Escherichia hermannii Infections in Humans: A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Data Search
2.2. Study Selection
2.3. Endpoints
2.4. Data Extraction and Definitions
3. Results
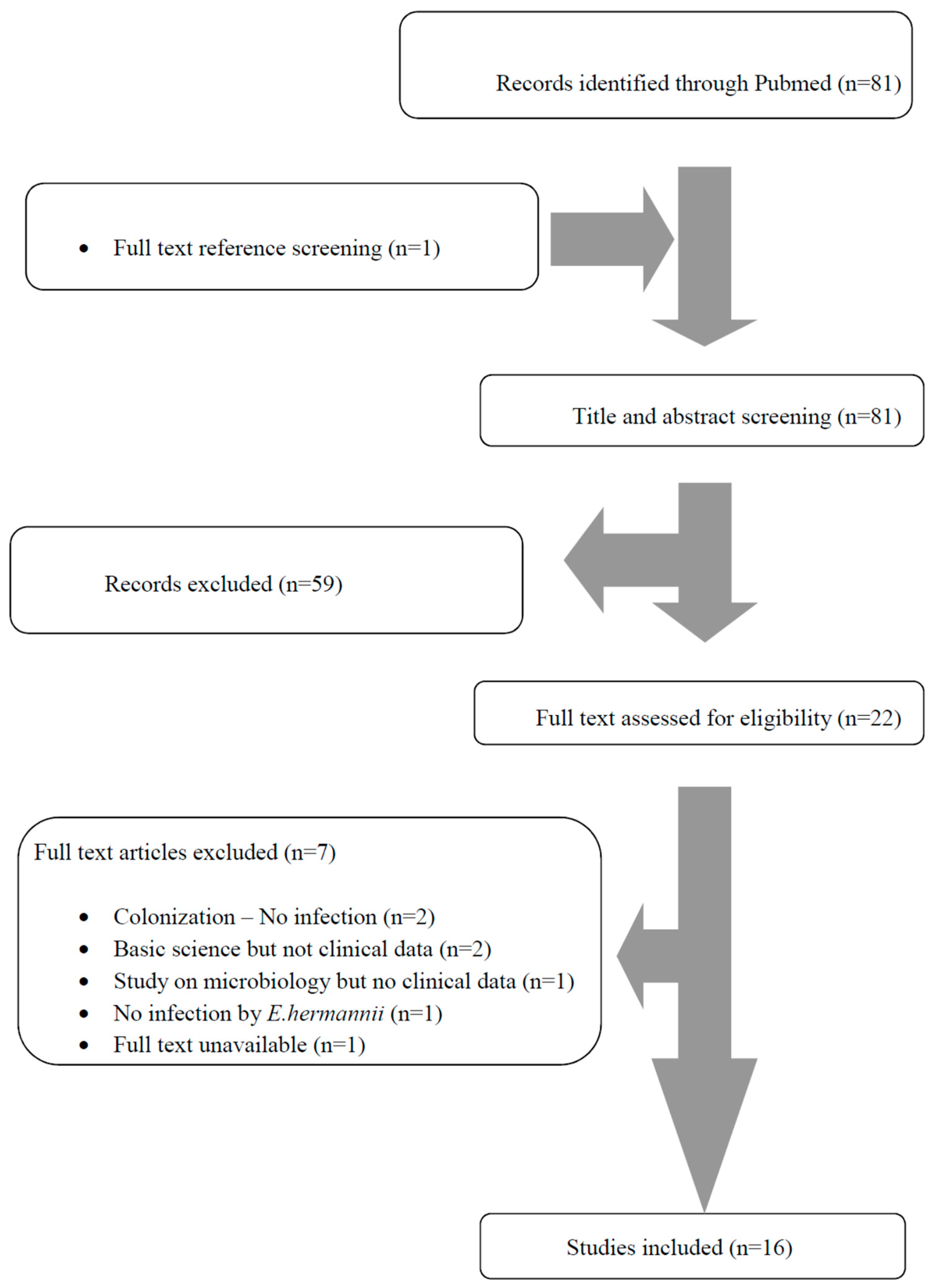
3.1. Literature Search
3.2. Included Studies’ Characteristics
3.3. Epidemiology, Microbiology, Antimicrobial Resistance Patterns, Treatment, and Outcomes of E. hermannii Infections
3.4. Bacteremias
3.5. Urinary Tract Infections
4. Discussion
Funding
Conflicts of Interest
References
- Brenner, D.J.; Davis, B.R.; Steigerwalt, A.G.; Riddle, C.F.; McWhorter, A.C.; Allen, S.D.; Farmer, J.J.; Saitoh, Y.; Fanning, G.R. Atypical biogroups of Escherichia coli found in clinical specimens and description of Escherichia hermannii sp. nov. J. Clin. Microbiol. 1982, 15, 703–713. [Google Scholar] [PubMed]
- Pien, F.D.; Shrum, S.; Swenson, J.M.; Hill, B.C.; Thornsberry, C.; Farmer, J.J. Colonization of human wounds by Escherichia vulneris and Escherichia hermannii. J. Clin. Microbiol. 1985, 22, 283–285. [Google Scholar] [PubMed]
- Dahl, K.M.; Barry, J.; DeBiasi, R.L. Escherichia hermannii infection of a cephalohematoma: Case report, review of the literature, and description of a novel invasive pathogen. Clin. Infect. Dis. 2002, 35, e96–e98. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.Q.; Xin, B.; Sun, S.Q. Pyelonephritis Caused Solely by Escherichia hermanii. Jundishapur J. Microbiol. 2014, 7, e18138. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Chaudhury, A.; Nath, G.; Tikoo, A.; Sanyal, S.C. Enteropathogenicity and antimicrobial susceptibility of new Escherichia spp. J. Diarrhoeal. Dis. Res. 1999, 17, 85–87. [Google Scholar] [PubMed]
- Sedlock, C.; Tokarczyk, M.; Sternlieb, M.; Flomenberg, P. PICC-associated infection with Escherichia hermannii: A case report and review of the literature. IDCases 2018, 13, e00444. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, H.G.; Daum, R.S. Escherichia hermannii sepsis with duodenal perforation in a neonate. Pediatr. Infect. Dis. J. 1987, 6, 300–302. [Google Scholar]
- Popescu, G.A.; Daha, I.; Popescu, C.; Mitache, E. Staphylococcus aureus and Escherichia hermanii in diabetes patient. Emerg. Infect. Dis. 2004, 10, 1335–1337. [Google Scholar] [CrossRef]
- Poulou, A.; Dimitroulia, E.; Markou, F.; Tsakris, A. Escherichia hermannii as the sole isolate from a patient with purulent conjunctivitis. J. Clin. Microbiol. 2008, 46, 3848–3849. [Google Scholar] [CrossRef] [PubMed]
- Kaewpoowat, Q.; Permpalung, N.; Sentochnik, D.E. Emerging Escherichia pathogen. J. Clin. Microbiol. 2013, 51, 2785–2786. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, S.; Seet, C. Escherichia hermannii bloodstream infection in a long-term haemodialysis patient. Pathology 2013, 45, 531. [Google Scholar] [CrossRef] [PubMed]
- Rank, C.U.; Lommer, K.P.; Schrøder, H.D.; Brandi, L. Catheter Related Escherichia hermannii Sepsis in a Haemodialysis Patient. Open Microbiol. J. 2016, 10, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Leski, T.A.; Taitt, C.R.; Bangura, U.; Stockelman, M.G.; Ansumana, R.; Cooper, W.H.; Stenger, D.A.; Vora, G.J. High prevalence of multidrug resistant Enterobacteriaceae isolated from outpatient urine samples but not the hospital environment in Bo, Sierra Leone. BMC Infect. Dis. 2016, 18, 167. [Google Scholar] [CrossRef] [PubMed]
- Powell, M.K.; Benková, K.; Selinger, P.; Dogoši, M.; Kinkorová, L.I.; Koutníková, H.; Laštíková, J.; Roubíčková, A.; Špůrková, Z.; Laclová, L.; et al. Opportunistic Infections in HIV-Infected Patients Differ Strongly in Frquencies and Spectra between Patients with Low CD4+ Cell Counts Examined Postmortem and Compensated Patients Examined Antemortem Irrespective of the HAART Era. PLoS ONE 2016, 11, e0162704. [Google Scholar] [CrossRef] [PubMed]
- Sood, S.; Hemrajani, S.K. Blood Stream Infection by Escherchia hermannii in a Neonate. J. Clin. Diagn. Res. 2016, 10, DD01–DD02. [Google Scholar] [CrossRef] [PubMed]
- Haasdijk, R.A.; van Ingen, J. Escherichia hermannii as the sole pathogen in urosepsis: Case report. New Microbes New Infect. 2017, 22, 100–101. [Google Scholar] [CrossRef] [PubMed]
- De Baere, T.; Wauters, G.; Huylenbroeck, A.; Claeys, G.; Peleman, R.; Verschraegen, G.; Allemeersch, D.; Vaneechoutte, M. Isolations of Leclercia adecarboxylata from a patient with a chronically inflamed gallbladder and from a patient with sepsis without focus. J. Clin. Microbiol. 2001, 39, 1674–1675. [Google Scholar] [CrossRef] [PubMed]
- Karkanaker, V.K.; Rai, R.; Shruthi, P.; Prasad, K. Septicaemia by Escherichia hermannii a perplexing diagnostic problem for a physician. Sci. Med. 2009, 1, 2. [Google Scholar]
- Murray, E.C.; Marek, A.; Thomson, P.C.; Coia, J.E. Gram-negative bacteraemia in haemodialysis. Nephrol. Dial. Transplant. 2015, 30, 1202–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qureshi, A.L.; Abid, K. Frequency of catheter related infections in haemodialysed uraemic patients. J. Pak. Med. Assoc. 2010, 60, 671–675. [Google Scholar]
- Mora-Rillo, M.; Fernández-Romero, N.; Navarro-San Francisco, C.; Díez-Sebastián, J.; Romero-Gómez, M.P.; Fernández, F.A.; López, J.R.A.; Mingorance, J. Impact of virulence genes on sepsis severity and survival in Escherichia coli bacteremia. Virulence 2015, 6, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ioannou, P.; Vamvoukaki, R.; Samonis, G. Rhodotorula species infections in humans: A systematic review. Mycoses 2018. [Google Scholar] [CrossRef] [PubMed]
- Stamatiades, G.A.; Ioannou, P.; Petrikkos, G.; Tsioutis, C. Fungal infections in patients with inflammatory bowel disease: A systematic review. Mycoses 2018, 61, 366–376. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Value |
|---|---|
| Male, n (%) | 7 out of 9 (77.8%) |
| Age, median (IQR) in years | 40 (16–64) |
| Medical history | |
| Central venous catheter, n (%) | 4 out of 7 (57.1%) |
| Chronic kidney disease, n (%) | 3 out of 9 (33.3%) |
| Solid organ transplantation, n (%) | 1 out of 9 (11.1%) |
| Malignancy on chemotherapy, n (%) | 1 out of 9 (11.1%) |
| Antibiotic susceptibility | |
| Antibiogram available, n (%) | 8 out of 9 (88.9%) |
| Penicillin resistance, n (%) | 7 out of 7 (100%) |
| Piperacillin tazobactam resistance, n (%) | 1 out of 4 (25%) |
| Tetracycline resistance, n (%) | 1 out of 4 (25%) |
| Carbapenem resistance, n (%) | 1 out of 4 (25%) |
| Quinolone resistance, n (%) | 1 out of 6 (16.7%) |
| Cephalosporine resistant, n (%) | 1 out of 7 (14.3%) |
| Information on infection | |
| Concomitant infection, n (%) | 2 out of 9 (22.2%) |
| Patients with fever, n (%) | 7 out of 9 (77.8%) |
| Patients with sepsis, n (%) | 6 out of 9 (66.7%) |
| Patients with organ dysfunction, n (%) | 2 out of 9 (22.2%) |
| Patients with shock, n (%) | 1 out of 9 (11.1%) |
| Patients requiring ICU care, n (%) | 2 out of 9 (22.2%) |
| Treatment of E. hermannii bacteremias | |
| Aminoglycosides, n (%) | 4 out of 8 (50%) |
| Piperacillin tazobactam, n (%) | 3 out of 8 (37.5%) |
| Cephalosporins, n (%) | 2 out of 8 (25%) |
| Quinolones, n (%) | 2 out of 8 (25%) |
| Trimethoprim sulfomethoxazole, n (%) | 2 out of 8 (25%) |
| Carbapenems, n (%) | 1 out of 8 (12.5%) |
| Amoxicillin clavulanate, n (%) | 1 out of 8 (12.5%) |
| Duration of treatment, median (IQR) in days | 14 (14–14) |
| Outcome | |
| Clinical cure, n (%) | 6 out of 7 (85.7%) |
| Deaths due to the infection, n (%) | 1 out of 7 (14.3%) |
| Deaths overall, n (%) | 1 out of 7 (14.3%) |
| Characteristic | Value |
|---|---|
| Male, n (%) | 2 out of 3 (66.7%) |
| Age, median (IQR) in years | 54 (43–65) |
| Medical history | |
| Solid organ transplantation, n (%) | 1 out of 4 (25%) |
| Antibiotic susceptibility | |
| Antibiogram available, n (%) | 4 out of 4 (100%) |
| Penicillin resistance, n (%) | 4 out of 4 (100%) |
| Piperacillin tazobactam resistance, n (%) | 1 out of 2 (50%) |
| Cephalosporin resistance, n (%) | 1 out of 3 (33.3%) |
| Quinolone resistance, n (%) | 1 out of 3 (33.3%) |
| Aminoglycoside resistance, n (%) | 1 out of 3 (33.3%) |
| ESBL phenotype, n (%) | 1 out of 3 (33.3%) |
| Information on infection | |
| Concomitant infection, n (%) | 1 out of 4 (25%) |
| Patients with fever, n (%) | 2 out of 3 (66.7%) |
| Patients with sepsis, n (%) | 2 out of 3 (66.7%) |
| Patients with organ dysfunction, n (%) | 1 out of 3 (33.3%) |
| Patients with shock, n (%) | 0 out of 3 (0%) |
| Patients requiring ICU care, n (%) | 0 out of 3 (0%) |
| Treatment of E. hermannii bacteremias | |
| Cephalosporins, n (%) | 2 out of 3 (66.7%) |
| Trimethoprim sulfomethoxazole, n (%) | 2 out of 3 (66.7%) |
| Aminoglycosides, n (%) | 1 out of 3 (33.3%) |
| Quinolones, n (%) | 1 out of 3 (33.3%) |
| Amoxicillin clavulanate, n (%) | 1 out of 4 (25%) |
| Duration of treatment, median (IQR) in days | 35 (14–56) |
| Outcome | |
| Clinical cure, n (%) | 3 out of 3 (100%) |
| Deaths overall, n (%) | 0 out of 3 (0%) |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioannou, P. Escherichia hermannii Infections in Humans: A Systematic Review. Trop. Med. Infect. Dis. 2019, 4, 17. https://doi.org/10.3390/tropicalmed4010017
Ioannou P. Escherichia hermannii Infections in Humans: A Systematic Review. Tropical Medicine and Infectious Disease. 2019; 4(1):17. https://doi.org/10.3390/tropicalmed4010017
Chicago/Turabian StyleIoannou, Petros. 2019. "Escherichia hermannii Infections in Humans: A Systematic Review" Tropical Medicine and Infectious Disease 4, no. 1: 17. https://doi.org/10.3390/tropicalmed4010017
APA StyleIoannou, P. (2019). Escherichia hermannii Infections in Humans: A Systematic Review. Tropical Medicine and Infectious Disease, 4(1), 17. https://doi.org/10.3390/tropicalmed4010017