
Newborn Screening for SCID: Experience in Spain (Catalonia)

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
1.1. Newborn Screening (NBS) Programs in Spain
1.2. Newborn Screening for SCID in Spain
1.3. Newborn Screening in Catalonia
1.4. Newborn Screening for SCID in Catalonia
2. Materials and Methods
2.1. Population
2.2. Sample Testing
2.3. Pilot Study
Methodology and Algorithm Validation
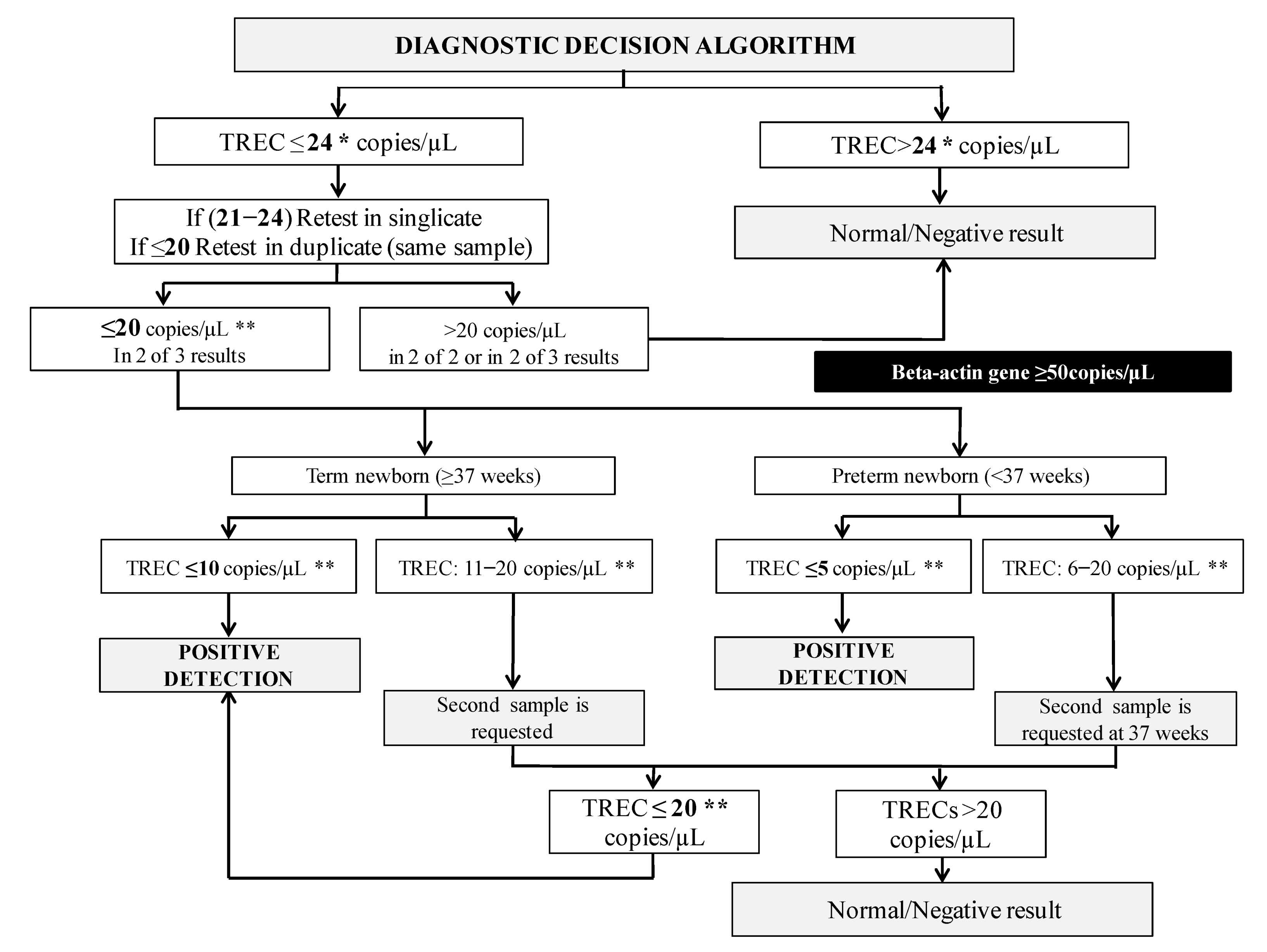
2.4. Currently Decision Algorithm for SCID Detection
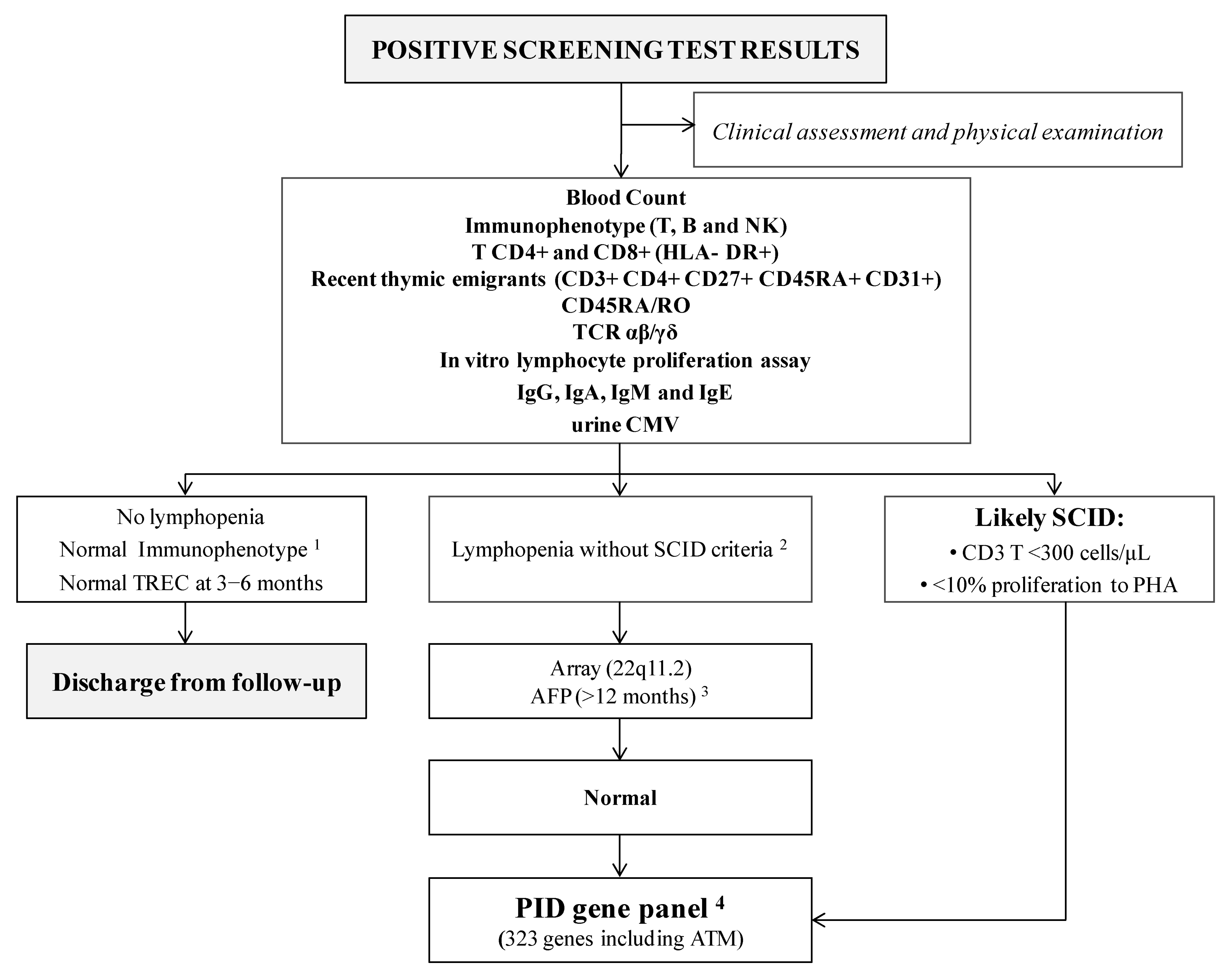
2.5. Protocol for SCID Positive Detections
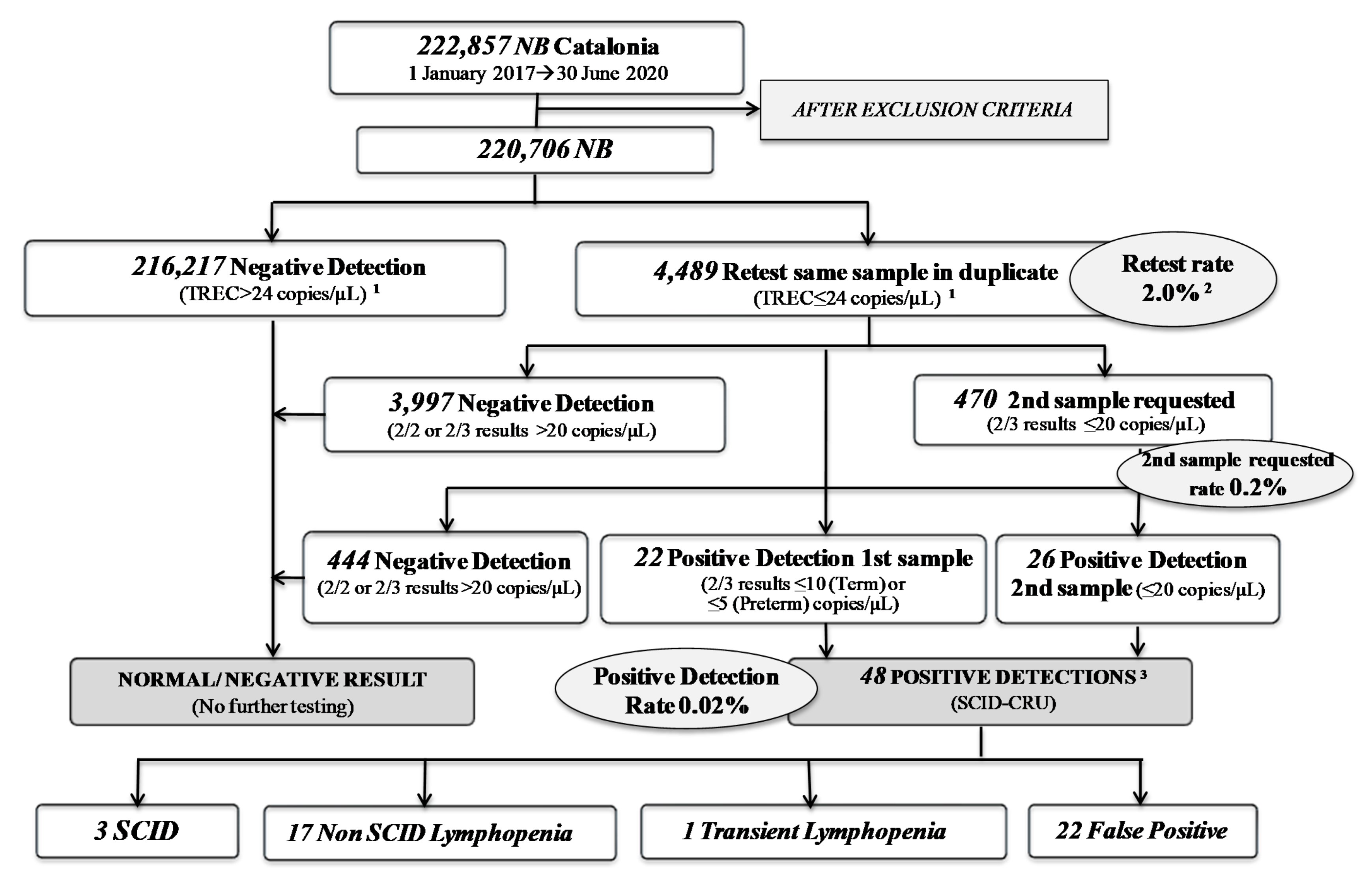
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, L.; Xu-Bayford, J.; Allwood, Z.; Slatter, M.; Cant, A.; Davies, E.G.; Veys, P.; Gennery, A.R.; Gaspar, H.B. Neonatal diagnosis of severe combined immunodeficiency leads to significantly improved survival outcome: The case for newborn screening. Blood 2011, 117, 3243–3246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, R.; Schiff, S.; Schiff, R.; Markert, M.L.; Williams, L.W.; Roberts, J.L.; Myers, L.A.; Ward, F.E. Hematopoietic stem-cell transplantation for the treatment of severe combined immunodeficiency. N. Engl. J. Med. 1999, 340, 508–516. [Google Scholar] [PubMed]
- Chan, K.; Puck, J.M. Development of a population-based screening for severe combined immunodeficiency. J. Allergy Clin. Immunol. 2005, 115, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, C.; Durand-Zaleski, I.; Frenkiel, J.; Mirallié, S.; Léger, A.; Cheillan, D.; Audrain, M. Clinical and economic aspects of newborn screening for severe combined immunodeficiency: DEPISTREC study results. Clin. Immunol. 2019, 202, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Argudo-Ramírez, A.; Martín-Nalda, A.; Marín-Soria, J.L.; López-Galera, R.M.; Pajares-García, S.; González de Aledo-Castillo, J.M.; Martínez-Gallo, M.; García-Prat, M.; Colobran, R.; Riviere, J.G.; et al. First Universal Newborn Screening Program for Severe Combined Immunodeficiency in Europe. Two-Years’ Experience in Catalonia (Spain). Front Immunol. 2019, 10, 2406. [Google Scholar] [CrossRef] [PubMed]
- Marín Soria, J.L.; González de Aledo Castillo, J.M.; Argudo Ramírez, A.; López Galera, R.M.; García, S.P.; Rubió, R.A.; Villoria, J.G.; Yahyaoui, R.; Álvarez Ríos, A.I.; Madrid, E.M.; et al. Inicio, evolución y situación actual de los Programas de Cribado Neonatal en España [Beginnings, evolution and current situation of the Newborn Screening Programs in Spain.]. Rev. Esp. Salud Publica 2021, 95, 1–29. [Google Scholar]
- Pajares, S.; López, R.M.; Gort, L.; Argudo-Ramírez, A.; Marín, J.L.; González de Aledo-Castillo, J.M.; García-Villoria, J.; Arranz, J.A.; Del Toro, M.; Tort, F.; et al. An incidental finding in newborn screening leading to the diagnosis of a patient with ECHS1 mutations. Mol. Genet. Metab. Rep. 2020, 22, 100553. [Google Scholar] [CrossRef] [PubMed]
- de Felipe, B.; Olbrich, P.; Lucenas, J.M.; Delgado-Pecellin, C.; Pavon-Delgado, A.; Marquez, J.; Salamanca, C.; Soler-Palacin, P.; Gonzalez-Granado, L.I.; Antolin, L.F.; et al. Prospective neonatal screening for severe T and B-lymphocyte deficiencies in Seville. Pediatric Allergy Immunol. 2016, 27, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Yahyaoui, R.; (Clinical Laboratory and Newborn Screening Center of Eastern Andalucia; Málaga Regional Hospital; 29011 Málaga, Spain). Personal communication, 2021.
- Marín Soria, J.L.; López Galera, R.M.; Argudo Ramírez, A.; González de Aledo, J.M.; Pajares García, S.; Navarro Sastre, A.; Hernández Pérez, J.M.; Ribes Rubio, A.; Gort Mas, L.; García Villoria, J.; et al. 50 años del Programa de Cribado Neonatal en Cataluña [50 years of the Neonatal Screening Program in Catalonia.]. Rev. Esp. Salud Publica 2020, 94, e1–e15. [Google Scholar]
- Audrain, M.; Léger, A.; Hémont, C.; Mirallié, S.M.; Cheillan, D.; Rimbert, M.G.M.; Le Thuaut, A.M.-P.; Sébille-Rivain, V.A.; Prat, A.; Pinel, E.M.Q.; et al. Newborn Screening for Severe Combined Immunodeficiency: Analytic and Clinical Performance of the T Cell Receptor Excision Circle Assay in France (DEPISTREC Study). J. Clin. Immunol. 2018, 38, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Van der Spek, J.; Groenwold, R.H.H.; van der Burg, M.; Van Montfrans, J.M. TREC based newborn screening for severe combined immunodeficiency disease: A systematic review. J. Clin. Immunol. 2015, 35, 416–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rechavi, E.; Lev, A.; Simon, A.J.; Stauber, T.; Daas, S.; Saraf-Levy, T.; Broides, A.; Nahum, A.; Marcus, N.; Hanna, S.; et al. First Year of Israeli Newborn Screening for Severe Combined Immunodeficiency—Clinical Achievements and Insights. Front. Immunol. 2017, 8, 1448. [Google Scholar] [CrossRef] [Green Version]
- Blom, M.; Pico-Knijnenburg, I.; Sijne-van Veen, M.; Boelen, A.; Bredius, R.G.; van der Burg, M.; Schielen, P.C. An evaluation of the TREC assay with regard to the integration of SCID screening into the Dutch newborn screening program. Clin. Immunol. 2017, 180, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.P.; Rashid, S.; Premachandra, T.; Harvey, K.; Ifederu, A.; Wilson, M.C.; Gaspar, H.B. Screening of neonatal UK dried blood spots using a duplex TREC screening assay. J. Clin. Immunol. 2014, 34, 323–330. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inherited Metabolic Diseases | |
|---|---|
| Phenylketonuria and Hyperphenyalaninemias | ß-Ketothiolase deficiency |
| Maple syrup urine disease | Propionic acidemia |
| Tyrosinemia type I | Medium-chainacyl-CoA dehydrogenase deficiency |
| Citrullinemia | Very long-chain acyl-CoA dehydrogenase deficiency |
| Homocystinuria (CBS deficiency) | Mitochondrial trifunctional protein deficiency//Long-chain L-3 hydroxyacyl-CoA dehydrogenase deficiency |
| Glutaric aciduria type I | Multiple acyl-CoA dehydrogenase deficiency |
| Isovaleric acidemia | Primary carnitine deficiency |
| Methylmalonic aciduria | Carnitine palmitoyltransferase 1 deficiency |
| Methylmalonic aciduria with Homocystinuria | Carnitine palmitoyltransferase 2 deficiency |
| 3-Hydroxy-3-methylglutaryl-CoA lyase deficiency | Carnitine-acylcarnitine translocase deficiency |
| Other Diseases | |
| Cystic Fibrosis | Sickle cell disease |
| Congenital Hypothyroidism | Severe combined immunodeficiency |
| PARAMETER | 2020 (January–June) | 2019 | 2018 | 2017 |
|---|---|---|---|---|
| Sample size | 30,296 | 61,460 | 64,290 | 66,811 |
| Repetition Cutoff (same sample in duplicate) | 24 copies/µL | 24 copies/µL | 24 copies/µL | 34 copies/µL |
| 1st Sample Retest Rate | 1.5% (n = 464) | 1.5% (n = 915) | 1.4% (n = 898) | 3.34% (n = 2212) |
| 2nd Sample Request Rate | 0.19% (n = 57) | 0.17% (n = 108) | 0.26% (n = 167) | 0.21% (n = 138) |
| Positive Detection Rate | 0.02% (n = 7) | 0.02% (n = 11) | 0.02% (n = 15) | 0.02% (n = 15) |
| Incidence | 1/74,187 * | 1/193,002 | 1/130,903 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argudo-Ramírez, A.; Martín-Nalda, A.; González de Aledo-Castillo, J.M.; López-Galera, R.; Marín-Soria, J.L.; Pajares-García, S.; Martínez-Gallo, M.; García-Prat, M.; Colobran, R.; Riviere, J.G.; et al. Newborn Screening for SCID: Experience in Spain (Catalonia). Int. J. Neonatal Screen. 2021, 7, 46. https://doi.org/10.3390/ijns7030046
Argudo-Ramírez A, Martín-Nalda A, González de Aledo-Castillo JM, López-Galera R, Marín-Soria JL, Pajares-García S, Martínez-Gallo M, García-Prat M, Colobran R, Riviere JG, et al. Newborn Screening for SCID: Experience in Spain (Catalonia). International Journal of Neonatal Screening. 2021; 7(3):46. https://doi.org/10.3390/ijns7030046
Chicago/Turabian StyleArgudo-Ramírez, Ana, Andrea Martín-Nalda, Jose Manuel González de Aledo-Castillo, Rosa López-Galera, Jose Luis Marín-Soria, Sonia Pajares-García, Mónica Martínez-Gallo, Marina García-Prat, Roger Colobran, Jacques G. Riviere, and et al. 2021. "Newborn Screening for SCID: Experience in Spain (Catalonia)" International Journal of Neonatal Screening 7, no. 3: 46. https://doi.org/10.3390/ijns7030046
APA StyleArgudo-Ramírez, A., Martín-Nalda, A., González de Aledo-Castillo, J. M., López-Galera, R., Marín-Soria, J. L., Pajares-García, S., Martínez-Gallo, M., García-Prat, M., Colobran, R., Riviere, J. G., Quintero, Y., Collado, T., Ribes, A., García-Villoria, J., & Soler-Palacín, P. (2021). Newborn Screening for SCID: Experience in Spain (Catalonia). International Journal of Neonatal Screening, 7(3), 46. https://doi.org/10.3390/ijns7030046