Functional Imaging of the Ocular Fundus Using an 8-Band Retinal Multispectral Imaging System


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Hyperspectral Fundus Camera
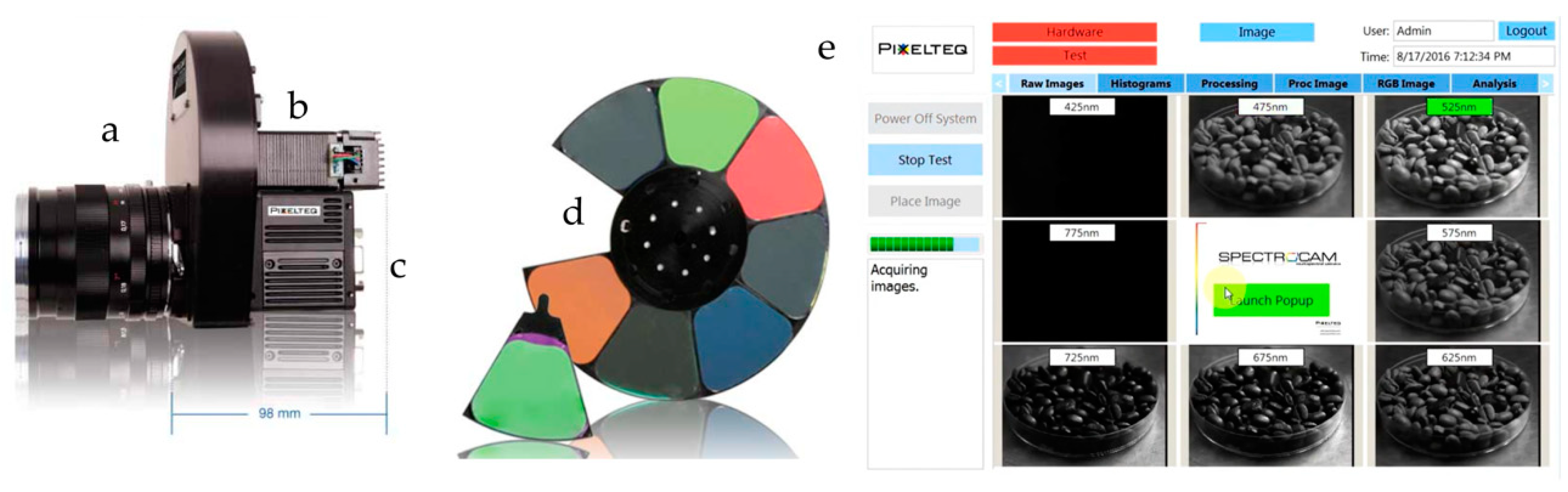
2.2. The Multispectral Fundus Camera
2.3. Participants and Image Acquisition
2.4. Data Pre-Processing and Analysis
- 1.
- A linear function g(λ) with g(A) = RA and g(C) = RC is determined.
- 2.
- A linear function f(λ) with f(A) = XA and f(C) = XC is determined.
- 3.
- The measured data are added by the difference between g(λ) and f(λ):
- 4.
- A second correction step is applied to the data X′(λ) in order to correct for different conditions of illumination and measurement between the sample spectrum and the reference spectra. In this correction step the data X′(λ) is stretched and compressed around the line g(λ) to match the reference data at isosbestic wavelength B:
- 5.
- The oxygen saturation (OS) is indicated by X″(D) on a linear scale between RHb(D) and RHbO(D):
3. Results
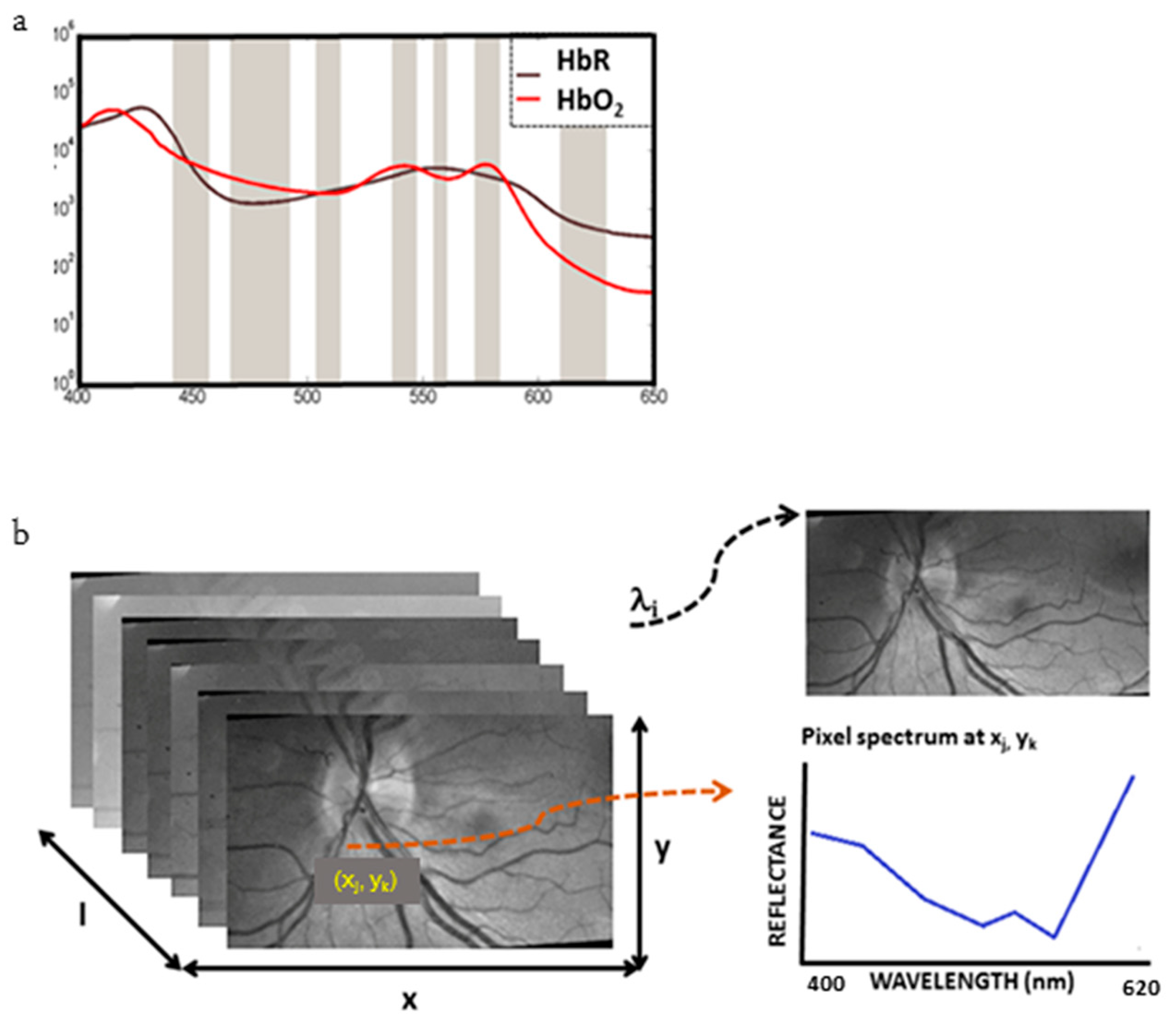
3.1. The Ocular Fundus Hypercube
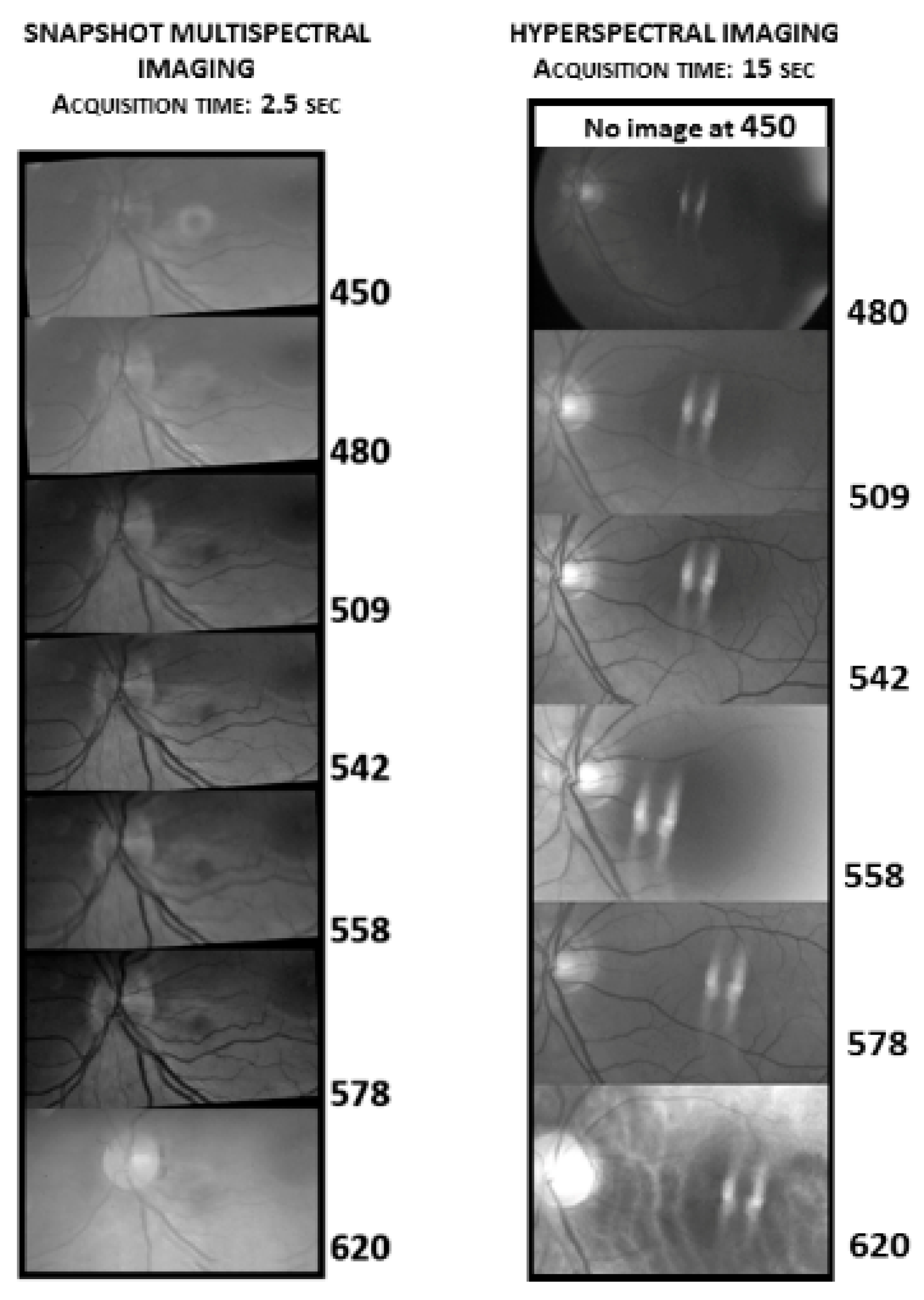
3.2. Comparison of MSI with HSI
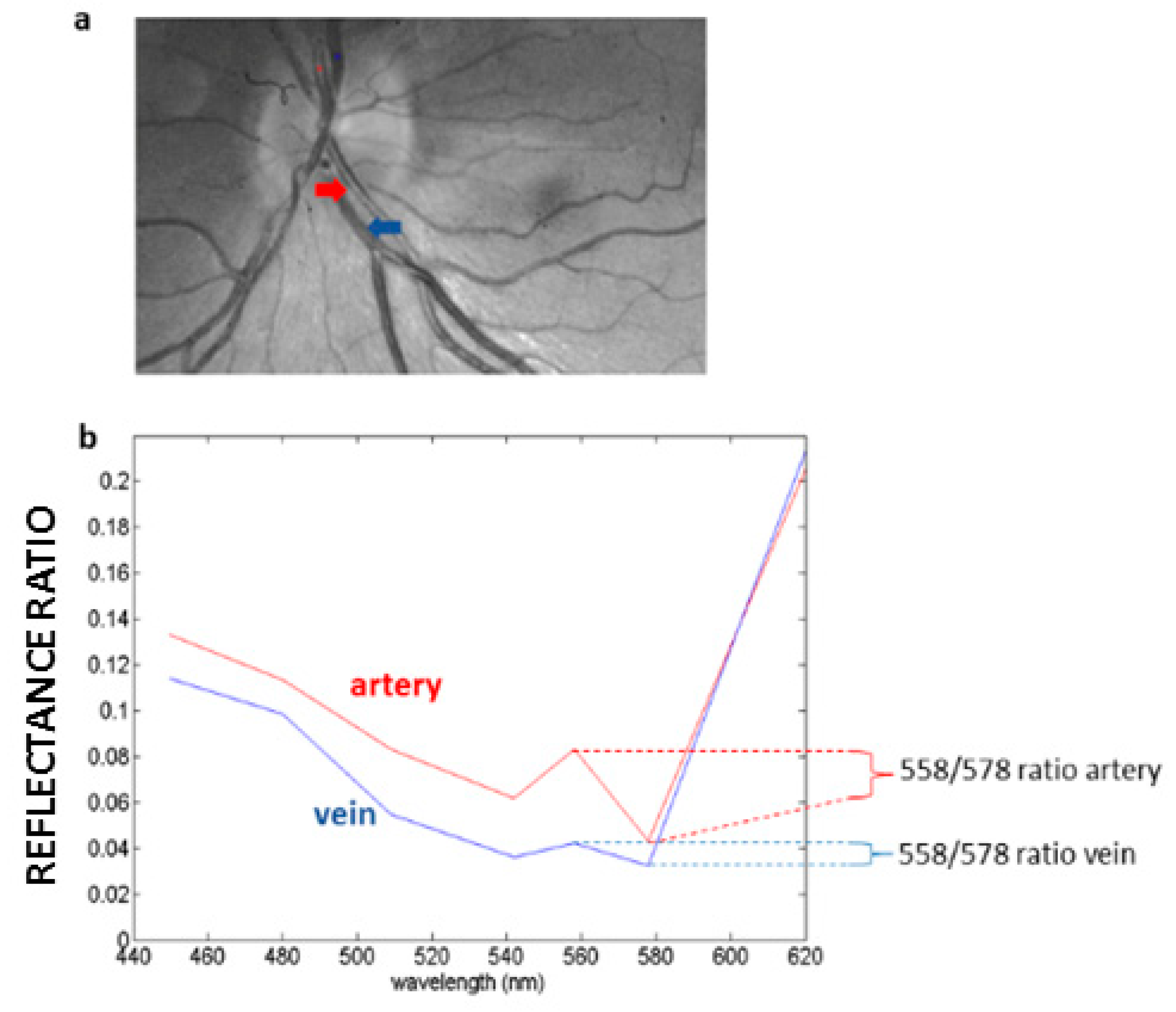
3.3. Haemoglobin Reflectance Measurements in the Retina
3.4. Estimation of Relative Oxygen Saturation from Reflectance Spectra
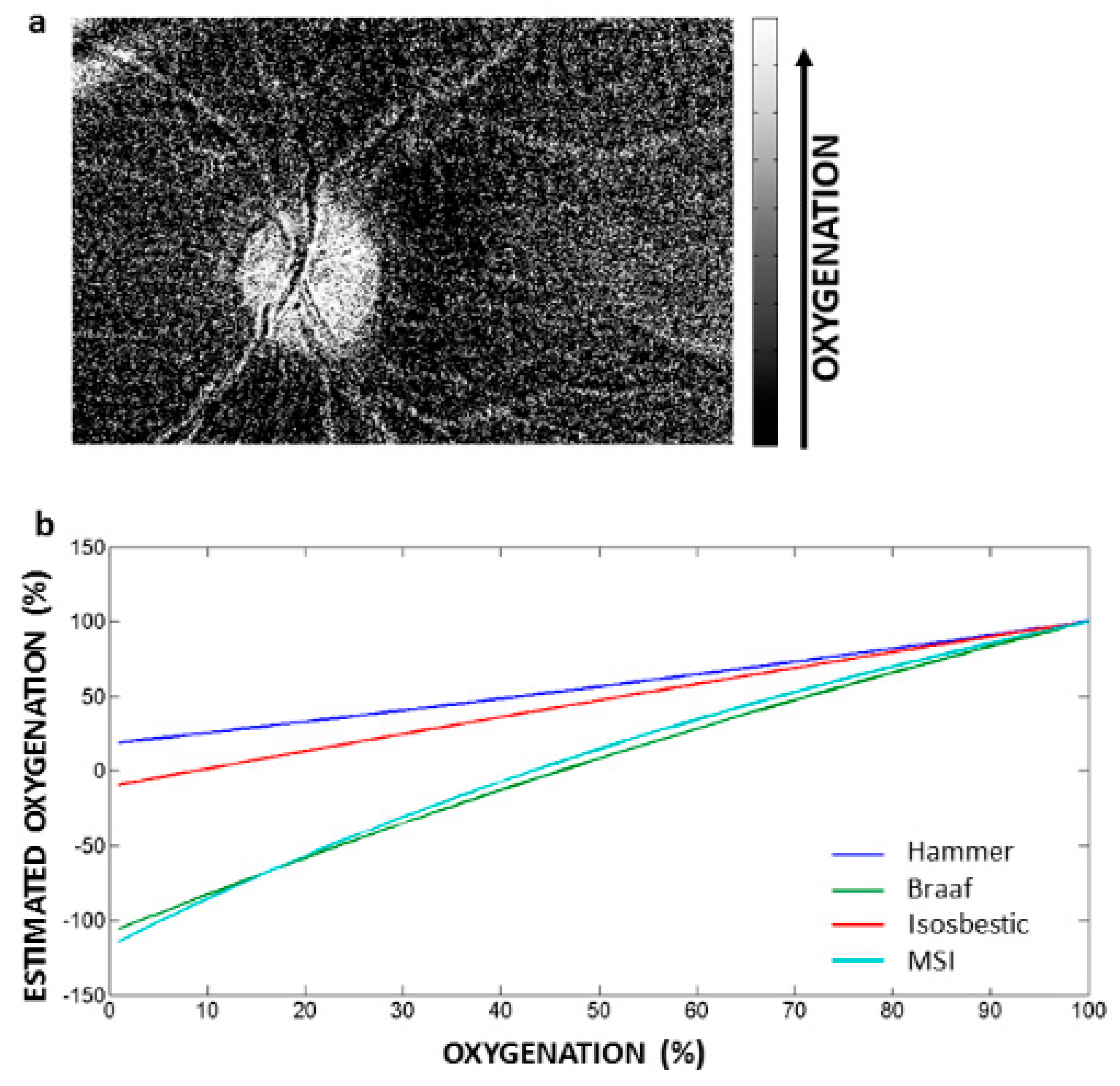
3.5. Application of the Hammer Correction Algorithm to estimate Relative Retinal Oxygen Saturation
3.6. Uneven Distribution of HbO2 in Retinal Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morris, H.R.; Hoyt, C.C.; Treado, P.J. Imaging Spectrometers for Fluorescence and Raman Microscopy - Acoustooptic and Liquid-Crystal Tunable Filters. Appl. Spectrosc. 1994, 48, 857–866. [Google Scholar] [CrossRef]
- Choi, H.; Wadduwage, D.; Matsudaira, P.T.; So, P.T.C. Depth resolved hyperspectral imaging spectrometer based on structured light illumination and Fourier transform interferometry. Biomed. Opt. Express 2014, 5, 3494–3507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gramatikov, B.I. Modern technologies for retinal scanning and imaging: An introduction for the biomedical engineer. Biomed. Eng. Online 2014, 13, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Barbastathis, G.; Psaltis, D. Volume holographic hyperspectral imaging. Appl. Opt. 2004, 43, 3581–3599. [Google Scholar] [CrossRef] [Green Version]
- Hagen, N.; Kudenov, M.W. Review of snapshot spectral imaging technologies. Opt. Eng. 2013, 52, 090901. [Google Scholar] [CrossRef] [Green Version]
- Gorman, A.; Fletcher-Holmes, D.W.; Harvey, A.R. Generalization of the Lyot filter and its application to snapshot spectral imaging. Opt. Express 2010, 18, 5602–5608. [Google Scholar] [CrossRef]
- Mordant, D.J.; Al-Abboud, I.; Muyo, G.; Gorman, A.; Sallam, A.; Ritchie, P.; Harvey, A.R.; McNaught, A.I. Spectral imaging of the retina. Eye 2011, 25, 309–320. [Google Scholar] [CrossRef] [Green Version]
- Hirohara, Y.; Okawa, Y.; Mihashi, T.; Yamaguchi, T.; Nakazawa, N.; Tsuruga, Y.; Aoki, H.; Maeda, N.; Uchida, I.; Fujikado, T. Validity of retinal oxygen saturation analysis: Hyperspectral imaging in visible wavelength with fundus camera and liquid crystal wavelength tunable filter. Opt. Rev. 2007, 14, 151–158. [Google Scholar] [CrossRef]
- Johnson, W.R.; Wilson, D.W.; Fink, W.; Humayun, M.; Bearman, G. Snapshot hyperspectral imaging in ophthalmology. J. Biomed. Opt. 2007, 12. [Google Scholar] [CrossRef] [Green Version]
- Muqit, M.M.K.; Denniss, J.; Nourrit, V.; Marcellino, G.R.; Henson, D.B.; Schiessl, I.; Stanga, P.E. Spatial and Spectral Imaging of Retinal Laser Photocoagulation Burns. Invest. Ophthalmol. Vis. Sci. 2011, 52, 994–1002. [Google Scholar] [CrossRef] [Green Version]
- Nourrit, V.; Denniss, J.; Muqit, M.M.K.; Schiessl, I.; Fenerty, C.; Stanga, P.E.; Henson, D.B. High-resolution hyperspectral imaging of the retina with a modified fundus camera. J. Fr. Ophtalmol. 2010, 33, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Tiedeman, J.S.; Kirk, S.E.; Srinivas, S.; Beach, J.M. Retinal oxygen consumption during hyperglycemia in patients with diabetes without retinopathy. Ophthalmology 1998, 105, 31–36. [Google Scholar] [CrossRef]
- Masquelier, T.; Portelli, G.; Kornprobst, P. Microsaccades enable efficient synchrony-based coding in the retina: A simulation study. Sci. Rep. 2016, 6, 24086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Carvalho, J.E.R.; Verbraak, F.D.; Aalders, M.C.; van Noorden, C.J.; Schlingemann, R.O. Recent advances in ophthalmic molecular imaging. Surv. Ophthalmol. 2014, 59, 393–413. [Google Scholar] [CrossRef] [PubMed]
- Geladi, P.; Burger, J.; Lestander, T. Hyperspectral imaging: Calibration problems and solutions. Chemometr. Intell. Lab. 2004, 72, 209–217. [Google Scholar] [CrossRef]
- Everdell, N.L.; Styles, I.B.; Calcagni, A.; Gibson, J.; Hebden, J.; Claridge, E. Multispectral imaging of the ocular fundus using light emitting diode illumination. Rev. Sci. Instrum. 2010, 81, 093706. [Google Scholar] [CrossRef] [Green Version]
- Beach, J.M.; Schwenzer, K.J.; Srinivas, S.; Kim, D.; Tiedeman, J.S. Oximetry of retinal vessels by dual-wavelength imaging: Calibration and influence of pigmentation. J. Appl. Physiol. 1999, 86, 748–758. [Google Scholar] [CrossRef] [Green Version]
- Pittman, R.N.; Duling, B.R. Measurement of Percent Oxyhemoglobin in Microvasculature. J. Appl. Physiol. 1975, 38, 321–327. [Google Scholar] [CrossRef]
- Hammer, M.; Thamm, E.; Schweitzer, D. A simple algorithm for in vivo ocular fundus oximetry compensating for non-haemoglobin absorption and scattering. Phys. Med. Biol. 2002, 47, N233–N238. [Google Scholar] [CrossRef] [Green Version]
- Fenton, B.M.; Gayeski, T.E.J. Determination of Microvascular Oxyhemoglobin Saturations Using Cryospectrophotometry. Am. J. Physiol. 1990, 259, H1912–H1920. [Google Scholar] [CrossRef]
- Pittman, R.N.; Duling, B.R. New Method for Measurement of Percent Oxyhemoglobin. J. Appl. Physiol. 1975, 38, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, D.; Hammer, M.; Kraft, J.; Thamm, E.; Konigsdorffer, E.; Strobel, J. In vivo measurement of the oxygen saturation of retinal vessels in healthy volunteers. IEEE Trans. Biomed. Eng. 1999, 46, 1454–1465. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, D.; Thamm, E.; Hammer, M.; Kraft, J. A new method for the measurement of oxygen saturation at the human ocular fundus. Int. Ophthalmol. 2001, 23, 347–353. [Google Scholar] [CrossRef]
- Beach, J. Pathway to Retinal Oximetry. Transl. Vis. Sci. Technol. 2014, 3, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delori, F.C.; Webb, R.H.; Sliney, D.H. Maximum permissible exposures for ocular safety (ANSI 2000), with emphasis on ophthalmic devices. J. Opt. Soc. Am. A 2007, 24, 1250–1265. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.J.; Dhanoa, M.S.; Lister, S.J. Standard Normal Variate Transformation and De-Trending of near-Infrared Diffuse Reflectance Spectra. Appl. Spectrosc. 1989, 43, 772–777. [Google Scholar] [CrossRef]
- Lowe, D.G. Distinctive image features from scale-invariant keypoints. Int. J. Comput. Vis. 2004, 60, 91–110. [Google Scholar] [CrossRef]
- Braaf, B.; Nadort, A.; Faber, D.; ter Wee, R.; van Leeuwen, T.; Aalders, M. Blood oxygen saturation of frozen tissue determined by hyperspectral imaging. In Proceedings of the Imaging, Manipulation, and Analysis of Biomolecules, Cells, and Tissues VI, San Jose, CA, USA, 21–23 January 2008. [Google Scholar] [CrossRef]
- Desjardins, M.; Sylvestre, J.P.; Jafari, R.; Kulasekara, S.; Rose, K.; Trussart, R.; Arbour, J.D.; Hudson, C.; Lesage, F. Preliminary investigation of multispectral retinal tissue oximetry mapping using a hyperspectral retinal camera. Exp. Eye Res. 2016, 146, 330–340. [Google Scholar] [CrossRef]
- Shore, J.; Lubin, B. Spectral goodness of fit for network models. Soc. Netw. 2015, 43, 16–27. [Google Scholar] [CrossRef] [Green Version]
- Delori, F.C. Noninvasive technique for oximetry of blood in retinal vessels. Appl. Opt. 1988, 27, 1113–1125. [Google Scholar] [CrossRef]
- Smith, M.H. Optimum wavelength combinations for retinal vessel oximetry. Appl. Opt. 1999, 38, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Bosschaart, N.; Edelman, G.J.; Aalders, M.C.G.; van Leeuwen, T.G.; Faber, D.J. A literature review and novel theoretical approach on the optical properties of whole blood. Laser Med. Sci. 2014, 29, 453–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammer, M.; Leistritz, S.; Leistritz, L.; Schweitzer, D. Light paths in retinal vessel oxymetry. IEEE Trans. Biomed. Eng. 2001, 48, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Styles, I.B.; Calcagni, A.; Claridge, E.; Orihuela-Espina, F.; Gibson, J.M. Quantitative analysis of multi-spectral fundus images. Med. Image Anal. 2006, 10, 578–597. [Google Scholar] [CrossRef] [Green Version]
- Hammer, M.; Roggan, A.; Schweitzer, D.; Muller, G. Optical-Properties of Ocular Fundus Tissues-an in-Vitro Study Using the Double-Integrating-Sphere Technique and Inverse Monte-Carlo Simulation. Phys. Med. Biol. 1995, 40, 963–978. [Google Scholar] [CrossRef] [Green Version]
- Vankampen, E.J.; Zijlstra, W.G. Spectrophotometry of Hemoglobin and Hemoglobin Derivatives. Adv. Clin. Chem. 1983, 23, 199–257. [Google Scholar] [CrossRef]
- Devor, A.; Sakadzic, S.; Saisan, P.A.; Yaseen, M.A.; Roussakis, E.; Srinivasan, V.J.; Vinogradov, S.A.; Rosen, B.R.; Buxton, R.B.; Dale, A.M.; et al. “Overshoot” of O(2) is required to maintain baseline tissue oxygenation at locations distal to blood vessels. J. Neurosci. 2011, 31, 13676–13681. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| This Study | Hammer et al. | Braaf et al. | Isosbestic | |
|---|---|---|---|---|
| A | 509 | 522 | 530 | 522 |
| B | 542 | 569 | 542 | 549 |
| C | 578 | 586 | 582 | 586 |
| D | 558 | 560 | 562 | 560 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Carvalho, E.R.; Hoveling, R.J.M.; van Noorden, C.J.F.; Schlingemann, R.O.; Aalders, M.C.G. Functional Imaging of the Ocular Fundus Using an 8-Band Retinal Multispectral Imaging System. Instruments 2020, 4, 12. https://doi.org/10.3390/instruments4020012
de Carvalho ER, Hoveling RJM, van Noorden CJF, Schlingemann RO, Aalders MCG. Functional Imaging of the Ocular Fundus Using an 8-Band Retinal Multispectral Imaging System. Instruments. 2020; 4(2):12. https://doi.org/10.3390/instruments4020012
Chicago/Turabian Stylede Carvalho, Emanuel R., Richelle J. M. Hoveling, Cornelis J. F. van Noorden, Reinier O. Schlingemann, and Maurice C. G. Aalders. 2020. "Functional Imaging of the Ocular Fundus Using an 8-Band Retinal Multispectral Imaging System" Instruments 4, no. 2: 12. https://doi.org/10.3390/instruments4020012
APA Stylede Carvalho, E. R., Hoveling, R. J. M., van Noorden, C. J. F., Schlingemann, R. O., & Aalders, M. C. G. (2020). Functional Imaging of the Ocular Fundus Using an 8-Band Retinal Multispectral Imaging System. Instruments, 4(2), 12. https://doi.org/10.3390/instruments4020012