Newborn Screening for Selected Disorders in Nepal: A Pilot Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Birth Weight Statistics
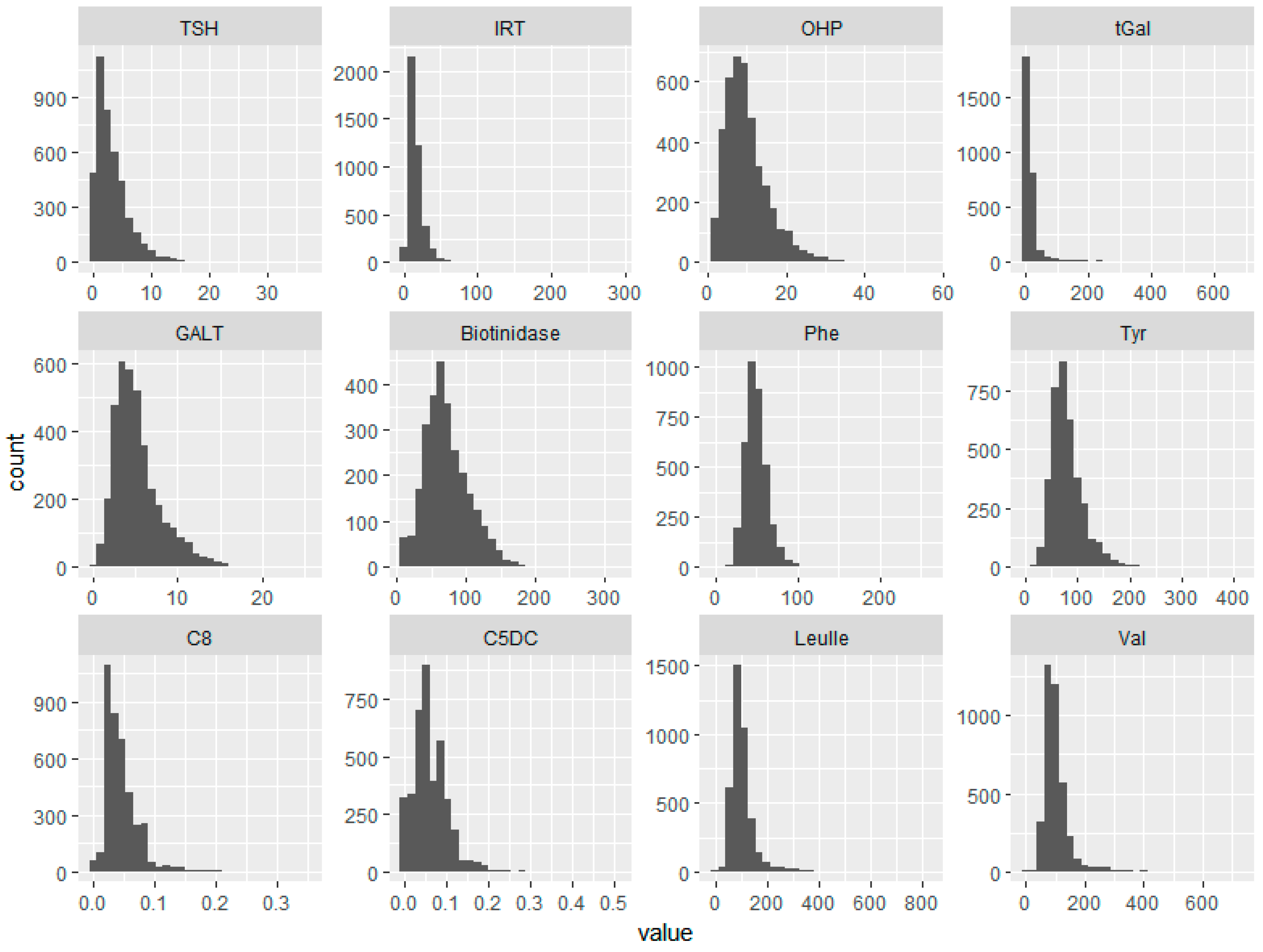
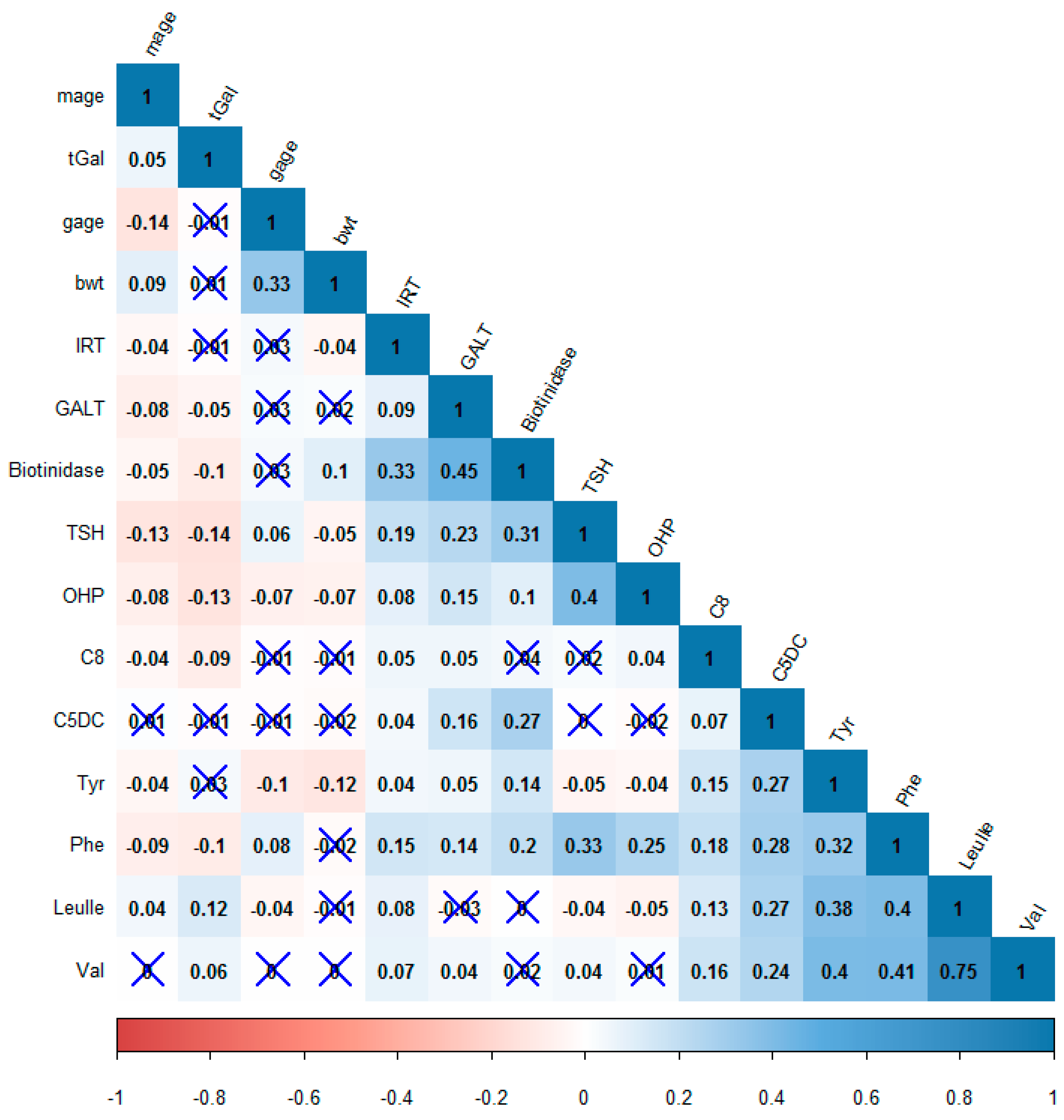
3.2. Overview of Analytes
3.3. Gestational Age
3.4. Biotinidase
3.5. IRT
3.6. OHP
3.7. TSH
3.8. Galactose
3.9. Amino Acids
3.10. Carnitines
4. Discussion
4.1.TSH
4.2. OHP
4.3. IRT
4.4. Galactose, GALT, and Biotidinase
4.5. Amino Acids
4.6. Implications for Nepal
5. Limitations of Study
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lanpher, B.; Brunetti-Pierri, N.; Lee, B. Inborn Errors of Metabolism: The Flux from Mendelian to Complex Diseases. Nat. Rev. Genet. 2006, 7, 449–460. [Google Scholar] [CrossRef] [PubMed]
- WHO | ICD-11 Revision. Available online: http://www.who.int/classifications/icd/revision/en/ (accessed on 19 March 2019).
- Central Bureau of Statistics. National Population and Housing Census 2011 Vol. 2; Government of Nepal: Kathmandu, Nepal, 2012. Available online: http://mofald.gov.np/mofald/userfiles/docs_206.pdf (accessed on 25 March 2019).
- A Survey of the Nepali People in 2017—Infographics. The Asia Foundation. Available online: https://asiafoundation.org/publication/survey-nepali-people-2017-infographics/ (accessed on 21 March 2019).
- Modiano, G.; Morpurgo, G.; Terrenato, L.; Novelletto, A.; di Rienzo, A.; Colombo, B.; Purpura, M.; Mariani, M.; Santachiara-Benerecetti, S.; Brega, A. Protection against Malaria Morbidity: Near-Fixation of the α-Thalassemia Gene in a Nepalese Population. Am. J. Hum. Genet. 1991, 48, 390–397. [Google Scholar] [PubMed]
- Das, R.N.; Shetty, K.J.; Dham, S.K. A Man with Pigmented Skin, Dark Urine and Arthritis: What Is Your Diagnosis? APLAR J. Rheumatol. 2005, 8, 131–134. [Google Scholar] [CrossRef]
- Khatiwada, B.; Pokharel, A. Lysosomal Storage Disease. JNMA J. Nepal Med. Assoc. 2009, 48, 242–245. [Google Scholar] [CrossRef]
- Malla, K.K.; Malla, T.; Basnet, S.; Rao, K.S.; Tiwari, P.K.; Ghosh, A.; Kc, N. Morquio Syndrome in Two Siblings: A Case Report. J. Nepal Paediatr. Soc. 2011, 31, 68–71. [Google Scholar] [CrossRef]
- Karki, S.T.; Rai, G.K.; Karki, B.B.; Gurung, R. Clinico-Aetiological Profile of Congenital Hypothyroidism. J. Nepal Paediatr. Soc. 2016, 36, 126–130. [Google Scholar] [CrossRef]
- Shreevastava, N.K.; Pandey, A.S. Screening Mentally Retarded Children for Inborn Errors of Metabolism. J. Nepal Health Res. Counc. 2017, 15, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Karki, K.B.; Aryal, K.K.; Thapa, P.; Dhimal, M.; Bista, B.; Joshi, A.; Poudyal, A.; Dhakal, P. Anemia and Its Determinants among Women of Reproductive Age in Mid–Western Tarai of Nepal, 2015; Nepal Health Research Council: Kathmandu, Nepal, 2016; p. 23. Available online: http://nhrc.gov.np/wp-content/uploads/2017/06/ANEMIA-REPORT-book.pdf (accessed on 25 March 2019).
- Jha, R. Distribution of Hemoglobinopathies in Patients Presenting for Electrophoresis and Comparison of Result with High Performance Liquid Chromatography. J. Pathol. Nepal 2015, 5, 850–858. [Google Scholar] [CrossRef]
- Sakai, Y.; Kobayashi, S.; Shibata, H.; Furuumi, H.; Endo, T.; Fucharoen, S.; Hamano, S.; Acharya, G.P.; Kawasaki, T.; Fukumaki, Y. Molecular Analysis of α-Thalassemia in Nepal: Correlation with Malaria Endemicity. J. Hum. Genet. 2000, 45, 127. [Google Scholar] [CrossRef] [PubMed]
- Burton, B.K. Inborn Errors of Metabolism in Infancy: A Guide to Diagnosis. Pediatrics 1998, 102, e69. [Google Scholar] [CrossRef] [PubMed]
- Saudubray, J.-M.; Garcia-Cazorla, À. Inborn Errors of Metabolism Overview: Pathophysiology, Manifestations, Evaluation, and Management. Pediatr. Clin. N. Am. 2018, 65, 179–208. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Population, Nepal; New Era. Nepal Demographic and Health Survey 2016; Ministry of Health and Population: Kathmandu, Nepal, 2017. Available online: https://www.dhsprogram.com/pubs/pdf/fr336/fr336.pdf (accessed on 25 March 2019).
- GHO | By Country | Switzerland—Statistics Summary (2002—Present). Available online: http://apps.who.int/gho/data/node.country.country-CHE (accessed on 19 March 2019).
- Newborn Screening. Available online: http://www.Neoscreening.Ch/Display.Cfm/Id/100489/Disp_type/Dmssimple/PageID/80690.Pdf80690.Pdf (accessed on 25 March 2019).
- R Core Team. R: A Language and Environment for Statistical Computing; Version 3.4.2; [Computer Software]; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Wei, T.L.M.; Simko, V. R Package “Corrplot”: Visualization of a Correlation Matrix (Version 0.84). 2017. Available online: https://github.com/taiyun/corrplot (accessed on 19 March 2019).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Use R! Springer: New York, NY, USA, 2009. [Google Scholar]
- Government of Nepal. Statistical Year Book; Central Bureau of Statistics: Kathmandu, Nepal, 2015.
- Bista, D. People of Nepal, 7th ed.; Ratna Pustak Bhandar: Kathmandu, Nepal, 2000. [Google Scholar]
- VanVleck, N.; Wolf, B.; Seeterlin, M.; Monaghan, K.G.; Stanley, E.; Hawkins, H.; Taffe, B. Improved Identification of Partial Biotinidase Deficiency by Newborn Screening Using Age-Related Enzyme Activity Cutoffs: Reduction of the False-Positive Rate. Int. J. Neonatal Screen. 2015, 1, 45–56. [Google Scholar] [CrossRef]
- The State of the World’s Children 2016 Statistical Tables. Available online: https://data.unicef.org/resources/state-worlds-children-2016-statistical-tables/ (accessed on 19 March 2019).
- Brosnan, J.T.; Brosnan, M.E. Branched-Chain Amino Acids: Enzyme and Substrate Regulation. J. Nutr. 2006, 136, 207S–211S. [Google Scholar] [CrossRef]
- Lee, S.Y. Perinatal Factors Associated with Neonatal Thyroid-Stimulating Hormone in Normal Newborns. Ann. Pediatr. Endocrinol. Metab. 2016, 21, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Räihä, N.C.R. Biochemical Basis for Nutritional Management of Preterm Infants. Pediatrics 1974, 53, 147–156. [Google Scholar] [PubMed]
- Büyükgebiz, A. Newborn Screening for Congenital Hypothyroidism. J. Clin. Res. Pediatr. Endocrinol. 2013, 5, S8–S12. [Google Scholar] [CrossRef]
- Corbetta, C.; Weber, G.; Cortinovis, F.; Calebiro, D.; Passoni, A.; Vigone, M.C.; Beck-Peccoz, P.; Chiumello, G.; Persani, L. A 7-Year Experience with Low Blood TSH Cutoff Levels for Neonatal Screening Reveals an Unsuspected Frequency of Congenital Hypothyroidism (CH). Clin. Endocrinol. 2009, 71, 739–745. [Google Scholar] [CrossRef]
- Kapoor, S.; Thelma, B.K. Status of Newborn Screening and Inborn Errors of Metabolism in India. Indian J. Pediatr. 2018, 85, 1110–1117. [Google Scholar] [CrossRef]
- Khatiwada, S.; Gelal, B.; Gautam, S.; Lamsal, M.; Baral, N. Iodine Status among School Children of Remote Hilly Regions of Nepal. Indian Pediatr. 2015, 52, 436–437. [Google Scholar] [PubMed]
- Upadhyaya, T.L.; Kc, A.; Paudel, S. Prevalence and Complications of Hypothyroidism during Pregnancy in Western Nepal. Nepal J. Med. Sci. 2014, 3, 48–50. [Google Scholar] [CrossRef]
- Chaudhary, L.N.; Khatiwada, S.; Gelal, B.; Gautam, S.; Lamsal, M.; Pokharel, H.; Baral, N. Iodine and Thyroid Function Status, and Anti-Thyroid Peroxidase Antibody among Pregnant Women in Eastern Nepal. J. Nepal Health Res. Counc. 2017, 15, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, G.; Faure, C.; Brondi, M.F.; Vallejos, C.; Soares, D.; Oliveira, É.; Brito, V.N.; Mendonca, B.B.; Bachega, T.A.S.S. Weight-Adjusted Neonatal 17OH-Progesterone Cutoff Levels Improve the Efficiency of Newborn Screening for Congenital Adrenal Hyperplasia. Arq. Bras. Endocrinol. AMP Metab. 2011, 55, 632–637. [Google Scholar] [CrossRef]
- Pearce, M.; DeMartino, L.; McMahon, R.; Hamel, R.; Maloney, B.; Stansfield, D.-M.; McGrath, E.C.; Occhionero, A.; Gearhart, A.; Caggana, M.; et al. Newborn Screening for Congenital Adrenal Hyperplasia in New York State. Mol. Genet. Metab. Rep. 2016, 7, 1–7. [Google Scholar] [CrossRef]
- Pant, V.; Baral, S.; Shrestha, B.; Tumbapo, A. A child with hypertension and ambiguous genitalia—An uncommon variant of congenital adrenal hyperplasia: A case report. J. Med. Case Rep. 2017, 11, 168. [Google Scholar] [CrossRef] [PubMed]
- Regmi, E. Stories of Intersex People from Nepal. Available online: https://ihra.org.au/wp-content/uploads/2016/04/Intersex-Stories-in-Nepal.pdf (accessed on 25 March 2019).
- Massie, J.; Curnow, L.; Tzanakos, N.; Francis, I.; Robertson, C.F. Markedly Elevated Neonatal Immunoreactive Trypsinogen Levels in the Absence of Cystic Fibrosis Gene Mutations Is Not an Indication for Further Testing. Arch. Dis. Child. 2006, 91, 222–225. [Google Scholar] [CrossRef]
- Lecoq, I.; Brouard, J.; Laroche, D.; Férec, C.; Travert, G. Blood Immunoreactive Trypsinogen Concentrations Are Genetically Determined in Healthy and Cystic Fibrosis Newborns. Acta Paediatr. 1999, 88, 338–341. [Google Scholar] [CrossRef]
- Siegel, C.D.; Sparks, J.W.; Battaglia, F.C. Patterns of Serum Glucose and Galactose Concentrations in Term Newborn Infants after Milk Feeding. Neonatology 1988, 54, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Segal, S.; Blair, A. Some Observations on the Metabolism of d-Galactose in Normal Man. J. Clin. Investig. 1961, 40, 2016–2025. [Google Scholar] [CrossRef] [PubMed]
- Slupsky, C.M.; He, X.; Hernell, O.; Andersson, Y.; Rudolph, C.; Lönnerdal, B.; West, C.E. Postprandial Metabolic Response of Breast-Fed Infants and Infants Fed Lactose-Free vs Regular Infant Formula: A Randomized Controlled Trial. Sci. Rep. 2017, 7, 3640. [Google Scholar] [CrossRef]
- Koletzko, B.; Baker, S.; Cleghorn, G.; Neto, U.F.; Gopalan, S.; Hernell, O.; Hock, Q.S.; Jirapinyo, P.; Lonnerdal, B.; Pencharz, P.; et al. Global Standard for the Composition of Infant Formula: Recommendations of an ESPGHAN Coordinated International Expert Group. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 584–599. [Google Scholar] [CrossRef]
- Cavell, B. Gastric Emptying in Infants Fed Human Milk or Infant Formula. Acta Paediatr. Scand. 1981, 70, 639–641. [Google Scholar] [CrossRef] [PubMed]
- Population Based Screening of Sickle Cell Disorder in Tharu Community of Bardiya District, Nepal (Updated on June 21, 2018)—Nepal Health Research Council. Available online: http://nhrc.gov.np/projects/prevalence-of-sickle-cell-disease-in-tharu-community-of-bardiya-district-nepal/ (accessed on 19 March 2019).
- Lobitz, S.; Telfer, P.; Cela, E.; Allaf, B.; Angastiniotis, M.; Backman Johansson, C.; Badens, C.; Bento, C.; Bouva, M.J.; Canatan, D.; et al. Newborn Screening for Sickle Cell Disease in Europe: Recommendations from a Pan-European Consensus Conference. Br. J. Haematol. 2018, 183, 648–660. [Google Scholar] [CrossRef] [PubMed]
- Shook, L.M.; Ware, R.E. Effective Screening Leads to Better Outcomes in Sickle Cell Disease. Arch. Dis. Child. 2018, 103, 628–630. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Range | mean | SD | Percentiles | |||
|---|---|---|---|---|---|---|---|
| Nepalese | Swiss | ||||||
| 1st | 99th | 1st | 99th | ||||
| Gestational age | 27–44 | 38.99 | 1.68 | 33 | 42 | * | * |
| Birth weight (g) | 815–5515 | 2975.82 | 442.70 | 1902.2 | 3957.25 | 1195 | 4420 |
| Mother’s age (years) | 15–45 | 24.95 | 4.61 | 17 | 39 | * | * |
| TSH (mIU/mL) | 0–230 | 3.33 | 2.84 | 0.1 | 13.1 | 0.30 | 6.30 |
| IRT (μg/L) | 0.1–290.9 | 16.81 | 12.67 | 3 | 63.3 | 5.8 | 49.0 |
| OHP (nmol/L) | 1–55.5 | 10.08 | 5.68 | 2 | 28.9 | 1.6 | 14.5 |
| tGal (μmol/L) | 0–680.4 | 24.23 | 56.56 | 0 | 312.87 | 0 | 532.7 |
| GALT (U/dl) | 0–25.2 | 5.30 | 2.84 | 1.1 | 14.3 | 5.9 | 22.7 |
| Biotinidase (U) | 6.8–315.8 | 72.72 | 32.18 | 11 | 157.50 | 100.2 | 353.9 |
| Phe (μmol/L) | 0–259.6 | 50.39 | 14.57 | 25.08 | 90.63 | 25.7 | 69.2 |
| Tyr (μmol/L) | 6.95–420.73 | 80.35 | 31.76 | 31.68 | 182.67 | 28.5 | 206.1 |
| C8 (μmol/L) | 0–4.03 | 0.050 | 0.07 | 0 | 0.17 | 0.00 | 0.14 |
| C5DC (μmol/L) | 0–3.62 | 0.064 | 0.07 | 0 | 0.21 | 0.02 | 0.21 |
| Leu/Ile (μmol/L) | 0–1499.16 | 106.43 | 55.60 | 42.36 | 312.53 | 71.5 | 255.1 |
| Val (μmol/L) | 0–2578.74 | 104.63 | 67.53 | 44.35 | 320.03 | 56.6 | 245.9 |
| Variable | W | Difference in Location | p-Value | Confidence Interval (95%) | Mean | |
|---|---|---|---|---|---|---|
| ≥36 weeks | <36 weeks | |||||
| Birth weight (g) | 387,580 | 530 | <0.001 | 450, 615 | 2993.7 | 2449.09 |
| Mother’s age (years) | 173,840 | −1.00 | 0.0147 | −2.16, 0.00003 | 24.91 | 26.1 |
| TSH (mIU/L) | 254,590 | 0.40 | 0.017 | −0.099, 0.799 | 3.26 | 2.88 |
| IRT (μg/L) | 249,790 | 1.299 | 0.031 | −0.1, 2.499 | 16.58 | 15.50 |
| OHP (nmol/L) | 199,820 | −0.999 | 0.042 | −1.9, 0 | 9.94 | 11.42 |
| tGal (μmol/L) | 111,950 | 0.599 | 0.358 | −0.699, 2.20 | 24.79 | 18.03 |
| GALT (U) | 182,070 | 0.099 | 0.654 | −0.299, 0.499 | 5.04 | 4.71 |
| Biotinidase (U) | 92,178 | 3.90 | 0.188 | −1.90, −9.99 | 68.83 | 63.52 |
| Phe (μmol/L) | 171,240 | 1.01 | 0.425 | −1.48, 3.52 | 50.05 | 48.83 |
| Tyr (μmol/L) | 141,630 | −12.99 | <0.001 | −20.23, −6.02 | 79.09 | 94.60 |
| C8 (μmol/L) | 170,950 | −0.01 | 0.007 | −0.01, −0.00005 | 0.05 | 0.06 |
| C5DC (μmol/L) | 197,350 | 0 | 0.813 | −0.01, 0.01 | 0.062 | 0.07 |
| Leu/Ile (μmol/L) | 180,800 | −5.86 | 0.080 | −12.51, 0.72 | 106.45 | 114.83 |
| Val (μmol/L) | 188,490 | −3.27 | 0.290 | −9.53, 2.86 | 104.67 | 107.48 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma Pandey, A.; Joshi, S.; Rajbhandari, R.; Kansakar, P.; Dhakal, S.; Fingerhut, R. Newborn Screening for Selected Disorders in Nepal: A Pilot Study. Int. J. Neonatal Screen. 2019, 5, 18. https://doi.org/10.3390/ijns5020018
Sharma Pandey A, Joshi S, Rajbhandari R, Kansakar P, Dhakal S, Fingerhut R. Newborn Screening for Selected Disorders in Nepal: A Pilot Study. International Journal of Neonatal Screening. 2019; 5(2):18. https://doi.org/10.3390/ijns5020018
Chicago/Turabian StyleSharma Pandey, Arti, Suchita Joshi, Rateena Rajbhandari, Prerana Kansakar, Sadichhya Dhakal, and Ralph Fingerhut. 2019. "Newborn Screening for Selected Disorders in Nepal: A Pilot Study" International Journal of Neonatal Screening 5, no. 2: 18. https://doi.org/10.3390/ijns5020018
APA StyleSharma Pandey, A., Joshi, S., Rajbhandari, R., Kansakar, P., Dhakal, S., & Fingerhut, R. (2019). Newborn Screening for Selected Disorders in Nepal: A Pilot Study. International Journal of Neonatal Screening, 5(2), 18. https://doi.org/10.3390/ijns5020018