
Pilot Program of Newborn Screening for 5q Spinal Muscular Atrophy in the Russian Federation

 ,
,  , , , ,
, , , , 
Abstract
:1. Introduction
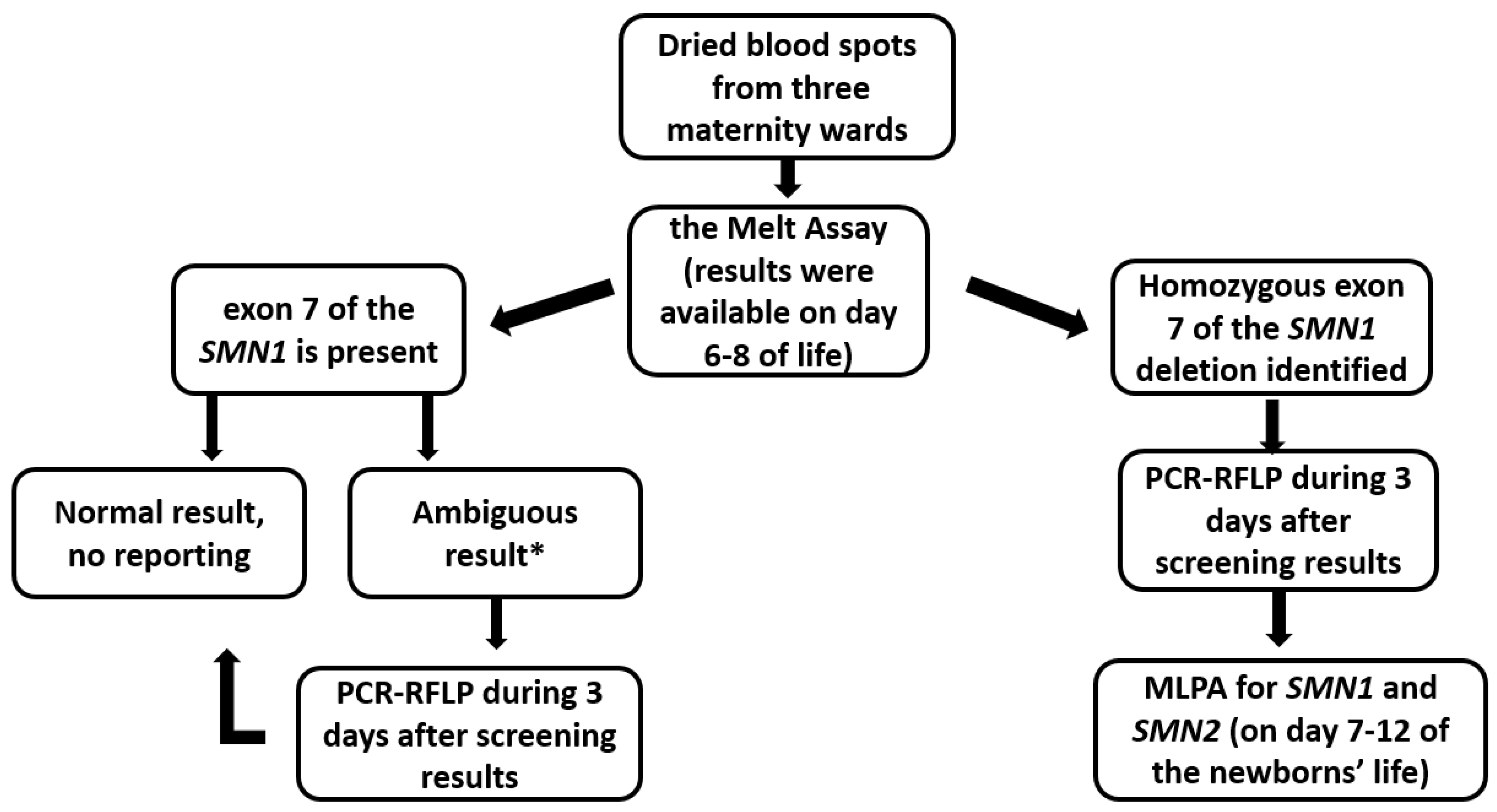
2. Materials and Methods
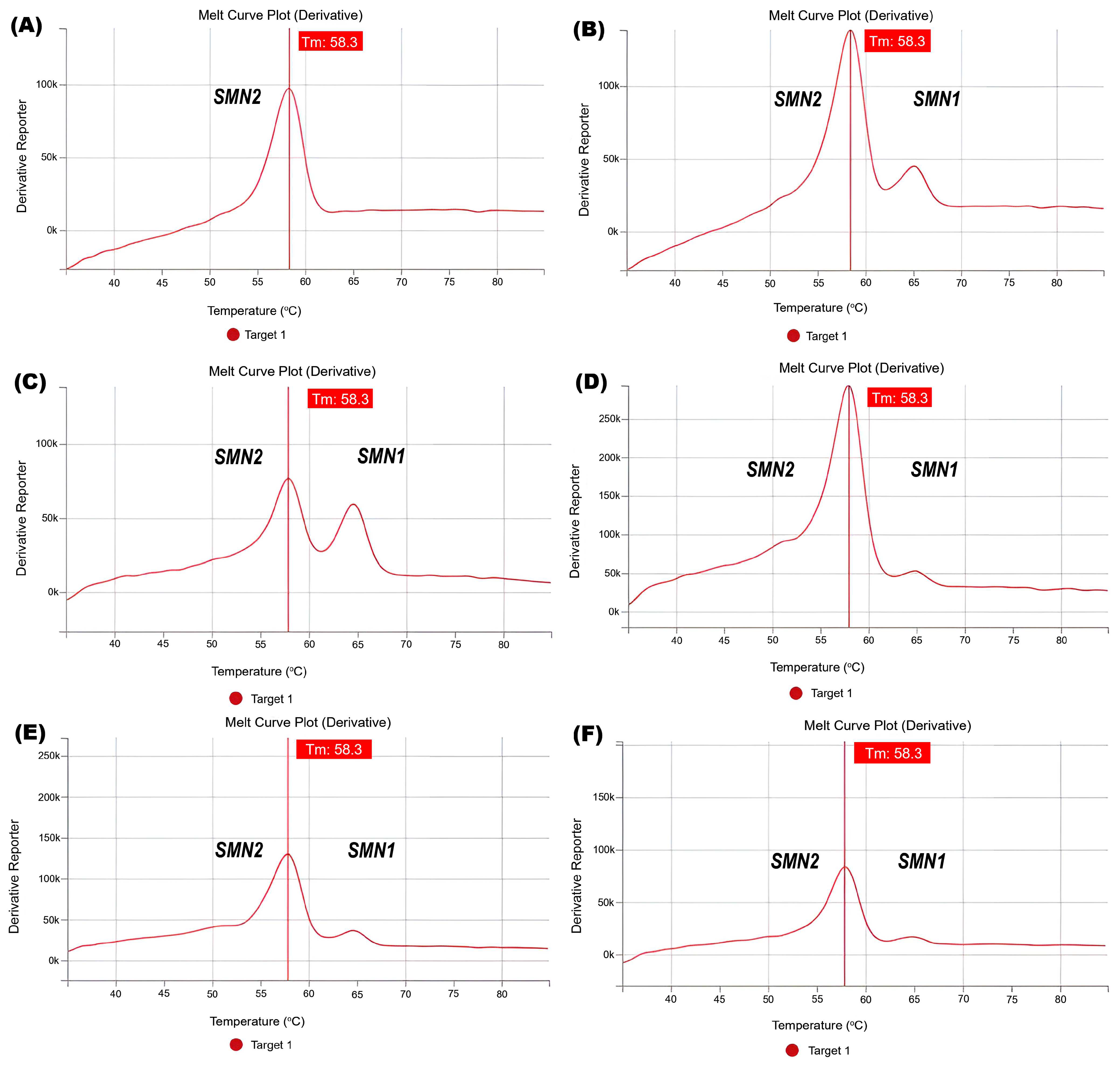
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Tubes | PCR Buffer, µL | dNTP, µL | Primer (7 or 8) Mix Volume, µL | The Volume of Taq Polymerase, µL | Volume of H2O, µL |
|---|---|---|---|---|---|
| 1 | 6 | 2.5 | 0.7 | 0.2 | 13.6 |
- (1)
- Prepare 0.5 mL restriction tubes by numbering and arranging them appropriately in a rack. Add 10 µL of amplificant from the corresponding tube to each tube after PCR;
- (2)
- Prepare a restriction mixture consisting of buffer, enzyme, and water according to Table A2.
| Number of Tubes | Volume of 10X Restriction Buffer, µL | Volume of H2O, µL | Enzyme Volume, µL |
|---|---|---|---|
| 1.5 | 2.9 | 0.6 |
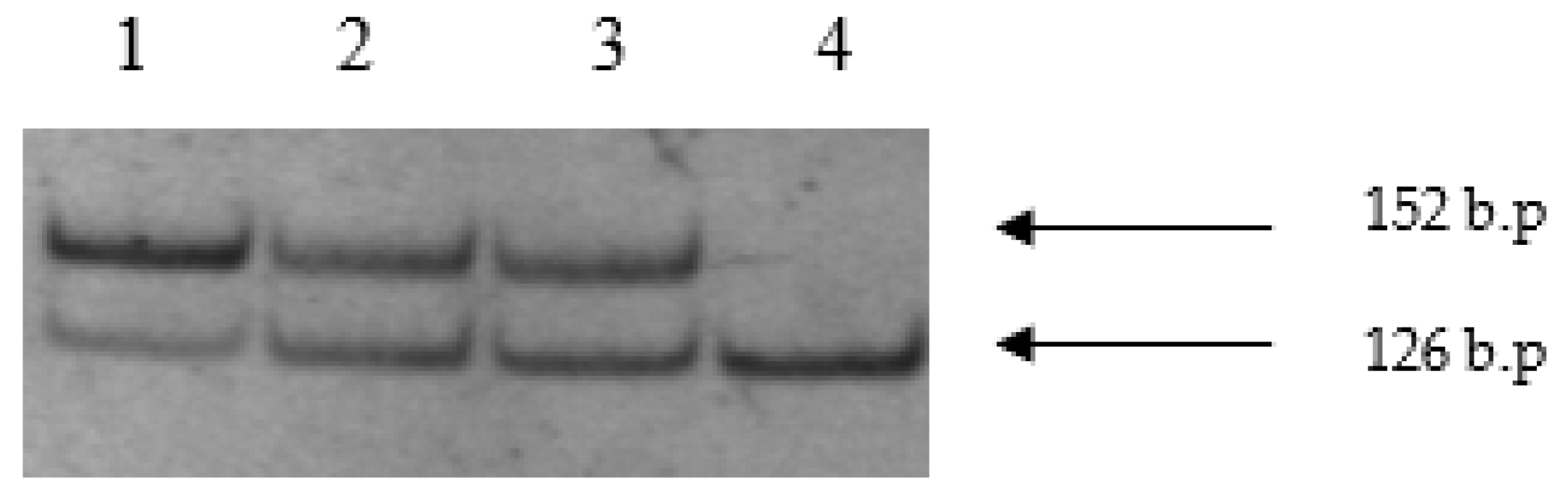
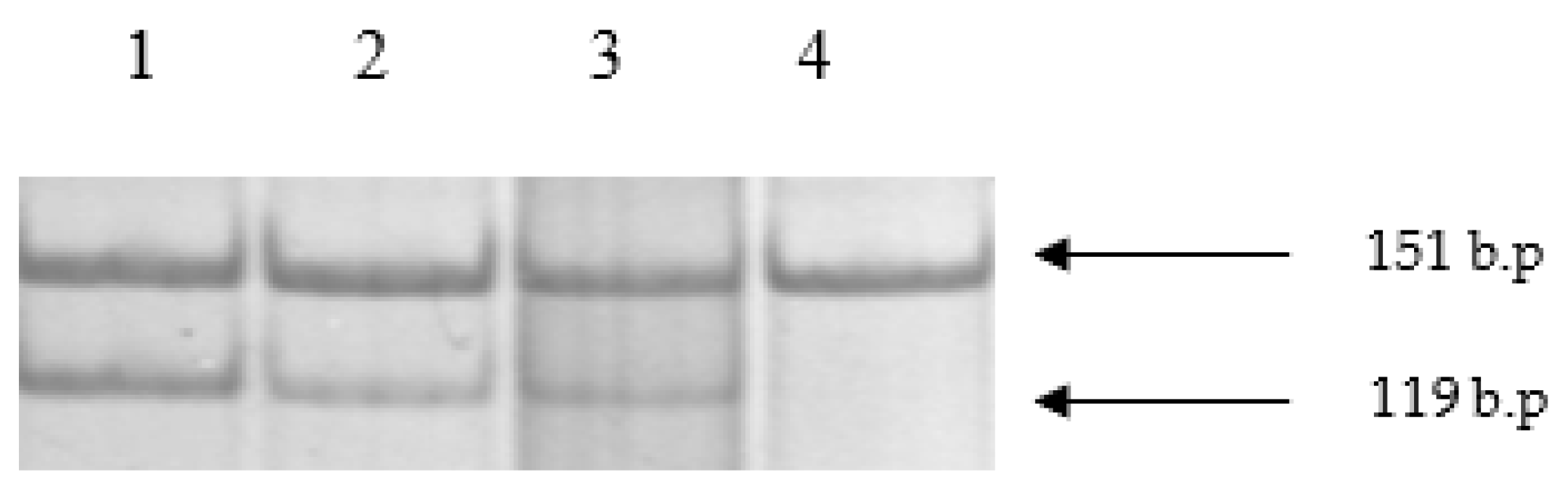
Appendix A.1. Analysis of Results
- exon 7 of the SMN1 gene—152 b.p. exon 8 of the SMN2 gene—151 b.p.
- exon 7 of the SMN2 gene—126 b.p. exon 8 of the SMN1 gene—119 b.p.


References
- Russman, B.S. Spinal Muscular Atrophy: Clinical Classification and Disease Heterogeneity. J. Child Neurol. 2007, 22, 946–951. [Google Scholar] [CrossRef]
- Crawford, T.O. Textbook of Neuromuscular Disorders of Infancy, Childhood, and Adolescence: A Clinician’s Approach, Butterworth-Heinemann; Darras, B., Jones, H.R., Jr., Ryan, M., De Vivo, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2003; Chapter 8; pp. 145–166. [Google Scholar]
- Zabnenkova, V.V.; Dadali, E.L.; Spiridonova, M.G.; Zinchenko, R.A.; Poliakov, A.V. Heterozygous carrier rate for type I–IV proximal spinal muscular atrophy in Chuvashes, Udmurts, and residents of the Moscow region. Russ. J. Genet. 2012, 48, 838–845. [Google Scholar] [CrossRef]
- Zabnenkova, V.V.; Shchagina, O.A.; Polyakov, A.V. Carrier screen of spinal muscular atrophy using a new medical technology «Quantitative detection methods of copy number analysis of SMA locus genes». Med. Genet. 2016, 15, 18–23. (In Russian) [Google Scholar]
- Zabnenkova, V.V.; Dadali, E.L.; Swarovskaya, M.; Zinchenko, R.; Polyakov, A.V. Spinal muscular atrophy carrier frequency in Russian Federation. In Proceedings of the Conference on American Society of Human Genetics (ASHG 2016), Vancouver, BC, Canada, 18–22 October 2016; p. 2476W. [Google Scholar]
- McLean, M.D.; Roy, N.; MacKenzie, A.E.; Salih, M.; Burghes, A.H.; Simard, L.; Korneluk, R.G.; Ikeda, J.E.; Surh, L. Two 5q13 simple tandem repeat loci are in linkage disequilibrium with type 1 spinal muscular atrophy. Hum. Mol. Genet. 1994, 3, 1951–1956. [Google Scholar] [CrossRef]
- Bürglen, L.; Lefebvre, S.; Clermont, O.; Burlet, P.; Viollet, L.; Cruaud, C.; Munnich, A.; Melki, J. Structure and organization of the human survival motor neurone (SMN) gene. Genomics 1996, 32, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Lorson, C.L.; Hahnen, E.; Androphy, E.J.; Wirth, B. A single nucleotide in the SMN gene regulates splicing and is responsible for spinal muscular atrophy. Proc. Natl. Acad. Sci. USA 1999, 96, 6307–6311. [Google Scholar] [CrossRef]
- Rochette, C.F.; Gilbert, N.; Simard, L.R. SMN gene duplication and the emergence of the SMN2 gene occurred in distinct hominids: SMN2 is unique to Homo sapiens. Hum. Genet. 2001, 108, 255–266. [Google Scholar] [CrossRef]
- Jędrzejowska, M. Advances in Newborn Screening and Presymptomatic Diagnosis of Spinal Muscular Atrophy. Degener. Neurol. Neuromuscul. Dis. 2020, 10, 39–47. [Google Scholar] [CrossRef]
- Su, Y.N.; Hung, C.C.; Lin, S.Y.; Chen, F.Y.; Chern, J.P.; Tsai, C.; Chang, T.S.; Yang, C.C.; Li, H.; Ho, H.N.; et al. Carrier Screening for Spinal Muscular Atrophy (SMA) in 107,611 Pregnant Women during the Period 2005–2009: A Prospective Population-Based Cohort Study. PLoS ONE 2011, 6, e17067. [Google Scholar] [CrossRef] [PubMed]
- Kucera, K.S.; Taylor, J.L.; Robles, V.R.; Clinard, K.; Migliore, B.; Boyea, B.L.; Okoniewski, K.C.; Duparc, M.; Rehder, C.W.; Shone, S.; et al. Presymptomatic Diagnosis of Spinal Muscular Atrophy Through Newborn Screening. J. Pediatr. 2021, 190, 124–129.e121. [Google Scholar] [CrossRef]
- Dangouloff, T.; Vrščaj, E.; Servais, L.; Osredkar, D.; SMA NBS World Study Group. Newborn screening programs for spinal muscular atrophy worldwide: Where we stand and where to go. Neuromuscul. Disord. 2021, 31, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Ogino, S.; Wilson, R.; Gold, B. New insights on the evolution of the SMN1 and SMN2 region: Simulation and meta-analysis for allele and haplotype frequency calculations. Eur. J. Hum. Genet. 2004, 12, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Hale, K.; Ojodu, J.; Singh, S. Landscape of Spinal Muscular Atrophy Newborn Screening in the United States: 2018–2021. Int. J. Neonatal Screen. 2021, 7, 33. [Google Scholar] [CrossRef]
- Wirth, B.; Herz, M.; Wetter, A.; Moskau, S.; Hahnen, E.; Rudnik-Schöneborn, S.; Wienker, T.; Zerres, K. Quantitative Analysis of Survival Motor Neuron Copies: Identification of Subtle SMN1 Mutations in Patients with Spinal Muscular Atrophy, Genotype-Phenotype Correlation, and Implications for Genetic Counseling. Am. J. Hum. Genet. 1999, 64, 1340–1356. [Google Scholar] [CrossRef] [PubMed]
- Feldkötter, M.; Schwarzer, V.; Wirth, R.; Wienker, T.F.; Wirth, B. Quantitative Analyses of SMN1 and SMN2 Based on Real-Time LightCycler PCR: Fast and Highly Reliable Carrier Testing and Prediction of Severity of Spinal Muscular Atrophy. Am. J. Hum. Genet. 2002, 70, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Vill, K.; Schwartz, O.; Blaschek, A.; Gläser, D.; Nennstiel, U.; Wirth, B.; Burggraf, S.; Röschinger, W.; Becker, M.; Czibere, L.; et al. Newborn screening for spinal muscular atrophy in Germany: Clinical results after 2 years. Orphanet. J. Rare Dis. 2021, 16, 153. [Google Scholar] [CrossRef]
- Boemer, F.; Caberg, J.H.; Beckers, P.; Dideberg, V.; di Fiore, S.; Bours, V.; Marie, S.; Dewulf, J.; Marcelis, L.; Deconinck, N.; et al. Three years pilot of spinal muscular atrophy newborn screening turned into official program in Southern Belgium. Sci. Rep. 2021, 11, 19922. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Calabro, V.; Chong, B.; Gardiner, N.; Cowie, S.; du Sart, D. Population screening and cascade testing for carriers of SMA. Eur. J. Hum. Genet. 2007, 15, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Calì, F.; Ruggeri, G.; Chiavetta, V.; Scuderi, C.; Bianca, S.; Barone, C.; Ragalmuto, A.; Schinocca, P.; Vitello, G.A.; Romano, V.; et al. Carrier screening for spinal muscular atrophy in Italian population. J. Genet. 2014, 93, 179–181. [Google Scholar] [CrossRef]
- Abiusi, E.; Vaisfeld, A.; Fiori, S.; Novelli, A.; Spartano, S.; Faggiano, M.V.; Giovanniello, T.; Angeloni, A.; Vento, G.; Santoloci, R.; et al. Experience of a 2-year spinal muscular atrophy NBS pilot study in Italy: Towards specific guidelines and standard operating procedures for the molecular diagnosis. J. Med. Genet. 2022, 2022, 108873. [Google Scholar] [CrossRef]
- McAndrew, P.E.; Parsons, D.W.; Simard, L.R.; Rochette, C.; Ray, P.N.; Mendell, J.R.; Prior, T.W.; Burghes, A.H. Identification of proximal spinal muscular atrophy carriers and patients by analysis of SMNT and SMNC gene copy number. Am. J. Hum. Genet. 1997, 60, 1411–1422. [Google Scholar] [CrossRef] [PubMed]
- McMillan, H.J.; Kernohan, K.D.; Yeh, E.; Amburgey, K.; Boyd, J.; Campbell, C.; Dowling, J.J.; Gonorazky, H.; Marcadier, J.; Tarnopolsky, M.A.; et al. Newborn Screening for Spinal Muscular Atrophy: Ontario Testing and Follow-up Recommendations. Can. J. Neurol. Sci. 2021, 48, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Diep Tran, T.; Kroepfl, T.; Saito, M.; Nagura, M.; Ichiseki, H.; Kubota, M.; Toda, T.; Sakakihara, Y. The gene copy ratios of SMN1/SMN2 in Japanese carriers with type I spinal muscular atrophy. Brain Dev. 2001, 23, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Kimizu, T.; Ida, S.; Okamoto, K.; Awano, H.; Niba, E.T.E.; Wijaya, Y.O.S.; Okazaki, S.; Shimomura, H.; Lee, T.; Tominaga, K.; et al. Spinal Muscular Atrophy: Diagnosis, Incidence, and Newborn Screening in Japan. Int. J. Neonatal Screen. 2021, 7, 45. [Google Scholar] [CrossRef]
- Chan, V.; Yip, B.; Yam, I.; Au, P.; Lin, C.K.; Wong, V.; Chan, T.K. Carrier incidence for spinal muscular atrophy in southern Chinese. J. Neurol. 2004, 251, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Lin, C.H.; Yin, X.; Zhu, L.; Yang, J.; Shen, Y.; Yang, C.; Chen, X.; Hu, H.; Ma, Q.; et al. Newborn Screening for Spinal Muscular Atrophy in China Using DNA Mass Spectrometry. Front. Genet. 2019, 10, 1255. [Google Scholar] [CrossRef]
- The European Alliance for Newborn Screening in Spinal Muscular Atrophy. Available online: https://www.sma-screening-alliance.org/map/ (accessed on 22 December 2022).
- Gailite, L.; Sterna, O.; Konika, M.; Isakovs, A.; Isakova, J.; Micule, I.; Setlere, S.; Diriks, M.; Auzenbaha, M. New-Born Screening for Spinal Muscular Atrophy: Results of a Latvian Pilot Study. Int. J. Neonatal Screen. 2022, 8, 15. [Google Scholar] [CrossRef]


| Country/Region | Project Start Month | Carrier Frequency/Estimated 5q SMA Prevalence | Methodology Tier 1/Tier 2 | Detected Cases per Number of Newborns | 5q SMA Prevalence According to the Screening Results | Estimated 5q SMA Prevalence |
|---|---|---|---|---|---|---|
| Taiwan | 11/14 | 1:48 [11] | qPCR/ MLPA/ | 7:120,267 [12] | 1:17,181 [13] | 1:8968 |
| USA | 01/16 | 1:53 [14] | var methods ddPCR-qPCR | 180:2,395,718 [13,15] | 1:13,310 [1] | 1:11,236 |
| Germany | 01/18 | 1:30 [16,17] | qPCR/ MLPA | 43:297,163 [18] | 1:6911 [13] | 1:3600 |
| Belgium | 03/18 | No data | qPCR/ MLPA | 9:136,339 [13,19] | 1:15,149 | No data |
| Australia | 08/18 | 1:49 [20] | qPCR/ ddPCR | 18:202,388 [13] | 1:11,244 | 1:6724 |
| Italy | 09/19 | 1:35 [21] | qPCR/ qPCR | 15:90,885 [22] | 1:6059 | 1:4900 |
| Canada | 01/20 | 1:54 [23] | Mass/ MLPA | 5:139,810 [13,24] | 1:27,962 | 1:11,664 |
| Japan | 05/20 | 1:32,362 (according to the retrospective analysis data 2007–2016) [25] | qPCR/ MLPA | 0:22,209 [13] | Not detected | 1:32,362 |
| Japan (Osaka) | 02/21 | 1:32,362 | qPCR/ MLPA | 0:10,000 [26] | Not detected | 1:32,362 |
| China | 03/18 | 1:53 [27] | The Agena iPLEX assay (Mass)/ MLPA | 3:29,364 [28] | 1:9788 | 1:11,236 |
| Latvia | 02/21 | 1:9091 (according to the retrospective analysis data 2007–2017) [29] | qPCR/ qPCR and MLPA | 2:10,411 [30] | 1:5206 | 1:9069 |
| Russia (Moscow) | 08/19 | 1:36 1:5184 [3] | The Melt Assay/ MLPA | 3:23,405 | 1:7801 | 1:5184 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikhalchuk, K.; Shchagina, O.; Chukhrova, A.; Zabnenkova, V.; Chausova, P.; Ryadninskaya, N.; Vlodavets, D.; Kutsev, S.I.; Polyakov, A. Pilot Program of Newborn Screening for 5q Spinal Muscular Atrophy in the Russian Federation. Int. J. Neonatal Screen. 2023, 9, 29. https://doi.org/10.3390/ijns9020029
Mikhalchuk K, Shchagina O, Chukhrova A, Zabnenkova V, Chausova P, Ryadninskaya N, Vlodavets D, Kutsev SI, Polyakov A. Pilot Program of Newborn Screening for 5q Spinal Muscular Atrophy in the Russian Federation. International Journal of Neonatal Screening. 2023; 9(2):29. https://doi.org/10.3390/ijns9020029
Chicago/Turabian StyleMikhalchuk, Kristina, Olga Shchagina, Alena Chukhrova, Viktoria Zabnenkova, Polina Chausova, Nina Ryadninskaya, Dmitry Vlodavets, Sergei I. Kutsev, and Alexander Polyakov. 2023. "Pilot Program of Newborn Screening for 5q Spinal Muscular Atrophy in the Russian Federation" International Journal of Neonatal Screening 9, no. 2: 29. https://doi.org/10.3390/ijns9020029
APA StyleMikhalchuk, K., Shchagina, O., Chukhrova, A., Zabnenkova, V., Chausova, P., Ryadninskaya, N., Vlodavets, D., Kutsev, S. I., & Polyakov, A. (2023). Pilot Program of Newborn Screening for 5q Spinal Muscular Atrophy in the Russian Federation. International Journal of Neonatal Screening, 9(2), 29. https://doi.org/10.3390/ijns9020029