Trends in Tuberculosis Incidence in the Australian-Born in Victoria: Opportunities and Challenges to Elimination



Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics
3.2. Clinical Characteristics
3.3. Treatment Outcomes
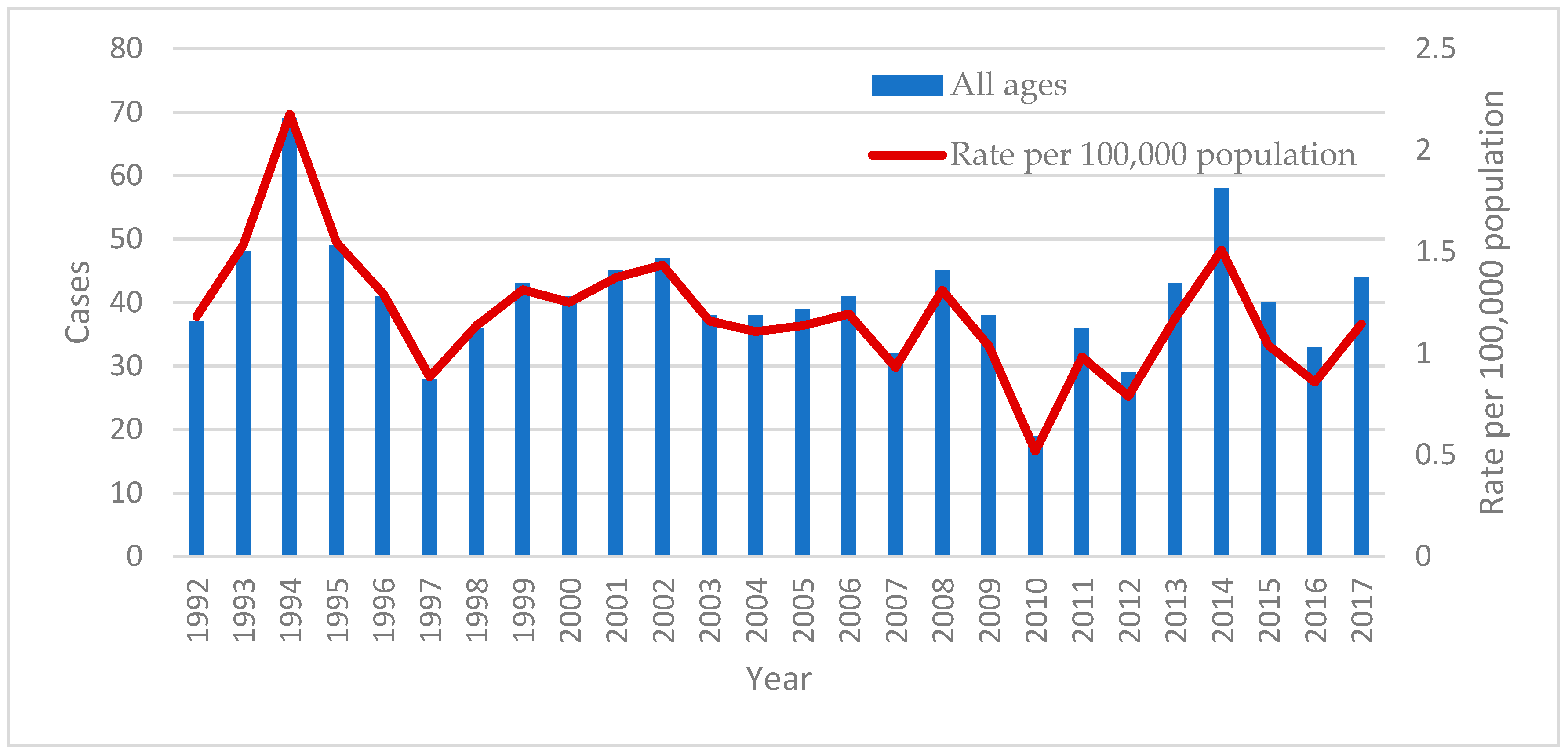
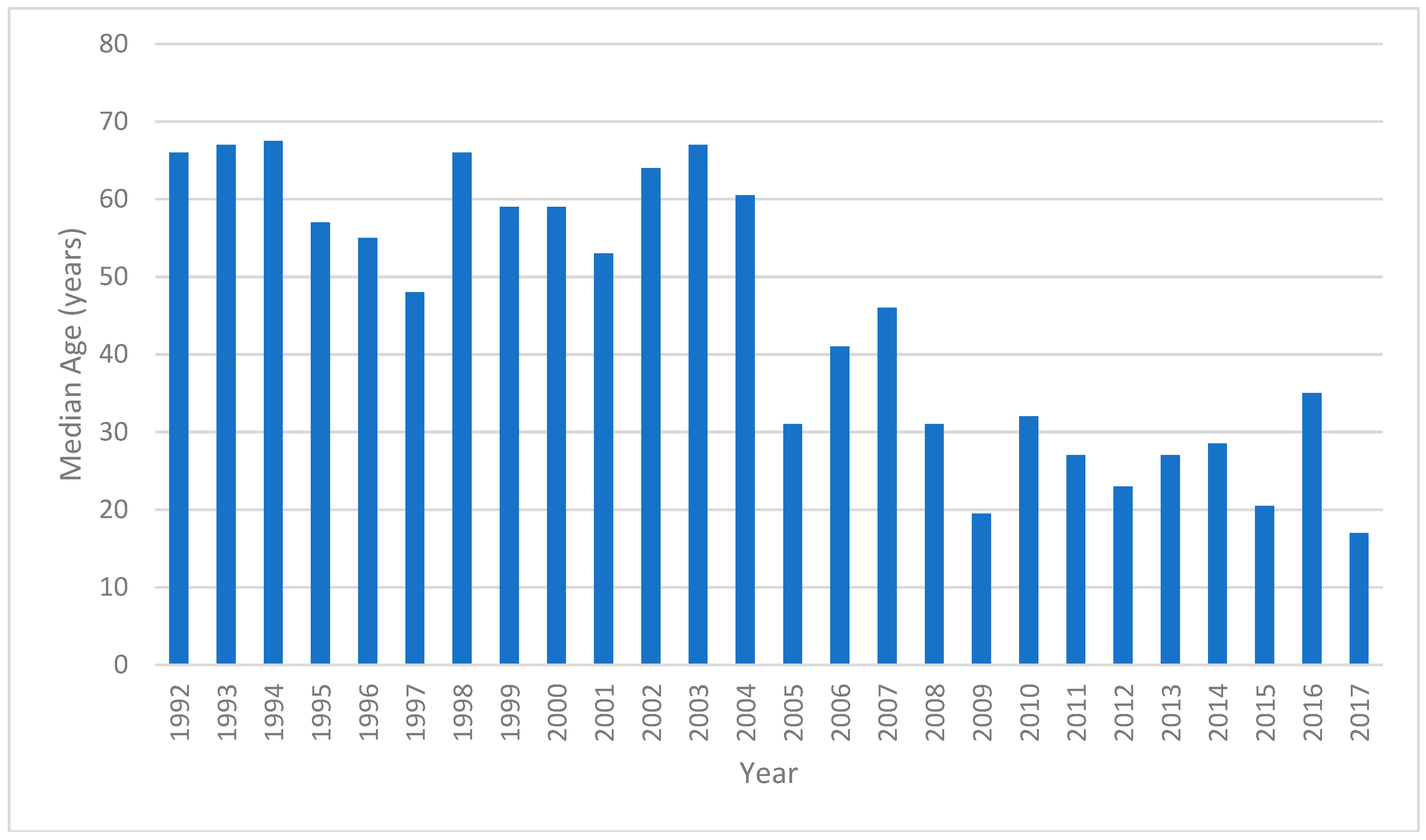
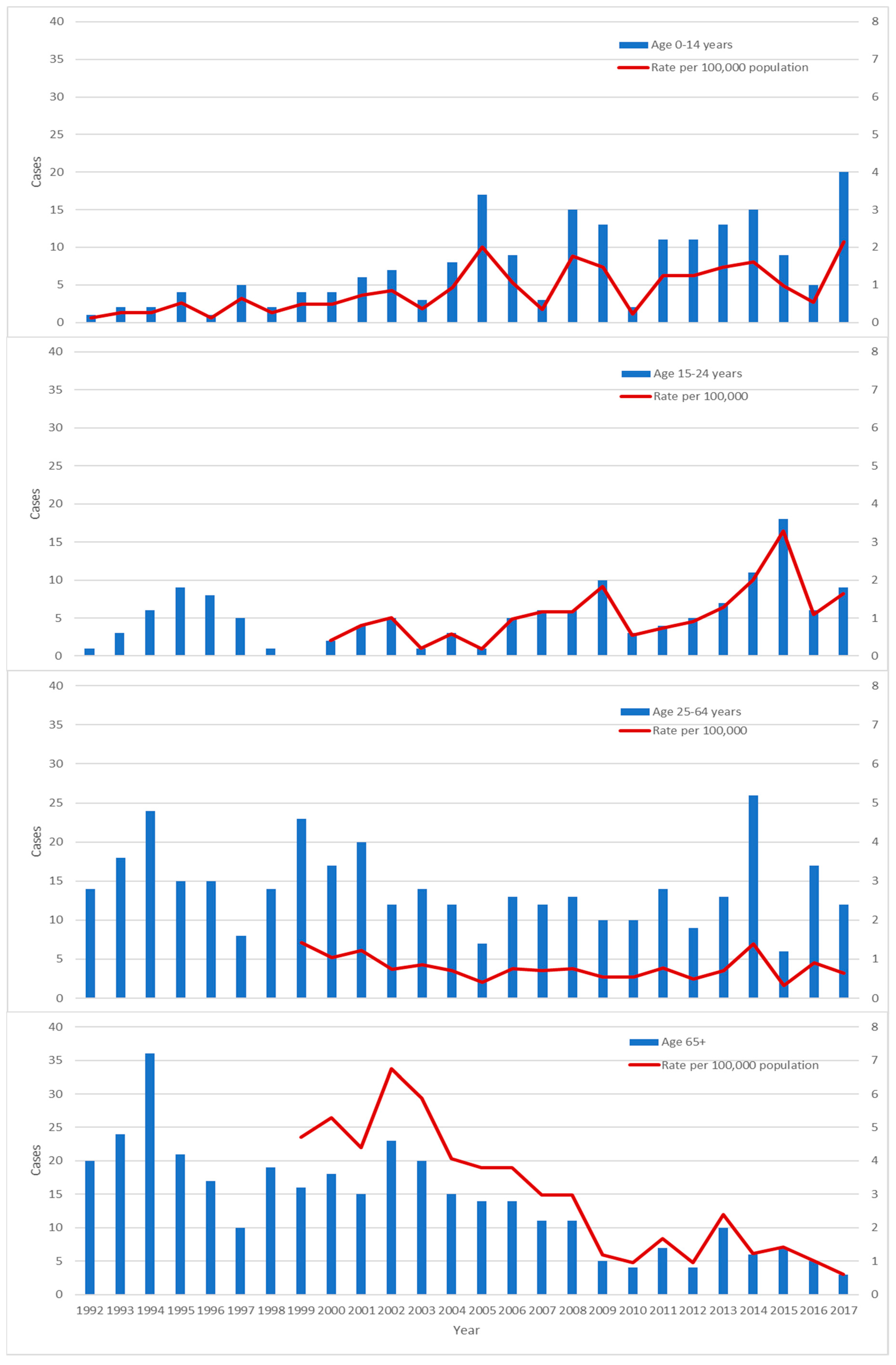
3.4. Trends
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). The End TB Strategy: Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Lonnroth, K.; Migliori, G.B.; Abubakar, I.; D’Ambrosio, L.; de Vries, G.; Diel, R.; Douglas, P.; Falzon, D.; Gaudreau, M.A.; Goletti, D.; et al. Towards tuberculosis elimination: An action framework for low-incidence countries. Eur. Respir. J. 2015, 45, 928–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toms, C.; Stapledon, R.; Waring, J.; Douglas, P. Tuberculosis notifications in Australia, 2012 and 2013. Commun. Dis. Intell. Q. Rep. 2015, 39, 217–235. [Google Scholar]
- Lavender, C.J.; Globan, M.; Kelly, H.; Brown, L.K.; Sievers, A.; Fyfe, J.A.; Lauer, T.; Leslie, D.E. Epidemiology and control of tuberculosis in Victoria, a low-burden state in south-eastern Australia, 2005–2010. Int. J. Tuberc. Lung Dis. 2013, 17, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Bareja, C.; Waring, J.; Stapledon, R.; Toms, C.; Douglas, P. Tuberculosis notifications in Australia, 2011. Commun. Dis. Intell. Q. Rep. 2014, 38, 356–368. [Google Scholar]
- 3101.0: Australian Demographic Statistics. September 2017. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/mf/3101.0 (accessed on 17 June 2018).
- Tuberculosis Case Definition. Available online: http://www.health.gov.au/internet/main/publishing.nsf/content/cda-surveil-nndss-casedefs-cd_tb.htm (accessed on 19 June 2018).
- WHO. Tuberculosis Country Profiles. Available online: http://www.who.int/tb/country/data/profiles/en/ (accessed on 26 June 2018).
- Dale, K.; Tay, E.; Trevan, P.; Denholm, J.T. Mortality among tuberculosis cases in Victoria, 2002–2013: Case fatality and factors associated with death. Int. J. Tuberc. Lung Dis. 2016, 20, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Census of Population and Housing. 1991. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/2101.01991?OpenDocument (accessed on 23 June 2018).
- Census of Population and Housing. 1996. Available online: http://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/1996/communityprofile/2?opendocument (accessed on 23 June 2018).
- Census of Population and Housing. 2001. Available online: http://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2001/quickstat/2?opendocument (accessed on 23 June 2018).
- Census of Population and Housing. 2006. Available online: http://abs.gov.au/websitedbs/censushome.nsf/home/historicaldata2006 (accessed on 23 June 2018).
- Census of Population and Housing. 2011. Available online: http://www.abs.gov.au/websitedbs/censushome.nsf/home/historicaldata2011?opendocument&navpos=280 (accessed on 23 June 2018).
- Census of Population and Housing. 2016. Available online: http://www.abs.gov.au/websitedbs/D3310114.nsf/Home/Census?OpenDocument&ref=topBar (accessed on 23 June 2018).
- McPherson, M.E.; Leslie, D.; Sievers, A.; Patel, M.; Kelly, H. Epidemiology of laboratory confirmed tuberculosis in Victoria, 1990 to 2004. Commun. Dis. Intell. Q. Rep. 2008, 32, 237–241. [Google Scholar] [PubMed]
- Globan, M.; Lavender, C.; Leslie, D.; Brown, L.; Denholm, J.; Raios, K.; Sievers, A.; Kelly, H.; Fyfe, J. Molecular epidemiology of tuberculosis in Victoria, Australia, reveals low level of transmission. Int. J. Tuberc. Lung Dis. 2016, 20, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Dale, K.D.; Globan, M.; Tay, E.L.; Trauer, J.M.; Trevan, P.G.; Denholm, J.T. Recurrence of tuberculosis in a low-incidence setting without directly observed treatment: Victoria, Australia, 2002–2014. Int. J. Tuberc. Lung Dis. 2017, 21, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Parvaresh, L.; Crighton, T.; Martinez, E.; Bustamante, A.; Chen, S.; Sintchenko, V. Recurrence of tuberculosis in a low-incidence setting: A retrospective cross-sectional study augmented by whole genome sequencing. BMC Infect. Dis. 2018, 18, 265. [Google Scholar] [CrossRef] [PubMed]
- Teo, S.S.; Tay, E.L.; Douglas, P.; Krause, V.L.; Graham, S.M. The epidemiology of tuberculosis in children in Australia, 2003–2012. Med. J. Aust. 2015, 203, 440. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.J.; Johnston, V.; Appuhamy, R.D.; Kaczmarek, M.; Hurwitz, M. The epidemiology of tuberculosis in the Australia Capital Territory, 2006–2015. Commun. Dis. Intell. Q. Rep. 2017, 41, 231–240. [Google Scholar]
- 3412.0—Migration, Australia, 2016–2017. Available online: http://www.abs.gov.au/ausstats/[email protected]/mf/3412.0/ (accessed on 8 August 2018).
- Denholm, J.T.; McBryde, E.S. Can Australia eliminate TB? Modelling immigration strategies for reaching MDG targets in a low-transmission setting. Aust. N. Z. J. Public Health 2014, 38, 78–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denholm, J.T.; Matteelli, A.; Reis, A. Latent tuberculous infection: Ethical considerations in formulating public health policy. Int. J. Tuberc. Lung Dis. 2015, 19, 137–140. [Google Scholar] [CrossRef] [PubMed]
- ASID. Recommendations for Comprehensive Post-Arrival Health Assessment for People from Refugee-Like Backgrounds; Australian Society for Infectious Diseases: Surry Hills, NSW, Australia, 2016.
- The BCG vaccine: Information and recommendations for use in Australia. National Tuberculosis Advisory Committee update October 2012. Commun. Dis. Intell. Q. Rep. 2013, 37, 65–72.




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Ages | 0–14 Years | ≥15 Years |
|---|---|---|---|
| Number of cases | 1057 | 192 | 865 |
| Median age (IQR) | 47 years (20, 73) | 3 years (2, 7) | 57 years (31, 76) |
| Male (%) | 618 (58.5) | 106 (55.2) | 512 (59.2) |
| Metropolitan (%) | 830 (78.5) | 178 (92.7) | 652 (75.4) |
| HIV co-infection 1 | 7 | 0 | 7 |
| Method of diagnosis (%) | |||
| Culture | 712 (67.4) | 62 (32.3) | 650 (75.1) |
| Radiologic | 145 (13.7) | 96 (50.0) | 49 (5.7) |
| Nucleic acid testing/microscopy | 61 (5.8) | 14 (7.3) | 47 (5.4) |
| Histology | 39 (3.7) | 3 (1.6) | 36 (4.2) |
| Clinical | 34 (3.2) | 12 (6.3) | 22 (2.5) |
| Missing | 66 (6.2) | 5 (2.6) | 61 (7.1) |
| Multi-drug resistance 2 | 8 | 1 | 7 |
| Manifestation (%) 3 | |||
| Pulmonary only | 610 (57.7) | 106 (55.2) | 504 (58.3) |
| Pulmonary and extrapulmonary | 128 (12.1) | 25 (13.0) | 103 (11.9) |
| Miliary | 20 (1.9) | 6 (3.1) | 14 |
| Extrapulmonary only | 273 (25.8) | 59 (30.7) | 214 (24.7) |
| Extrapulmonary manifestations | |||
| Lymphadenitis | 127 (12.0) | 50 (26.0) | 77 (8.9) |
| Pleural | 105 (9.9) | 6 (3.1) | 99 (11.4) |
| Bone/joint | 38 (3.6) | 5 (2.6) | 33 (3.8) |
| Genitourinary | 33 (3.1) | 1 (0.5) | 32 (3.7) |
| Meningeal | 18 (1.7) | 9 (4.7) | 9 (1.0) |
| Cutaneous | 7 (0.7) | 1 (0.5) | 6 (0.7) |
| Pericardial | 5 (0.5) | 0 | 5 (0.6) |
| Other | 5 (0.5) | 2 (1.0) | 3 (0.3) |
| Recurrence (%) | 13 (1.2) | 2 (1.0) | 11 (1.3) |
| Treatment outcomes 4 | |||
| Median duration (IQR) | 212 days (184, 278) | ||
| Completed treatment | 508 | 140 | 368 |
| Still on treatment | 36 | 18 | 18 |
| Death during treatment | 57 | 0 | 57 |
| Death from TB | 8 | 0 | 8 |
| Default | 4 | 1 | 3 |
| Lost to follow-up | 8 | 2 | 6 |
| Country or Region | Number (%) |
|---|---|
| Total | 149 |
| Africa | 60 (40.3) |
| Sudan | 24 (16.1) |
| Somalia | 25 (16.8) |
| Ethiopia | 9 (6.0) |
| Algeria | 1 (0.7) |
| Zimbabwe | 1 (0.7) |
| Southeast Asia | 49 (32.9) |
| Vietnam | 26 (17.4) |
| Philippines | 9 (6.0) |
| Indonesia | 3 (2.0) |
| Malaysia | 2 (1.3) |
| Timor-Leste | 2 (1.3) |
| Laos | 3 (2.0) |
| Cambodia | 3 (2.0) |
| Myanmar | 1 (0.7) |
| North Asia | 7 (4.7) |
| China | 6 (4.0) |
| Tibet | 1 (0.7) |
| South Asia | 15 (10.0) |
| India | 14 (9.4) |
| Pakistan | 1 (0.7) |
| Middle East | 8 (5.4) |
| Afghanistan | 7 (4.7) |
| Iraq | 1 (0.7) |
| Pacific Islands | 9 (6.0) |
| Tonga | 4 (2.7) |
| Samoa | 4 (2.7) |
| Fiji | 1 (0.7) |
| South America | |
| Peru | 1 (0.7) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, O.; Tay, E.L.; Denholm, J. Trends in Tuberculosis Incidence in the Australian-Born in Victoria: Opportunities and Challenges to Elimination. Trop. Med. Infect. Dis. 2018, 3, 112. https://doi.org/10.3390/tropicalmed3040112
Xie O, Tay EL, Denholm J. Trends in Tuberculosis Incidence in the Australian-Born in Victoria: Opportunities and Challenges to Elimination. Tropical Medicine and Infectious Disease. 2018; 3(4):112. https://doi.org/10.3390/tropicalmed3040112
Chicago/Turabian StyleXie, Ouli, Ee Laine Tay, and Justin Denholm. 2018. "Trends in Tuberculosis Incidence in the Australian-Born in Victoria: Opportunities and Challenges to Elimination" Tropical Medicine and Infectious Disease 3, no. 4: 112. https://doi.org/10.3390/tropicalmed3040112
APA StyleXie, O., Tay, E. L., & Denholm, J. (2018). Trends in Tuberculosis Incidence in the Australian-Born in Victoria: Opportunities and Challenges to Elimination. Tropical Medicine and Infectious Disease, 3(4), 112. https://doi.org/10.3390/tropicalmed3040112