
The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts




Abstract
:1. Introduction
2. Materials and Methods
2.1. Newborn Screening Translational Research Network
2.2. Development of Common Data Elements (CDEs)
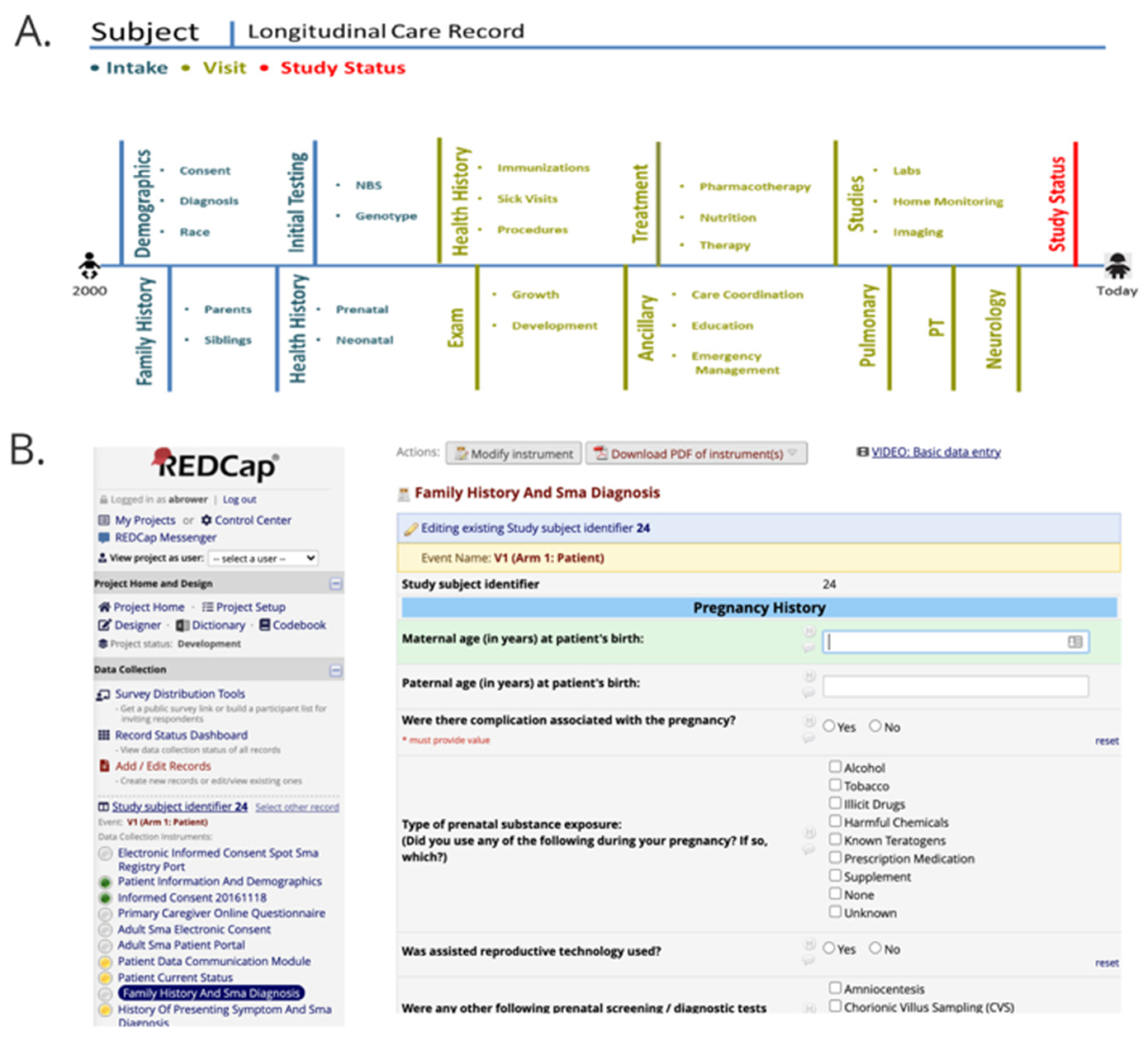
2.3. Longitudinal Pediatric Data Resource
3. Results
3.1. CDE Sets
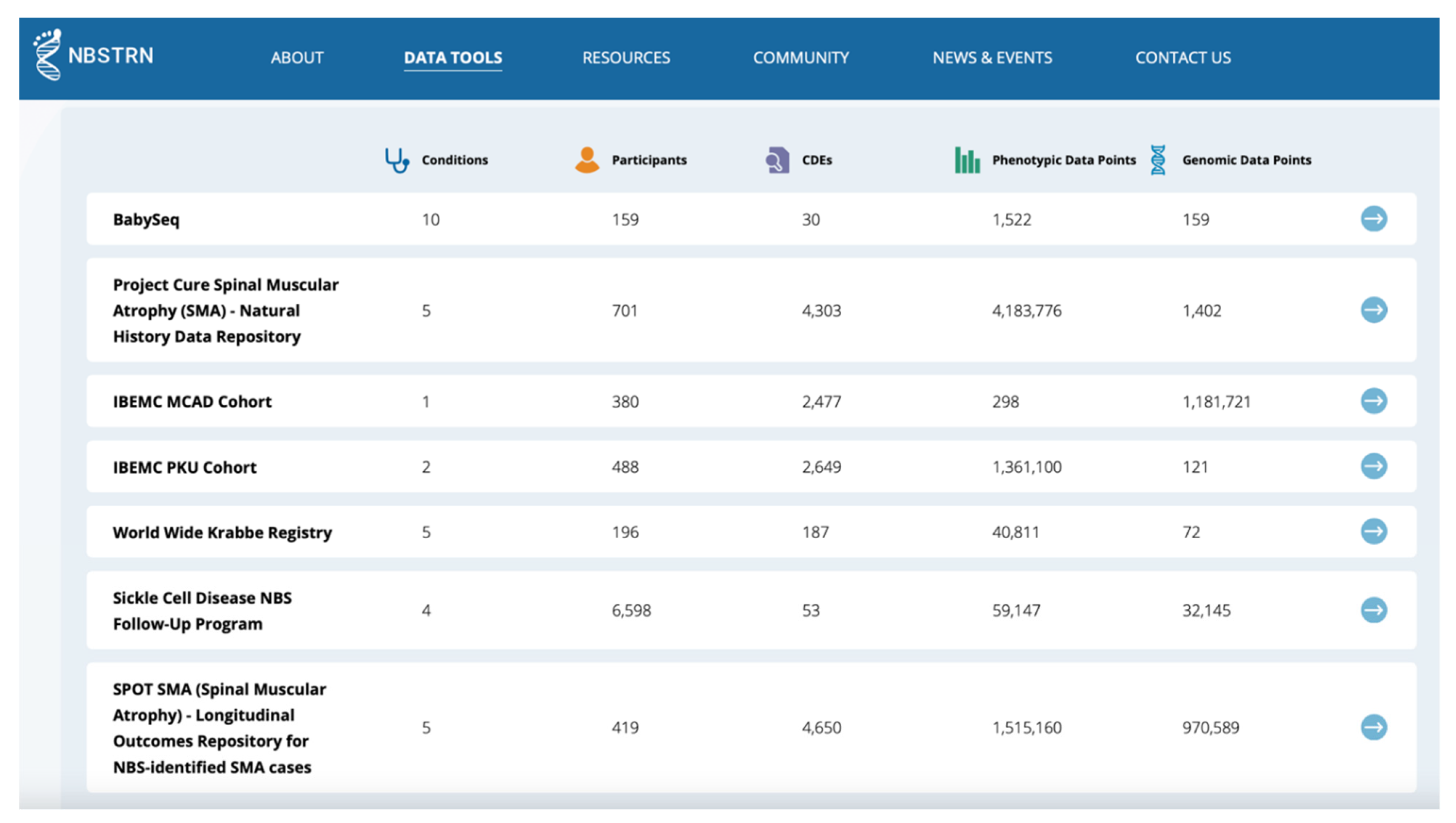
3.2. LPDR: Phenotypic and Genomic Data
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
List of 118 Conditions with CDE Sets
References
- Advisory Committee on Heritable Disorders in Newborns and Children. Recommended Uniform Screening Panel. Available online: https://www.hrsa.gov/advisorycommittees/mchbadvisory/heritabledisorders/recommendedpanel/index.html (accessed on 12 April 2021).
- Lloyd-Puryear, M.A.; Brower, A.M. Long-term follow-up in newborn screening: A systems approach for improving health outcomes. Genet. Med. 2010, 12, S256–S260. [Google Scholar] [CrossRef]
- Sontag, M.K.; Yusuf, C.; Grosse, S.D.; Edelman, S.; Miller, J.I.; McKasson, S.; Kellar-Guenther, Y.; Gaffney, M.; Hinton, C.F.; Cuthbert, C.; et al. Infants with congenital disorders identified through newborn screening—United states, 2015–2017. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1265–1268. [Google Scholar] [CrossRef]
- Kemper, A.R.; Boyle, C.A.; Aceves, J.; Dougherty, D.; Figge, J.; Fisch, J.L.; Hinman, A.R.; Greene, C.L.; Kus, C.A.; Miller, J.; et al. Long-term follow-up after diagnosis resulting from newborn screening: Statement of the US Secretary of Health and Human Services’ Advisory Committee on Heritable Disorders and Genetic Diseases in Newborns and Children. Genet. Med. 2008, 10, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Hinton, C.F.; Feuchtbaum, L.; Kus, C.A.; Kemper, A.R.; Berry, S.A.; Levy-Fisch, J.; Luedtke, J.; Kaye, C.; Boyle, C.A. What questions should newborn screening long-term follow-up be able to answer? A statement of the US Secretary for Health and Human Services’ Advisory Committee on Heritable Disorders in Newborns and Children. Genet. Med. 2011, 13, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Hinton, C.F.; Homer, C.J.; Thompson, A.A.; Williams, A.; Hassell, K.L.; Feuchtbaum, L.; Berry, S.A.; Comeau, A.M.; Therrell, B.L.; Brower, A.; et al. A framework for assessing outcomes from newborn screening: On the road to measuring its promise. Mol. Genet. Metab. 2016, 118, 221–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senate of the United States. H.R.1281—Newborn Screening Saves Lives Reauthorization Act of 2014. 2014. Available online: https://www.congress.gov/bill/113th-congress/house-bill/1281 (accessed on 12 April 2021).
- Alexander, D.; Hansen, J.W. NICHD research initiative in newborn screening. Ment. Retard. Dev. Disabil. Res. Rev. 2006, 12, 229–315. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Puryear, M.; Brower, A.; Berry, S.A.; Brosco, J.P.; Bowdish, B.; Watson, M.S. Foundation of the Newborn Screening Translational Research Network and its tools for research. Genet. Med. 2019, 21, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Kaye, C.; Bodurtha, J.; Edick, M.; Ginsburg, S.; Keehn, A.; Lloyd-Puryear, M.; Lochner Doyle, D.; Lyon, M.; Ostrander, R.; Taylor, M. Regional models of genetic services in the United States. Genet. Med. 2020, 22, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brower, A. Long-Term Follow-Up in Newborn Screening: An Update on ACMG’s Work on the NBSTRN and NCC. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/meetings/Heritable%20Disorders%202004-2015/2015/May%2011-12,%202015/brower.pdf (accessed on 13 April 2021).
- Follow-Up and Treatment Workgroup. The Role of Quality Measures to Promote Long-Term Follow-Up of Children Identified by Newborn Screening Programs. 2018. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/reports-recommendations/reports/role-of-quality-measures-in-nbs-sept2018-508c.pdf (accessed on 13 April 2021).
- NIH. NIH CDE Repository. Available online: https://cde.nlm.nih.gov/cde/search?selectedOrg=NICHD (accessed on 12 April 2021).
- NBSTRN. Longitudinal Pediatric Data Resource (LPDR). Available online: https://nbstrn.org/tools/lpdr (accessed on 12 April 2021).
- Public Law 107–347—17 December 2002. 2002. Available online: https://www.congress.gov/107/plaws/publ347/PLAW-107publ347.pdf (accessed on 12 April 2021).
- NIH. Science and Technology Research Infrastructure for Discovery, Experimentation, and Sustainability (STRIDES) Initiative. Available online: https://datascience.nih.gov/strides (accessed on 13 April 2021).
- Obeid, J.S.; McGraw, C.A.; Minor, B.L.; Conde, J.G.; Pawluk, R.; Lin, M.; Wang, J.; Banks, S.R.; Hemphill, S.A.; Taylor, R.; et al. Procurement of shared data instruments for Research Electronic Data Capture (REDCap). J. Biomed. Inform. 2013, 46, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. National Library of Medicine. Newborn Screening Coding and Terminology Guide. Data Standards for Electronic Reporting. 2018. Available online: https://lhncbc.nlm.nih.gov/newbornscreeningcodes/ (accessed on 13 April 2021).
- Office of Science and Data Policy, ASPE. Web-Based Information Exchange and Information Services Concept to Support the Exchange of Newborn Screening Information Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. 2009. Available online: https://aspe.hhs.gov/basic-report/web-based-information-exchange-and-information-services-concept-support-exchange-newborn-screening-information (accessed on 29 June 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Project | Condition(s) | Population | CDEs | Subjects | Max Data Entry Time Points | User Type | Data Available? * (Yes/No) | Status |
|---|---|---|---|---|---|---|---|---|
| Sickle Cell Disease Newborn Screening Follow-Up | Sickle Cell Disease | Diagnosed Cases | 57 | 8346 | 9 | Community-Based Organization (CBO) | Yes | Active |
| Inborn Errors in Metabolism Consortium (IBEMC) | 43 RUSP Conditions ** | Diagnosed Cases | 2649 | 2078 | 30 | Clinician | Yes | Completed |
| Project CURE Spinal Muscular Atrophy (SMA) | SMA | Diagnosed Cases | 4337 | 701 | 5 | Clinician | Yes | Active |
| SPOT SMA | SMA | Newborns | 4759 | 434 | 4 | Clinician | Yes | Active |
| Krabbe Registry | Krabbe | Diagnosed Newborns | 187 | 196 | 1 | Clinician and Parent | Yes | Completed |
| Rady NSIGHT2 | Variety | Neonatal Intensive Care Unit (NICU) | 45 | 214 | 2 | Clinician | Yes | Completed |
| BabySeq | Variety | NICU; Healthy at Birth | 30 | 159 | 2 | Clinician | Yes | Completed |
| NC NEXUS | RUSP *** | Newborns | 180 | 200 | 2 | Clinician | Yes | Completed |
| NY State LTFU | X-linked Adrenoleukodystrophy, Severe Combined Immune Deficiency, Fatty Acid Oxidation Disorders, Krabbe | Newborns | 202 | 10 | 5 | State NBS Program | No | Active |
| Duchenne NBS Pilot | Duchenne Muscular Dystrophy | Newborns | 624 | 17 | 6 | Clinician and State NBS Program | No | Active |
| eXtraordinarY Babies Study | Chromosome Aneuploidy | Newborns | 320 | 200 | 5 | Clinician | No | Active |
| CPT1A Arctic Variant | CPT1A Arctic Variant | Newborn and Children | 69 | TBD | 4 | Clinician | No | Active |
| Oregon Health & Science University | RUSP *** | Newborns | 894 | TBD | 2 | Clinician | No | Active |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brower, A.; Chan, K.; Hartnett, M.; Taylor, J. The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts. Int. J. Neonatal Screen. 2021, 7, 37. https://doi.org/10.3390/ijns7030037
Brower A, Chan K, Hartnett M, Taylor J. The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts. International Journal of Neonatal Screening. 2021; 7(3):37. https://doi.org/10.3390/ijns7030037
Chicago/Turabian StyleBrower, Amy, Kee Chan, Michael Hartnett, and Jennifer Taylor. 2021. "The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts" International Journal of Neonatal Screening 7, no. 3: 37. https://doi.org/10.3390/ijns7030037
APA StyleBrower, A., Chan, K., Hartnett, M., & Taylor, J. (2021). The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts. International Journal of Neonatal Screening, 7(3), 37. https://doi.org/10.3390/ijns7030037