Heterogeneity of Rabies Vaccination Recommendations across Asia

Abstract
:Highlights
- The recommended practices for rabies pre- and post-exposure prophylaxis vary widely from country to country in Asia.
- Overall, the WHO recommendations for wound management are consistent in national guidelines. The post-exposure prophylaxis (PEP) 5-dose Essen and 4-dose Zagreb intramuscular (IM) regimens are uniformly recommended.
- The value of intradermal (ID) administration in reducing costs is not considered in several country guidelines.
- In the majority of the national recommendations, concurrent administration of rabies immunoglobulin (RIG) in category III exposures is recommended; however, there are concerns regarding availability and cost.
- Booster recommendations are not included in all guidelines, with limited clarity on booster requirement across the spectrum of risk of rabies exposure.
- Limited recommendations are available for special populations including pregnant women, aged population, and immunocompromised patients.
1. Introduction
2. Methods
3. Findings
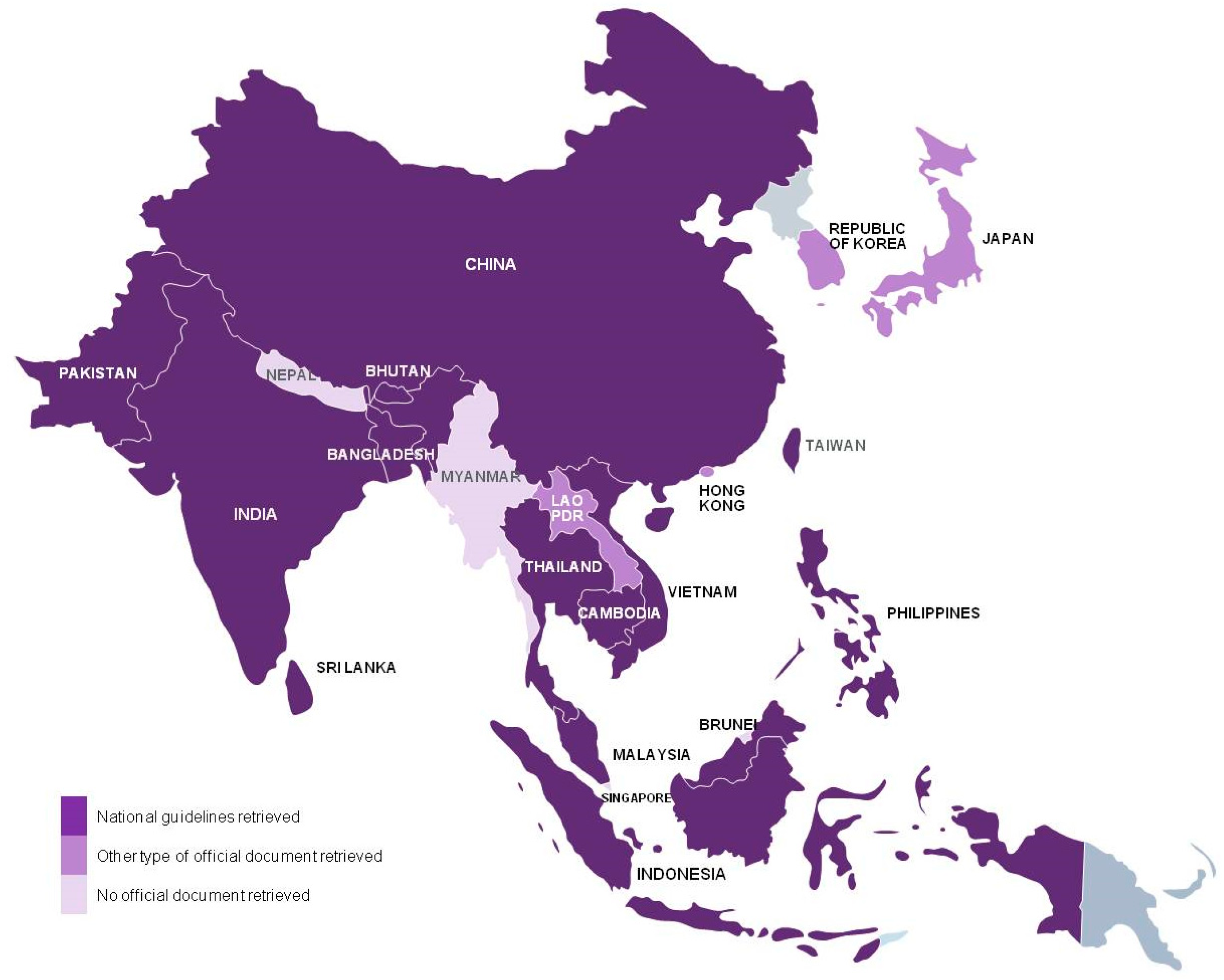
3.1. Overall Findings
3.2. Post-Exposure Prophylaxis (PEP)
3.2.1. Wound Care
3.2.2. RIG
3.2.3. PEP Vaccination Schedules
- The 5-dose Essen, 4-dose Zagreb, or both schedules were the regimens of choice for IM administration. The Essen is used in Bhutan, Cambodia, China, India, Philippines, Sri Lanka, Taiwan, Thailand, Vietnam; and Zagreb in Bangladesh, Cambodia, China, Indonesia, Pakistan, Philippines, Sri Lanka (Table 2). The 4-dose shortened Essen was the regimen of choice in the Malaysian recommendations, and was also recommended in the guidelines of Philippines (Table 2 and Table 3).
- We found recommendation for ID administration in 9 of the 13 retrieved national guidelines; the guidelines of China, Indonesia, Malaysia, and Taiwan do not include such recommendation (Table 2 and Table 3). Also in the official documents retrieved for Japan and Lao PDR we did not find ID recommendations (Table 2 and Table 3). All guidelines with ID recommendation suggested the updated Thai Red Cross regimen (Table 2 and Table 3).
- The Japanese guidelines recommend only subcutaneous (SC) administration as shown in Table 2.
3.2.4. PEP Vaccination for Re-Exposed Individuals
3.3. Pre-Exposure Prophylaxis (PrEP)
3.3.1. PrEP Vaccination Schedules
3.3.2. Booster after PrEP Vaccination
3.4. Vaccination Recommendations for Special Populations
- Pregnant and lactating women: The guidelines of Bangladesh, Bhutan, Cambodia, India, Pakistan, Philippines, and Sri Lanka state that there is no contraindication for vaccination in this population. The Chinese guidelines do not directly state whether PEP should be given or not, however they make reference to studies demonstrating that rabies vaccines are safe for pregnant women and for the fetus.
- Aged population and individuals with comorbidities: the same as above in the guidelines of Bangladesh, India, Pakistan, Philippines, and Sri Lanka.
- Immunocompromised population: full PEP and IM route is recommended in the guidelines of Bangladesh, Bhutan, India, Malaysia, Philippines, and Sri Lanka. There is no special reference to this population in the guidelines of Cambodia and Pakistan. Chinese guidelines indicate that passive immunization can be administered in patients with immunodeficiency disorder and that the antibody response should be closely monitored.
- Individuals on treatment for malaria taking chloroquine: ID is contraindicated and IM is recommended in the guidelines of Bangladesh, Cambodia, India, Malaysia, Pakistan, Philippines, and Sri Lanka.
- Other populations: Philippine’s guidelines also note that IM is contraindicated for individuals with hematologic conditions, for whom the ID route should be chosen and that ID is contraindicated for individuals with chronic liver disease.
4. Discussion
4.1. Characteristics of Human Rabies Burden
4.2. Rabies: An Unjustified Disease Burden
4.3. Rabies Vaccination Schedules Across Asia: Current Situation
PEP Recommendations
4.4. PrEP Recommendations
4.5. Country-Specific Information for Countries Whose National Guidelines Were Not Retrieved
4.6. Future Perspective
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| Ab | antibody |
| APCRI | Association for Prevention and Control of Rabies in India |
| CCEEV | cell culture vaccine and embryonated egg-based vaccines |
| CCV | cell culture vaccine |
| ERIG | equine immunoglobulin |
| FAO | Food and Agriculture Organization |
| GARC | Global Alliance for Rabies Control |
| HDCV | human diploid cells vaccine |
| HIV | human immunodeficiency virus |
| HRIG | human immunoglobulin |
| IAP | Indian Academy of Pediatrics |
| ID | intradermal |
| IM | intramuscular |
| NTD | Neglected Tropical Diseases |
| OIE | World Organization for Animal Health |
| PAHO | Pan American Health Organization |
| PCECV | purified chick embryo cell vaccine |
| PDEV | purified duck embryo vaccine |
| PEP | post-exposure prophylaxis |
| PHKCV | primary hamster kidney cell vaccine |
| PrEP | pre-exposure prophylaxis |
| PVRV | purified Vero rabies vaccine |
| RIG | rabies immunoglobulin |
| RVNA | rabies virus neutralizing antibodies |
| SAGE | Strategic Advisory Group of Experts |
| SC | subcutaneous |
| SDG | Sustainable Development Goals |
| SEARS | South-East Asia Rabies Strategy |
| UN | United Nations |
| WHO | World Health Organization |
References
- World Health Organization. WHO Expert Consultation on Rabies (Second Report); World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Hampson, K.; Coudeville, L.; Lembo, T.; Sambo, M.; Kieffer, A.; Attlan, M.; Barrat, J.; Blanton, J.D.; Briggs, D.J.; Cleaveland, S.; et al. Estimating the global burden of endemic canine rabies. PLoS Negl. Trop. Dis. 2015, 9, e0003709. [Google Scholar] [CrossRef]
- Fahrion, A.; Mikhailov, A.; Abela-Ridder, B.; Giacinti, J.; Harries, J. Human Rabies Transmitted by Dogs: Current Status of Global Data, 2015; World Health Organisation: Geneva, Switzerland, 2016. [Google Scholar]
- Food and Agriculture Organization of the United Nations (FAO). Developing a Stepwise Approach for Rabies Prevention and Control; FAO: Rome, Italy, 2013. [Google Scholar]
- World Health Organization; World Organisation for Animal Health (OIE); Food and Agriculture Organization of the United Nations (FAO); Global Alliance for Rabies Control (GARC). Global Elimination of Dog-Mediated Human Rabies: The Time is Now; Report of the Rabies Global Conference, 10–11 December 2015, Geneva, Switzerland; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Lavan, R.P.; King, A.I.; Sutton, D.J.; Tunceli, K. Rationale and support for a One Health program for canine vaccination as the most cost-effective means of controlling zoonotic rabies in endemic settings. Vaccine 2017, 35, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Cleaveland, S.; Lankester, F.; Townsend, S.; Lembo, T.; Hampson, K. Rabies control and elimination: A test case for One Health. Vet. Rec. 2014, 175, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Wangdi, K.; Ward, M.P. Human and animal rabies prevention and control cost in Bhutan, 2001–2008: The cost-benefit of dog rabies elimination. Vaccine 2012, 31, 260–270. [Google Scholar] [CrossRef]
- Maurya, I.; Vagholkar, K.; Patel, B.; Siddiqui, M.; Tiwari, S.; Maurya, P. State of globe: Rabies: The lethality since antiquity! J. Glob. Infect. Dis. 2015, 7, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Canine Rabies Blueprint. The Stepwise Approach towards Rabies Elimination: A Tool for Planning and Evaluation. Available online: http://caninerabiesblueprint.org/IMG/pdf/sare_outline_2017_f.pdf (accessed on 2 April 2017).
- Sugiyama, M.; Ito, N. Control of rabies: Epidemiology of rabies in Asia and development of new-generation vaccines for rabies. Comp. Immunol. Microbiol. Infect. Dis. 2007, 30, 273–286. [Google Scholar] [CrossRef] [PubMed]
- Dodet, B.; Goswami, A.; Gunasekera, A.; de Guzman, F.; Jamali, S.; Montalban, C.; Purba, W.; Quiambao, B.; Salahuddin, N.; Sampath, G.; Tang, Q.; Tantawichien, T.; Wimalaratne, O.; Ziauddin, A. Rabies awareness in eight Asian countries. Vaccine 2008, 26, 6344–6348. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Rabies Vaccines: WHO Position Paper; Weekly Epidemiological Record, No. 32 (85); World Health Organization: Geneva, Switzerland, 2010; Available online: http://www.who.int/wer/2010/wer8532.pdf?ua=1 (accessed on 6 April 2017).
- Wilde, H. Failures of post-exposure rabies prophylaxis. Vaccine 2007, 25, 7605–7609. [Google Scholar] [CrossRef] [PubMed]
- Madhusudana, S.N.; Mani, R.S. Intradermal vaccination for rabies prophylaxis: Conceptualization, evolution, present status and future. Expert Rev. Vaccines 2014, 13, 641–655. [Google Scholar] [CrossRef] [PubMed]
- Narayana, A.; Manoharan, A.; Narayan, M.S.; Kalappa, S.M.; Biligumba, G.; Haradanahalli, R.; Anand, A.M. Comparison of safety and immunogenicity of 2 WHO prequalified rabies vaccines administered by one week, 4 site intradermal regimen (4-4-4-0-0) in animal bite cases. Hum. Vaccines Immunother. 2015, 11, 1748–1753. [Google Scholar] [CrossRef] [PubMed]
- Tarantola, A.; Blanchi, S.; Cappelle, J.; Ly, S.; Chan, M.; In, S.; Peng, Y.; Hing, C.; Taing, C.N.; Ly, S.; et al. Rabies postexposure prophylaxis (PEP) noncompletion after dog bites: Estimating the unseen to meet the needs of the underserved. Am. J. Epidemiol. 2017. (accepted for publication). [Google Scholar]
- Dhaduk, K.M.; Unadkat, S.V.; Katharotiya, P.R.; Mer, A.R.; Chaudhary, M.C.; Prajapati, M.M. Case profile, volume analysis, and dropout rate of antirabies vaccination regimens among animal bite victims in Gujarat. Indian J. Public Health 2016, 60, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Tarantola, A. Four thousand years of concepts relating to rabies in animals and humans, its prevention and its cure. Trop. Med. Infect. Dis. 2017, 2. [Google Scholar] [CrossRef]
- Mahendra, B.J.; Narayana, D.A.; Agarkhedkar, S.; Ravish, H.S.; Harish, B.R.; Agarkhedkar, S.; Madhusudana, S.N.; Belludi, A.; Ahmed, K.; Jonnalagedda, R.; et al. Comparative study on the immunogenicity and safety of a purified chick embryo cell rabies vaccine (PCECV) administered according to two different simulated post exposure intramuscular regimens (Zagreb versus Essen). Hum. Vaccines Immunother. 2015, 11, 428–434. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Strategic Advisory Group of Experts (SAGE) Working Group on Rabies Vaccines and Rabies Immunoglobulins (Established July 2016). Available online: http://www.who.int/immunization/policy/sage/sage_wg_rabies_jul2016/en/ (accessed on 22 June 2017).
- World Health Organization. Human Rabies: 2016 Updates and Call for Data; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Bangladesh Disease Control Unit Directorate General of Health Services. National Guideline for Rabies Prophylaxis and Intra-Dermal Application of Cell Culture Rabies Vaccines; Ahmad, Z., Amin, R., Ussaman, S., Jamil, M., Ahmed, M., Eds.; Ministry of Health & Family Welfare: Dhaka, Bangladesh, 2010.
- Royal Government of Bhutan Ministry of Health Department of Pubic Health Zoonotic Disease Program. National Guideline for Management of Rabies, 2nd ed.; Royal Government of Bhutan Ministry of Health: Thimphu, Bhutan, 2014.
- Vanneth, D. Rabies Vaccine Procedure SOP-OPD-02–004, Rev. 2; National Institute of Public Health: Phnom Penh, Cambodia, 2012. [Google Scholar]
- Zhou, H.; Li, Y.; Chen, R.F.; Tao, X.Y.; Yu, P.C.; Cao, S.C.; Li, L.; Chen, Z.H.; Zhu, W.Y.; Yin, W.W.; et al. Technical guideline for human rabies prevention and control (2016). Zhonghua Liu Xing Bing Xue Za Zhi 2016, 37, 139–163. [Google Scholar] [PubMed]
- Indian National Centre for Disease Control. National Rabies Control Programme. National Guidelines on Rabies Prophylaxis; Directorate General of Health Services: Sham Nath Marg, Delhi, India, 2015.
- Vashishtha, V.M.; Choudhary, J.; Jog, P.; Yadav, S.; Unni, J.C.; Kamath, S.; Sachdeva, A.; Srirampur, S.; Prajapati, B.; Parekh, B.; et al. Indian Academy of Pediatrics (IAP) recommended immunization schedule for children aged 0 through 18 years—India, 2016 and updates on immunization. Indian Pediatr. 2016. (accepted for publication). [Google Scholar]
- Indonesia Kementerian Kesehatan RI Directorat Jenderal PP dan PL. Pedoman Pelaksanaan Program Penanggulangan Rabies Di Indonesia; Indonesia Ministry of Health: Jakarta, Indonesia, 2011. [Google Scholar]
- Malaysia Disease Control Division, Ministry of Health. Interim Guideline for Human Rabies Prevention & Control in Malaysia; Ministry of Health: Putrajaya, Malaysia, 2015.
- Pakistan Rabies Control Programme. Country Guidelines for the Prevention of Rabies; World Health Organization in consultation with Provincial Health Deaprtments: Geneva, Switzerland, 2013. [Google Scholar]
- Republic of the Philippines. New Guidelines on the Management of Rabies Exposures; Department of Health Office of the Secretary: Manila, Philippines, 2014. [Google Scholar]
- Mahipala, P.G.; Director General of Health Services. Protocol for Anti-Rabies Post Exposure Therapy (PET); Medical Research Institute: Colombo, Sri Lanka, 2016.
- Taiwan Center for Disease Control. (2016) Rabies Post Exposure Guidelines. Dissertation. Available online: http://www.cdc.gov.tw/professional/page.aspx?treeid=beac9c103df952c4&nowtreeid=b2db963d0bad6639 (accessed on 17 May 2017).
- Thai Department of Disease Control MOPH. Rabies Guideline and Frequent Questions; Thai Department of Disease Control MOPH: Nonthaburi, Thailand, 2015.
- Socialist Republic of Vietnam, Ministry of Health. Guidelines on Human Rabies Surveillance and Prevention; Ministry of Health: Hanoi, Vietnam, 2014.
- Hong Kong Center for Health Protection, Department of Health The Goverment of Hong Kong Special Administrative Region. Rabies. Available online: http://www.chp.gov.hk/en/content/9/24/3149.html (accessed on 29 March 2017).
- Hong Kong Center for Health Protection. Scientific Committee on Emerging and Zoonotic Diseases—Prevention and Control of Rabies; Hong Kong Center for Health Protection: Kowloon, Hong Kong, China, 2005.
- Hong Kong Travel Health Service Department of Health The Government of Hong Kong Special Administrative Region. Vaccine and Prophylaxis—Rabies Vaccination. Available online: http://www.travelhealth.gov.hk/english/vaccine_prophylaxis/rabies.html (accessed on 29 March 2017).
- Japan Ministry of Health Labour and Welfare. Q & A on Rabies Vaccination Guidelines. Available online: http://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou10/07.html (accessed on 17 May 2017).
- World Health Organization. Intradermal Application of Rabies Vaccines—Report of a WHO Consultation, Bangkok, Thailand; WHO Communicable Disease Surveillance and Control: Geneva, Switzerland, 2000. [Google Scholar]
- Korea Society of Infectious Disease. Recommended Adult Immunization for Foreign Travel. Available online: http://www.ksid.or.kr/file/vaccine_eng.pdf (accessed on 19 May 2017).
- Association of Southeast Asian Nations (ASEAN). ASEAN Rabies Elimination Strategy; OIE World Organisation for Animal Health: Bankok, Thailand, 2016. [Google Scholar]
- Knobel, D.L.; Cleaveland, S.; Coleman, P.G.; Fevre, E.M.; Meltzer, M.I.; Miranda, M.E.; Shaw, A.; Zinsstag, J.; Meslin, F.X. Re-evaluating the burden of rabies in Africa and Asia. Bull. World Health Organ. 2005, 83, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Sudarshan, M.K.; Madhusudana, S.N.; Mahendra, B.J.; Rao, N.S.; Narayana, D.A.; Rahman, S.A.; Meslin, F.X.; Lobo, D.; Ravikumar, K.; Gangaboraiah. Assessing the burden of human rabies in India: Results of a national multi-center epidemiological survey. Int. J. Infect. Dis. 2007, 11, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.H.; Hampson, K.; Fahrion, A.; Abela-Ridder, B.; Nel, L.H. Difficulties in estimating the human burden of canine rabies. Acta Trop. 2017, 165, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Banyard, A.C.; Horton, D.L.; Freuling, C.; Muller, T.; Fooks, A.R. Control and prevention of canine rabies: The need for building laboratory-based surveillance capacity. Antivir. Res. 2013, 98, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Ly, S.; Buchy, P.; Heng, N.Y.; Ong, S.; Chhor, N.; Bourhy, H.; Vong, S. Rabies situation in Cambodia. PLoS Negl. Trop. Dis. 2009, 3, e511. [Google Scholar] [CrossRef] [PubMed]
- Daniels, D.M.; Ritzi, R.B.; O’Neil, J.; Scherer, L.R. Analysis of nonfatal dog bites in children. J. Trauma Acute Care Surg. 2009, 66, S17–S22. [Google Scholar] [CrossRef] [PubMed]
- Dhand, N.K.; Gyeltshen, T.; Firestone, S.; Zangmo, C.; Dema, C.; Gyeltshen, R.; Ward, M.P. Dog bites in humans and estimating human rabies mortality in rabies endemic areas of Bhutan. PLoS Negl. Trop. Dis. 2011, 5, e1391. [Google Scholar] [CrossRef]
- Schalamon, J.; Ainoedhofer, H.; Singer, G.; Petnehazy, T.; Mayr, J.; Kiss, K.; Hollwarth, M.E. Analysis of dog bites in children who are younger than 17 years. Pediatrics 2006, 117, e374–e379. [Google Scholar] [CrossRef] [PubMed]
- Dodet, B. Report of the sixth AREB meeting, Manila, The Philippines, 10–12 November 2009. Vaccine 2010, 28, 3265–3268. [Google Scholar] [CrossRef] [PubMed]
- Sudarshan, M.K. Guidelines for Rabies Prophylaxis in Children. In Textbook of Pediatric Infectious Diseases, 1st ed.; Parthasarathy, A., Kundu, R., Agrawal, R., Eds.; Jaypee Brothers Medical Publishers: New Delhi, India, 2013; pp. 424–431. [Google Scholar]
- Matibag, G.C.; Kamigaki, T.; Kumarasiri, P.V.; Wijewardana, T.G.; Kalupahana, A.W.; Dissanayake, D.R.; De Silva, D.D.; Gunawardena, G.S.; Obayashi, Y.; Kanda, K.; et al. Knowledge, attitudes, and practices survey of rabies in a community in Sri Lanka. Environ. Health Prev. Med. 2007, 12, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Dhand, N.K.; Rai, B.D.; Tenzin, S.; Tsheten, K.; Ugyen, P.; Singye, K.; Ward, M.P. Community-based study on knowledge, attitudes and perception of rabies in Gelephu, south-central Bhutan. Int. Health 2012, 4, 210–219. [Google Scholar] [CrossRef]
- Salahuddin, N.; Gohar, M.A.; Baig-Ansari, N. Reducing cost of rabies post-exposure prophylaxis: experience of a tertiary care hospital in Pakistan. PLoS Negl. Trop. Dis. 2016, 10, e0004448. [Google Scholar] [CrossRef] [PubMed]
- Hampson, K.; Cleaveland, S.; Briggs, D. Evaluation of cost-effective strategies for rabies post-exposure vaccination in low-income countries. PLoS Negl. Trop. Dis. 2011, 5, e982. [Google Scholar] [CrossRef] [PubMed]
- Hemachudha, T.; Ugolini, G.; Wacharapluesadee, S.; Sungkarat, W.; Shuangshoti, S.; Laothamatas, J. Human rabies: Neuropathogenesis, diagnosis, and management. Lancet Neurol. 2013, 12, 498–513. [Google Scholar] [CrossRef]
- Rupprecht, C.E.; Briggs, D.; Brown, C.M.; Franka, R.; Katz, S.L.; Kerr, H.D.; Lett, S.; Levis, R.; Meltzer, M.I.; Schaffner, W.; et al. Evidence for a 4-dose vaccine schedule for human rabies post-exposure prophylaxis in previously non-vaccinated individuals. Vaccine 2009, 27, 7141–7148. [Google Scholar] [CrossRef] [PubMed]
- Dodet, B. An important date in rabies history. Vaccine 2007, 25, 8647–8650. [Google Scholar] [CrossRef] [PubMed]
- Tarantola, A.; Ly, S.; In, S.; Ong, S.; Peng, Y.; Heng, N.; Buchy, P. Rabies vaccine and rabies immunoglobulin in Cambodia: use and obstacles to use. J. Travel Med. 2015, 22, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Kessels, J.A.; Recuenco, S.; Navarro-Vela, A.M.; Deray, R.; Vigilato, M.; Ertl, H.; Durrheim, D.; Rees, H.; Nel, L.H.; Abela-Ridder, B.; et al. Pre-exposure rabies prophylaxis: A systematic review. Bull. World Health Organ. 2017, 95, 210–219C. [Google Scholar] [CrossRef] [PubMed]
- Davlin, S.L.; Lapiz, S.M.; Miranda, M.E.; Murray, K.O. Knowledge, attitudes, and practices regarding rabies in Filipinos following implementation of the Bohol Rabies Prevention and Elimination Programme. Epidemiol. Infect. 2014, 142, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- The South-East Asia Dog Rabies Elimination Strategy (SEARS). Rabies; OIE Regional Commission: Bangkok, Thailand, 2013. [Google Scholar]
- Devleesschauwer, B.; Aryal, A.; Sharma, B.K.; Ale, A.; Declercq, A.; Depraz, S.; Gaire, T.N.; Gongal, G.; Karki, S.; Pandey, B.D.; et al. Epidemiology, impact and control of rabies in Nepal: A systematic review. PLoS Negl. Trop. Dis. 2016, 10, e0004461. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 SDG Collaborators. Measuring the health-related Sustainable Development Goals in 188 countries: A baseline analysis from the Global Burden of Disease Study 2015. Lancet 2016, 388, 1813–1850. [Google Scholar] [CrossRef]
- Vigilato, M.A.; Clavijo, A.; Knobl, T.; Silva, H.M.; Cosivi, O.; Schneider, M.C.; Leanes, L.F.; Belotto, A.J.; Espinal, M.A. Progress towards eliminating canine rabies: Policies and perspectives from Latin America and the Caribbean. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2013, 368, 20120143. [Google Scholar] [CrossRef] [PubMed]
- Scott, T.P.; Coetzer, A.; de, B.K.; Wright, N.; Nel, L.H. The Pan-African Rabies Control Network (PARACON): A unified approach to eliminating canine rabies in Africa. Antivir. Res. 2015, 124, 93–100. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Categories of Exposure to Suspected or Confirmed Rabid Animal and Actions Required | |
|---|---|
| Category I |
|
| |
| |
| Action required: not regarded as exposures, no post-exposure prophylaxis is required | |
| Category II |
|
| |
| Action required: thorough local wound care and vaccine injection as soon as possible | |
| Category III |
|
| |
| |
| |
| Action required: thorough local wound care and administration of vaccine and RIG as soon as possible | |
| Passive Immunization: Rabies Immunoglobulin (RIG) | |
| Target population |
|
| |
| |
| Type, dose |
|
| |
| |
| Time and site |
|
| |
| Active Immunization: Vaccines | |
| Types | Cell culture vaccine (CCV) and embryonated egg-based vaccines (CCEEVs): |
| |
| |
| |
| and | |
| |
| Potency | ≥2.5 IU per single IM |
| Route of administration, dose, vaccine type, and injection sites |
|
| |
| Sites: | |
| |
| |
| |
| |
| |
| Sites: | |
| |
| |
| |
| Pre-Exposure Prophylaxis | |
| Indication |
|
| |
| |
| IM vaccination regimen | 3 doses, one IM dose on each of days 0, 7, and 21 or 28 |
| ID vaccination regimen | 3 doses, one ID injection of 0.1 mL on each of days 0, 7, and 21 or 28 * |
| Booster injections | Only for those working under continuous or frequent risk of exposure †, if rabies-virus neutralizing antibody titers is <0.5 IU/mL |
| Post-Exposure Prophylaxis | |
| Indication |
|
| |
| |
| Wound care |
|
| |
| |
| |
| |
| IM vaccination regimen § | 5-dose, Essen regimen (1-1-1-1-1): |
| one dose on each of days 0, 3, 7, 14, and 28 | |
| 4-dose, Zagreb regimen (2-0-1-0-1 or 2-1-1): | |
| 2 doses on day 0 (one in each of the two deltoid or thigh sites) followed by one dose on each of days 7 and 21 | |
| 4-dose shortened Essen regimen (1-1-1-1-0) for fully immunocompetent, exposed people who received wound care + high quality RIG + WHO prequalified rabies vaccine: | |
| One dose on each of days 0, 3, 7, and 14 | |
| For immunocompromised individuals including patients with HIV/AIDS: | |
| 5-dose CCEEV regimen + wound care + local infiltration with human RIG. Evaluation of the rabies-virus neutralizing antibody 2–4 weeks after vaccination and administration of an additional vaccine dose if needed. | |
| ID vaccination regimen § | The updated Thai Red Cross regimen (2-2-2-0-2): |
| Injections of 0.1 mL at two sites (deltoid and thigh) on each of days 0, 3, 7, and 28 | |
| Short Post-Exposure Prophylaxis for Previously Vaccinated Individuals | |
| Exposed or re-exposed individuals, or individuals with rabies-virus neutralizing antibody titers of ≥0.5 IU/mL: | |
| |
| |
| |
| Individuals exposed or re-exposed three months after complete vaccination: | |
| |
| Individuals with category III re- exposure who were vaccinated with a vaccine of unproven potency, or have received an incomplete course of vaccination: | |
| |
| Country | Document Title | Published by, (Year) | Available Vaccine Types (Route) | PEP Vaccination Schedule | PrEP Vaccination Schedule |
|---|---|---|---|---|---|
| Bangladesh | National Guideline for Rabies Prophylaxis and Intra-dermal Application of Cell Culture Rabies Vaccines [23] | Disease Control Unit, Ministry of Health & Family Welfare (2010) | PVRV (IM, ID) PCECV (IM, ID) ID administration is recommended as cost-effective and the technique is thoroughly described (not indicated for immunocompromised individuals) | IM: 4-dose Zagreb (Essen schedule described but not favored by the government) | IM: 3 doses, one injection on each of days 0, 7, and 21 or 28 |
| ID: Updated Thai Red Cross | ID: 3 doses, one injection on each of days 0, 7, and 21 or 28 | ||||
| Re-exposed previously vaccinated: 2 doses, one injection (IM or ID) on each of days 0 and 3, if re-exposure was ≤5 years after full PEP + wound washing (RIG not necessary) | Booster: 1 dose when titers <0.5 IU/mL, for individuals working under risk for rabies exposure, monitoring Ab titers every 6 months | ||||
| Bhutan | National Guideline for Management of Rabies [24] | Ministry of Health, Department of Public Health Zoonotic Disease Program (2014) | HDCV (IM) PVRV (IM, ID) | IM: 5-dose Essen | IM: 3 doses, one injection on each of days 0, 7, and 21 or 28 |
| ID: Updated Thai Red Cross | ID: 3 doses, one injection on each of days 0, 7, and 21 or 28 | ||||
| Re-exposed previously vaccinated: 2 doses (IM or ID), each on days 0 and 3, for those who have documented previous full vaccination. | Booster: 1 site ID at 1 year and every 3 years to lab staff, veterinarians, animal handlers, dog catchers, wildlife workers. Regular (exact timing not specified) monitoring of Ab titers and administration of a booster dose when titers <0.5 IU/mL. | ||||
| Cambodia | Rabies Vaccine Procedure SOP-OPD-02-004 [25] | National Institute of Public Health, National Public Health Laboratory (2012) | PDEV (IM) PCECV (IM, ID) HDCV (IM) PVRV (IM, ID) | IM: 5-dose Essen 4-dose Zagreb | IM: 3 doses, one injection on each of days 0, 7, 21–28 |
| ID: The updated Thai Red Cross 8-site Oxford (8-0-4-0-1-1 injection sites on days 0, 7, 28 and 90) | ID: 3 doses, one injection on each of days 0, 7, 21–28 | ||||
| Re-exposed previously vaccinated: 2 doses, one injection on each of days 0 and 3, in individuals who had receive at least 3 doses of any PEP regimen | |||||
| China | Technical Guidelines for Human Rabies Control and Prevention [26] | Chinese Center for Disease Control and Prevention (2016) | PVRV, (IM) HDCV, (IM) PHKCV, (IM) PCECV, (IM) | IM: 5-dose Essen 4-dose Zagreb | IM: 3 doses, one injection on each of days 0, 7, and 21 or 28 |
| Re-exposed previously vaccinated: 2 injections each on days 0 and 3 if >3 months have passed from previous full vaccination, if <3 months have passed, booster may be deferred if animal is healthy, vaccinated and accessible for observation | Booster: 1 booster dose when titers <0.5 IU/mL, for individuals working under risk for rabies exposure (monitoring every 6 months for lab workers and every 24 months for veterinarians/animal health officers) | ||||
| Hong Kong | Web page: Rabies [37] | Center for Health Protection, Department of Health (2017) | (not specified) | Thorough wound cleansing Vaccination if necessary | Travelers to endemic areas |
| Web page: Vaccine and Prophylaxis—Rabies Vaccination [39] | Travel Health Service, Department of Health (2012) | (not specified) | (not specified) | For Travelers to endemic areas, one month before the trip: 3 doses, one injection on each of days 0, 7, and 21 or 28 (Route is not specified) | |
| Scientific Committee on Emerging and Zoonotic Diseases — Prevention and Control of Rabies [38] | Center for Health Protection (2005) | (not specified) | (not specified) | (not specified) | |
| India | National Guidelines on Rabies Prophylaxis [27] | National Center for Disease Control (2015) | PCECV (IM, ID) PVRV (IM, ID) HDCV (IM) PDEV (IM) | IM: 5-dose Essen | IM: 3 doses, one injection on each of days 0, 7, and 21 or 28 |
| ID: Updated Thai Red Cross | Booster: 1 booster dose when Ab titers <0.5 IU/mL, for individuals working under risk for rabies exposure (monitoring every 6 months for the first 2 years and every 24 months thereafter) | ||||
| Re-exposed previously vaccinated: 2 doses (IM or ID), each on days 0 and 3, for those who have received full vaccination and re-exposed | |||||
| Indian Academy of Pediatrics (IAP) Recommended Immunization for Children Aged 0 through 18 years—India, 2016 and Updates on Immunization [28] | Indian Pediatrics (2016) | HDCV (IM) PCECV (IM) PDEV (IM) PVRV (IM) ID not in individual practice | IM: 5 doses, one dose on each day 0, 3, 7, 14, and 30, and for individuals with severe debility or immunosuppressed, and optional 6th dose on day 90 | IM: 3 doses, one injection on each of days 0, 7, 21, or 28 (day 28 is preferred) | |
| Re-exposed previously vaccinated: 2 doses for those who have received full vaccination and re-exposed | |||||
| Indonesia | National Guidelines for Rabies Vaccination [29] | Center for Disease Control, Ministry of Health (2011) | PVRV (IM) PCECV (IM) | IM: 4-dose Zagreb | IM: 3 doses, one injection on each of days 0, 7, 21, or 28 |
| Re-exposed previously vaccinated: 1 dose if re-exposure occurred 3–12 months from full vaccination, no vaccination below 3 months, full vaccination over 12 months | |||||
| Japan | Questions and answers on rabies [40] | Ministry of Health (2017) | (not specified) ID is not approved RIG is not approved | SC: 6 doses on days 0, 3, 7, 14, 30, and 90 | SC: week 0, 4 and month 6–12 |
| Re-exposed previously vaccinated: 2 injections for those who have received full vaccination, on days 0 and 3 | |||||
| Lao People’s Democratic Republic | Intradermal application of rabies vaccines. Report of a WHO consultation. Bangkok, Thailand 2000 [41] | WHO, Communicable Disease Surveillance and Control (2000) | PVRV (IM) PCECV (IM) ID not yet used, RIG is rarely used due high cost The ID route is not used | (not specified) | (not specified) |
| Malaysia | Interim guideline for human rabies prevention & control [30] | Ministry of Health, Disease Control Division (2015) | PVRV (IM) | IM: 4-dose shortened Essen | (not specified) |
| Re-exposed previously vaccinated: 2 doses on days 0 and 3 | |||||
| Pakistan | Country Guidelines for Prevention of Rabies. Pakistan Rabies Control Programme [31] | WHO in consultation with Provincial Health Departments (2013) | PVRV (IM, ID) PCECV (IM, ID) PDEV (IM) | IM: 4-dose Zagreb | IM: 3 doses, one injection on each of days 0, 7, 21, or 28 |
| ID: The updated Thai Red Cross | ID: 3 doses, one injection on each of days 0, 7, 21, or 28 | ||||
| Re-exposed previously vaccinated: 2 injections (IM or ID), for those who have received full vaccination, on days 0 and 3 | |||||
| Philippines | New Guidelines on the Management of Rabies Exposure [32] | Republic of Philippines. Department of Health (2014) | PVRV (IM, ID) PCECV (IM, ID) Among the first countries that adopted ID | IM: 5-dose Essen 4-dose Zagreb 4-dose shortened Essen | IM: 3 doses, one injection on each of days 0, 7, 21, or 28 |
| ID: The updated Thai Red Cross | ID: 3 doses, one injection on each of days 0, 7, 21, or 28 | ||||
| Re-exposed previously vaccinated: 2 injections (IM or ID), each on days 0 and 3 if the re-exposed individual had previously receive full vaccination, and full vaccination if he/she had not receive full vaccination course | Booster: Routine booster for individual with occupational risk: 1 dose after one year from full vaccination and one more thereafter in case of Ab titers <0.5 IU/mL | ||||
| Republic of Korea | Recommended Adult Immunizations for Foreign Travel [42] | Korea Society of Infectious Disease (2012) | (not specified) | 3 doses | |
| Sri Lanka | Protocol for anti-rabies post exposure therapy [33] | Director General of Health Services (2016) | PVRV (IM, ID) PCECV (IM, ID) | IM: 5-dose Essen 4-dose Zagreb | IM: 3 doses, one injection on each of days 0, 7, 21, or 28 |
| ID: Updated Thai Red Cross Modified 4-site ( 4-2-2-0-2): one dose at 4 sites on day 0 and one dose at 2 sites on days 3, 7, and 30 | ID: 3 doses, one injection on each of days 0, 7, 21, or 28 | ||||
| Re-exposed previously vaccinated: 2 injections (IM or ID), one on each of day 0 and 3, OR 4 ID at four sites on the same visit | Booster: One injection on the 1st year following full vaccination, and one more every five years | ||||
| Taiwan | Post-exposure guidelines [34] | Centers for Disease Control (2016) | (not specified, ID not recommended) | IM: 5-dose Essen | IM: one dose, on day 0, 7, 21 or 28 (3 doses) |
| Booster: For individuals at high risk (e.g., laboratory workers): 2 injections, one on each day 0 and 4 when Ab titers <0.5 IU/mL, For workers in animal health: One booster dose one year following full vaccination and every 3–5 years thereafter | |||||
| Thailand | Thai rabies management guidelines [35] | Queen Saovabha Memorial Institute (2015) | PCEVC (IM, ID) PVRV (IM, ID) PDEV (IM) | IM: 5-dose Essen | IM: 3 doses, one injection on each of days 0, 7, 21, or 28 |
| ID: Updated Thai Red Cross | ID: 3 doses, one injection on each of days 0, 7, 21, or 28 Only for PVRV: 2 doses, one injection on each of days 0 and 28 | ||||
| Re-exposed previously vaccinated: (a) 2 injections, each on day 0 and 3 if exposure occurred within 6 months from vaccination, no RIG; (b) same as previous or 4-site ID on a single visit if >6 months have elapsed from previous vaccination to exposure | Booster: For individuals at continuous or frequent risk of exposure: One booster vaccination if Ab titers <0.5 IU/mL | ||||
| Vietnam | Guidelines on human rabies surveillance and prevention [36] | Ministry of Health (2014) | Cell culture vaccines (not specified) | IM: 5-dose Essen | IM: 3 doses, one injection on each of days 0, 7, 21, or 28 One repeated injection every year |
| ID: Updated Thai Red Cross | Booster: One injection on 1st year from previous full vaccination and every year thereafter | ||||
| Re-exposed previously vaccinated: (a) 2 injections, each on days 0 and 3 if time from previous full vaccination <5 years; (b) Full vaccination if previous was not completed or >5 years have elapsed from previous full vaccination |
| Country | 5-Dose Essen (1-1-1-1-1) | 4-Dose Zagreb (2-0-1-0-1 or 2-1-1) | 4-Dose Essen (1-1-1-1-0) | Updated Thai Red Cross (2-2-2-0-2) |
|---|---|---|---|---|
| Bangladesh | X | X | X | |
| Bhutan | X | X | ||
| Cambodia | X | X | X | |
| China | X | X | ||
| India | X | X | ||
| Indonesia | X | |||
| Malaysia | X | |||
| Pakistan | X | X | ||
| Philippines | X | X | X | X |
| Sri Lanka | X | X | X | |
| Taiwan | X | |||
| Thailand | X | X | ||
| Vietnam | X | X |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchy, P.; Preiss, S.; Singh, V.; Mukherjee, P. Heterogeneity of Rabies Vaccination Recommendations across Asia. Trop. Med. Infect. Dis. 2017, 2, 23. https://doi.org/10.3390/tropicalmed2030023
Buchy P, Preiss S, Singh V, Mukherjee P. Heterogeneity of Rabies Vaccination Recommendations across Asia. Tropical Medicine and Infectious Disease. 2017; 2(3):23. https://doi.org/10.3390/tropicalmed2030023
Chicago/Turabian StyleBuchy, Philippe, Scott Preiss, Ved Singh, and Piyali Mukherjee. 2017. "Heterogeneity of Rabies Vaccination Recommendations across Asia" Tropical Medicine and Infectious Disease 2, no. 3: 23. https://doi.org/10.3390/tropicalmed2030023
APA StyleBuchy, P., Preiss, S., Singh, V., & Mukherjee, P. (2017). Heterogeneity of Rabies Vaccination Recommendations across Asia. Tropical Medicine and Infectious Disease, 2(3), 23. https://doi.org/10.3390/tropicalmed2030023