
Smart Monitoring Pad for Prediction of Pressure Ulcers with an Automatically Activated Integrated Electro-Therapy System


Abstract
:1. Introduction
2. Materials and Methods
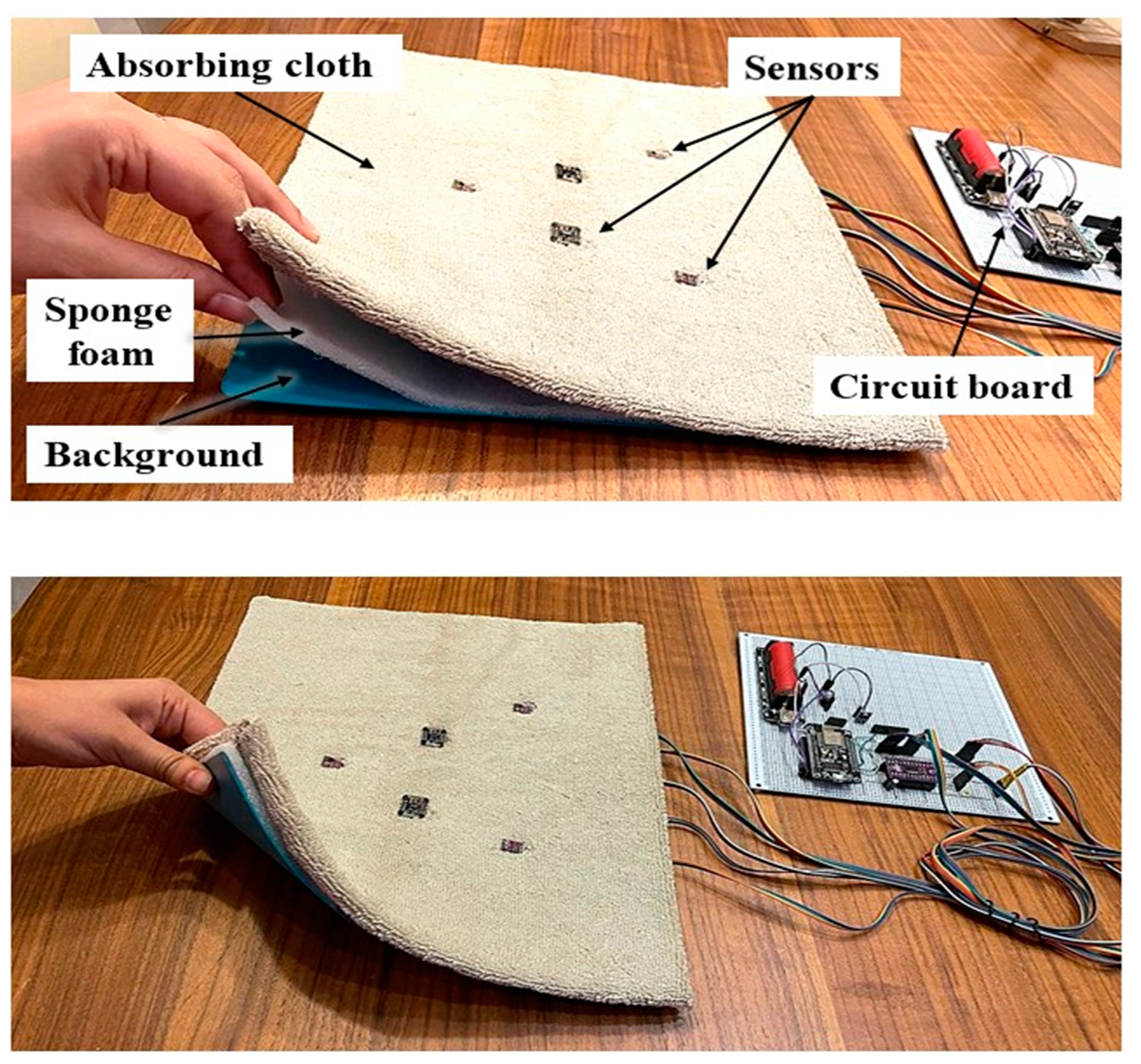
2.1. Hardware Design
2.2. Software
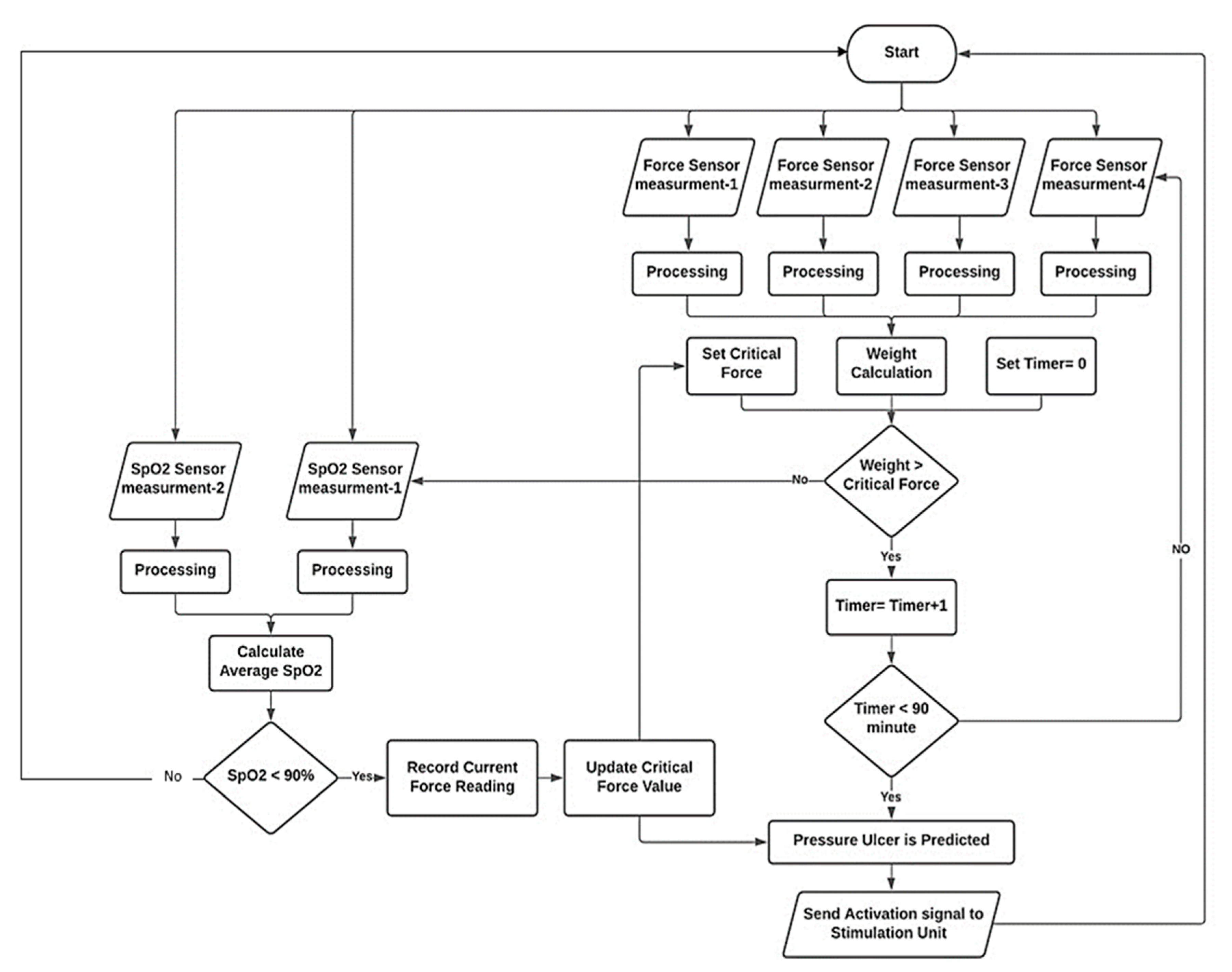
- Decision-making of PU prediction is a multi-step algorithm built based on the physiological process that leads to PU formation. The main indicator of PU is saturation of oxygen in blood (SpO2); oxygen drops due to the force applied on the area causing the collapse of blood vessels, this force is basically a portion of the subject’s weight applied to the sacral region; many researchers assumed different levels of critical force that leads to PU formation [28]. These values are set as “initial critical force”, and this value is continuously updated based on SpO2 levels. As the subject lay down in supine position (bedridden posture), both force and SpO2 levels are measured simultaneously, and the value of force that will cause oxygen levels to drop is detected and recorded which is a specific value for that certain subject. This value is set as the “updated critical force”; if force exceeds this threshold, the microcontroller checks oxygen level; if it is not affected, then no prediction occurs, but if the critical force persists at high level for more than a critical time (90 min based on previous research [7,8,9,10,11,12,13,14,15,16,17,18,19,20]), then the prediction is true. The SpO2 is monitored continuously, and if oxygen concentration falls below a critical range (90–89%) PU prediction is set to true immediately. When PU prediction is true, the system automatically activates the ES unit to begin the electrotherapy session; the stimulation increases blood flow and increases SpO2 level, and it also causes muscle movement (contraction), making the area more resistant to PU. Figure 5 shows a simplified flowchart of the prediction algorithm.
- Prediction of bacterial infection is based on monitoring and preventing the growth of skin bacteria known as Staphylococcus aureus [29]. It is one of the most common bacteria that grows alongside PU scars [30,31]. The system aims to prevent the favorable growth environment of this bacteria. The two main factors in bacterial growth in the skin are temperature and humidity, hence the system continuously monitors these two factors using the (SHT30) Humidity/Temperature sensor at three different locations on the subject’s back to cover the sacral area. Next, the system runs calculations comparing the sensor’s readings against preset thresholds to estimate the risk of developing the infection. Once the risk is detected, an alarm message is sent to the user interface alerting the healthcare givers to take preventive measures, for example, “use cloth to remove sweating and adjust skin temperature”. The threshold for temperature is (>35 °C) and (<39–40 °C), relative humidity between (70–80%). These conditions mark the favorable environment for developing infection in ulcerated skin if they occur together [32]. In this case, time is not accounted for, so when predicted, the healthcare giver is instructed to adjust relative humidity/temperature immediately by drying the skin or ventilating the area, for example. In the case of temperatures dropping below 20 °C, an alarm message will be sent, because it has been shown that lower temperatures leads to low blood flow, which encourages PU formation. Additionally, if temperature is above 38 °C, an alarm indicating that the subject has developed a fever will be shown on the user interface screen. Figure 6 shows a simplified algorithm for bacterial infection prediction.
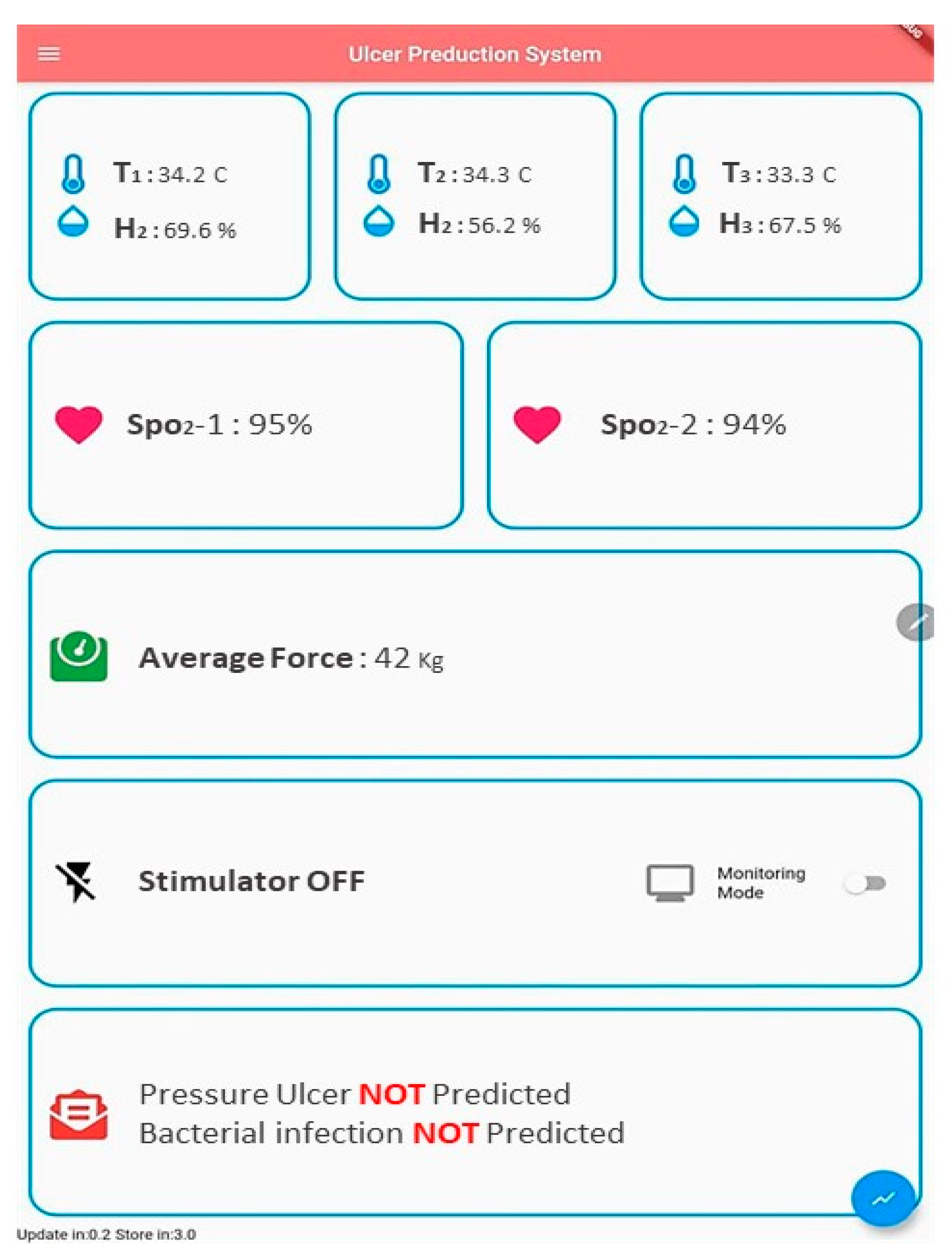
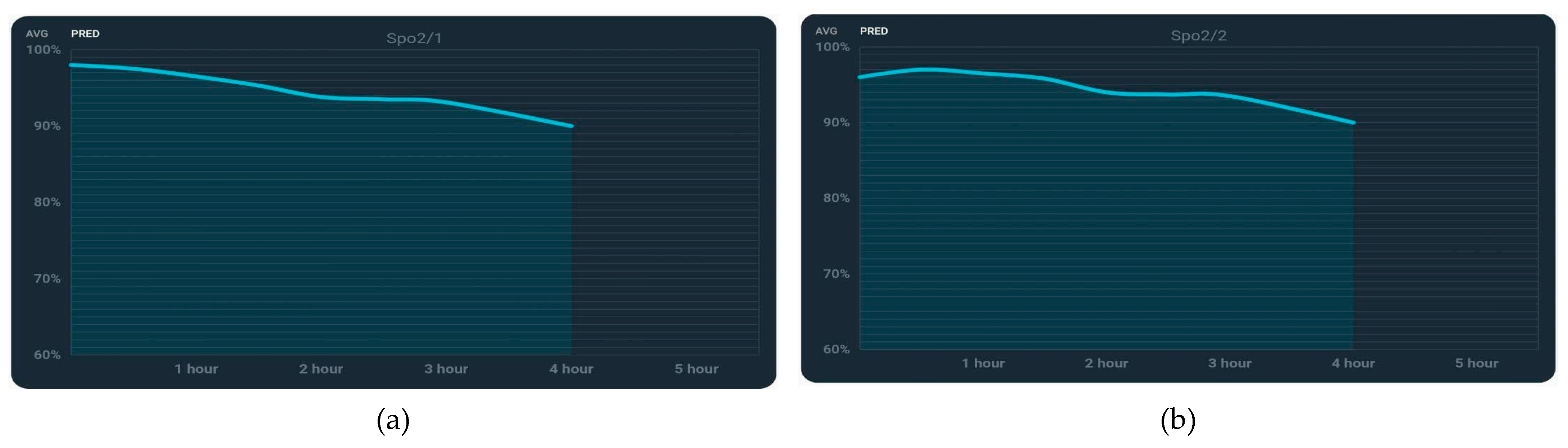
2.3. User Interface
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhattacharya, S.; Mishra, R.K. Pressure ulcers: Current understanding and newer modalities of treatment. Indian J. Plast. Surg. 2015, 48, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Josef, G.; Keith, H.; Steuart, E. ABC of wound healing Pressure Ulcers. BMJ J. 2006, 332, 472–475. [Google Scholar]
- Hadiza, M.; Farouk, M.A. Pressure Ulcer Stages among Bed-Ridden Patients in Ahmadu Bello University Teaching Hospital (ABUTH). IOSR J. Nurs. Health Sci. 2014, 3, 1. [Google Scholar]
- Pressure Sore Facts & Statistics. Available online: https://aquilacorp.com/resources/pressure-sores/statistics/ (accessed on 15 September 2020).
- Kaur, S.; Singh, A.; Tewari, M.K.; Kaur, T.R. Comparison of Two Intervention Strategies on Prevention of Bedsores among the Bedridden Patients: A Quasi Experimental Community-based Trial. Indian J. Palliat Care 2018, 24, 28–34. [Google Scholar] [PubMed]
- Thomas, D.R. Issues and Dilemmas in the Prevention and Treatment of Pressure Ulcers: A Review. J. Gerontol. Ser. A 2001, 56, M328–M340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauvage, P. Pressure ulcers prevention efficacy of an alternating pressure air mattress in elderly patients: E2MAO a randomized study. J. Wound Care 2017, 26, 304–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Chen, S.; Huang, H.; Kuo, S.; Shiu, Y. The Development of an Intelligent Monitoring and Caution System for Pressure ulcer Prevention. In Proceedings of the 2011 International Conference on Machine Learning and Cybernetics, Guilin, China, 10–13 July 2011. [Google Scholar]
- Nourani, M.; Pompeo, M.Q.; Tamil, L.S.; Ostadabbas, S.; Yousefi, R. Methods and Systems for Preventing Pressure Ulcers. U.S. Patent US20130090571A1, 11 April 2013. [Google Scholar]
- Cicceri, G.; Vita, F.D.; Bruneo, D.; Merlino, G.; Puliafito, A. A deep learning approach for pressure ulcer prevention using wearable computing. Hum. Cent. Comput. Inf. Sci. 2020, 10, 5869. [Google Scholar] [CrossRef]
- Aloweni, F.; Ang, S.Y.; Fook-Chong, S.; Agus, N.; Yong, P.; Goh, M.; Tucker-Kellogg, L.; Soh, R. A prediction tool for hospital-acquired pressure ulcers among surgical patients: Surgical pressure ulcer risk score. Int. Wound J. 2019, 16, 164–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cichosz, S.L.; Voelsang, A.; Tarnow, L.; Hasenkam, J.M.; Fleischer, J. Prediction of In-Hospital Pressure Ulcer Development. Adv. Wound Care 2019, 8, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousefi, R.; Ostadabbas, S.; Faezipour, M.; Nourani, M. A smart bed platform for monitoring & Ulcer prevention. In Proceedings of the 2011 4th International Conference on Biomedical Engineering and Informatics (BMEI), Shanghai, China, 15–17 October 2011. [Google Scholar]
- Brush, Z.; Bowling, A.; Tadros, M.; Russell, M. Design and control of a smart bed for pressure ulcer prevention. In Proceedings of the 2013 IEEE/ASME International Conference on Advanced Intelligent Mechatronics, Wollongong, Australia, 9–12 July 2013. [Google Scholar]
- Chesterton, L.S.; Foster, N.E.; Wright, C.C.; Baxter, G.D.; Barlas, P. Effects of TENS frequency, intensity and stimulation site parameter manipulation on pressure pain thresholds in healthy human subjects. PAIN J. 2003, 106, 73–80. [Google Scholar] [CrossRef]
- Jin, H.-K.; Hwang, T.-Y.; Cho, S.-H. Effect of Electrical Stimulation on Blood Flow Velocity and Vessel Size. Open Med. J. 2017, 12, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Cramp, A.F.; Gilsenan, C.; Lowe, A.S.; Walsh, D.W. The effect of high and low-frequency transcutaneous electrical nerve stimulation upon cutaneous blood flow and skin temperature in healthy subjects. Clin. Physiol. J. 2000, 20, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Nisar, H.; Malik, A.R.; Asawal, M.; Cheema, H.M. An Electrical Stimulation based Therapeutic Wearable for Pressure Ulcer Prevention. In Proceedings of the IEEE EMBS Conference on Biomedical Engineering and Sciences, Kuala Lumpur, Malaysia, 4–8 December 2016. [Google Scholar]
- Kottner, J.; Black, J.; Call, E.; Gefen, A.; Santamaria, N. Microclimate: A critical review in the context of pressure ulcer prevention. Clin. Biomech. J. 2018, 59, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Burns, T.; Breathnach, S.; Cox, N.; Griffiths, C. Rook’s Textbook of Dermatology, 4 Volume Set, 9th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2010. [Google Scholar]
- Bader, D.L.; Bouten, C.V.; Colin, D.; Oomens, C.W. Pressure Ulcers Research Current and Future Perspectives; Springer: Berlin/Heidelberg, Germany, 2005. [Google Scholar]
- Teferra, M.N. Functional Electrical Stimulation (FES): Review. Int. J. Latest Res. Eng. Technol. 2017, 24, 795–802. [Google Scholar]
- Flexiforce Sensoratasheet. Available online: https://cdn.sparkfun.com/datasheets/Sensors/ForceFlex/FLX-A201-A.pdf (accessed on 15 September 2020).
- Loadcell Datasheet. Available online: https://media.digikey.com/pdf/Data%20Sheets/Seeed%20Technology/114990100_Web.pdf (accessed on 15 September 2020).
- Datasheet of MAX30102 Sensor. Available online: https://www.alldatasheet.com/datasheet-pdf/pdf/859400/MAXIM/MAX30102.html (accessed on 15 September 2020).
- Datasheet SHT30. Available online: https://www.alldatasheet.com/datasheet-pdf/pdf/897974/ETC2/SHT30.html (accessed on 15 September 2020).
- Garcia-Vidal, C.; Sanjuan, G.; Puerta-Alcalde, P.; Moreno-Garcí, E.; Soriano, A. Artificial intelligence to support clinical decision-making processes. EBioMedicine 2019, 46, 27–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynn, L.A. Artificial intelligence systems for complex decision-making in acute care medicine: A review. Patient Saf. Surg. 2014, 13, 7575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sen, D.; McNeill, J.; Mendelson, Y.; Dunn, R.; Hickle, K. A New Vision for Preventing Pressure Ulcers: Wearable wireless devices could help solve a common-and serious-problem. IEEE J. 2018, 9, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.Y.C.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G. Staphylococcus aureus Infections: Epidemiology, Pathophysiology, Clinical Manifestations, and Management. Clin. Microbiol. Rev. J. 2015, 28, 603–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dana, A.N.; Bauman, W.A. Bacteriology of pressure ulcers in individuals with spinal cord injury: What we know and what we should know. J. Spinal Cord Med. 2015, 38, 147–160. [Google Scholar] [CrossRef] [Green Version]
- Wilkoff, V.L.; Westbrook, L.; Dixon, G. Factors affecting the persistence of Staphylococcus aureus on fabrics. Appl. Microbiol. J. 1969, 17, 268–274. [Google Scholar] [CrossRef] [PubMed]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensor | Range | Accuracy | Response Time |
|---|---|---|---|
| Flexiforce | 0.5–45 kg | ±3% | 5 µs |
| Load Cells | 50 kg | ±0.018% | 1 s |
| MAX30102 | 0–100% | ± 1% | 0.01 s |
| SHT30 | RH = 0–100% T = −40–125 °C | RH = ±1.5% T = ±0.2 °C | 2 s |
| Subject 9 | Age/Years | Gender | Weight kg | BMI kg/m2 | Condition |
|---|---|---|---|---|---|
| Subject 1 | 29 | Male | 75 | 29.3 | Control |
| Subject 2 | 25 | Male | 60 | 22 | Control |
| Subject 3 | 33 | Male | 90 | 28 | Control |
| Subject 4 | 43 | Male | 57 | 18.3 | Sacral ulcer |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saleh, Z.S.; Al-Neami, A.Q.; Raad, H.K. Smart Monitoring Pad for Prediction of Pressure Ulcers with an Automatically Activated Integrated Electro-Therapy System. Designs 2021, 5, 47. https://doi.org/10.3390/designs5030047
Saleh ZS, Al-Neami AQ, Raad HK. Smart Monitoring Pad for Prediction of Pressure Ulcers with an Automatically Activated Integrated Electro-Therapy System. Designs. 2021; 5(3):47. https://doi.org/10.3390/designs5030047
Chicago/Turabian StyleSaleh, Zeena Sh., Auns Qusai Al-Neami, and Haider K. Raad. 2021. "Smart Monitoring Pad for Prediction of Pressure Ulcers with an Automatically Activated Integrated Electro-Therapy System" Designs 5, no. 3: 47. https://doi.org/10.3390/designs5030047
APA StyleSaleh, Z. S., Al-Neami, A. Q., & Raad, H. K. (2021). Smart Monitoring Pad for Prediction of Pressure Ulcers with an Automatically Activated Integrated Electro-Therapy System. Designs, 5(3), 47. https://doi.org/10.3390/designs5030047