumar Vaddamanu, Marco Cicciù, and Giuseppe Minervini. 2023. "An Investigation of the Fracture Loads Involved in the Framework of Removable Partial Dentures Using Two Types of All-Ceramic Restorations" Biomimetics 8, no. 1: 113. https://doi.org/10.3390/biomimetics8010113
APA StyleAlhamoudi, F. H., Aldosari, L. I. N., Alshadidi, A. A. F., Hassan, S. A. B., Alwadi, M. A. M., Vaddamanu, S. K., Cicciù, M., & Minervini, G. (2023). An Investigation of the Fracture Loads Involved in the Framework of Removable Partial Dentures Using Two Types of All-Ceramic Restorations. Biomimetics, 8(1), 113. https://doi.org/10.3390/biomimetics8010113