
Newborn Screening for Congenital Hypothyroidism-Clinical Evaluation and Comparison of Two Different Test Kits for the Determination of TSH in Dried Blood Samples on Two Different Platforms


Abstract
:1. Introduction
2. Materials and Methods
3. Result
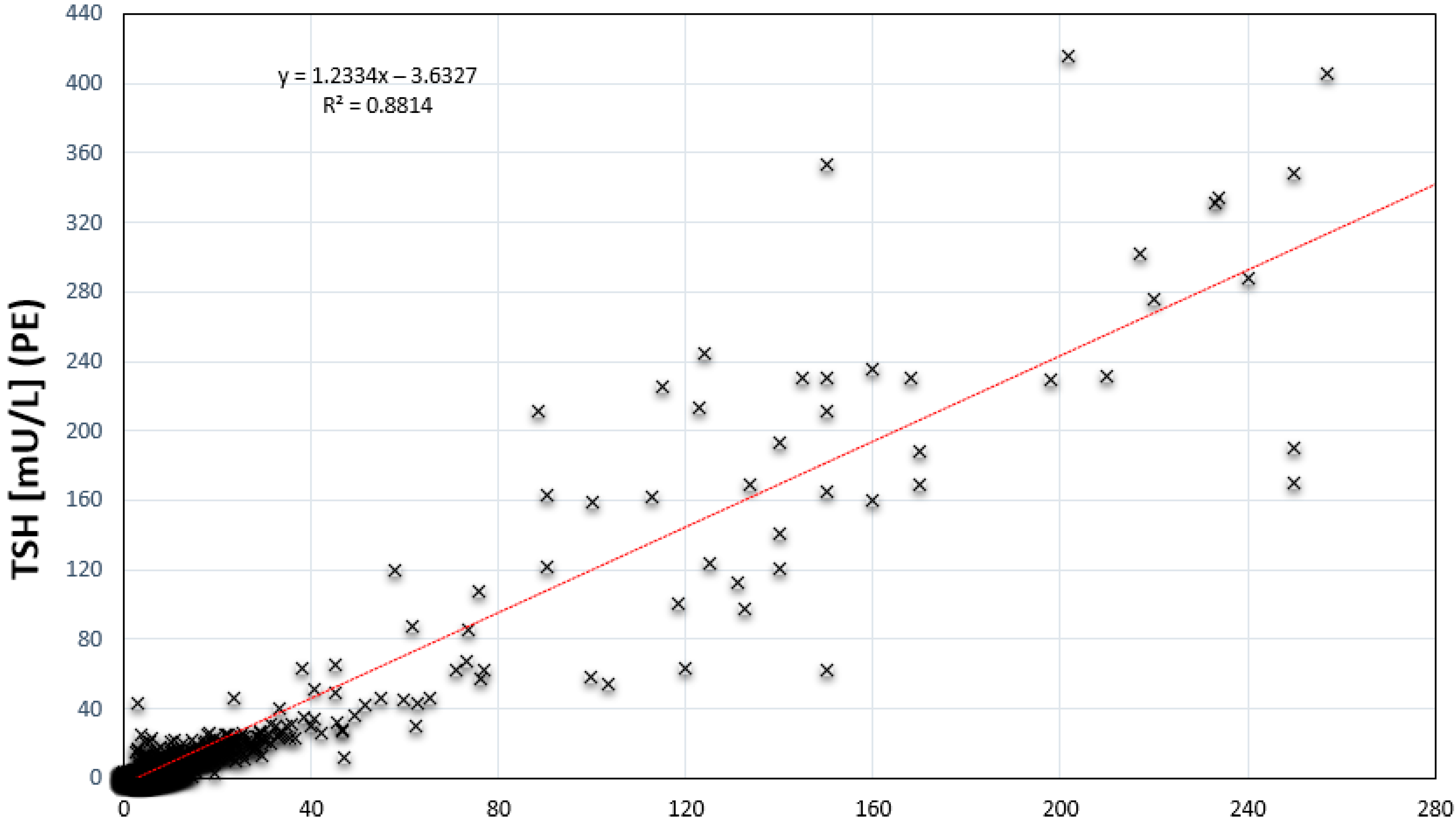
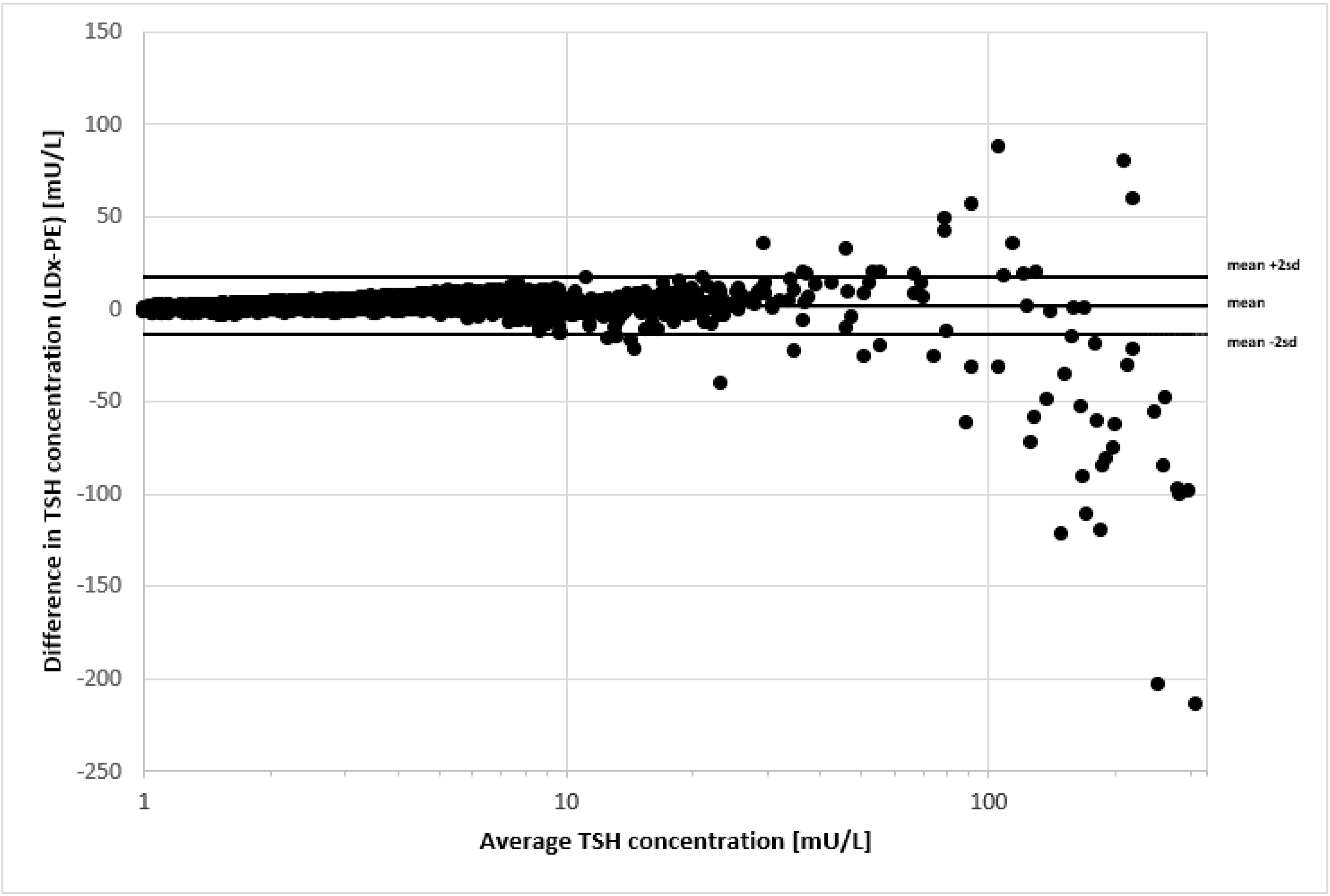
3.1. Comparison of 5501 Newborn Samples
3.2. Comparison of 472 Newborn Samples in Duplicate
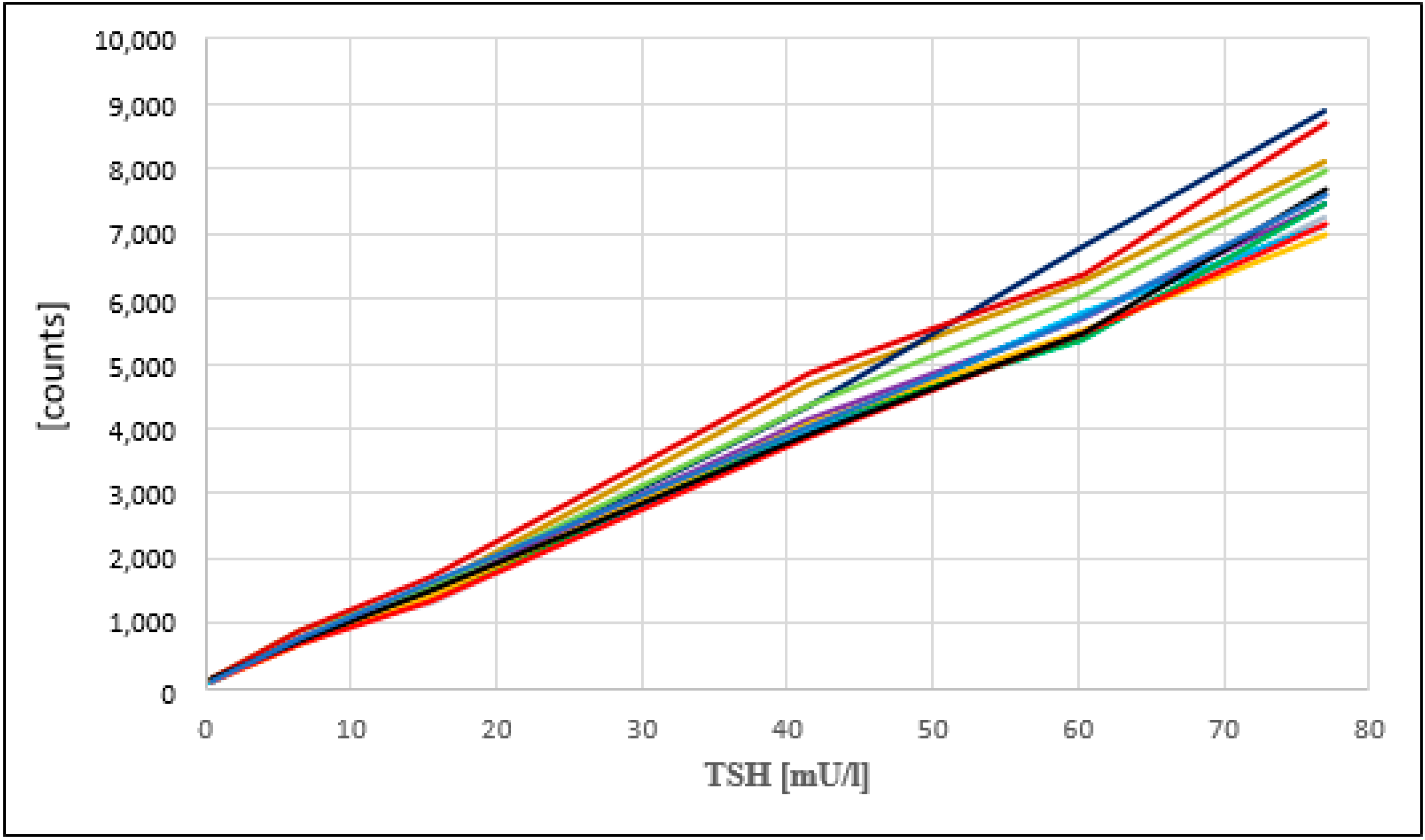
3.3. Day to Day Reproducibility
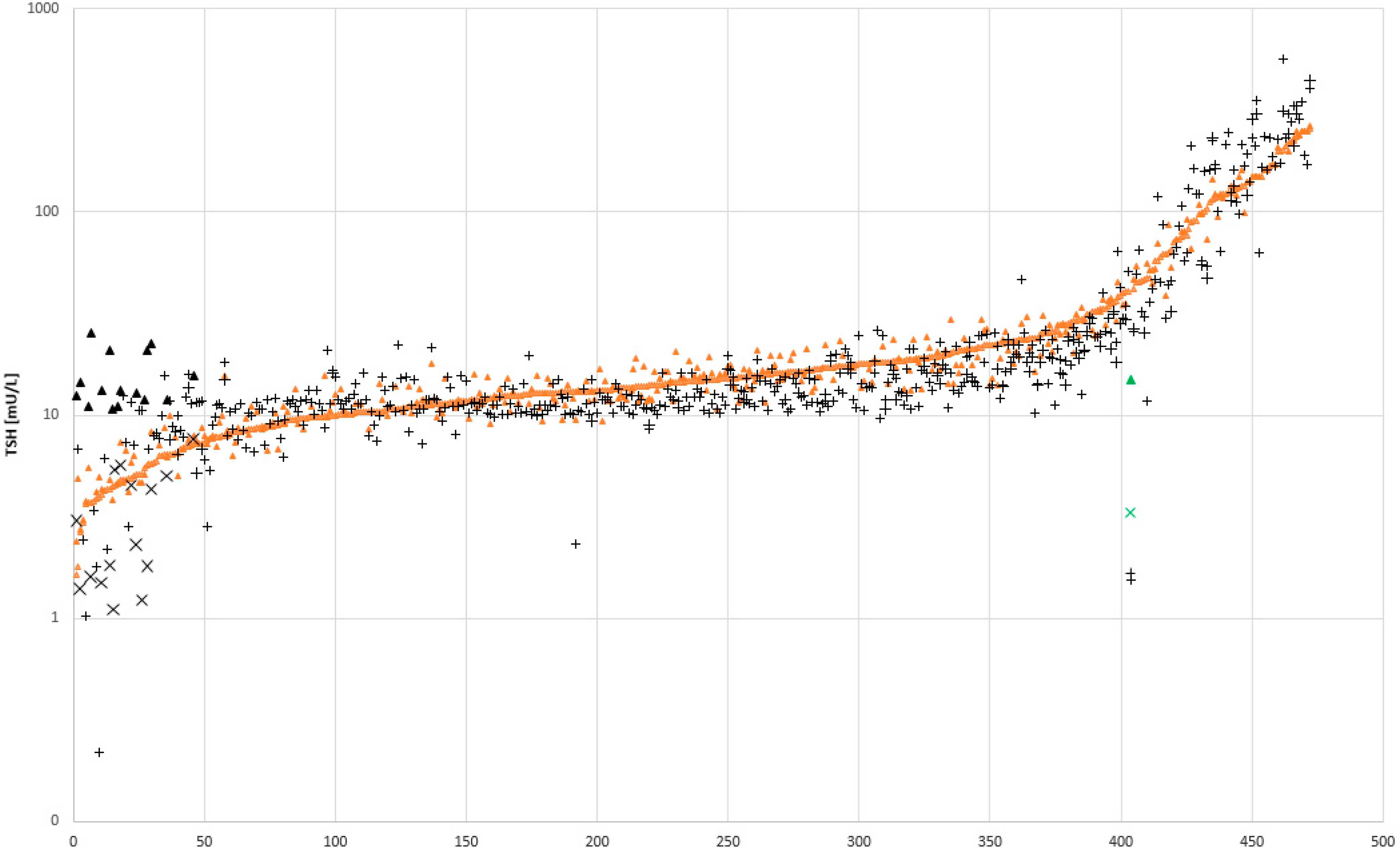
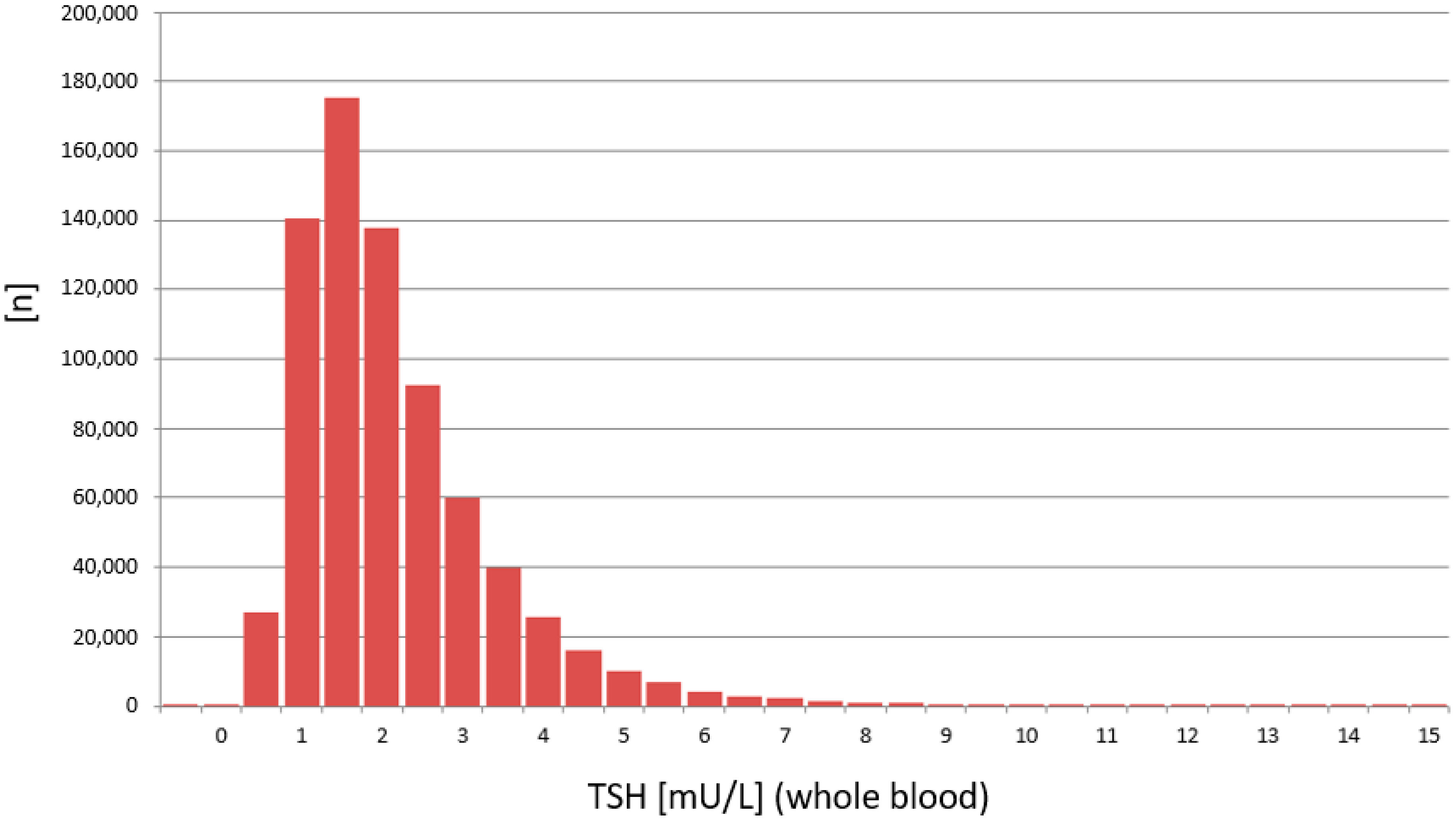
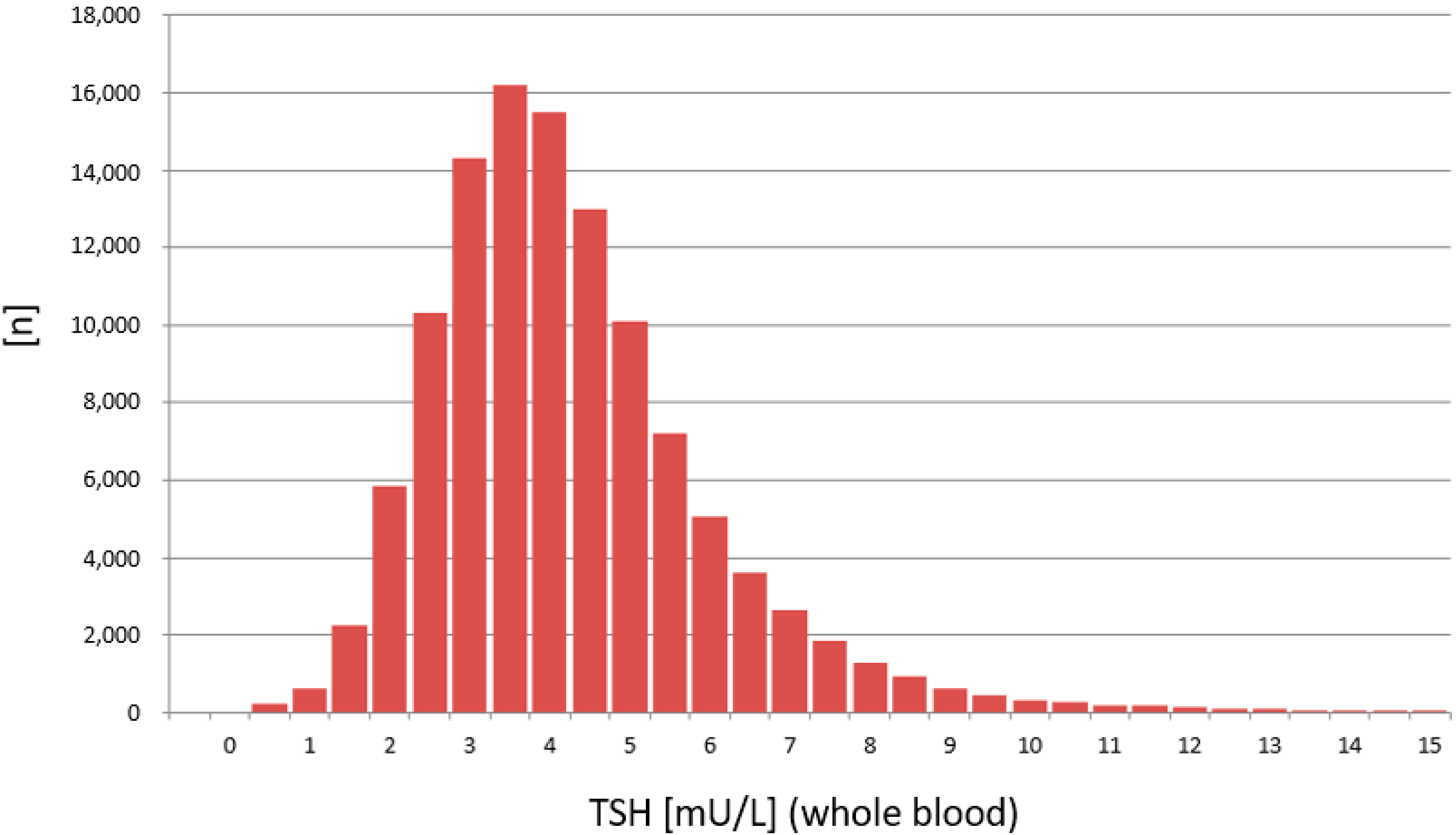
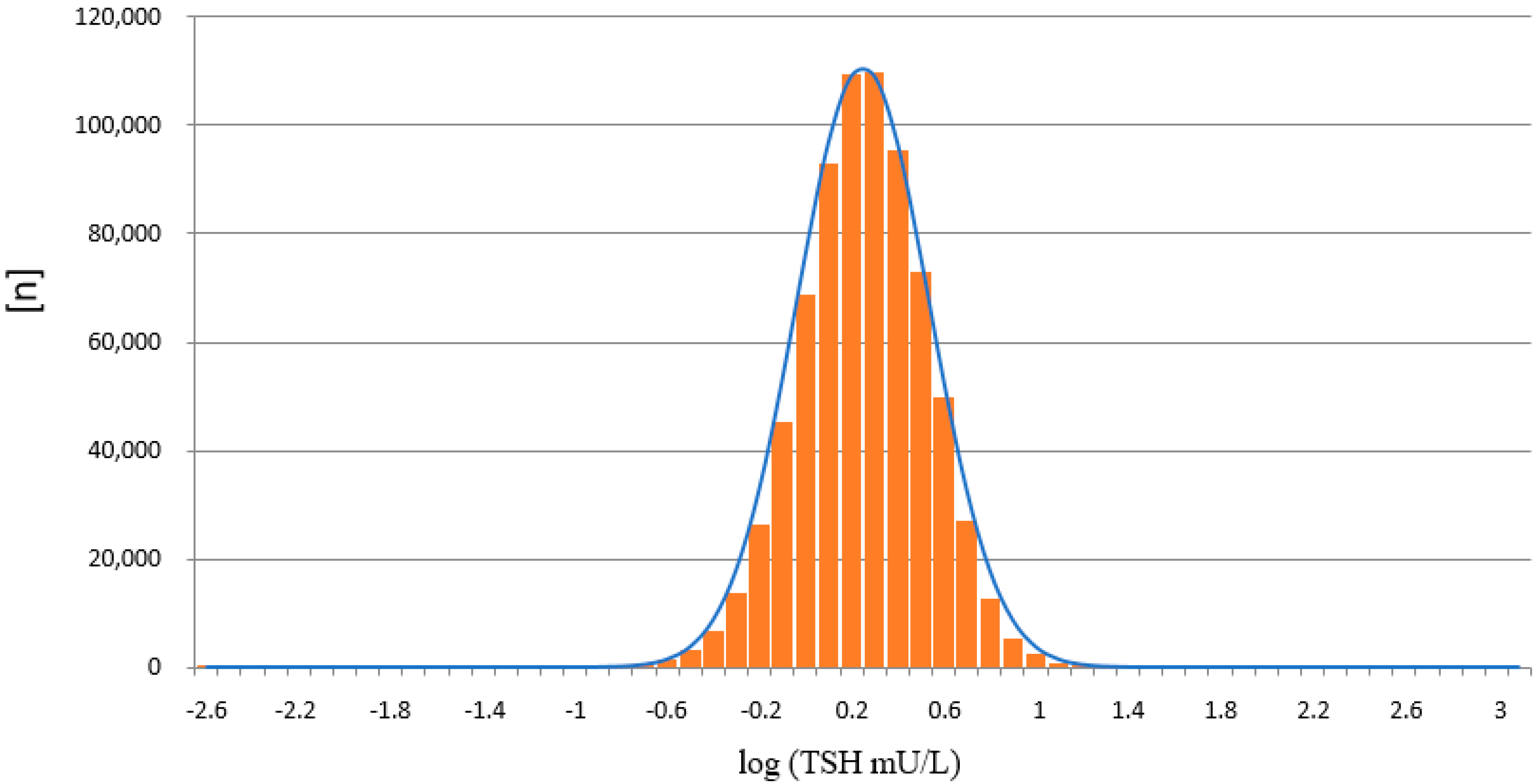
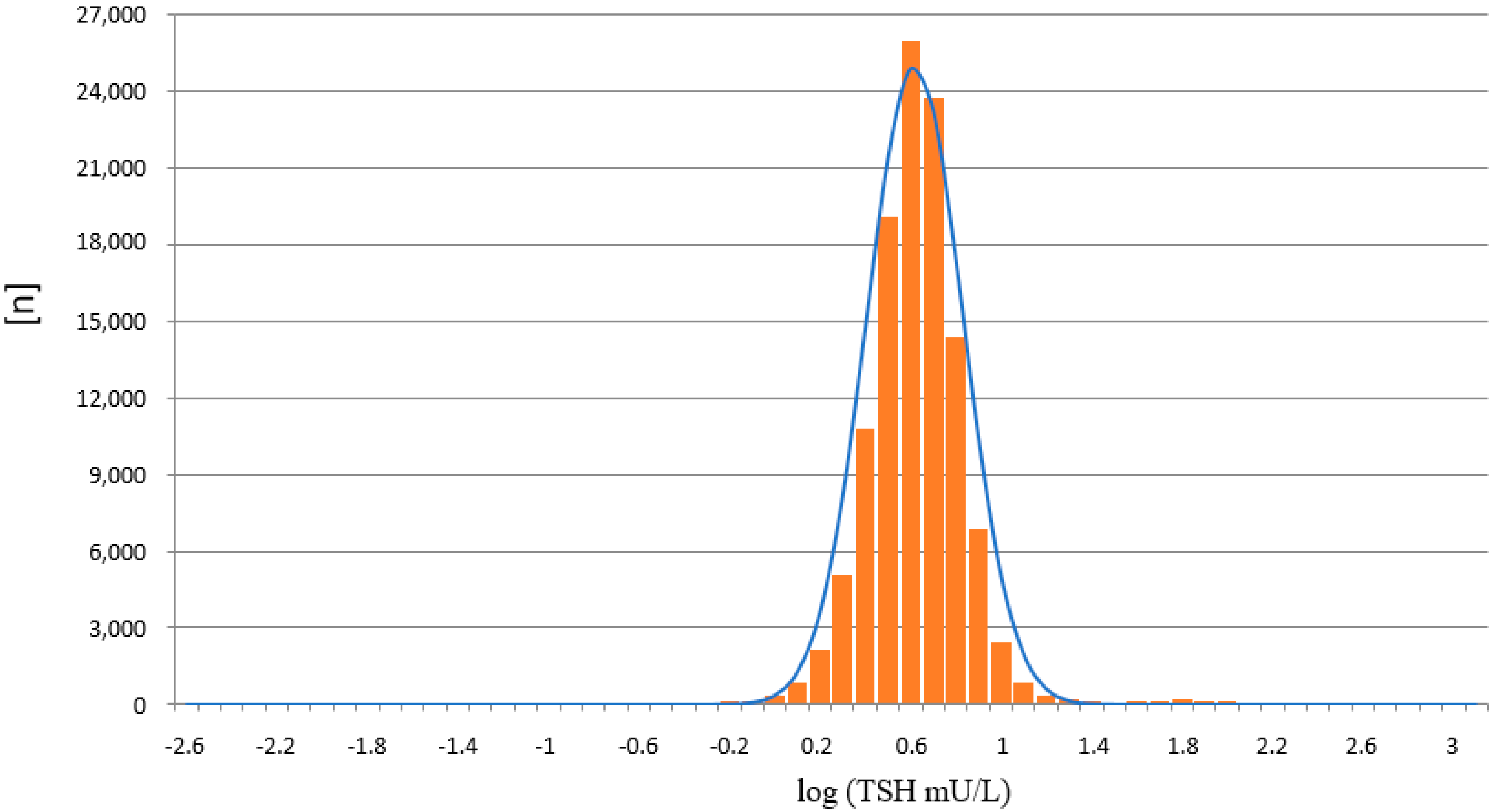
3.4. Comparison of the Distribution of TSH Values
3.5. Internal and External Quality Control
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larsen, P.R.; Broskin, K. Thyroxine (T4) immunoassay using a filter paper blood samples for screening of neonates for hypothyroidism. Pediatr. Res. 1975, 9, 604–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irie, M.; Enomoto, K.; Naruse, H. Measurement of thyroid-stimulating hormone in dried blood spot. Lancet 1975, 2, 1233–1234. [Google Scholar] [CrossRef]
- Walfish, P.G. Evaluation of three thyroid-function screening tests for detecting neonatal hypothyroidism. Lancet 1976, 1, 1208–1210. [Google Scholar] [CrossRef]
- Larsson, A.; Ljunggren, J.G.; Ekman, K.; Nilsson, A.; Olin, P. Screening for congenital hypothyroidism. I. Laboratory results of a pilot study based on dried blood samples collected for PKU screening. Acta. Paediatr. Scand. 1981, 70, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.; Ljunggren, J.G.; Ekman, K.; Nilsson, A.; Olin, P.; Bodegård, G. Screening for congenital hypothyroidism. II. Clinical findings in infants with positive screening tests. Acta. Paediatr. Scand. 1981, 70, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Cherella, C.E.; Wassner, A.J. Update on congenital hypothyroidism. Curr. Opin. Endocrinol. Diabetes. Obes. 2020, 27, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Loeber, J.G.; Platis, D.; Rolf, H.; Zetterström, R.H.; Shlomo, A.S.; François, B.F.; James, R.; Bonham, J.R.; Patricia Borde, P.; Brincat, I.; et al. Neonatal Screening in Europe Revisited: An ISNS Perspective on the Current State and Developments Since 2010. Int. J. Neonatal. Screen 2021, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Kilberg, M.J.; Rasooly, I.R.; LaFranchi, S.H.; Bauer, A.J.; Hawkes, C.P. Newborn Screening in the US May Miss Mild Persistent Hypothyroidism. J. Pediatr. 2018, 192, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.M.; Ekin, R.P. Theoretical limitations on immunoassay sensitivity. Current practice and potential advantages of fluorescent Eu3+ chelates as non-radioisotopic tracers. J. Immunol. Methods. 1986, 87, 13–20. [Google Scholar] [CrossRef]
- Hemmiläa, I.; Dakubu, S.; Mukkalaa, V.-M.; Siitaria, H.; Lövgren, T. Europium as a label in time-resolved immunofluorometric assays. Anal. Biochem. 1984, 137, 335–343. [Google Scholar] [CrossRef]
- Woolley, C.F.; Hayes, M.A.; Mahanti, P.; Gilman, S.D.; Taylor, T. Theoretical Limitations of Quantification for Noncompetitive Sandwich Immunoassays. Anal. Bioanal. Chem. 2015, 407, 8605–8615. [Google Scholar] [CrossRef] [PubMed]
- Fingerhut, R.; Torresani, T. Evaluation of the genetic screening processor (GSPTM) for newborn Screening. Anal. Methods 2013, 5, 4769–4776. [Google Scholar] [CrossRef] [Green Version]
- Fingerhur, R.; Sluka, S.H.M. A Simple Method to Overcome the “Floating Disc Problem” Using the GALT-Assay on the PerkinElmer GSP—Remeasurement on a Stand Alone Plate Fluorimeter. Int. J. Neonatal. Screen 2016, 2, 11. [Google Scholar] [CrossRef] [Green Version]
- Cennamo, M.; La Civita, E.; Curci, A.; Liotti, A.; Braschi, U.; Terracciano, D. Comparison between a new thyroglobulin assay with well-established Beckmann Access immunoassay: A preliminary report. J. Clin. Lab. Anal. 2020, 35, e23589. [Google Scholar] [CrossRef] [PubMed]
- Caputo, M.J. The use of probability plots and log-transformations in normal range determinations. Am. J. Med. Technol. 1972, 38, 1–5. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Calibrator A | Calibrator B | Calibrator C | Calibrator D | Calibrator E | Calibrator F |
|---|---|---|---|---|---|
| 138 (13) | 768 (10) | 1484 (12) | 4190 (8) | 5824 (8) | 7690 (10) |
| Intra-Assay Variation (CV) | Intrer-Assay Variation (CV) | Mean Recovery [%] * | |
|---|---|---|---|
| Control 1 | 6.3 (at 9.7 mU/L; n = 10) | 15.7 (at 9.7 mU/L; n = 14) | 103.0 |
| Control 2 | 8.5 (at 25.1 mU/L; n = 10) | 6.6 (at 25.1 mU/L; n = 14) | |
| CDC | 4.3 (at 18.7 mU/L; n = 4) | 6.8 (at 45.3 mU/L; n = 14) |
| Sample | Result [mU/L] PE/GSP | Result [mU/L] LDx/NS2400 | Target [mU/L] | Range [mU/L] |
|---|---|---|---|---|
| RfB-1 | 2.05 | 3.22 | 0.82–5.62 | |
| RfB-2 | 3.53 | 5.30 | 2.90–7.70 | |
| RfB-3 | 3.41 | 5.60 | 3.20–8.00 | |
| RfB-4 | 7.74 | 6.90 | 4.83–8.97 | |
| RfB-5 | 5.78 | 7.34 | 4.40–10.30 | |
| RfB-6 | 9.53 | 8.90 | 6.23–11.60 | |
| RfB-7 | 6.45 | 9.05 | 5.43–12.70 | |
| RfB-8 | 8.99 | 9.90 | 6.93–12.90 | |
| RfB-9 | 9.87 | 12.10 | 7.26–17.00 | |
| RfB-10 | 9.62 | 13.00 | 7.80–18.20 | |
| RfB-11 | 14.52 | 17.00 | 10.20–23.80 | |
| RfB-12 | 16.94 | 18.00 | 12.60–23.40 | |
| RfB-13 | 13.92 | 18.80 | 11.20–26.40 | |
| RfB-14 | 15.12 | 23.00 | 13.80–32.20 | |
| RfB-15 | 18.30 | 24.50 | 17.10–31.90 | |
| RfB-16 | 25.51 | 26.50 | 15.90–37.10 | |
| RfB-17 | 24.19 | 26.70 | 18.60–34.80 | |
| RfB-18 | 42.67 | 33.00 | 23.10–42.90 | |
| RfB-19 | 23.48 | 33.30 | 19.90–46.70 | |
| RfB-20 | 39.52 | 35.20 | 24.60–45.80 | |
| RfB-21 | 39.25 | 51.90 | 31.10–72.70 | |
| UK-NEQUAS-1 | 3.40 | 3.33 | 3.60 | 1.50–5.70 |
| UK-NEQUAS-2 | 4.30 | 4.53 | 4.60 | 2.50–6.70 |
| UK-NEQUAS-3 | 5.90 | 5.65 | 5.80 | 3.40–8.20 |
| UK-NEQUAS-4 | 11.90 | 10.27 | 12.20 | 7.40–17.00 |
| UK-NEQUAS-5 | 20.00 | 15.18 | 20.40 | 14.40–26.40 |
| UK-NEQUAS-6 | 19.90 | 18.24 | 21.50 | 15.80–27.20 |
| UK-NEQUAS-7 | 30.90 | 27.10 | 32.90 | 22.10–43.70 |
| UK-NEQUAS-8 | 29.30 | 28.42 | 34.20 | 22.80–45.60 |
| UK-NEQUAS-9 | 56.30 | 66.02 | 66.00 | 48.00–84.00 |
| UK-NEQUAS-10 | 69.60 | 58.91 | 80.10 | 56.10–104.10 |
| UK-NEQUAS-11 | 76.50 | 65.71 | 85.00 | 56.80–113.20 |
| CDC-1 | 18.53 | 18.70 | 11.00–26.30 | |
| CDC-2 | 20.40 | 22.7 | 13.40–32.00 | |
| CDC-3 | 49.30 | 41.50 | 24.40–58.60 | |
| CDC-4 | 44.67 | 45.30 | 26.60–64.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fingerhut, R. Newborn Screening for Congenital Hypothyroidism-Clinical Evaluation and Comparison of Two Different Test Kits for the Determination of TSH in Dried Blood Samples on Two Different Platforms. Int. J. Neonatal Screen. 2021, 7, 51. https://doi.org/10.3390/ijns7030051
Fingerhut R. Newborn Screening for Congenital Hypothyroidism-Clinical Evaluation and Comparison of Two Different Test Kits for the Determination of TSH in Dried Blood Samples on Two Different Platforms. International Journal of Neonatal Screening. 2021; 7(3):51. https://doi.org/10.3390/ijns7030051
Chicago/Turabian StyleFingerhut, Ralph. 2021. "Newborn Screening for Congenital Hypothyroidism-Clinical Evaluation and Comparison of Two Different Test Kits for the Determination of TSH in Dried Blood Samples on Two Different Platforms" International Journal of Neonatal Screening 7, no. 3: 51. https://doi.org/10.3390/ijns7030051
APA StyleFingerhut, R. (2021). Newborn Screening for Congenital Hypothyroidism-Clinical Evaluation and Comparison of Two Different Test Kits for the Determination of TSH in Dried Blood Samples on Two Different Platforms. International Journal of Neonatal Screening, 7(3), 51. https://doi.org/10.3390/ijns7030051