Status of Schistosomiasis Elimination in the Caribbean Region

Abstract
:1. Introduction
2. Status of Schistosomiasis in the Caribbean
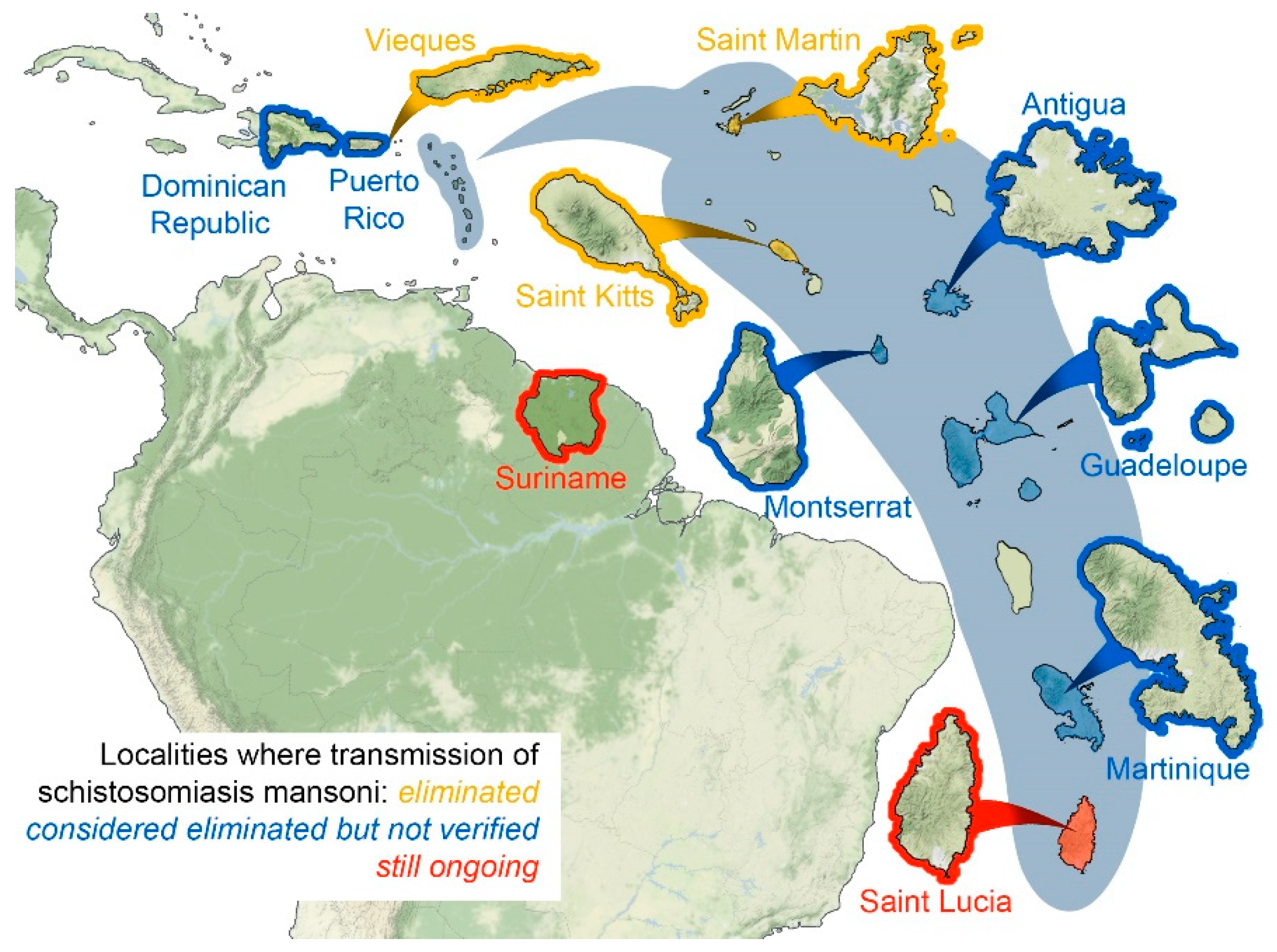
2.1. Localities Where Transmission of Schistosomiasis Mansoni Eliminated
2.1.1. Saint Martin
2.1.2. Saint Christopher (Saint Kitts)
2.1.3. Vieques
2.2. Localities Where Schistosomiasis Transmission Considered Eliminated but Not yet Verified
2.2.1. Puerto Rico
2.2.2. Dominican Republic
2.2.3. Antigua
2.2.4. Montserrat
2.2.5. Guadeloupe
2.2.6. Martinique
2.3. Localities Where Schistosomiasis Transmission Still Considered Ongoing
2.3.1. Saint Lucia
2.3.2. Suriname
3. Research and Control Needs
3.1. Updating Epidemiological Surveillance
3.2. Regional Snail Inventory
3.3. Animal Reservoir Hosts
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Manson, P. Report of a case of bilharzia from the West Indies. Br. Med. J. 1902, 2, 1894–1895. [Google Scholar] [CrossRef] [PubMed]
- Faust, E.C. Studies on Schistosomiasis mansoni in Puerto Rico. I. The history of schistosomiasis in Puerto Rico. P. R. J. Public Health Trop. Med. 1933, 9, 154–161. [Google Scholar]
- Prentice, M.A. Schistosomiasis and its intermediate hosts in the lesser Antillean islands of the Caribbean. Bull. Pan Am. Health Organ 1980, 14, 258–268. [Google Scholar] [PubMed]
- DeJong, R.J.; Morgan, J.A.T.; Paraense, W.L.; Pointier, J.P.; Amarista, M.; Ayeh-Kumi, P.F.K.; Babiker, A.; Barbosa, C.S.; Brémond, P.; Canese, A.P.; et al. Evolutionary relationships and biogeography of Biomphalaria (Gastropoda: Planorbidae) with implications regarding its role as host of the human bloodfluke, Schistosoma mansoni. Mol. Biol. Evol. 2001, 18, 2225–2239. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.A.T.; Dejong, R.J.; Adeoye, G.O.; Ansa, E.D.O.; Barbosa, C.S.; Brémond, P.; Cesari, I.M.; Charbonnel, N.; Corrêa, L.R.; Coulibaly, G.; et al. Origin and diversification of the human parasite Schistosoma mansoni. Mol. Ecol. 2005, 14, 3889–3902. [Google Scholar] [CrossRef] [PubMed]
- Cameron, T.W.M. A new definitive host for Schistosoma mansoni. J. Helminthol. 1928, 6, 219–222. [Google Scholar] [CrossRef]
- Swellengrebel, N.H.; Rijpstra, A.C. Lateral-spined schistosome ova in the intestine of a squirrel monkey from Suriname. Trop. Geogr. Med. 1965, 17, 80–84. [Google Scholar] [PubMed]
- Alarcón de Noya, B.; Pointier, J.P.; Colmenares, C.; Théron, A.; Balzan, C.; Cesari, I.M.; González, S.; Noya, O. Natural Schistosoma mansoni infection in wild rats from Guadeloupe: Parasitological and immunological aspects. Acta Trop. 1997, 68, 11–21. [Google Scholar] [CrossRef]
- Zoni, A.C.; Catalá, L.; Ault, S.K. Schistosomiasis prevalence and intensity of infection in Latin America and the Caribbean countries, 1942–2014, A systematic review in the context of a regional elimination goal. PLoS Negl. Trop. Dis. 2016, 10, e0004493. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, W.A. From San Juan to Aruba. P. R. J. Public Health Trop. Med. 1929, 5, 357–369. [Google Scholar]
- Jones, S.B. Intestinal bilharziasis in St. Kitts, British West Indies. J. Trop. Med. 1932, 35, 129–136. [Google Scholar]
- Ferguson, F.F.; Richards, C.S.; Sebastian, S.T.; Buchanan, I.C. Natural abatement of Schistosoma mansoni in St. Kitts, British West Indies. Public Health 1960, 74, 261–265. [Google Scholar] [CrossRef]
- Ferguson, F.F.; Palmer, J.R.; Jobin, W.R. Control of schistosomiasis on Vieques Island, Puerto Rico. Am. J. Trop. Med. Hyg. 1968, 17, 858–863. [Google Scholar] [CrossRef] [PubMed]
- Bundy, D.A.P. Caribbean schistosomiasis. Parasit 1984, 89, 377–406. [Google Scholar] [CrossRef]
- Jordan, P. Schistosomiasis: The St. Lucia Project; Cambridge University Press: Cambridge, UK, 1985; p. 442. [Google Scholar]
- Ivy, J.A.; King, C.H.; Cook, J.A.; Colley, D.G. Historical perspective: Revisiting the St. Lucia Project, a multi-year comparison trial of schistosomiasis control strategies. PLoS Negl. Trop. Dis. 2018, 12, e0006223. [Google Scholar] [CrossRef] [PubMed]
- Cameron, T.W.M. Observations on a parasitological tour of the Lesser Antilles. Proc. R. Soc. Med. 1929, 22, 37–45. [Google Scholar]
- PAHO. PAHO/WHO Schistosomiasis Regional Meeting: Defining a Road Map toward Verification of Elimination of Schistosomiasis Transmission in Latin America and the Caribbean by 2020; Pan American Health Organization: Washington, DC, USA, 2014; Available online: https://www.paho.org/hq/dmdocuments/2014/2014-cha-sch-regional-meeting-report.pdf (accessed on 10 December 2018).
- Giboda, M.; Malek, E.A.; Correa, R. Human schistosomiasis in Puerto Rico: Reduced prevalence rate and absence of Biomphalaria glabrata. Am. J. Trop. Med. Hyg. 1997, 57, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Haddock, K.C. Control of schistosomiasis: The Puerto Rican experience. Soc. Sci. Med. Part D Med. Geogr. 1981, 15, 501–514. [Google Scholar] [CrossRef]
- Jobin, W.R. Sugar and snails: The ecology of bilharziasis related to agriculture in Puerto Rico. Am. J. Trop. Med. Hyg. 1980, 29, 86–94. [Google Scholar] [CrossRef]
- Negro-Aponte, H.; Jobin, W.R. Schistosomiasis control in Puerto Rico. Twenty-five years of operational experience. Am. J. Trop. Med. Hyg. 1979, 28, 515–525. [Google Scholar] [CrossRef]
- Hillyer, G.V. The rise and fall of Bilharzia in Puerto Rico: Its centennial 1904–2004. P. R. Health Sci. J. 2005, 24, 225–235. [Google Scholar] [PubMed]
- Harry, H.; Aldrich, D. The ecology of Australorbis glabratus in Puerto Rico. Bull. World Health Organ 1958, 18, 819–832. [Google Scholar] [PubMed]
- Pointier, J.P.; Jourdane, J. Biological control of the snail hosts of schistosomiasis in areas of low transmission: The example of the Caribbean area. Acta Trop. 2000, 77, 53–60. [Google Scholar] [CrossRef]
- Pointier, J.P.; David, P.; Jarne, P. The biological control of the snail hosts of schistosomes: The role of competitor snails and biological invasions. In Biomphalaria Snails and Larval Trematodes; Toledo, R., Fried, B., Eds.; Springer: New York, NY, USA, 2011; pp. 215–238. [Google Scholar]
- Butler, J.M.; Ferguson, F.F.; Palmer, J.R.; Jobin, W.R. Displacement of a colony of Biomphalaria glabrata by an invading population of Tarebia granifera in a small stream in Puerto Rico. Caribb. J. Sci. 1980, 16, 73–80. [Google Scholar]
- Chaniotis, B.N.; Butler, J.M., Jr.; Ferguson, F.F.; Jobin, W.R. Bionomics of Tarebia granifera (Gastropoda: Thiaridae) in Puerto Rico, an Asiatic vector of Paragonimiasis westermani. Caribb. J. Sci. 1980, 16, 81–90. [Google Scholar]
- Jobin, W.R.; Ferguson, F.F.; Palmer, J.R. Control of schistosomiasis in Guayama and Arroyo, Puerto Rico. Bull. World Health Organ 1970, 42, 151–156. [Google Scholar] [PubMed]
- Palmer, J.R.; Colón, A.Z.; Ferguson, F.F.; Jobin, W.R. The control of schistosomiasis in Patillas. P. R. Public Health Rep. 1969, 84, 1003–1007. [Google Scholar] [CrossRef]
- McMullen, D.B. Discussion of the paper by Willard H. Wright: “Schistosomiasis as a world problem”. Bull. N. Y. Acad. Med. 1968, 44, 3–6. [Google Scholar]
- Iatroski, L.S.; Davis, A. The schistosomiasis problem in the world: Results of a WHO questionnaire survey. Bull. World Health Organ 1981, 59, 115–127. [Google Scholar]
- Jobin, W.R.; Brown, R.A.; Vélez, S.P.; Ferguson, F.F. Biological control of Biomphalaria glabrata in major reservoirs of Puerto Rico. Am. J. Trop. Med. Hyg. 1977, 26, 1018–1024. [Google Scholar] [CrossRef]
- Utroska, J.A.; Chen, M.G.; Dixon, H.; Yoon, S.; Helling-Borda, M.; Hogerzeil, H.V.; Mott, K.E. An Estimate of Global Needs for Praziquantel within Schistosomiasis Control Programmes. Available online: http://whqlibdoc.who.int/ HQ/1989/WHO_SCHISTO_89.102_Rev1.pdf (accessed on 15 December 2018).
- Central Intelligence Organization. The World Factbook 2017–18; Washington, DC, USA, 2018. Available online: https://www.cia.gov/library/publications/the-world-factbook/fields/2212.html (accessed on 10 December 2018).
- U. S. Bureau of the Census. U.S. Census of Population: 1950, Volume 1 Number of Inhabitants; U. S. Government Printing Office: Washington, DC, USA, 1952; pp. 53–56. Available online: https://www2.census.gov/prod2/decennial/documents/23761117v1ch12.pdf (accessed on 15 December 2018).
- Ponce Pinedo, A.M. Schistosomiasis mansoni in the Republic of Santo Domingo with a report of six cases studied. P. R. J. Public Health Trop. Med. 1947, 22, 308–324. [Google Scholar]
- WHO. Atlas of the Global Distribution of Schistosomiasis—Dominican Republic, Puerto Rico; World Health Organization: Geneva, Switzerland, 1987. [Google Scholar]
- Schneider, C.R.; Hiatt, R.A.; Malek, E.A.; Ruiz-Tiben, E. Assessment of schistosomiasis in the Dominican Republic. Public Health Rep. 1985, 100, 524–530. [Google Scholar] [PubMed]
- Vaughn, C.M.; Olivier, L.; Hendricks, J.R.; Mackie, T.T. Mollusciciding operations in an endemic area of schistosomiasis in the Dominican Republic. Am. J. Trop. Med. Hyg. 1952, 3, 518–528. [Google Scholar] [CrossRef]
- Wright, W.H. Schistosomiasis as a World Problem. Bull. N. Y. Acad. Med. 1968, 44, 301–312. [Google Scholar] [PubMed]
- Hotez, P.J.; Bottazzi, M.E.; Franco-Paredes, C.; Ault, S.K.; Periago, M.R. The neglected tropical diseases of Latin America and the Caribbean: A review of disease burden and distribution and a roadmap for control and elimination. PLoS Negl. Trop. Dis. 2008, 2, e300. [Google Scholar] [CrossRef] [PubMed]
- Rollinson, D.; Knopp, S.; Levitza, S.; Stothard, J.R.; Tchuem Tchuentée, L.A.; Garba, A.; Mohammed, K.A.; Schurb, N.; Person, B.; Colley, D.G.; et al. Time to set the agenda for schistosomiasis elimination. Acta Trop. 2013, 128, 423–440. [Google Scholar] [CrossRef] [PubMed]
- PAHO. Neglected Infectious Diseases in the Americas: Success Stories and Innovation to Reach the Neediest; Pan American Health Organization: Washington, DC, USA, 2016; Available online: http://iris.paho.org/xmlui/handle/123456789/31250 (accessed on 15 December 2018).
- Sodeman, W.A., Jr. Thiara (Tarebia) granifera (Lamarck): An agent for biological control of Biomphalaria. In Aquaculture and Schistosomiasis, Proceedings of the a Network Meeting, Manila, Philippines, 6–10 August 1991; National Research Council, Ed.; National Academy Press: Washington, DC, USA, 1992. Available online: http://www.nzdl.org/gsdlmod?e=d-00000-00---off-0hdl--00-0----0-10-0---0---0direct-10---4-------0-1l--11-en-50---20-about---00-0-1-00-0--4----0-0-11-10-0utfZz-8-00&cl=CL1.1&d=HASHb35dbf907ec64c6abd14b3.6.3.1&gc=0 (accessed on 10 December 2015).
- Chitsulo, L.; Engels, D.; Montresor, A.; Savioli, L. The global status of schistosomiasis and its control. Acta Trop. 2000, 77, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Tikasingh, E.S.; Wooding, C.D.; Long, E.; Lee, C.P.; Edwards, C. The presence of Schistosoma mansoni in Montserrat Leeward Islands. J. Trop. Med. Hyg. 1982, 85, 41–43. [Google Scholar]
- WHO. WHO Schistosomiasis Progress Report 2001–2011 and Strategic Plan 2012–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Facon, B.; Pointier, J.P.; Glaubrecht, M.; Poux, C.; Jarne, P.; David, P. A molecular phylogeography approach to biological invasions of the New World by parthenogenetic Thiarid snails. Mol. Ecol. 2003, 12, 3027–3039. [Google Scholar] [CrossRef]
- Théron, A.; Sire, C.; Rognon, A.; Prugnolle, F.; Durand, P. Molecular ecology of Schistosoma mansoni transmission inferred from the genetic composition of larval and adult infrapopulations within intermediate and definitive hosts. Parasit 2004, 126, 1–15. [Google Scholar] [CrossRef]
- Théron, A. Early and late shedding patterns of Schistosoma mansoni cercariae: Ecological significance in transmission to human and murine hosts. J. Parasitol. 1984, 70, 652–655. [Google Scholar]
- Théron, A.; Pointier, J.P.; Combes, C. Approche écologique du problème de la responsibilité de l’homme et du rat dans le fonctionnement d’un site de transmission à Schistosoma mansoni en Guadeloupe. Ann. Parasitol. Hum. Comp. 1978, 53, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Pointier, J.P.; Théron, A. Transmission de la bilharziose intestinale aux Antilles Guyane. Bull. D’Alerte Surveillance Antilles Guyane 2006, 1, 1–4. [Google Scholar]
- Pointier, J.; Théron, A.; Borel, G. Ecology of the introduced snail Melanoides tuberculata (Gastropoda; Thiaridae) in relation to Biomphalaria glabrata in the marshy forest area of Guadeloupe, French West Indies. J. Molluscan Stud. 1993, 59, 421–428. [Google Scholar] [CrossRef]
- Mazé, H. Catalogue des coquilles terrestres et fluviatiles recueillies à la Martinique en 1873. J. Conchyliol. 1874, 22, 158–173. [Google Scholar]
- Noc, F. La bilharziose á la Martinique. Bull. Soc. Path Exot. 1910, 3, 26. [Google Scholar]
- Guyard, A.; Pointier, J.P. Faune malacologique dulcaquicole et vecteurs de la schistosome en Martinique (Antilles francaises). Ann. Parasitol. Hum. Comp. 1979, 54, 193–205. [Google Scholar] [CrossRef]
- Pointier, J.P.; Guyard, A.; Théron, A.; Dumoutier, A. Le fonctionnement d’un site de transmission à Schistosoma mansoni en Martinique (Antilles françaises). Ann. Parasitol. Hum. Comp. 1984, 59, 589–595. [Google Scholar] [CrossRef]
- Dreyfuss, R. Les planorbes de la Martinique. Bull. Soc. Fr. Hist. Nat. Ant. 1953, 2, 41–45. [Google Scholar]
- Guyard, A.; Pointier, J.P.; Théron, A.; Gilles, A. Mollusques hôtes intermédiaires de la schistosomose intestinale dans les Petites Antilles. Hypothèses sur le rôle de Biompbalaria glabrata et B. straminea en Martinique. Malacologia 1982, 22, 103–107. [Google Scholar]
- Pointier, J. Invading freshwater snails and biological control in Martinique Island, French West Indies. Mem. Inst. Oswaldo Cruz 2001, 96, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pointier, J.P.; Guyard, A. Biological control of the snail intermediate hosts of Schistosoma mansoni in Martinique, French West Indies. Trop. Med. Parasitol. 1992, 43, 98–101. [Google Scholar]
- Pointier, J.P.; Samadi, S.; Jarne, P.; Delay, B. Introduction and spread of Thiara granifera (Lamarck, 1822) in Martinique, French West Indies. Biodivers. Conserv. 1998, 7, 1277–1290. [Google Scholar] [CrossRef]
- Vinter, N.S.B. Schistosomiasis in St. Lucia. Br. Med. J. 1964, 1, 119. [Google Scholar] [CrossRef]
- Sturrock, R.F.; Barnish, G.; Upatham, E.S. Snail findings from an experimental mollusciciding programme to control Schistosoma mansoni transmission on St. Lucia. Int. J. Parasitol. 1974, 4, 231–240. [Google Scholar] [CrossRef]
- PAHO. Schistosomiasis in Suriname. PAHO/WHO Preparatory Meeting on Epidemiological Data Needed to Plan Elimination of Schistosomiasis in the Caribbean; Pan American Health Organization: Washington, DC, USA, 2007. [Google Scholar]
- Sturrock, R.F. Field studies on the transmission of schistosomiasis mansoni and on the bionomics of its intermediate host, Biomphalaria glabrata, on St Lucia, West Indies. Int. J. Parasitol. 1973, 3, 175–194. [Google Scholar] [CrossRef]
- Sturrock, R.F. Control of Schistosoma mansoni transmission: Strategy for using molluscicides on St Lucia. Int. J. Parasitol. 1973, 3, 795–801. [Google Scholar] [CrossRef]
- Upatham, E.S. Exposure of caged Biomphalaria glabrata (Say) to investigate dispersion of miracidia of Schistosoma mansoni Sambon in outdoor habitats in St Lucia. J. Helminthol. 1972, 46, 297–306. [Google Scholar] [CrossRef]
- Jordan, P.; Woodstock, L.; Unrau, G.O.; Cook, J.A. Control of Schistosoma mansoni transmission by provision of domestic water supplies: A preliminary report of a study in St Lucia. Bull. World Health Organ 1975, 52, 9–20. [Google Scholar] [PubMed]
- Unrau, G.O. Individual household water supplies as a control measure against Schistosoma mansoni: A study in rural St Lucia. Bull. World Health Organ 1975, 52, 1–8. [Google Scholar]
- Jordan, P. Schistosomiasis—Research to control. Am. J. Trop. Med. Hyg. 1977, 26, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Jordan, P.; Barnish, G.; Bartholomew, R.K.; Grist, E.; Christie, J.D. Evaluation of an experimental mollusciding programme to control Schistosoma mansoni transmission in St Lucia. Bull. World Health Organ 1978, 56, 139–146. [Google Scholar] [PubMed]
- Jordan, P.; Bartholomew, R.K.; Unrau, G.O.; Upatham, E.S.; Grist, E.; Christie, J.D. Further observations from St Lucia on control of Schistosoma mansoni transmission by provision of domestic water supplies. Bull. World Health Organ 1978, 56, 965–973. [Google Scholar] [PubMed]
- Pointier, J.P. The introduction of Melanoides tuberculata (Mollusca: Thiaridae) to the island of Saint Lucia (West Indies) and its role in the decline of Biomphalaria glabrata, the snail intermediate host of Schistosoma mansoni. Acta Trop. 1993, 54, 13–18. [Google Scholar] [CrossRef]
- Kurup, R.; Hunjan, G.S. Intestinal parasites in St Lucia: A retrospective, laboratory-based study. J. Rural Trop. Public Health 2010, 9, 24–30. [Google Scholar]
- Kurup, R.; Hunjan, G.S. Epidemiology and control of schistosomiasis and other intestinal parasitic infections among children in three rural villages of south Saint Lucia. J. Vector Borne Dis. 2010, 47, 228–234. [Google Scholar] [PubMed]
- Paraense, W.L. The schistosome vectors in the Americas. Mem. Inst. Oswaldo Cruz 2001, 96, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Van Der Kuyp, E. Schistosomiasis in the Surinam District of Surinam. Trop. Geogr. Med. 1961, 13, 357–373. [Google Scholar]
- PAHO. Control and Elimination of Five Neglected Diseases in Latin America and the Caribbean, 2010–2015. Analysis of Progress, Priorities and Lines of Action for Lymphatic filariasis, Schistosomiasis, Onchocerciasis, Trachoma and Soil-Transmitted Helminthiases; Pan American Health Organization: Washington, DC, USA, 2010. [Google Scholar]
- Noya, O.; Katz, N.; Pointier, J.P.; Théron, A.; Alarcón de Noya, B. Schistosomiasis in America. In Neglected Tropical Diseases—Latin America and the Caribbean, Neglected Tropical Diseases; Franco-Paredes, C., Santos-Preciado, J.I., Eds.; Springer: Vienna, Austria, 2015; pp. 11–43. [Google Scholar]
- Van Der Kuyp, E. Schistosomiasis mansoni in the Saramacca District of Surinam. Trop. Geogr. Med. 1969, 21, 88–92. [Google Scholar]
- PAHO. Epidemiological Profiles of Neglected Diseases and Other Infections Related to Poverty in Latin America and the Caribbean; Pan American Health Organization: Washington, DC, USA, 2009. [Google Scholar]
- Alberda, A.; Weits, J.; Limburg, A.J.; Grond, J.; Ilic, P. Chronic schistosomiasis in Surinam subjects: Symptoms, treatment and course. Nederlands tijdschrift voor Geneeskunde 1987, 131, 2308–2312. [Google Scholar]
- WHO. WHO Technical Report Series 830, The Control of Schistosomiasis, Second Report of the WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Locketz, L. Health education in rural Surinam: Use of videotape in a national campaign against schistosomiasis. Bull. Pan Am. Health Organ 1976, 10, 219–226. [Google Scholar] [PubMed]
- Colston, J.; Saboyá, M. Soil-transmitted helminthiasis in Latin America and the Caribbean: Modelling the determinants, prevalence, population at risk and costs of control at sub-national level. Geospat. Health 2013, 7, 321–340. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Commerce. United States Census Bureau: Quick Facts Puerto Rico. Available online: https://www.census.gov/quickfacts/fact/table/pr/PST045218 (accessed on 15 January 2019).
- U.S. Central Intelligence Agency: World Factbook, Saint Martin. Available online: https://www.cia.gov/library/publications/the-world-factbook/geos/print_rn.html (accessed on 15 January 2019).
- PAHO. Health in the Americas. Available online: https://www.paho.org/salud-en-las-americas-2017/ (accessed on 15 January 2019).
- PAHO. Resolution CD49.R19 Elimination of Neglected Diseases and Other Poverty-Related Infections. In Proceedings of the 49th Directing Council, 61st Session of the Regional Committee, PAHO, Washington, DC, USA, 28 September–2 October 2009; Available online: http://iris.paho.org/xmlui/bitstream/handle/123456789/399/CD49.R19%20%28Eng.%29.pdf?sequence=1&isAllowed=y (accessed on 15 December 2018).
- WHO. Resolution WHA65.21 Elimination of Schistosomiasis. Agenda Item 13.11. In Proceedings of the Sixty-fifth World Health Assembly, Geneva, Switzerland, 26 May 2012; Available online: https://www.who.int/neglected_diseases/mediacentre/WHA_65.21_Eng.pdf (accessed on 10 December 2018).
- Chernin, E.; Michelson, E.H.; Augustine, D.L. Studies on the biological control of schistosome-bearing snails. I. The control of Australorbis glabratus populations by the snail, Marisa cornuarietis, under laboratory conditions. Am. J. Trop. Med. Hyg. 1956, 5, 297–307. [Google Scholar] [CrossRef]
- Gomez Perez, J.; Vargas, M.; Malek, E.A. Displacement of Biomphalaria glabrata by Thiara granifera under natural conditions in the Dominican Republic. Mem. Inst. Oswaldo Cruz 1991, 86, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Rijpstra, A.C.; Swellengrebel, N.H. Lateral-spined schistosome ova in a great anteater, Myrmecophaga tridactyla L. (Edentata) from Suriname. Trop. Geogr. Med. 1962, 14, 279–483. [Google Scholar] [PubMed]
- Combes, C.; Imbert-Establet, D. Infectivity in rodents of Schistosoma mansoni cercariae of human and murine origin. J. Helminthol. 1980, 54, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Combes, C.; Leger, N.; Golvan, Y.J. Rats et Bilharzia en Guadeloupe. Acta Trop. 1975, 32, 304–308. [Google Scholar]


{kind=link}
| Transmission Status. | Locality | Current Population 1 | Interventions/Natural Changes Impacting Transmission | Animal Reservoirs |
|---|---|---|---|---|
| Eliminated | Saint Martin | 32,284 (2018) | Deforestation Hydrological changes Climate change | |
| Saint Kitts | 34,918 (2011) | Hydrological Changes Water and sanitation improvement Mollusciciding Competitor snails (A) 3 | Monkeys 4 | |
| Vieques | 8669 (2017) | Mollusciciding Chemotherapy | ||
| Considered eliminated but not yet verified | Puerto Rico | 3,337,177 (2017) 2 | Water and sanitation improvement Chemotherapy (selective) Mollusciciding Competitor snails (A,B) 3 Health education | |
| Dominican Republic | 10,649,000 (2016) | Mollusciciding Health education Competitor snails (A,B,C) 3 Environmental management | ||
| Antigua | 90,755 (2015) | Hydrological changes Water and sanitation improvements Competitor snails (B,C) 3 | ||
| Montserrat | 5241 (2015) | Volcanic eruption Competitor snails (C) 3 | ||
| Guadeloupe | 402,119 (2013) | Chemotherapy (selective) Environmental management Competitor snails (A,C,D) 3 | Rats 5 | |
| Martinique | 385,551 (2013) | Water and sanitation improvements Health education Chemotherapy (selective) Competitor snails (B,C) 3 | ||
| Ongoing | Saint Lucia | 172,255 (2014) | Health education Water and sanitation improvements Chemotherapy (selective) Mollusciciding Competitor snails (C) 3 | |
| Suriname | 541,638 (2012) | Chemotherapy (selective) Mollusciciding Environmental management Water and sanitation improvements Agricultural practices Health education |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hewitt, R.; Willingham, A.L. Status of Schistosomiasis Elimination in the Caribbean Region. Trop. Med. Infect. Dis. 2019, 4, 24. https://doi.org/10.3390/tropicalmed4010024
Hewitt R, Willingham AL. Status of Schistosomiasis Elimination in the Caribbean Region. Tropical Medicine and Infectious Disease. 2019; 4(1):24. https://doi.org/10.3390/tropicalmed4010024
Chicago/Turabian StyleHewitt, Reynold, and Arve Lee Willingham. 2019. "Status of Schistosomiasis Elimination in the Caribbean Region" Tropical Medicine and Infectious Disease 4, no. 1: 24. https://doi.org/10.3390/tropicalmed4010024
APA StyleHewitt, R., & Willingham, A. L. (2019). Status of Schistosomiasis Elimination in the Caribbean Region. Tropical Medicine and Infectious Disease, 4(1), 24. https://doi.org/10.3390/tropicalmed4010024