Acute Cardiometabolic Responses to Multi-Modal Integrative Neuromuscular Training in Children

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Peak Aerobic Capacity Testing
2.3. Integrative Neuromuscular Training Protocol
2.4. Treadmill Protocol
2.5. Experimental Measurements: Oxygen Uptake and Heart Rate
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Aubert, S.; Barnes, J.; Abdeta, C.; Abi Nader, P.; Adeniyi, A.; Aguilar-Farias, N.; Andrade Tenesaca, D.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis From 49 Countries. J. Phys. Act. Health 2018, 15, S251–S273. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A.; Rial Rebullido, T.; MacDonald, J. The unsolved problem of paediatric physical inactivity: It is time for a new perspective. Acta Paediatr. 2018, 107, 1857–1859. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, B.; Henley, W.; Wilkin, T. Effectiveness of intervention on physical activity of children: Systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). BMJ 2012, 345, e5888. [Google Scholar] [CrossRef] [PubMed]
- Carlin, A.; Murphy, M.; Nevill, A.; Gallagher, A. Effects of a peer-led Walking In ScHools intervention (the WISH study) on physical activity levels of adolescent girls: a cluster randomised pilot study. Trials 2018, 19, 31. [Google Scholar] [CrossRef] [PubMed]
- Villa-González, E.; Ruiz, J.; Mendoza, J.; Chillón, P. Effects of a school-based intervention on active commuting to school and health-related fitness. BMC Public Health 2017, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Hermosa, A.; Martínez-Vizcaíno, V.; Alvarez-Bueno, C.; García-Prieto, J.; Pardo-Guijarro, M.; Sánchez-López, M. No association between active commuting to school, adiposity, fitness, and cognition in Spanish children: The MOVI-KIDS Study. J. Sch. Health 2018, 88, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, G.; Cohen, D. Temporal trends in muscular fitness of English 10-year-olds 1998–2014: An allometric approach. J. Sci. Med. Sport 2019, 22, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Fraser, B.; Blizzard, L.; Tomkinson, G.; Lycett, K.; Wake, M.; Burgner, D.; Ranganathan, S.; Juonala, M.; Dwyer, T.; Venn, A.; et al. The great leap backward: changes in the jumping performance of Australian children aged 11-12-years between 1985 and 2015. J. Sports Sci. 2019, 37, 748–754. [Google Scholar] [CrossRef]
- Smith, J.; Eather, N.; Weaver, R.; Riley, N.; Beets, M.; Lubans, D. Behavioral correlates of muscular fitness in children and adolescents: A systematic review. Sports Med. 2019. epub ahead of print. [Google Scholar] [CrossRef]
- Myer, G.; Faigenbaum, A.; Ford, K.; Best, T.; Bergeron, M.; Hewett, T. When to initiate integrative neuromuscular training to reduce sports-related injuries and enhance health in youth? Curr. Sports Med. Rep. 2011, 10, 155–166. [Google Scholar] [CrossRef]
- Faigenbaum, A.; Farrell, A.; Fabiano, M.; Radler, T.; Naclerio, F.; Ratamess, N.; Kang, J.; Myer, G. Effects of integrated neuromuscular training on fitness performance in children. Pediatr. Exerc. Sci. 2011, 23, 573–584. [Google Scholar] [CrossRef]
- Duncan, M.; Eyre, E.; Oxford, S. The effects of 10 weeks Integrated Neuromuscular Training on fundamental movement skills and physical self-efficacy in 6–7 year old children. J. Strength Cond. Res. 2018, 32, 3348–3356. [Google Scholar] [CrossRef] [PubMed]
- Foss, K.; Thomas, S.; Khoury, J.; Myer, G.; Hewett, T. A school-based neuromuscular training program and sport-related injury incidence: A prospective randomized controlled clinical trial. J. Athl. Train. 2018, 53, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Faigenbaum, A.; Kang, J.; Ratamess, N.; Farrell, A.; Ellis, N.; Vought, I.; Bush, J. Acute cardiometabolic responses to medicine ball interval training in children. Int. J. Exerc. Sci. 2018, 11, 886–899. [Google Scholar] [PubMed]
- Faigenbaum, A.; Kang, J.; Ratamess, N.; Farrell, A.; Golda, S.; Stranieri, A.; Coe, J.; Bush, J. Acute cardiometabolic responses to battling rope exercise in children. J. Strength Cond. Res. 2018, 32, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Panagoulis, C.; Chatzinikolaou, A.; Avloniti, A.; Leontsini, D.; Deli, C.; Draganidis, D.; Stampoulis, T.; Oikonomou, T.; Papanikolaou, K.; Rafailakis, L.; et al. In-season integrative neuromuscular strength training improves performance of early adolescent soccer athletes. J. Strength Cond. Res. 2018. epub before print. [Google Scholar] [CrossRef]
- Tarp, J.; Child, A.; White, T.; Westgate, K.; Bugge, A.; Grøntved, A.; Wedderkopp, N.; Andersen, L.; Cardon, G.; Davey, R.; et al. Physical activity intensity, bout-duration, and cardiometabolic risk markers in children and adolescents. Int. J. Obes. (Lond.) 2018, 42, 1639–1650. [Google Scholar] [CrossRef] [Green Version]
- Aadland, E.; Andersen, L.; Anderssen, S.; Resaland, G.; Kvalheim, O. Associations of volumes and patterns of physical activity with metabolic health in children: A multivariate pattern analysis approach. Prev. Med. 2018, 115, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Stamatakis, E. Relative proportion of vigorous physical activity, total volume of moderate to vigorous activity, and body mass index in youth: the Millennium Cohort Study. Int. J. Obes. (Lond.) 2018, 42, 1239–1242. [Google Scholar] [CrossRef] [Green Version]
- Harris, N.; Dulson, D.; Logan, G.; Warbrick, I.; Merien, F.; Lubans, D. Acute responses to resistance and high-intensity interval training in early adolescents. J. Strength Cond. Res. 2016, 31, 1177–1186. [Google Scholar] [CrossRef]
- Bond, B.; Weston, K.; Williams, C.; Barker, A. Perspectives on high-intensity interval exercise for health promotion in children and adolescents. Open Access J. Sports Med. 2017, 8, 243–265. [Google Scholar] [CrossRef] [PubMed]
- Thivel, D.; Masurier, J.; Baquet, G.; Timmons, B.; Pereira, B.; Berthoin, S.; Duclos, M.; Aucouturier, J. High-intensity interval training in overweight and obese children and adolescents: systematic review and meta-analysis. J. Sports Med. Phys. Fitness 2019, 59, 310–324. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Educating the Student Body: Taking Physical Activity and Physical Education to School; The National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- Kotte, E.; DE Groot, J.; Bongers, B.; Winkler, A.; Takken, T. Validity and reproducibility of a new treadmill protocol: The fitkids treadmill test. Med. Sci. Sports Exerc. 2015, 47, 2241–2247. [Google Scholar] [CrossRef]
- Armstrong, N.; McManus, A. Aerobic Fitness. In Oxford Textbook of Children’s Sport and Exercise Medicine, 3rd ed.; Armstrong, N., van Mechelen, W., Eds.; Oxford University Press: Oxford, UK, 2017; pp. 161–180. [Google Scholar]
- Faigenbaum, A.D.; Milliken, L.A.; Cloutier, G.; Westcott, W.L. Perceived exertion during resistance exercise by children. Percept. Mot. Skills 2004, 98, 627–637. [Google Scholar] [CrossRef]
- Faigenbaum, A.; Bush, J.; McLoone, R.; Kreckel, M.; Farrell, A.; Ratamess, N.; Kang, J. Benefits of strength and skill-based training during primary school physical education. J. Strength Cond. Res. 2015, 29, 1255–1262. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans; U.S. Department of Health and Human Services: Washington, DC, USA, 2018; p. 49.
- Butte, N.; Watson, K.; Ridle, Y.K.; Zakeri, I.; McMurray, R.; Pfeiffer, K.; Crouter, S.; Herrmann, S.; Bassett, D.; Long, A.; et al. A Youth Compendium of Physical Activities: Activity Codes and Metabolic Intensities. Med. Sci. Sports Exerc. 2018, 50, 246–256. [Google Scholar] [CrossRef]
- Chuensiri, N.; Tanaka, H.; Suksom, D. The acute effects of supramaximal high-intensity intermittent exercise on vascular function in lean vs. obese prepubescent boys. Pediatr. Exerc. Sci. 2015, 27, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Baquet, G.; Gamelin, F.; Aucouturier, J.; Berthoin, S. Cardiorespiratory responses to continuous and intermittent exercise in children. Int. J. Sports Med. 2017, 38, 755–762. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott, Williams and Wilkins: Baltimore, MD, USA, 2018. [Google Scholar]
- Eddolls, W.; McNarry, M.; Stratton, G.; Winn, C.; Mackintosh, K. High-intensity interval training interventions in children and adolescents: A systematic review. Sports Med. 2017, 47, 2326–2374. [Google Scholar] [CrossRef]
- Birat, A.; Bourdier, P.; Piponnier, E.; Blazevich, A.; Maciejewski, H.; Duché, P.; Ratel, S. Metabolic and fatigue profiles are comparable between prepubertal children and well-trained adult endurance athletes. Front. Pediatr. 2018, 9, 387. [Google Scholar] [CrossRef]
- Ratamess, N.; Rosenberg, J.; Klei, S.; Dougherty, B.; Kang, J.; Smith, C.; Ross, R.; Faigenbaum, A. Comparison of the acute metabolic responses to traditional resistance, body-weight, and battling rope exercise. J. Strength Cond. Res. 2015, 29, 47–57. [Google Scholar] [CrossRef]
- Riddoch, C.; Mattocks, C.; Deere, K.; Saunders, J.; Kirkby, J.; Tilling, K.; Leary, S.; Blair, S.; Ness, A. Objective measurement of levels and patterns of physical activity. Arch. Dis. Childhood 2007, 92, 963–969. [Google Scholar] [CrossRef] [Green Version]
- Robertson, R.; Goss, F.; Aaron, D.; Nagle, E.; Gallagher, M.; Kane, I.; Tessmer, K.; Schafer, M.; Hunt, S. Concurrent muscle hurt and perceived exertion of children during resistance exercise. Med. Sci. Sports Exerc. 2009, 41, 1146–1154. [Google Scholar] [CrossRef]
- Malik, A.; Williams, C.; Bond, B.; Weston, K.; Barker, A. Acute cardiorespiratory, perceptual and enjoyment responses to high-intensity interval exercise in adolescents. Eur. J. Sport Sci. 2017, 17, 1335–1342. [Google Scholar] [CrossRef]
- Sebire, S.; Jago, R.; Fox, K.; Edwards, M.; Thompson, J. Testing a self-determination theory model of children’s physical activity motivation: a cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 111. [Google Scholar] [CrossRef]
- Ratamess, N. ACSM’s Foundations of Strength Training and Conditioning; Lippincott, Williams and Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Nikolaidis, P.; Kintziou, E.; Georgoudis, G.; Afonso, J.; Vancini, R.; Knechtle, B. The effect of body mass index on acute cardiometabolic responses to graded exercise testing in children: A narrative review. Sports 2018, 6, 103. [Google Scholar] [CrossRef]
- Murphy, J.; Button, D.; Chaouachi, A.; Behm, D. Prepubescent males are less susceptible to neuromuscular fatigue following resistance exercise. Eur. J. Appl. Physiol. 2014, 114, 825–835. [Google Scholar] [CrossRef]
- Singh, T.; Alexander, M.; Gauvreau, K.; Curran, T.; Rhodes, Y.; Rhodes, J. Recovery of oxygen consumption after maximal exercise in children. Med. Sci. Sports Exerc. 2011, 43, 555–559. [Google Scholar] [CrossRef]
- Hollis, J.; Williams, A.; Sutherland, R.; Campbell, E.; Nathan, N.; Wolfenden, L.; Morgan, P.; Lubans, D.; Wiggers, J. A systematic review and meta-analysis of moderate-to-vigorous physical activity levels in elementary school physical education lessons. Prev. Med. 2016, 86, 34–54. [Google Scholar] [CrossRef]
- Schlechter, C.; Rosenkranz, R.; Milliken, G.; Dzewaltowski, D. Physical activity levels during youth sport practice: Does coach training or experience have an influence? J. Sports Sci. 2017, 35, 22–28. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Interval (min) | INT EX/set | VO2 | VE | HR | RER | ||||
|---|---|---|---|---|---|---|---|---|---|
| INT | TM | INT | TM | INT | TM | INT | TM | ||
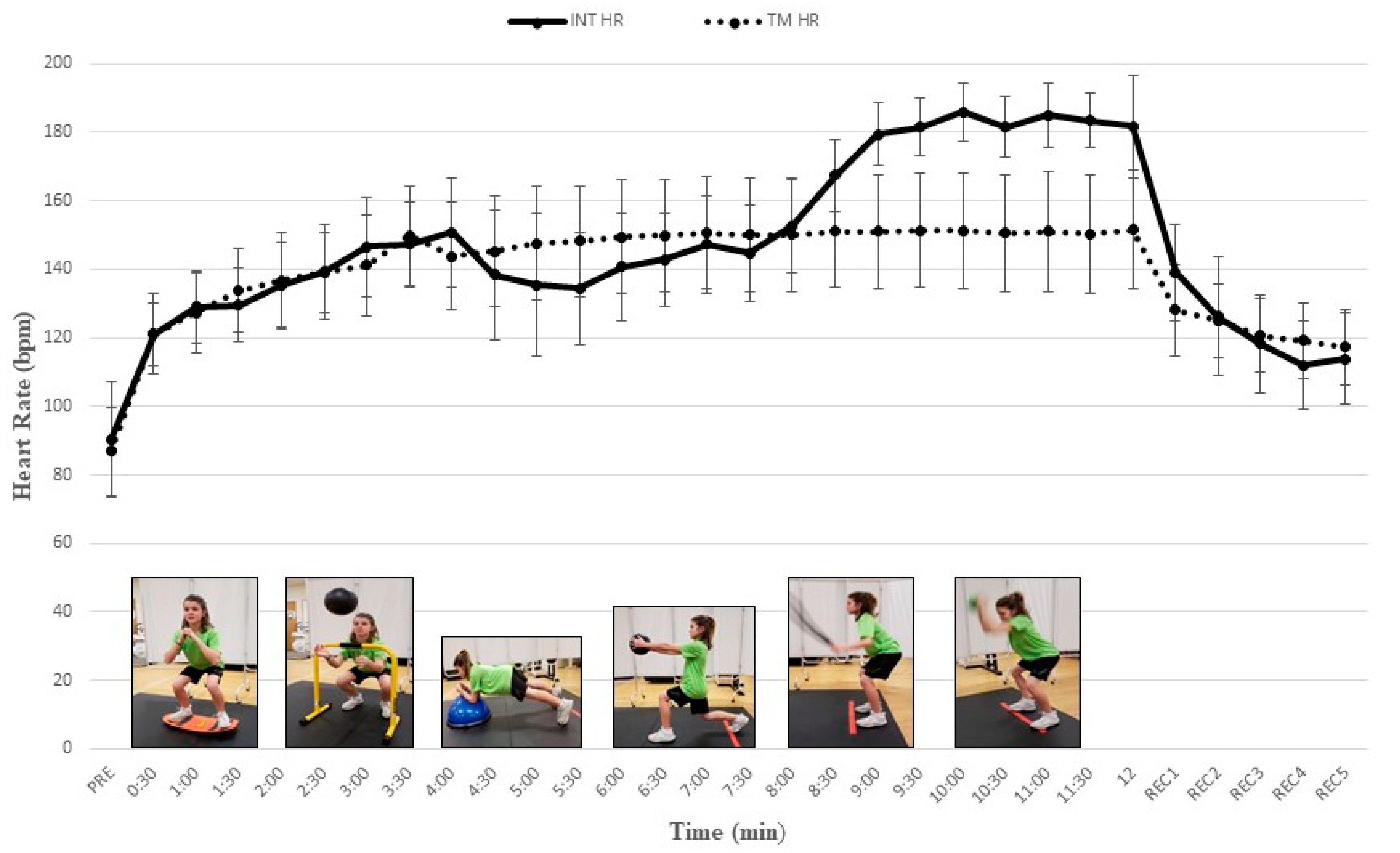
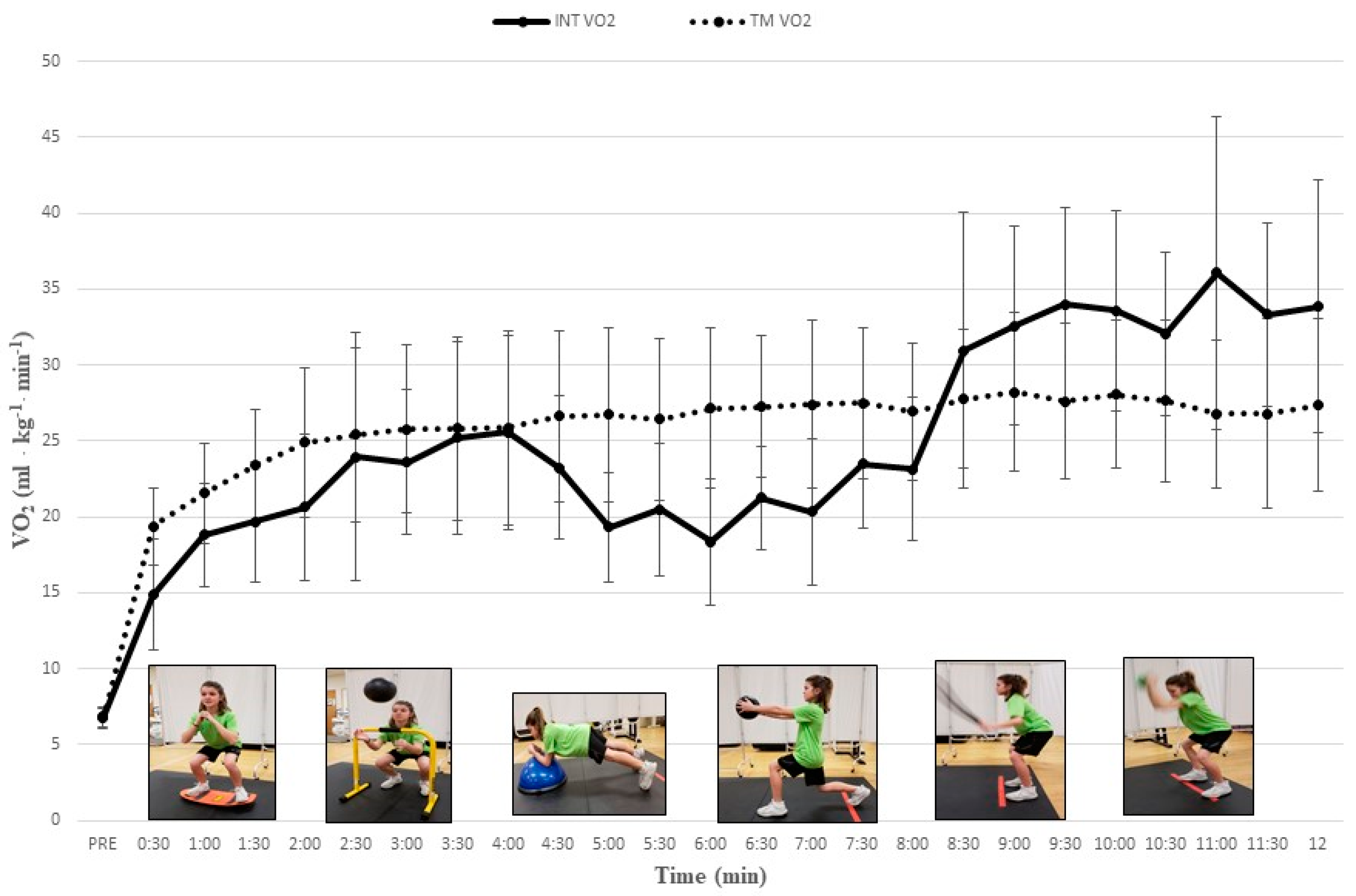
| 1 (0–0.5) | 1/1 | 14.9 ± 3.6 b−l | 19.2 ± 2.5 | 14.9 ± 4.5 b−l | 16.8 ± 2.5 | 121.1 ± 9.0 b−d,g−l | 121.1 ± 11.7 | 0.88 ± 0.07 j−l | 0.82 ± 0.05 |
| 2 (1.0–1.5) | 1/2 | 19.7 ± 3.9 a,d,h−l | 23.4 ± 3.7 | 19.7 ± 6.6 a,d,e,h−l | 20.8 ± 4.5 | 129.6 ± 10.9 a,c−d,g−l | 133.8 ± 12.2 | 0.88 ± 0.08 j−l | 0.85 ± 0.06 |
| 3 (2.0–2.5) | 2/1 | 23.9 ± 8.2 a,j−l | 25.4 ± 5.7 | 24.7 ± 7.7 a,i−l | 23.8 ± 6.0 | 139.1 ± 11.6 a,b,d,i−l | 139.3 ± 13.7 | 0.90 ± 0.07 j−l | 0.89 ± 0.04 |
| 4 (3.0–3.5) | 2/2 | 25.2 ± 6.3 a,b,j−l | 25.8 ± 6.6 | 27.9 ± 9.2 a,b,j−l | 24.2 ± 6.6 | 147.3 ± 12.4 a−c,i−l | 146.0 ± 14.5 | 0.93 ± 0/07 j−l | 0.90 ± 0.05 |
| 5 (4.0–4.5) | 3/1 | 23.2 ± 4.7 a,j−l | 26.6 ± 5.6 | 26.7 ± 9.5 a,b,i−l | 25.4 ± 7.0 | 138.4 ± 19.0 i−l | 145.1 ± 16.1 | 0.96 ± 0.07 j−l | 0.90 ± 0.06 |
| 6 (5.0–5.5) | 3/2 | 20.5 ± 4.3 a,h−l | 26.4 ± 5.3 * | 23.4 ± 9.4 a,h−l | 25.0 ± 6.9 | 134.3 ± 16.5 i−l | 148.1 ± 16.2 | 0.94 ± 0.06 j−l | 0.90 ± 0.06 |
| 7 (6.0–6.5) | 4/1 | 21.2 ± 3.4 a,h−l | 27.2 ± 4.7 * | 24.3 ± 9.1 a,b,i−l | 25.8 ± 5.8 | 142.8 ± 13.6 a,b,i−l | 150.0 ± 16.4 | 0.95 ± 0.07 j−l | 0.90 ± 0.04 |
| 8 (7.0–7.5) | 4/2 | 23.4 ± 4.2 a,b,f−l | 27.5 ± 4.9 * | 26.7 ± 9.1 a,b,f,i−l | 26.6 ± 7.0 | 144.8 ± 14.0 a,b,i−l | 150.1 ± 16.7 | 0.90 ± 0.05 j−l | 0.90 ± 0.05 |
| 9 (8.0–8.5) | 5/1 | 30.9 ± 9.1 a,b,f,g | 27.8 ± 4.6 | 38.3 ± 14.2 a−c,e−j | 26.7 ± 6.0 | 167.4 ± 10.5 a−h,j−l | 151.1 ± 16.1 | 0.95 ± 0.08 j−l | 0.91 ± 0.05 |
| 10 (9.0–9.5) | 5/2 | 34.0 ± 6.4 a−h | 27.6 ± 5.1 * | 52.2 ± 12.4 a−i | 26.4 ± 5.6 * | 181.6 ± 8.3 a−i, k,l | 151.3 ± 16.7 * | 1.15 ± 0.07 a−i | 0.90 ± 0.05 * |
| 11 (10–10.5) | 6/1 | 32.0 ± 5.4 a−h | 27.6 ± 5.3 * | 46.2 ± 10.2 a−h | 26.7 ± 5.7 * | 181.5 ± 9.0 a−i | 150.5 ± 17.2 * | 1.12 ± 0.07 a−i | 0.90 ± 0.05 * |
| 12 (11–11.5) | 6/2 | 33.3 ± 6.0 a−h | 26.8 ± 6.2 * | 48.6 ± 11.0 a−h | 25.1 ± 6.5 * | 183.5 ± 7.9 a−i | 150.4 ± 17.3 * | 1.07 ± 0.06 a−i | 0.89 ± 0.05 * |
| Interval (min) | INT EX/Set | % VO2 Peak | %HR Peak | ||
|---|---|---|---|---|---|
| INT | TM | INT | TM | ||
| 1 (0–0.5) | 1/1 | 28.2 | 36.3 | 61.0 | 61.0 |
| 2 (1.0–1.5) | 1/2 | 37.2 | 44.2 | 65.3 | 67.4 |
| 3 (2.0–2.5) | 2/1 | 45.1 | 48.0 | 70.1 | 70.1 |
| 4 (3.0–3.5) | 2/2 | 47.6 | 48.8 | 74.2 | 73.5 |
| 5 (4.0–4.5) | 3/1 | 43.8 | 50.2 | 69.7 | 73.1 |
| 6 (5.0–5.5) | 3/2 | 38.7 | 49.9 | 67.6 | 74.6 |
| 7 (6.0–6.5) | 4/1 | 40.0 | 51.4 | 71.9 | 75.6 |
| 8 (7.0–7.5) | 4/2 | 44.2 | 52.0 | 72.9 | 75.6 |
| 9 (8.0–8.5) | 5/1 | 58.4 | 52.5 | 84.3 | 76.1 |
| 10 (9.0–9.5) | 5/2 | 64.3 | 52.2 | 91.5 | 76.2 |
| 11 (10–10.5) | 6/1 | 60.5 | 52.2 | 91.4 | 75.8 |
| 12 (11–11.5) | 6/2 | 62.9 | 50.7 | 92.4 | 75.8 |
| INT | TM | |
|---|---|---|
| VO2 (mL∙kg−1∙min−1) | 25.4 ± 4.5 | 26.2 ± 4.5 |
| VE (l∙min−1) | 29.79 ± 8.0 | 24.7 ± 5.5 * |
| HR (beats∙min−1) | 153.4 ± 10.6 | 145.2 ± 15.0 * |
| RER | 0.96 ± 0.04 | 0.89 ± 0.05 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faigenbaum, A.D.; Kang, J.; Ratamess, N.A.; Farrell, A.C.; Belfert, M.; Duffy, S.; Jenson, C.; Bush, J. Acute Cardiometabolic Responses to Multi-Modal Integrative Neuromuscular Training in Children. J. Funct. Morphol. Kinesiol. 2019, 4, 39. https://doi.org/10.3390/jfmk4020039
Faigenbaum AD, Kang J, Ratamess NA, Farrell AC, Belfert M, Duffy S, Jenson C, Bush J. Acute Cardiometabolic Responses to Multi-Modal Integrative Neuromuscular Training in Children. Journal of Functional Morphology and Kinesiology. 2019; 4(2):39. https://doi.org/10.3390/jfmk4020039
Chicago/Turabian StyleFaigenbaum, Avery D., Jie Kang, Nicholas A. Ratamess, Anne C. Farrell, Mina Belfert, Sean Duffy, Cara Jenson, and Jill Bush. 2019. "Acute Cardiometabolic Responses to Multi-Modal Integrative Neuromuscular Training in Children" Journal of Functional Morphology and Kinesiology 4, no. 2: 39. https://doi.org/10.3390/jfmk4020039
APA StyleFaigenbaum, A. D., Kang, J., Ratamess, N. A., Farrell, A. C., Belfert, M., Duffy, S., Jenson, C., & Bush, J. (2019). Acute Cardiometabolic Responses to Multi-Modal Integrative Neuromuscular Training in Children. Journal of Functional Morphology and Kinesiology, 4(2), 39. https://doi.org/10.3390/jfmk4020039