
Effects of Electrical Stimulation on Delayed Onset Muscle Soreness (DOMS): Evidences from Laboratory and In-Field Studies

 , ,
, ,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Physiological Parameters, Scales for Physical Fatigue and Recovery Assessments (Study 1 and Study 2)
2.2. Blood Measurements (Study 1 and 2)
2.3. Urine Measurements (Study 2)
2.4. Thermographic Imaging (Study 1)
2.5. Isometric Handgrip Strength Test (Study 1)
2.6. Low-Intensity Electro-Stimulation (ES) (Study 1 and 2)
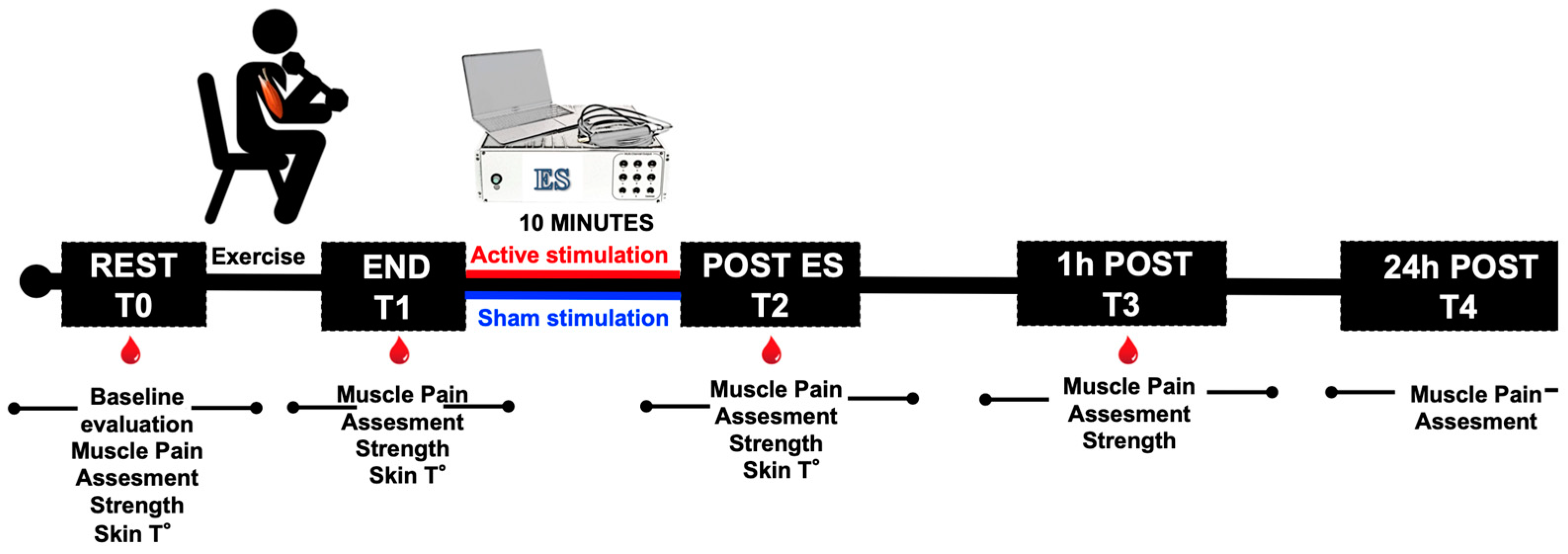
2.7. Laboratory Study—1, Participants and Experimental Protocol
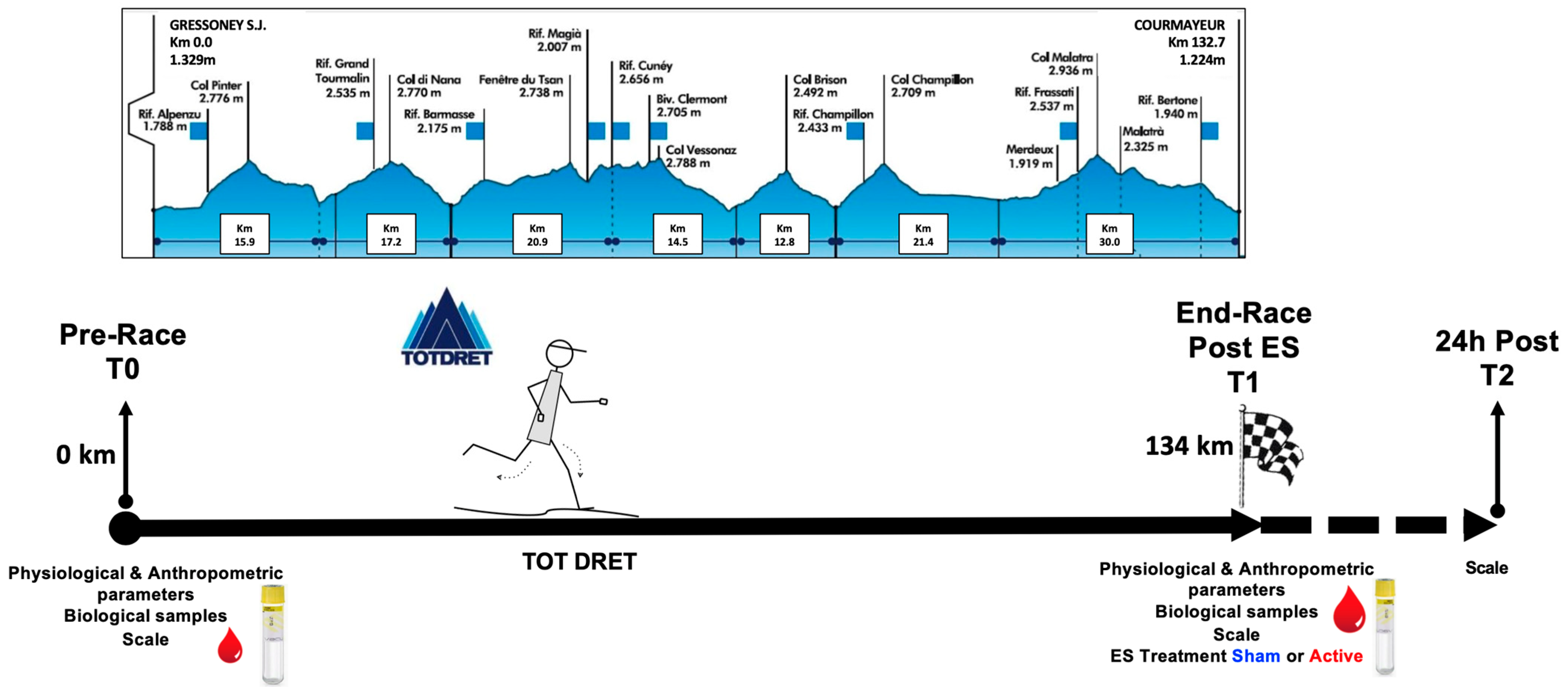
2.8. Field Study—2, Participants and Snapshot of the Race
2.9. Statistical Analysis
3. Results
3.1. Laboratory Experiment—Study 1
3.1.1. Physiological Parameters
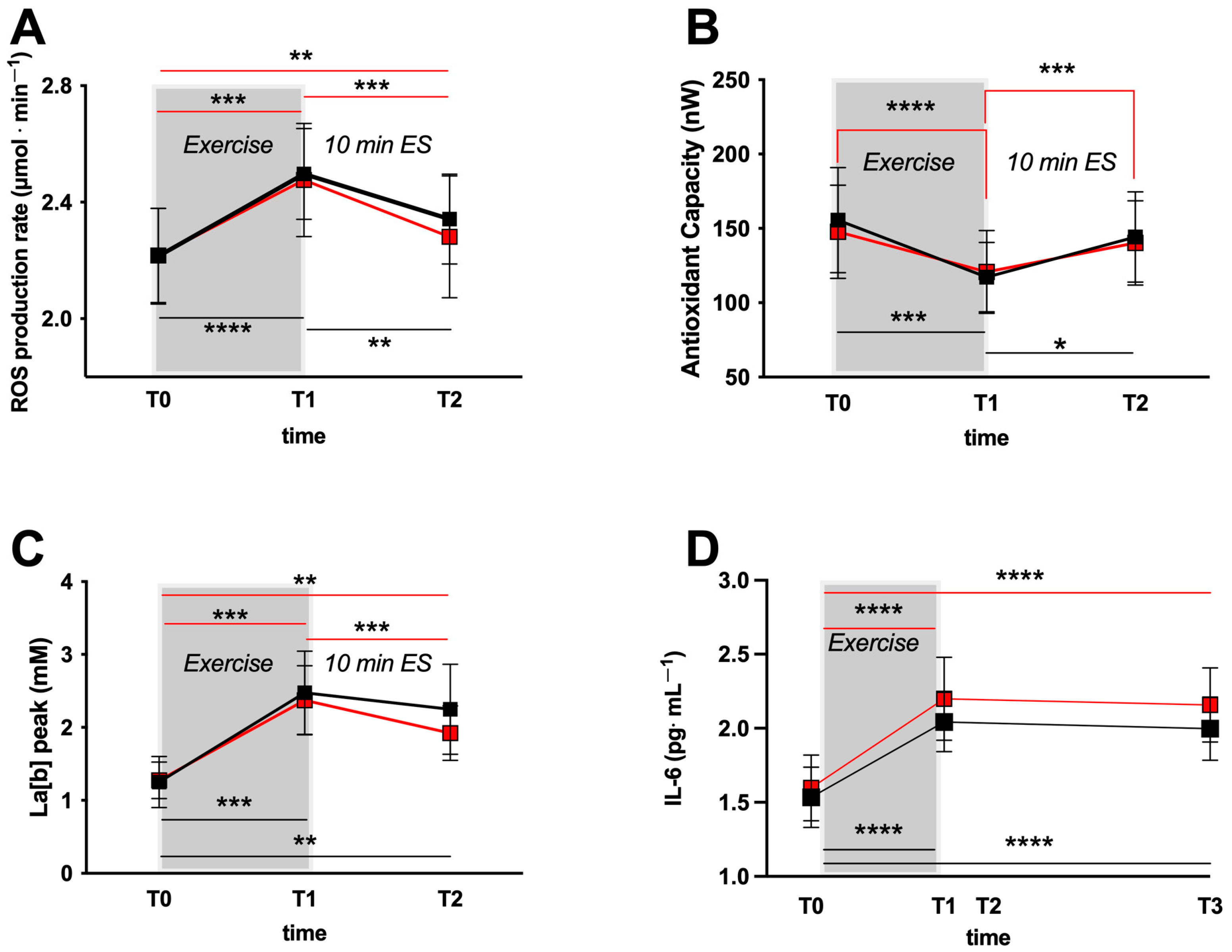
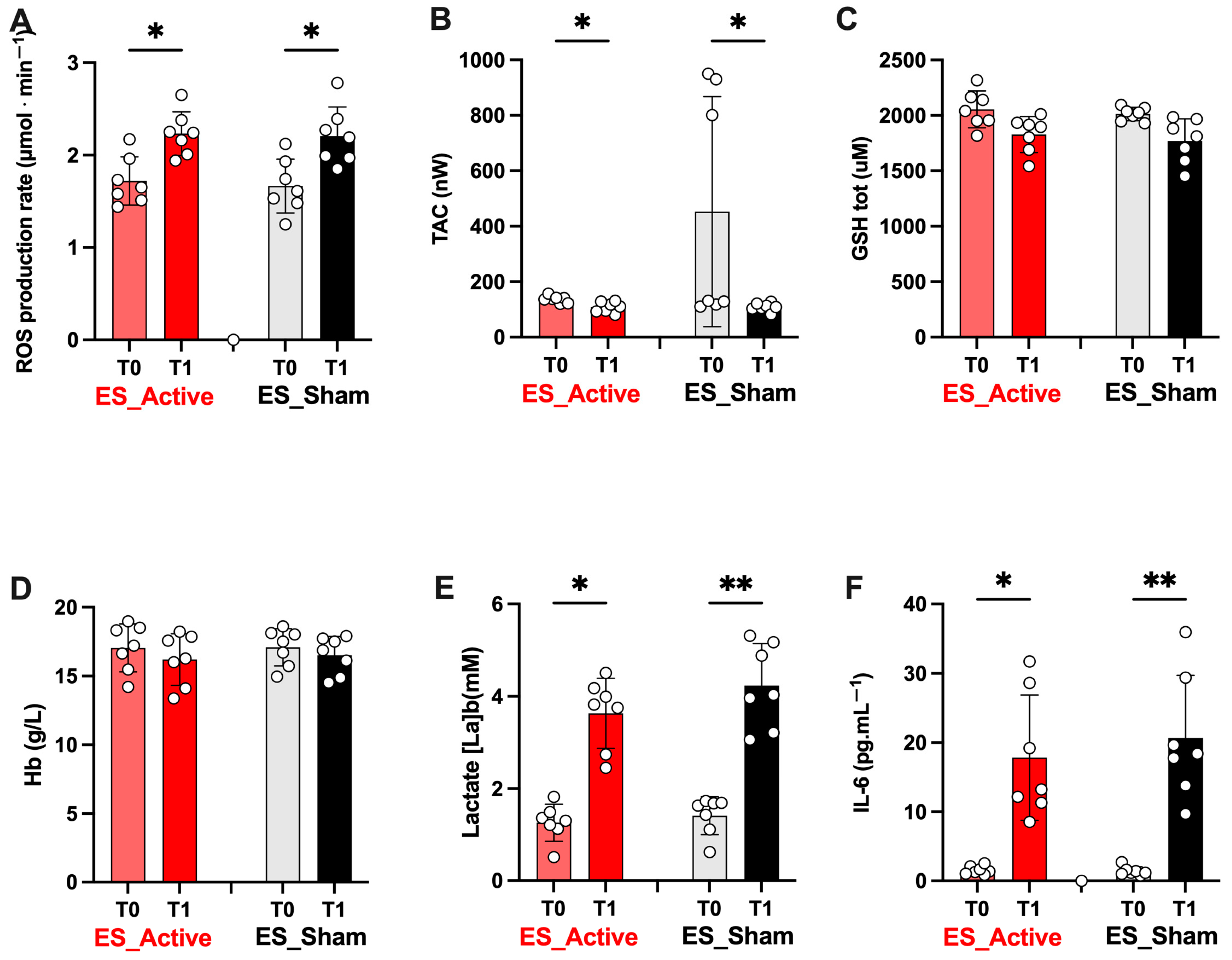
3.1.2. Laboratory Study 1, Biological Parameters (ROS, TAC, Lactate, IL-6)
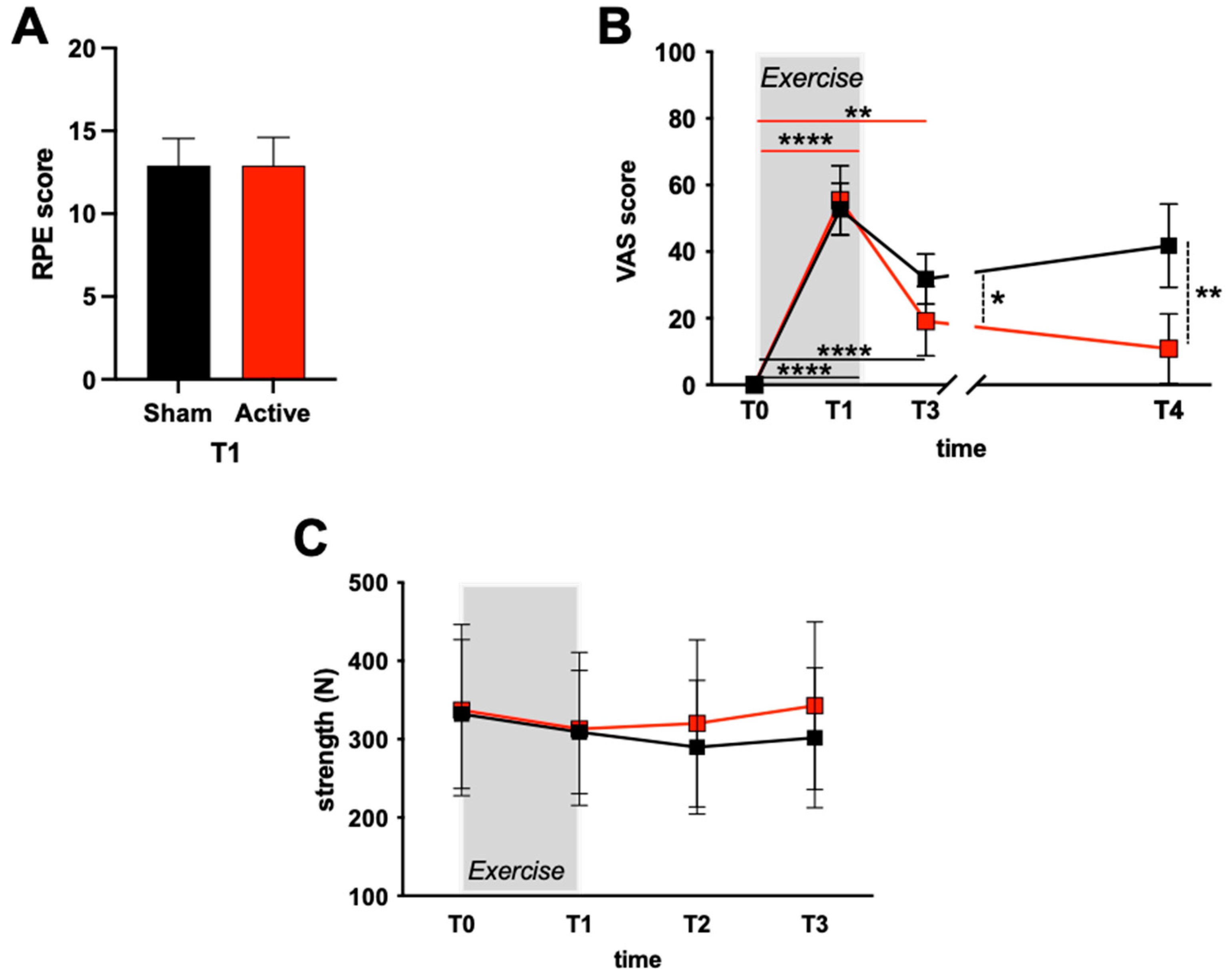
3.1.3. Isometric Handgrip Strength and Scores (RPE, VAS)
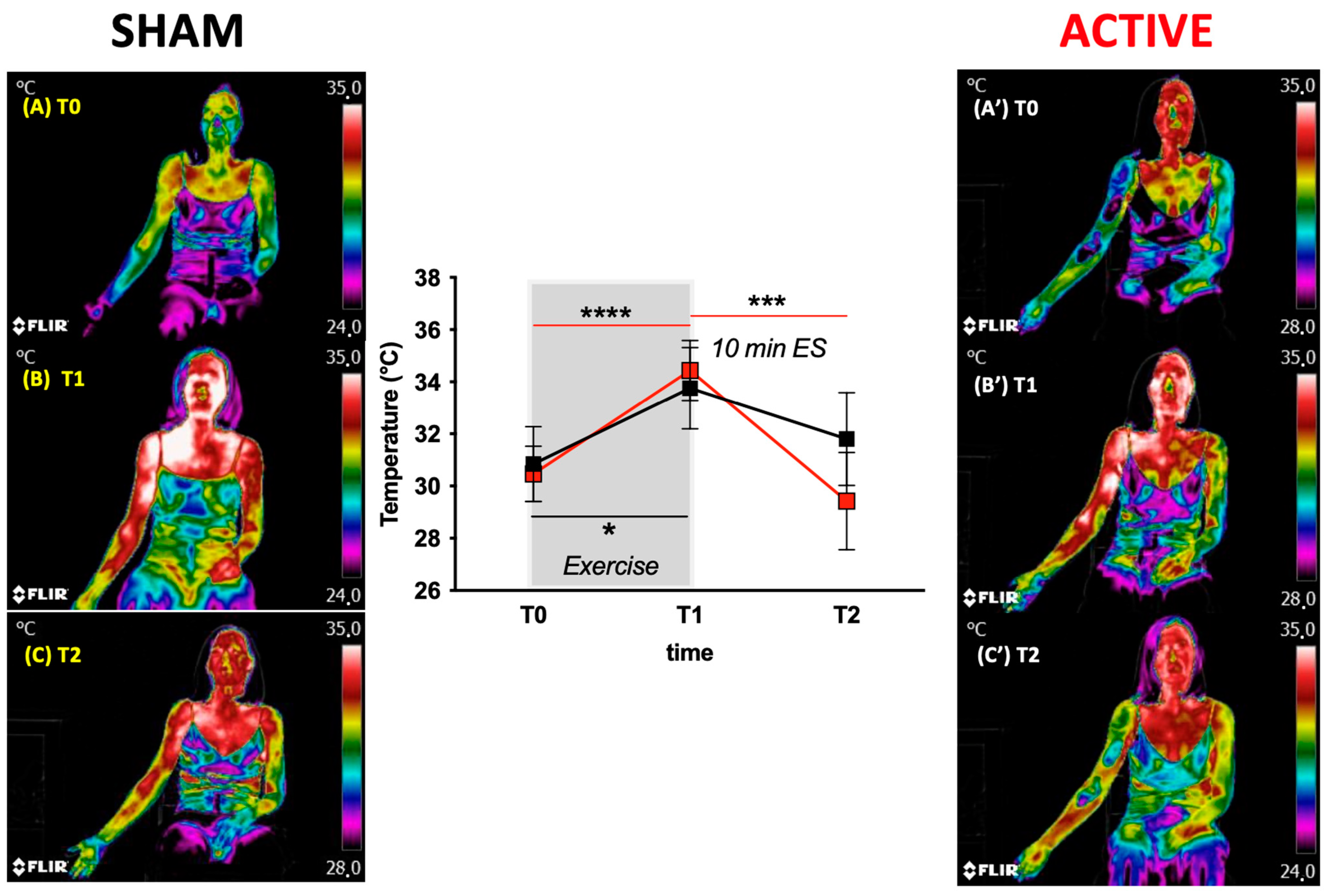
3.1.4. Skin Temperature
3.2. Field Experiment, “Tot Dret”—Study 2
3.2.1. Physiological Parameters
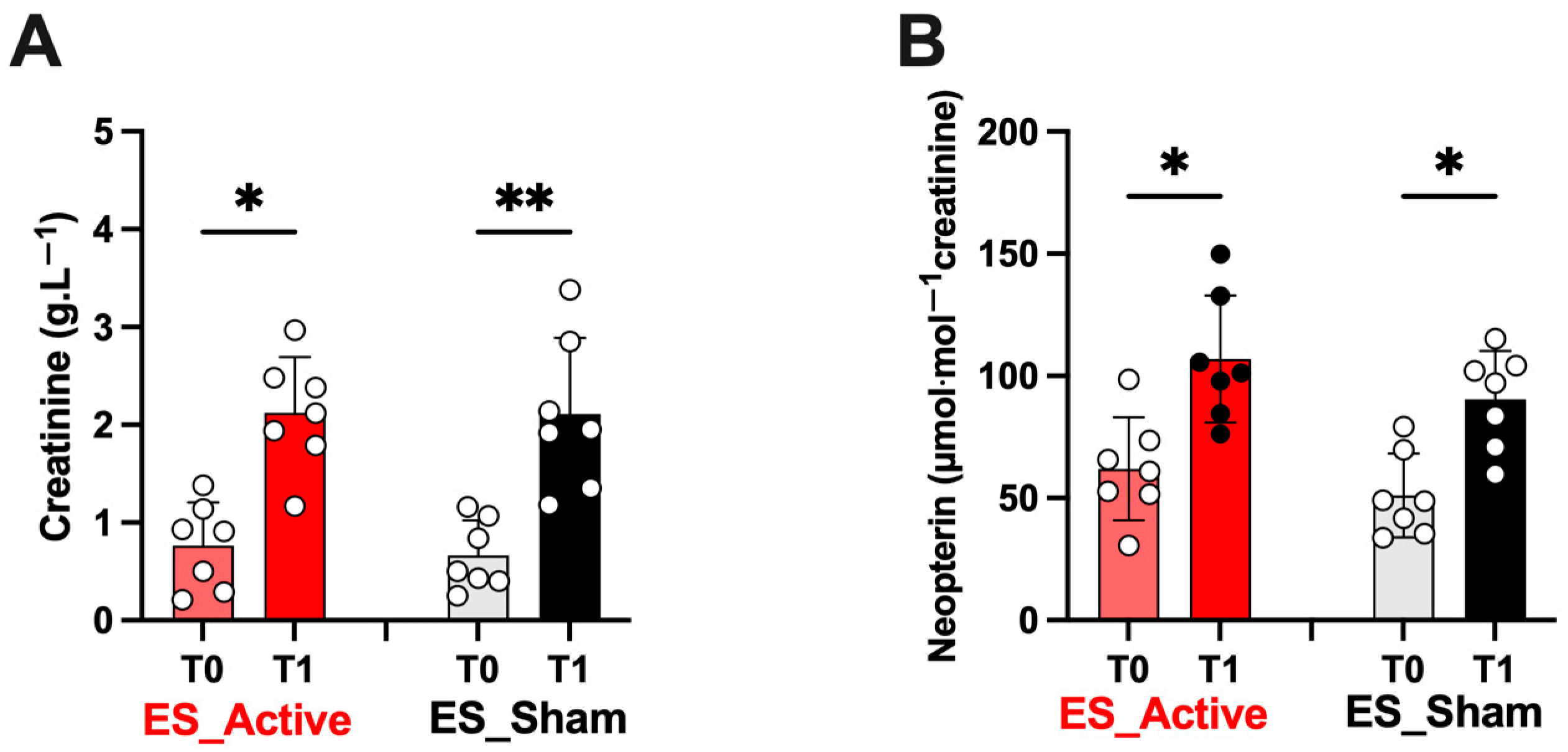
3.2.2. Biological Parameters
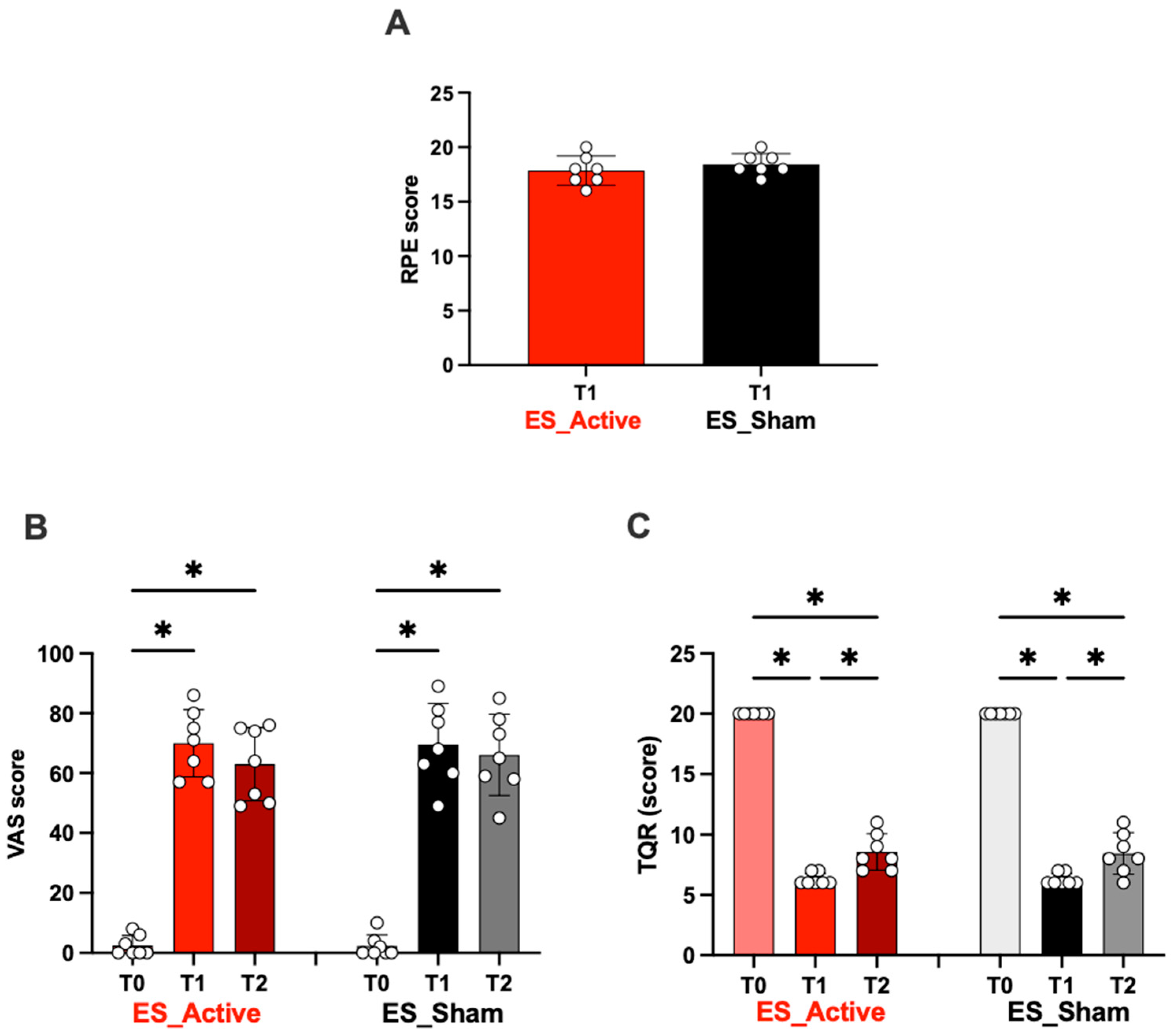
3.2.3. Scores (RPE, VAS, TQR)
4. Discussion
5. Practical Applications and Strengths of the Study
- The biological measurements have been conducted by adopting micro-invasive methods.
- The ES treatments were conducted in two different types of exercise, one involving the upper limbs and the other involving the lower ones.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EPR | Electron Paramagnetic Resonance |
| ES | Electrical Stimulation |
| FM | Fat Mass |
| FFM | Free Fat Mass |
| GSH | Glutathione |
| Hb | Hemoglobin |
| HPLC | High-Pressure Liquid Chromatography |
| IL-6 | Interleukin-6 |
| Lac | Lactate |
| OxS | Oxidative Stress |
| ROS | Reactive Oxygen Species |
| RPE | Rate of Perceived Exertion |
| TAC | Total Antioxidant Capacity |
| TBW | Total Body Water |
| TQR | Total Quality of Recovery |
| VAS | Visual Analog Scale |
References
- Miko, H.-C.; Zillmann, N.; Ring-Dimitriou, S.; Dorner, T.E.; Titze, S.; Bauer, R. Auswirkungen von Bewegung auf die Gesundheit. Gesundheitswesen 2020, 82, S184–S195. [Google Scholar] [CrossRef] [PubMed]
- Paluska, S.A.; Schwenk, T.L. Physical Activity and Mental Health: Current Concepts. Sports Med. 2000, 29, 167–180. [Google Scholar] [CrossRef]
- He, F.; Li, J.; Liu, Z.; Chuang, C.-C.; Yang, W.; Zuo, L. Redox Mechanism of Reactive Oxygen Species in Exercise. Front. Physiol. 2016, 7, 486–495. [Google Scholar] [CrossRef]
- Stožer, A.; Vodopivc, P.; Križančić Bombek, L. Pathophysiology of Exercise-Induced Muscle Damage and Its Structural, Functional, Metabolic, and Clinical Consequences. Physiol. Res. 2020, 69, 565–598. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, P.; Byrnes, W.; McCormick, K.; Turcotte, L.; White, J. Muscle Soreness and Serum Creatine Kinase Activity Following Isometric, Eccentric, and Concentric Exercise. Int. J. Sports Med. 1986, 07, 152–155. [Google Scholar] [CrossRef]
- Cleary, M.A.; Sweeney, L.A.; Kendrick, Z.V.; Sitler, M.R. Dehydration and Symptoms of Delayed-Onset Muscle Soreness in Hyperthermic Males. J. Athl. Train. 2005, 40, 288–297. [Google Scholar] [PubMed]
- Armstrong, R.B.; Warren, G.L.; Warren, J.A. Mechanisms of Exercise-Induced Muscle Fibre Injury. Sports Med. 1991, 12, 184–207. [Google Scholar] [CrossRef]
- Connolly, D.A.J.; Sayers, S.E.; Mchugh, M.P. Treatment and Prevention of Delayed Onset Muscle Soreness. J. Strength Cond. Res. 2003, 17, 197–208. [Google Scholar] [CrossRef]
- Hotfiel, T.; Freiwald, J.; Hoppe, M.; Lutter, C.; Forst, R.; Grim, C.; Bloch, W.; Hüttel, M.; Heiss, R. Advances in Delayed-Onset Muscle Soreness (DOMS): Part I: Pathogenesis and Diagnostics. Sportverletz. Sportschaden 2018, 32, 243–250. [Google Scholar] [CrossRef]
- Lee, J.; Goldfarb, A.H.; Rescino, M.H.; Hegde, S.; Patrick, S.; Apperson, K. Eccentric Exercise Effect on Blood Oxidative-Stress Markers and Delayed Onset of Muscle Soreness. Med. Sci. Sports Exerc. 2002, 34, 443–448. [Google Scholar] [CrossRef]
- Powers, S.K.; Nelson, W.B.; Hudson, M.B. Exercise-Induced Oxidative Stress in Humans: Cause and Consequences. Free. Radic. Biol. Med. 2011, 51, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Radak, Z.; Zhao, Z.; Koltai, E.; Ohno, H.; Atalay, M. Oxygen Consumption and Usage During Physical Exercise: The Balance Between Oxidative Stress and ROS-Dependent Adaptive Signaling. Antioxid. Redox Signal 2013, 18, 1208–1246. [Google Scholar] [CrossRef]
- Smith, L.L. Acute Inflammation: The Underlying Mechanism in Delayed Onset Muscle Soreness? Med. Sci. Sports Exerc. 1991, 23, 542–551. [Google Scholar] [CrossRef]
- MacIntyre, D.L.; Reid, W.D.; McKenzie, D.C. Delayed Muscle Soreness: The Inflammatory Response to Muscle Injury and Its Clinical Implications. Sports Med. 1995, 20, 24–40. [Google Scholar] [CrossRef]
- Toft, A.D.; Jensen, L.B.; Bruunsgaard, H.; Ibfelt, T.; Halkjær-Kristensen, J.; Febbraio, M.; Pedersen, B.K. Cytokine Response to Eccentric Exercise in Young and Elderly Humans. Am. J. Physiol. Cell Physiol. 2002, 283, C289–C295. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.L.; Lowe, D.A.; Armstrong, R.B. Measurement Tools Used in the Study of Eccentric Contraction-Induced Injury. Sports Med. 1999, 27, 43–59. [Google Scholar] [CrossRef] [PubMed]
- Mielgo-Ayuso, J.; Calleja-González, J.; Refoyo, I.; León-Guereño, P.; Cordova, A.; Del Coso, J. Exercise-Induced Muscle Damage and Cardiac Stress During a Marathon Could Be Associated with Dietary Intake During the Week Before the Race. Nutrients 2020, 12, 316. [Google Scholar] [CrossRef]
- Qu, C.; Wu, Z.; Xu, M.; Qin, F.; Dong, Y.; Wang, Z.; Zhao, J. Cryotherapy Models and Timing-Sequence Recovery of Exercise-Induced Muscle Damage in Middle- and Long-Distance Runners. J. Athl. Train. 2020, 55, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Udani, J.K.; Singh, B.B.; Singh, V.J.; Sandoval, E. BounceBackTM Capsules for Reduction of DOMS after Eccentric Exercise: A Randomized, Double-Blind, Placebo-Controlled, Crossover Pilot Study. J. Int. Soc. Sport Nutr. 2009, 6, 14. [Google Scholar] [CrossRef]
- Gulick, D.T.; Kimura, I.F. Delayed Onset Muscle Soreness: What Is It and How Do We Treat It? J. Sport Rehabil. 1996, 5, 234–243. [Google Scholar] [CrossRef]
- Heiss, R.; Lutter, C.; Freiwald, J.; Hoppe, M.; Grim, C.; Poettgen, K.; Forst, R.; Bloch, W.; Hüttel, M.; Hotfiel, T. Advances in Delayed-Onset Muscle Soreness (DOMS)—Part II: Treatment and Prevention. Sportverletz. Sportschaden 2019, 33, 21–29. [Google Scholar] [CrossRef]
- Akinci, B.; Zenginler Yazgan, Y.; Altinoluk, T. The Effectiveness of Three Different Recovery Methods on Blood Lactate, Acute Muscle Performance, and Delayed-Onset Muscle Soreness: A Randomized Comparative Study. J. Sports Med. Phys. Fit. 2020, 60, 345–354. [Google Scholar] [CrossRef]
- Sañudo, B.; Bartolomé, D.; Tejero, S.; Ponce-González, J.G.; Loza, J.P.; Figueroa, A. Impact of Active Recovery and Whole-Body Electromyostimulation on Blood-Flow and Blood Lactate Removal in Healthy People. Front. Physiol. 2020, 11, 310. [Google Scholar] [CrossRef]
- Menzies, P.; Menzies, C.; McIntyre, L.; Paterson, P.; Wilson, J.; Kemi, O.J. Blood Lactate Clearance during Active Recovery after an Intense Running Bout Depends on the Intensity of the Active Recovery. J. Sports Sci. 2010, 28, 975–982. [Google Scholar] [CrossRef]
- Stearns, R.L.; Nolan, J.K.; Huggins, R.A.; Maresh, C.M.; Munõz, C.X.; Pagnotta, K.D.; Volk, B.M.; Casa, D.J. Influence of Cold-Water Immersion on Recovery of Elite Triathletes Following the Ironman World Championship. J. Sci. Med. Sport 2018, 21, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Draper, S.N.; Kullman, E.L.; Sparks, K.E.; Thoman, J. Effects of Intermittent Pneumatic Compression on Delayed Onset Muscle Soreness (DOMS) in Long Distance Runners. Int. J. Exerc. Sci. 2020, 13, 75–86. [Google Scholar] [PubMed]
- Trombold, J.R.; Barnes, J.N.; Critchley, L.; Coyle, E.F. Ellagitannin Consumption Improves Strength Recovery 2-3 d after Eccentric Exercise. Med. Sci. Sports Exerc. 2010, 42, 493–498. [Google Scholar] [CrossRef]
- Sayers, S.P.; Knight, C.A.; Clarkson, P.M.; Van Wegen, E.H.; Kamen, G. Effect of Ketoprofen on Muscle Function and SEMG Activity after Eccentric Exercise. Med. Sci. Sports Exerc. 2001, 33, 702–710. [Google Scholar] [CrossRef]
- Gatterer, H.; Schenk, K.; Wille, M.; Murnig, P.; Burtscher, M. Effect of Massage under Hypoxic Conditions on Exercise-Induced Muscle Damage and Physical Strain Indices in Professional Soccer Players. Biol. Sport 2013, 30, 81–83. [Google Scholar] [CrossRef]
- Martin, V.; Millet, G.Y.; Lattier, G.; Perrod, L. Effects of Recovery Modes after Knee Extensor Muscles Eccentric Contractions. Med. Sci. Sports Exerc. 2004, 36, 1907–1915. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Kim, M.C. The Affect on Delayed Onset Muscle Soreness Recovery for Ultrasound with Bee Venom. J. Phys. Ther. Sci. 2014, 26, 1419–1421. [Google Scholar] [CrossRef] [PubMed]
- Hausswirth, C.; Louis, J.; Bieuzen, F.; Pournot, H.; Fournier, J.; Filliard, J.-R.; Brisswalter, J. Effects of Whole-Body Cryotherapy vs. Far-Infrared vs. Passive Modalities on Recovery from Exercise-Induced Muscle Damage in Highly-Trained Runners. PLoS ONE 2011, 6, e27749. [Google Scholar] [CrossRef]
- Burgess, L.; Immins, T.; Swain, I.; Wainwright, T. Effectiveness of Neuromuscular Electrical Stimulation for Reducing Oedema: A Systematic Review. J. Rehabil. Med. 2019, 51, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Finger, S.; Piccolino, M. The Shocking History of Electric Fishes: From Ancient Epochs to the Birth of Modern Neurophysiology; Oxford Academic Press: Oxford, UK, 2011. [Google Scholar] [CrossRef]
- Nielsen, A.; Dusek, J.A.; Taylor-Swanson, L.; Tickm, H. Acupuncture Therapy as an Evidence-Based Nonpharmacologic Strategy for Comprehensive Acute Pain Care: The Academic Consortium Pain Task Force White Paper Update. Pain Med. 2022, 23, 1582–1612. [Google Scholar] [CrossRef]
- William Gibson, W.; Wand, B.M.; Meads, C.; Catley, M.J.; O’Connell, N.E.; Pain, C. Palliative and Supportive Care Group. Transcutaneous electrical nerve stimulation (TENS) for chronic pain—An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 2019, CD011890. [Google Scholar] [CrossRef]
- Paley, C.A.; Wittkopf, P.G.; Jones, G.; Johnson, M.I. Does TENS Reduce the Intensity of Acute and Chronic Pain? A Comprehensive Appraisal of the Characteristics and Out-comes of 169 Reviews and 49 Meta-Analyses. Medicina 2021, 57, 1060. [Google Scholar] [CrossRef]
- Kim, D.-H.; Ryu, Y.; Hahm, D.H.; Sohn, B.Y.; Shim, I.; Kwon, O.S.; Chang, S.; Gwak, Y.S.; Kim, S.; Kim, J.H.; et al. Acupuncture points can be identified as cutaneous neurogenic in-flammatory spots. Sci. Rep. 2017, 7, 15214. [Google Scholar] [CrossRef]
- Babault, N.; Cometti, C.; Maffiuletti, N.A.; Deley, G. Does Electrical Stimulation Enhance Post-Exercise Performance Recovery? Eur. J. Appl. Physiol. 2011, 111, 2501–2507. [Google Scholar] [CrossRef]
- Menezes, M.A.; Menezes, D.A.; Vasconcelos, L.L.; DeSantana, J.M. Is Electrical Stimulation Effective in Preventing or Treating Delayed-Onset Muscle Soreness (DOMS) in Athletes and Untrained Adults? A Systematic Review With Meta-Analysis. J. Pain 2022, 23, 2013–2035. [Google Scholar] [CrossRef]
- Martínez-Gómez, R.; Valenzuela, P.L.; Lucia, A.; Barranco-Gil, D. Comparison of Different Recovery Strategies After High-Intensity Functional Training: A Crossover Randomized Controlled Trial. Front. Physiol. 2022, 13, 819588. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Jones, K.D. Adult Measures of Pain: The McGill Pain Questionnaire (MPQ), Rheumatoid Arthritis Pain Scale (RAPS), Short-Form McGill Pain Questionnaire (SF-MPQ), Verbal Descriptive Scale (VDS), Visual Analog Scale (VAS), and West Haven-Yale Multidisciplinary Pain Inventory (WHYMPI). Arthritis Rheum. Arthr. 2003, 49, S96–S104. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63, S240–S252. [Google Scholar] [CrossRef]
- Brizzolari, A.; Bosco, G.; Vezzoli, A.; Dellanoce, C.; Barassi, A.; Paganini, M.; Cialoni, D.; Mrakic-Sposta, S. Seasonal Oxy-Inflammation and Hydration Status in Non-Elite Freeskiing Racer: A Pilot Study by Non-Invasive Analytic Method. Int. J. Environ. Res. Public Health 2023, 20, 3157. [Google Scholar] [CrossRef] [PubMed]
- Mrakic-Sposta, S.; Vezzoli, A.; Maderna, L.; Gregorini, F.; Montorsi, M.; Moretti, S.; Greco, F.; Cova, E.; Gussoni, M. R(+)-Thioctic Acid Effects on Oxidative Stress and Peripheral Neuropathy in Type II Diabetic Patients: Preliminary Results by Electron Paramagnetic Resonance and Electroneurography. Oxid. Med. Cell. Longev. 2018, 2018, 1767265. [Google Scholar] [CrossRef]
- Kenttä, G.; Hassmén, P. Overtraining and Recovery: A Conceptual Model. Sports Med. 1998, 26, 1–16. [Google Scholar] [CrossRef]
- Mrakic-Sposta, S.; Gussoni, M.; Montorsi, M.; Porcelli, S.; Vezzoli, A. Assessment of a Standardized ROS Production Profile in Humans by Electron Paramagnetic Resonance. Oxid. Med. Cell. Longev. 2012, 2012, 973927. [Google Scholar] [CrossRef]
- Mrakic-Sposta, S.; Gussoni, M.; Montorsi, M.; Porcelli, S.; Vezzoli, A. A Quantitative Method to Monitor Reactive Oxygen Species Production by Electron Paramagnetic Resonance in Physiological and Pathological Conditions. Oxid. Med. Cell. Longev. 2014, 2014, e306179. [Google Scholar] [CrossRef] [PubMed]
- Mrakic-Sposta, S.; Gussoni, M.; Porcelli, S.; Pugliese, L.; Pavei, G.; Bellistri, G.; Montorsi, M.; Tacchini, P.; Vezzoli, A. Training Effects on ROS Production Determined by Electron Paramagnetic Resonance in Master Swimmers. Oxid. Med. Cell. Longev. 2015, 2015, 804794. [Google Scholar] [CrossRef]
- Mrakic-Sposta, S.; Gussoni, M.; Moretti, S.; Pratali, L.; Giardini, G.; Tacchini, P.; Dellanoce, C.; Tonacci, A.; Mastorci, F.; Borghini, A.; et al. Effects of Mountain Ultra-Marathon Running on ROS Production and Oxidative Damage by Micro-Invasive Analytic Techniques. PLoS ONE 2015, 10, e0141780. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Roussel, C.; Lagger, G.; Tacchini, P.; Girault, H.H. Antioxidant Sensors Based on DNA-Modified Electrodes. Anal. Chem. 2005, 77, 7687–7694. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Su, B.; Lagger, G.; Tacchini, P.; Girault, H.H. Antioxidant Redox Sensors Based on DNA Modified Carbon Screen-Printed Electrodes. Anal. Chem. 2006, 78, 6879–6884. [Google Scholar] [CrossRef] [PubMed]
- Giacon, T.A.; Bosco, G.; Vezzoli, A.; Dellanoce, C.; Cialoni, D.; Paganini, M.; Mrakic-Sposta, S. Oxidative Stress and Motion Sickness in One Crew during Competitive Offshore Sailing. Sci. Rep. 2022, 12, 1142. [Google Scholar] [CrossRef] [PubMed]
- Mrakic-Sposta, S.; Vezzoli, A.; D’Alessandro, F.; Paganini, M.; Dellanoce, C.; Cialoni, D.; Bosco, G. Change in Oxidative Stress Biomarkers During 30 Days in Saturation Dive: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 7118. [Google Scholar] [CrossRef] [PubMed]
- Bosco, G.; Giacon, T.A.; Paolocci, N.; Vezzoli, A.; Noce, C.D.; Paganini, M.; Agrimi, J.; Garetto, G.; Cialoni, D.; D’Alessandro, N.; et al. Dopamine/BDNF Loss Underscores Narcosis Cognitive Impairment in Divers: A Proof of Concept in a Dry Condition. Eur. J. Appl. Physiol. 2023, 123, 143–158. [Google Scholar] [CrossRef]
- Borges, R.C.; Carvalho, C.R.F.; Colombo, A.S.; Da Silva Borges, M.P.; Soriano, F.G. Physical Activity, Muscle Strength, and Exercise Capacity 3 Months after Severe Sepsis and Septic Shock. Intens. Care Med. 2015, 41, 1433–1444. [Google Scholar] [CrossRef] [PubMed]
- Serinken, M.A.; Gencoglu, C.; Kayatekin, B.M. The Effect of Eccentric Exercise-Induced Delayed-Onset Muscle Soreness on Positioning Sense and Shooting Percentage in Wheelchair Basketball Players. Balk. Med. J. 2013, 30, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Friesenbichler, B.; Stirling, L.M.; Federolf, P.; Nigg, B.M. Tissue Vibration in Prolonged Running. J. Biomech. 2011, 44, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Ispirlidis, I.; Fatouros, I.G.; Jamurtas, A.Z.; Nikolaidis, M.G.; Michailidis, I.; Douroudos, I.; Margonis, K.; Chatzinikolaou, A.; Kalistratos, E.; Katrabasas, I.; et al. Time-Course of Changes in Inflammatory and Performance Responses Following a Soccer Game. Clin. J. Sport Med. 2008, 18, 423–431. [Google Scholar] [CrossRef]
- Brown, S.J.; Child, R.B.; Day, S.H.; Donnelly, A.E. Exercise-Induced Skeletal Muscle Damage and Adaptation Following Repeated Bouts of Eccentric Muscle Contractions. J. Sports Sci. 1997, 15, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Mackey, A.L.; Bojsen-Moller, J.; Qvortrup, K.; Langberg, H.; Suetta, C.; Kalliokoski, K.K.; Kjaer, M.; Magnusson, S.P. Evidence of Skeletal Muscle Damage Following Electrically Stimulated Isometric Muscle Contractions in Humans. J. Appl. Physiol. 2008, 105, 1620–1627. [Google Scholar] [CrossRef]
- Twist, C.; Eston, R.G. The Effect of Exercise-Induced Muscle Damage on Perceived Exertion and Cycling Endurance Performance. Eur. J. Appl. Physiol. 2009, 105, 559–567. [Google Scholar] [CrossRef]
- Burt, D.G.; Twist, C. The Effects of Exercise-Induced Muscle Damage on Cycling Time-Trial Performance. J. Strength Cond. Res. 2011, 25, 2185–2192. [Google Scholar] [CrossRef]
- Lewis, P.B.; Ruby, D.; Bush-Joseph, C.A. Muscle soreness and delayed-onset muscle soreness. Clin. Sports Med. 2012, 31, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.; Hume, P.A.; Maxwell, L. Delayed Onset Muscle Soreness: Treatment Strategies and Performance Factors. Sports Med. 2003, 33, 145–164. [Google Scholar] [CrossRef]
- Barnett, A. Using Recovery Modalities between Training Sessions in Elite Athletes: Does It Help? Sports Med. 2006, 36, 781–796. [Google Scholar] [CrossRef]
- Vezzoli, A.; Dellanoce, C.; Mrakic-Sposta, S.; Montorsi, M.; Moretti, S.; Tonini, A.; Pratali, L.; Accinni, R. Oxidative Stress Assessment in Response to Ultraendurance Exercise: Thiols Redox Status and ROS Production According to Duration of a Competitive Race. Oxid. Med. Cell. Longev. 2016, 2016, 6439037. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, O.; Douzi, W.; Theurot, D.; Bosquet, L.; Dugué, B. An Evidence-Based Approach for Choosing Post-Exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation: A Systematic Review With Meta-Analysis. Front. Physiol. 2018, 9, 403. [Google Scholar] [CrossRef]
- Schenk, R.; Rauch, S.; Procter, E.; Grasegger, K.; Mrakic-Sposta, S.; Gattener, H. Changes in Factors Regulating Serum Sodium Homeostasis During Two Ultra-Endurance Mountain Races of Different Distances: 69 km vs. 121 km. Front. Physiol. 2021, 12, 764694. [Google Scholar] [CrossRef] [PubMed]
- Cheng, N.; Van Hoof, H.; Bockx, E.; Hoogmartens, M.J.; Mulier, J.C.; De Dijcker, F.J.; Sansen, W.M.; De Loecker, W. The Effects of Electric Currents on ATP Generation, Protein Synthesis, and Membrane Transport in Rat Skin. Clin. Orthop. Relat. Res. 1982, 171, 264. [Google Scholar] [CrossRef]
- Finniss, D.G. Placebo Effects: Historical and Modern Evaluation. In International Review of Neurobiology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 139, pp. 1–27. ISBN 978-0-12-815416-8. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physiological Parameters | |
|---|---|
| Age (years) | 56.07 ± 4.87 |
| Height (m) | 1.71 ± 0.09 |
| Gender | 6 Females/7 Males |
| Body Mass (kg) | 73.98 ± 15.54 |
| BMI (kg∗m−2) | 25.22 ± 4.11 |
| Fat Mass (kg) | 19.77 ± 7.10 |
| Free Fat Mass (kg) | 54.21 ± 12.86 |
| TBW (kg) | 37.62 ± 9.13 |
| Sham Stimulation | Active Stimulation | |||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| SaO2 (%) | 97.5 ± 0.7 | 96.8 ± 1.1 | 97.4 ± 1.0 | 97.4 ± 0.8 | 96.3 ± 1.4 | 97.2 ± 0.9 |
| HR (bpm) | 71.3 ± 8.1 | 85.7 ± 20.7 | 76.4 ± 10.9 | 71.00 ± 7.7 | 86.9 ± 19.7 | 77.0 ± 9.4 |
| Levene’s Test—EXP Lab (1) Active vs. Sham Stimulation | Effect Size- EXP Lab (1) | |||
|---|---|---|---|---|
| T0 | T1 | T2 | ||
| ROS | F = 0.02929 p-value = 0.8649 | F = 0.28806 p-value = 0.5943 | F = 0.37283 p-value = 0.5447 | η2 = 0.36 |
| IL-6 | F = 2.10077 p-value = 0.1546 | F = 0.49079 p-value = 0.4907 | F = 0.20208 p-value = 0.2020 | η2 = 0.68 |
| TAC | F = 0.00375 p-value = 0.9518 | F = 0.2018 p-value = 0.6581 | F = 0.04002 p-value = 0.8434 | η2 = 0.19 |
| Lactate | F = 0.40928 p-value = 0.5258 | F = 1.07138 p-value = 0.3065 | F = 0.82274 p-value = 0.3695 | η2 = 0.56 |
| T° | F = 0.63232 p-value = 0.4313 | F = 2.7096 p-value = 0.1079 | F = 4.24296 p-value = 0.4596 | η2 = 0.53 |
| Athletes’ Groups Tot Dret | |||||||
|---|---|---|---|---|---|---|---|
| ALL Athletes at (n = 25) | Finisher Athletes (n = 14) | ES—Active Group (n = 7) | ES—Sham Group (n = 7) | ||||
| Pre-Race T0 | Pre-Race T0 | Post-Race T1 | Pre-Race T0 | Post-Race T1 | Pre-Race T0 | Post-Race T1 | |
| Age (years) | 47.4 ± 10.2 | 48.0 ± 10.7 | - | 47.0 ± 12.1 | - | 49.0 ± 10.0 | - |
| Body Mass (kg) | 70.6 ± 10.1 | 70.0 ± 10.4 | 67.1 ± 9.5 *** | 70.7 ± 8.7 | 68.7 ± 8.7 * | 69.3 ± 12.5 | 65.5 ± 10.63 * |
| BMI(kg·m−2) | 23.0 ± 2.5 | 22.5 ± 2.4 | 22.0 ± 2.4 *** | 23.0 ± 2.2 | 22.3 ± 2.4 * | 22.0 ± 2.6 | 21.6 ± 2.5 * |
| FM (kg) | 7.9 ± 4.0 | 7.4 ± 4.3 | 4.9 ± 2.2 *** | 7.8 ± 4.0 | 6.1 ± 2.5 * | 8.7 ± 4.7 | 4.7 ± 2.2 * |
| FFM (kg) | 63.6 ± 8.5 | 62.7 ± 8.7 | 60.7 ± 8.3 ** | 64.7 ± 6.3 | 62.3 ± 6.1 * | 60.7 ± 10.7 | 58.4 ± 9.9 * |
| TBW (kg) | 41.5 ± 5.6 | 41.6 ± 5.3 | 40.6 ± 5.0 * | 41.9 ± 3.7 | 41.3 ± 6.9 | 41.3 ± 4.0 | 39.9 ± 6.1 |
| SaO2 (%) | 97.5 ± 1.0 | 97.7 ± 0.8 | 96.1 ± 0.6 *** | 97.6 ± 0.9 | 96.0 ± 0.8 * | 97.8 ± 1.0 | 96.2 ± 0.5 * |
| HR (bpm) | 63.5 ± 11.2 | 59.1 ± 7.9 | 84.8 ± 7.9 *** | 58.7 ± 8.2 | 82.4 ± 6.9 * | 59.5 ± 8.4 | 87.1 ± 7.5 * |
| SBP (mmHg) | 128.6 ± 14.7 | 125.9 ± 17.5 | 141.9 ± 14.3 *** | 125.0 ± 7.6 | 141.7 ± 10.8 * | 126.7 ± 24.49 | 142.0 ± 18.1 * |
| DBP (mmHg) | 76.1 ± 9.5 | 73.6 ± 8.8 | 82.6 ± 5.7 *** | 75.7 ± 8.8 | 84.9 ± 5.8 * | 71.6 ± 9.0 | 88.6 ± 5.3 * |
| Race completion time (h) | 32.15 ± 5.18 | - | 35.45 ± 4.98 | - | 35.31 ± 5.57 | 35.59 ± 4.75 | |
| Levene’s Test—EXP in Field (B) Active vs. Sham Stimulation | Size Effect—EXP in Field (B) | ||
|---|---|---|---|
| REST—T0 | END—T1 | ||
| ROS | F = 0.16619 p-value = 0.6868 | F = 3.25446 p-value = 0.0828 | η2 = 0.50 |
| IL-6 | F = 0.01206 p-value = 0.9133 | F = 1.36679 p-value = 0.2529 | η2 = 0.73 |
| TAC | F = 1.17291 p-value = 0.3000 | F = 1.33197 p-value = 0.2709 | η2= 0.48 |
| GSH | F = 0.48966 p-value = 0.4902 | F = 0.20224 p-value = 0.6566 | η2 =0.41 |
| Lactate | F = 4.06207 p-value = 0.0543 | F = 2.31256 p-value = 0.1404 | η2 = 0.74 |
| Hb | F = 0.19891 p-value = 0.6592 | F = 6.42359 p-value = 0.0176 | η2 = 0.06 |
| Creatinine | F = 1.09116 p-value = 0.3058 | F = 0.02641 p-value = 0.8721 | η2 = 0.67 |
| Neopterin | F = 1.29507 p-value = 0.2659 | F = 0.99735 p-value = 0.3275 | η2 = 0.53 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gussoni, M.; Moretti, S.; Vezzoli, A.; Genitoni, V.; Giardini, G.; Balestra, C.; Bosco, G.; Pratali, L.; Spagnolo, E.; Montorsi, M.; et al. Effects of Electrical Stimulation on Delayed Onset Muscle Soreness (DOMS): Evidences from Laboratory and In-Field Studies. J. Funct. Morphol. Kinesiol. 2023, 8, 146. https://doi.org/10.3390/jfmk8040146
Gussoni M, Moretti S, Vezzoli A, Genitoni V, Giardini G, Balestra C, Bosco G, Pratali L, Spagnolo E, Montorsi M, et al. Effects of Electrical Stimulation on Delayed Onset Muscle Soreness (DOMS): Evidences from Laboratory and In-Field Studies. Journal of Functional Morphology and Kinesiology. 2023; 8(4):146. https://doi.org/10.3390/jfmk8040146
Chicago/Turabian StyleGussoni, Maristella, Sarah Moretti, Alessandra Vezzoli, Valerio Genitoni, Guido Giardini, Costantino Balestra, Gerardo Bosco, Lorenza Pratali, Elisabetta Spagnolo, Michela Montorsi, and et al. 2023. "Effects of Electrical Stimulation on Delayed Onset Muscle Soreness (DOMS): Evidences from Laboratory and In-Field Studies" Journal of Functional Morphology and Kinesiology 8, no. 4: 146. https://doi.org/10.3390/jfmk8040146
APA StyleGussoni, M., Moretti, S., Vezzoli, A., Genitoni, V., Giardini, G., Balestra, C., Bosco, G., Pratali, L., Spagnolo, E., Montorsi, M., & Mrakic-Sposta, S. (2023). Effects of Electrical Stimulation on Delayed Onset Muscle Soreness (DOMS): Evidences from Laboratory and In-Field Studies. Journal of Functional Morphology and Kinesiology, 8(4), 146. https://doi.org/10.3390/jfmk8040146