Dengue Fever and Severe Dengue in Barbados, 2008–2016

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Sample Collection
2.3. Dengue Diagnosis
2.4. Virus Sequencing—Next Generation Sequencing (NGS)
2.5. Phylogenetic Analysis
2.6. Data Analysis
3. Results
3.1. Laboratory Testing and Clinical Symptoms
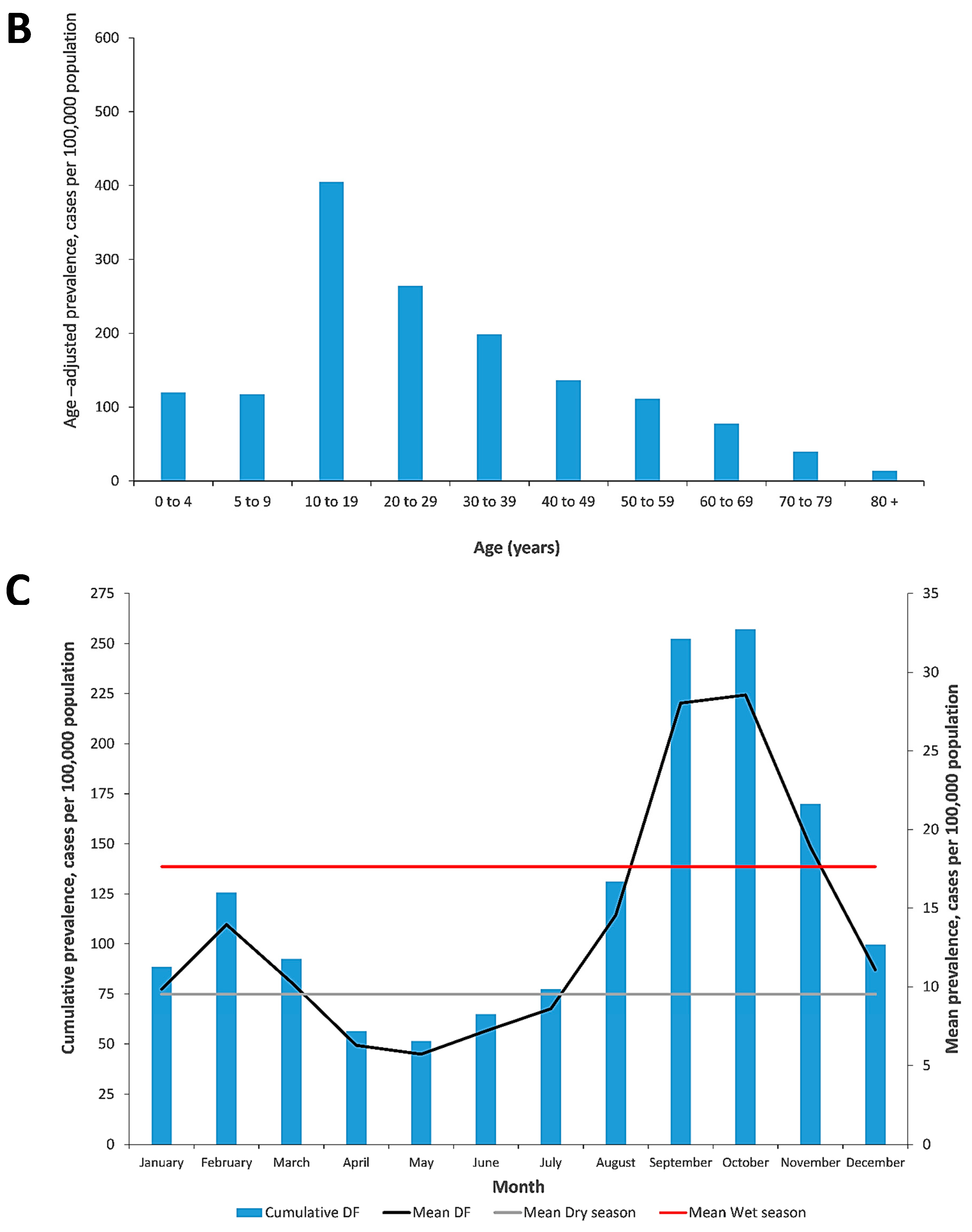
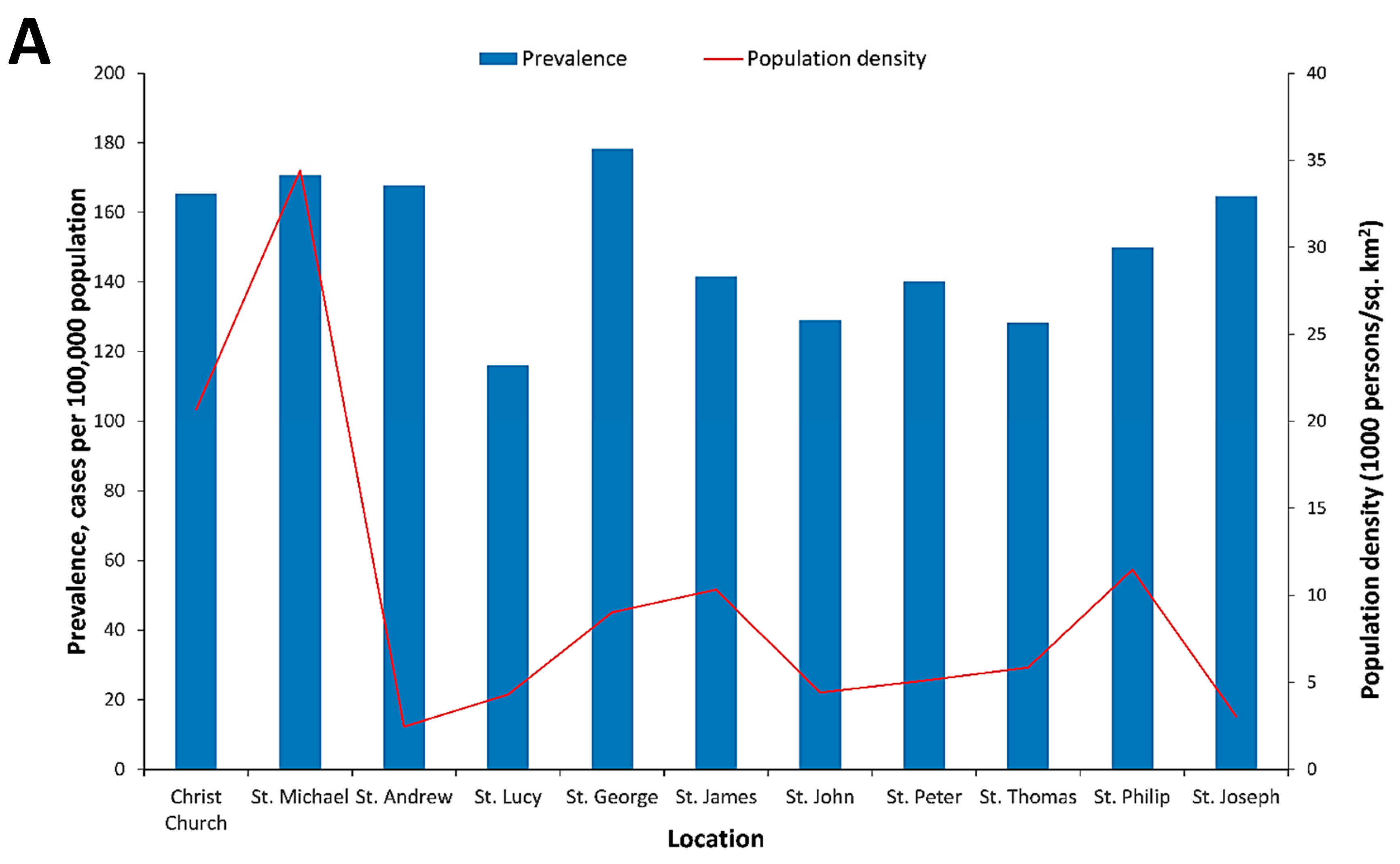
3.2. Epidemiological Patterns of Dengue in Barbados
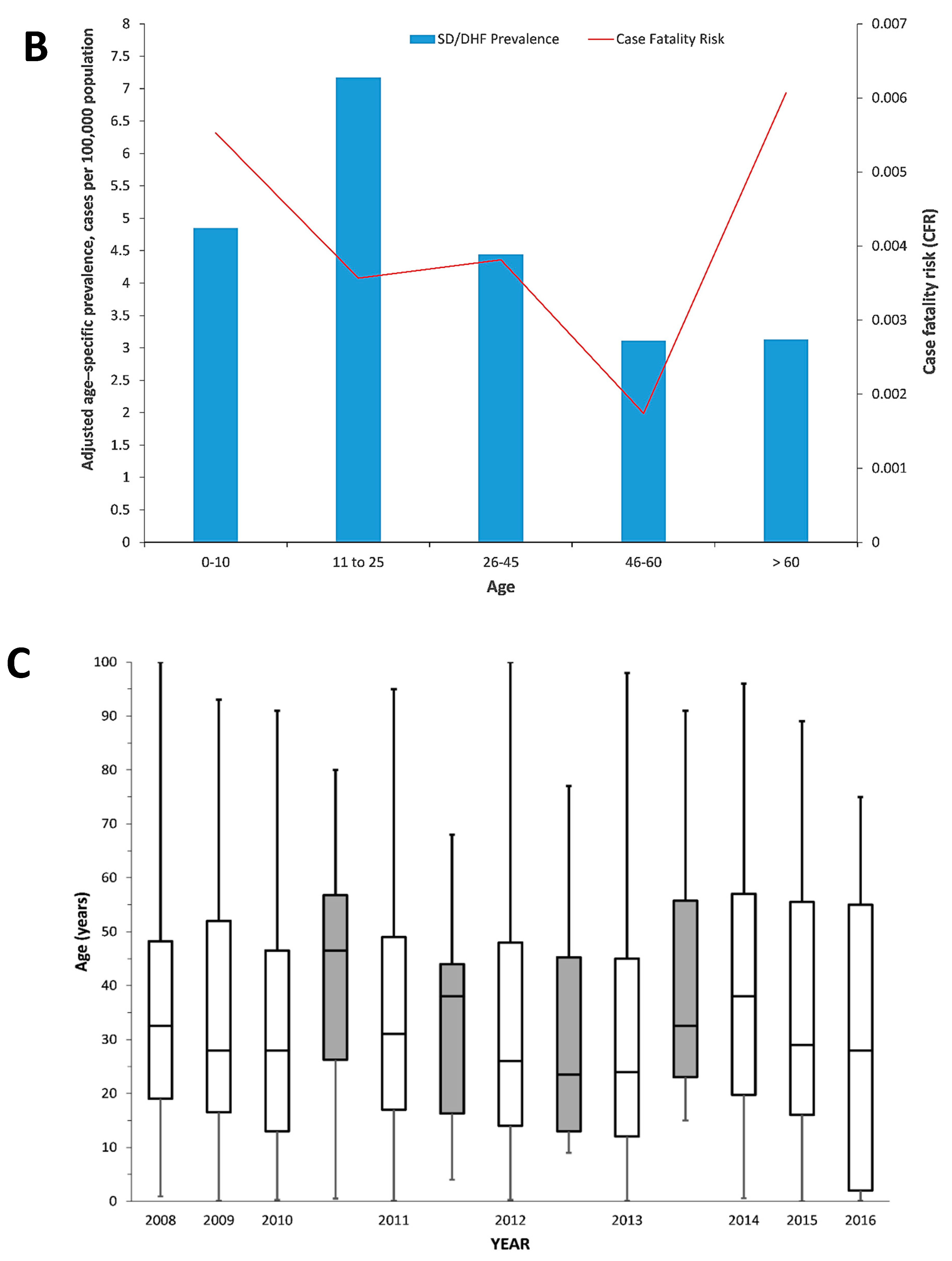
3.3. Severe Dengue in Barbados
3.4. DENV Sequencing in Dengue Patient Sera
4. Discussion
4.1. Seasonal Factors
4.2. Dengue and Gender
4.3. Dengue Disease Severity
4.4. Sequencing of DENV Envelope (E) Gene Region
4.5. Study Limitations
4.6. Future Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dick, O.B.; San Martín, J.L.; Montoya, R.H.; del Diego, J.; Zambrano, B.; Dayan, G.H. The history of dengue outbreaks in the Americas. Am. J. Trop. Med. Hyg. 2012, 87, 584–593. [Google Scholar] [CrossRef] [Green Version]
- Murray, N.E.A.; Quam, M.B.; Wilder-Smith, A. Epidemiology of dengue: Past, present and future prospects. Clin. Epidemiol. 2013, 5, 299–309. [Google Scholar] [CrossRef] [Green Version]
- Torres, J.R.; Orduna, T.A.; Piña-Pozas, M.; Vázquez-Vega, D.; Sarti, E. Epidemiological characteristics of dengue disease in Latin America and in the Caribbean: A systematic review of the literature. J. Trop. Med. 2017, 2017, 8045435. [Google Scholar] [CrossRef]
- Bellon, M.M.; MacLean, J.D. A point source dengue outbreak in Canadian tourists in Barbados. Can. Commun. Dis. Rep. 1998, 24, 161–164. [Google Scholar] [PubMed]
- Branch, S.L.; Levett, P.N. Evaluation of four methods for detection of immunoglobulin M antibodies to dengue virus. Clin. Diagn. Lab. Immunol. 1999, 6, 555–557. [Google Scholar] [CrossRef] [Green Version]
- Levett, P.N.; Branch, S.L.; Edwards, C.N. Detection of dengue infection in patients investigated for leptospirosis in Barbados. Am. J. Trop. Med. Hyg. 2000, 62, 112–114. [Google Scholar] [CrossRef] [Green Version]
- Gittens-St Hilaire, M.; Clarke-Greenidge, N. An analysis of the subtypes of dengue fever infections in Barbados 2003–2007 by reverse transcriptase polymerase chain reaction. Virol. J. 2008, 5, 152. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Gittens-St Hilaire, M.; Nielsen, A.L. Epidemiological trends and clinical manifestations of Dengue among children in one of the English-speaking Caribbean countries. Trans. R. Soc. Trop. Med. Hyg. 2013, 107, 254–260. [Google Scholar] [CrossRef]
- Kumar, A.; Gittens-St Hilaire, M.; Clarke-Greenidge, N.; Nielsen, A.L. Epidemiological Trend and Clinical Observations among Children and Adults with Dengue in Barbados. West Indian Med. J. 2015, 64, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Nielsen, A.L. Trends in the patterns of IgM and IgG antibodies in febrile persons with suspected dengue in Barbados, an English-speaking Caribbean country, 2006–2013. J. Infect. Public Health 2015, 8, 583–592. [Google Scholar] [CrossRef]
- Kumar, A.; Gittens-St Hilair, M.; Jason, V.; Ugwuagu, C.; Krishnamurthy, K. The clinical characteristics and outcome of children hospitalized with dengue in Barbados, an English Caribbean country. J. Infect. Dev. Ctries. 2015, 9, 394–401. [Google Scholar] [CrossRef]
- Chadee, D.; Mahabir, R.S.; Sutherland, J.M. Dengue Fever Epidemiology and Control in the Caribbean: A Status Report (2012). Carib. Med. J. 2012, 74, 17–21. [Google Scholar]
- Ahmad, O.; Boschi-Pinto, C.; Lopez, A.; Murray, C.; Lozano, R.; Inoue, M. Age Standardization of Rates: A New WHO Standard; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Groen, J.; Koraka, P.; Velzing, J.; Copra, C.; Osterhaus, A.D. Evaluation of six immunoassays for detection of dengue virus-specific immunoglobulin M and G antibodies. Clin. Diagn. Lab. Immunol. 2000, 7, 867–871. [Google Scholar] [CrossRef] [Green Version]
- Koraka, P.; Zeller, H.; Niedrig, M.; Osterhaus, A.D.; Groen, J. Reactivity of serum samples from patients with a flavivirus infection measured by immunofluorescence assay and ELISA. Microbes Infect. 2002, 4, 1209–1215. [Google Scholar] [CrossRef]
- Kumarasamy, V.; Wahab, A.A.; Chua, S.; Hassan, Z.; Mohamad, M.; Chua, K. Evaluation of a commercial dengue NS1 antigen-capture ELISA for laboratory diagnosis of acute dengue virus infection. J. Virol. Methods 2007, 140, 75–79. [Google Scholar] [CrossRef]
- Johnson, B.W.; Russell, B.J.; Lanciotti, R.S. Serotype-specific detection of dengue viruses in a fourplex real-time reverse transcriptase PCR assay. J. Clin. Microbiol. 2005, 43, 4977–4983. [Google Scholar] [CrossRef] [Green Version]
- Lahariya, C. Vaccine epidemiology: A review. J. Fam. Med. Prim. Care 2016, 5, 7. [Google Scholar] [CrossRef]
- Cafferata, M.L.; Bardach, A.; Rey-Ares, L.; Alcaraz, A.; Cormick, G.; Gibbons, L.; Romano, M.; Cesaroni, S.; Ruvinsky, S. Dengue epidemiology and burden of disease in Latin America and the Caribbean: A systematic review of the literature and meta-analysis. Value Health Reg. Issues 2013, 2, 347–356. [Google Scholar] [CrossRef] [Green Version]
- Gubler, D.J. Aedes aegypti and Aedes aegypti-borne disease control in the 1990s: Top down or bottom up. Am. J. Trop. Med. Hyg. 1989, 40, 571–578. [Google Scholar] [CrossRef]
- Hemme, R.R.; Tank, J.L.; Chadee, D.D.; Severson, D.W. Environmental conditions in water storage drums and influences on Aedes aegypti in Trinidad, West Indies. Acta Trop. 2009, 112, 59–66. [Google Scholar] [CrossRef] [Green Version]
- Getachew, D.; Tekie, H.; Gebre-Michael, T.; Balkew, M.; Mesfin, A. Breeding sites of Aedes aegypti: Potential dengue vectors in Dire Dawa, East Ethiopia. Interdiscip. Perspect. Infect. Dis. 2015, 2015, 706276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gubler, D.J. Dengue, urbanization and globalization: The unholy trinity of the 21st century. Trop. Med. Health 2011, 39 (Suppl. 4), S3–S11. [Google Scholar] [CrossRef] [Green Version]
- Shepard, D.S.; Coudeville, L.; Halasa, Y.A.; Zambrano, B.; Dayan, G.H. Economic impact of dengue illness in the Americas. Am. J. Trop. Med. Hyg. 2011, 84, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, G.L. Global dengue epidemiology trends. Rev. Inst. Med. Trop. Sao Paulo 2012, 54 (Suppl. 18), S5–S6. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Diagnosis, Treatment, Prevention and Control; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Lorenz, C.; Azevedo, T.S.; Chiaravalloti-Neto, F. COVID-19 and dengue fever: A dangerous combination for the health system in Brazil. Travel Med. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Joob, B.; Wiwanitkit, V. COVID-19 can present with a rash and be mistaken for Dengue. J. Am. Acad. Dermatol. 2020, 82, e177. [Google Scholar] [CrossRef]
- Yan, G.; Lee, C.K.; Lam, L.T.; Yan, B.; Chua, Y.X.; Lim, A.Y.; Phang, K.F.; Kew, G.S.; Teng, H.; Ngai, C.H. Covert COVID-19 and false-positive dengue serology in Singapore. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Saavedra-Velasco, M.; Chiara-Chilet, C.; Pichardo-Rodriguez, R.; Grandez-Urbina, A.; Inga-Berrospi, F. Coinfection between dengue and covid-19: Need for approach in endemic zones. Revista de la Facultad de Ciencias Medicas (Cordoba, Argentina) 2020, 77, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Castanha, P.; Cordeiro, M.; Martelli, C.; Souza, W.; Marques, E.; Braga, C. Force of infection of dengue serotypes in a population-based study in the northeast of Brazil. Epidemiol. Infect. 2013, 141, 1080–1088. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Barraquer, I.; Buathong, R.; Iamsirithaworn, S.; Nisalak, A.; Lessler, J.; Jarman, R.G.; Gibbons, R.V.; Cummings, D.A. Revisiting Rayong: Shifting seroprofiles of dengue in Thailand and their implications for transmission and control. Am. J. Epidemiol. 2014, 179, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Tam, C.C.; Tissera, H.; de Silva, A.M.; De Silva, A.D.; Margolis, H.S.; Amarasinge, A. Estimates of dengue force of infection in children in Colombo, Sri Lanka. PLoS Negl. Trop. Dis. 2013, 7, e2259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khampapongpane, B.; Lewis, H.C.; Ketmayoon, P.; Phonekeo, D.; Somoulay, V.; Khamsing, A.; Phengxay, M.; Sisouk, T.; Vongphrachanh, P.; Bryant, J.E. National dengue surveillance in the Lao People’s Democratic Republic, 2006–2012: Epidemiological and laboratory findings. West. Pac. Surveill. Response J. WPSAR 2014, 5, 7. [Google Scholar]
- Cummings, D.A.; Iamsirithaworn, S.; Lessler, J.T.; McDermott, A.; Prasanthong, R.; Nisalak, A.; Jarman, R.G.; Burke, D.S.; Gibbons, R.V. The impact of the demographic transition on dengue in Thailand: Insights from a statistical analysis and mathematical modeling. PLoS Med. 2009, 6, e1000139. [Google Scholar] [CrossRef] [Green Version]
- Thai, K.T.; Nishiura, H.; Hoang, P.L.; Tran, N.T.T.; Phan, G.T.; Le, H.Q.; Tran, B.Q.; Van Nguyen, N.; de Vries, P.J. Age-specificity of clinical dengue during primary and secondary infections. PLoS Negl. Trop. Dis. 2011, 5, e1180. [Google Scholar] [CrossRef] [PubMed]
- Prince, H.E.; Yeh, C.; Lapé-Nixon, M. Primary and probable secondary dengue virus (DV) infection rates in relation to age among DV IgM-positive patients residing in the United States mainland versus the Caribbean islands. Clin. Vaccine Immunol. 2012, 19, 105–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizumoto, K.; Ejima, K.; Yamamoto, T.; Nishiura, H. On the risk of severe dengue during secondary infection: A systematic review coupled with mathematical modeling. J. Vector Borne Dis. 2014, 51, 153. [Google Scholar] [PubMed]
- Morales, I.; Salje, H.; Saha, S.; Gurley, E.S. Seasonal Distribution and Climatic Correlates of Dengue Disease in Dhaka, Bangladesh. Am. J. Trop. Med. Hyg. 2016, 94, 1359–1361. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.; Tang, C.S.; McIver, L.; Hashizume, M.; Chan, V.; Abeyasinghe, R.R.; Iddings, S.; Huy, R. Effects of weather factors on dengue fever incidence and implications for interventions in Cambodia. BMC Public Health 2016, 16, 241. [Google Scholar] [CrossRef] [Green Version]
- Hii, Y.L.; Zaki, R.A.; Aghamohammadi, N.; Rocklöv, J. Research on Climate and Dengue in Malaysia: A Systematic Review. Curr. Environ. Health Rep. 2016, 3, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Bennett, S.N.; Drummond, A.J.; Kapan, D.D.; Suchard, M.A.; Munoz-Jordan, J.L.; Pybus, O.G.; Holmes, E.C.; Gubler, D.J. Epidemic dynamics revealed in dengue evolution. Mol. Biol. Evol. 2010, 27, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Johansson, M.A.; Cummings, D.A.; Glass, G.E. Multiyear climate variability and dengue—El Nino southern oscillation, weather, and dengue incidence in Puerto Rico, Mexico, and Thailand: A longitudinal data analysis. PLoS Med. 2009, 6, e1000168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, A.C.; Getis, A.; Santiago, M.; Rigau-Perez, J.G.; Reiter, P. Exploratory space-time analysis of reported dengue cases during an outbreak in Florida, Puerto Rico, 1991–1992. Am. J. Trop. Med. Hyg. 1998, 58, 287–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chadee, D.; Shivnauth, B.; Rawlins, S.; Chen, A. Climate, mosquito indices and the epidemiology of dengue fever in Trinidad (2002–2004). Ann. Trop. Med. Parasitol. 2007, 101, 69–77. [Google Scholar] [CrossRef]
- Depradine, C.; Lovell, E. Climatological variables and the incidence of Dengue fever in Barbados. Int. J. Environ. Health Res. 2004, 14, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Nagao, Y.; Thavara, U.; Chitnumsup, P.; Tawatsin, A.; Chansang, C.; Campbell-Lendrum, D. Climatic and social risk factors for Aedes infestation in rural Thailand. Trop. Med. Int. Health 2003, 8, 650–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcari, P.; Tapper, N.; Pfueller, S. Regional variability in relationships between climate and dengue/DHF in Indonesia. Singap. J. Trop. Geogr. 2007, 28, 251–272. [Google Scholar] [CrossRef]
- Banu, S.; Hu, W.; Hurst, C.; Tong, S. Dengue transmission in the Asia-Pacific region: Impact of climate change and socio-environmental factors. Trop. Med. Int. Health 2011, 16, 598–607. [Google Scholar] [CrossRef]
- Araujo, R.V.; Albertini, M.R.; Costa-da-Silva, A.L.; Suesdek, L.; Franceschi, N.C.S.; Bastos, N.M.; Katz, G.; Cardoso, V.A.; Castro, B.C.; Capurro, M.L. São Paulo urban heat islands have a higher incidence of dengue than other urban areas. Braz. J. Infect. Dis. 2015, 19, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, W.-P.; Suzuki, M.; Thiem, V.D.; White, R.G.; Tsuzuki, A.; Yoshida, L.-M.; Yanai, H.; Haque, U.; Anh, D.D.; Ariyoshi, K. Population density, water supply, and the risk of dengue fever in Vietnam: Cohort study and spatial analysis. PLoS Med. 2011, 8, e1001082. [Google Scholar] [CrossRef]
- Nonomura, A.; Kitahara, M.; Masuda, T. Impact of land use and land cover changes on the ambient temperature in a middle scale city, Takamatsu, in Southwest Japan. J. Environ. Manag. 2009, 90, 3297–3304. [Google Scholar] [CrossRef]
- Vanwambeke, S.O.; Bennett, S.N.; Kapan, D.D. Spatially disaggregated disease transmission risk: Land cover, land use and risk of dengue transmission on the island of Oahu. Trop. Med. Int. Health 2011, 16, 174–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zellweger, R.M.; Cano, J.; Mangeas, M.; Taglioni, F.; Mercier, A.; Despinoy, M.; Menkès, C.E.; Dupont-Rouzeyrol, M.; Nikolay, B.; Teurlai, M. Socioeconomic and environmental determinants of dengue transmission in an urban setting: An ecological study in Nouméa, New Caledonia. PLoS Negl. Trop. Dis. 2017, 11, e0005471. [Google Scholar] [CrossRef] [PubMed]
- Anker, M.; Arima, Y. Male-female differences in the number of reported incident dengue fever cases in six Asian countries. West. Pac. Surveill. Response J. WPSAR 2011, 2, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Yew, Y.W.; Ye, T.; Ang, L.W.; Ng, L.C.; Yap, G.; James, L.; Chew, S.K.; Goh, K.T. Seroepidemiology of dengue virus infection among adults in Singapore. Ann. Acad. Med. Singap. 2009, 38, 667–675. [Google Scholar] [PubMed]
- Kaplan, J.E.; Eliason, D.A.; Moore, M.; Sather, G.E.; Schonberger, L.B.; Cabrera-Coello, L.; Fernandez de Castro, J. Epidemiologic investigations of dengue infection in Mexico, 1980. Am. J. Epidemiol. 1983, 117, 335–343. [Google Scholar] [CrossRef]
- Lin, C.C.; Huang, Y.H.; Shu, P.Y.; Wu, H.S.; Lin, Y.S.; Yeh, T.M.; Liu, H.S.; Liu, C.C.; Lei, H.Y. Characteristic of dengue disease in Taiwan: 2002–2007. Am. J. Trop. Med. Hyg. 2010, 82, 731–739. [Google Scholar] [CrossRef] [Green Version]
- Da Rosa, A.T.; Vasconcelos, P.; Da Rosa, E.T.; Rodrigues, S.G.; Mondet, B.; Cruz, A.; Sousa, M.R.; Da Rosa, J.T. Dengue epidemic in Belém, Pará, Brazil, 1996–1997. Emerg. Infect. Dis. 2000, 6, 298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ooi, E.E. Changing pattern of dengue transmission in Singapore. Dengue Bull. 2001, 25, 40–44. [Google Scholar]
- Halstead, S.B. Dengue in the Americas and Southeast Asia: Do they differ? Revista Panamericana de Salud Publica 2006, 20, 407–415. [Google Scholar] [CrossRef]
- Case Fatality Rates of Dengue Fever and Dengue Haemorrhagic Fever (DF/DHF) in the Western Pacific Region, 2000–2010; World Health Organization: Geneva, Switzerland, 2011.
- Bravo, L.; Roque, V.G.; Brett, J.; Dizon, R.; L’Azou, M. Epidemiology of dengue disease in the Philippines (2000–2011): A systematic literature review. PLoS Negl. Trop. Dis. 2014, 8, e3027. [Google Scholar] [CrossRef] [Green Version]
- Karyanti, M.R.; Uiterwaal, C.S.; Kusriastuti, R.; Hadinegoro, S.R.; Rovers, M.M.; Heesterbeek, H.; Hoes, A.W.; Bruijning-Verhagen, P. The changing incidence of dengue haemorrhagic fever in Indonesia: A 45-year registry-based analysis. BMC Infect. Dis. 2014, 14, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, M.G.; Costa, M.C.; Coelho, G.; Barreto, M.L. Recent shift in age pattern of dengue hemorrhagic fever, Brazil. Emerg. Infect. Dis. 2008, 14, 1663. [Google Scholar] [CrossRef] [PubMed]
- Huy, R.; Buchy, P.; Conan, A.; Ngan, C.; Ong, S.; Ali, R.; Duong, V.; Yit, S.; Ung, S.; Te, V. National dengue surveillance in Cambodia 1980–2008: Epidemiological and virological trends and the impact of vector control. Bull. World Health Organ. 2010, 88, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Ooi, E.-E.; Goh, K.-T.; Gubler, D.J. Dengue prevention and 35 years of vector control in Singapore. Emerg. Infect. Dis. 2006, 12, 887. [Google Scholar] [CrossRef] [PubMed]
- Dengue and Dengue Haemorrhagic Fever Fact Sheet No. 117; World Health Organization: Geneva, Switzerland, March 2009; Available online: http://www.who.int/mediacentre/factsheets/fs117/en/ (accessed on 6 April 2011).
- Kularatne, S.; Seneviratne, S.; Malavige, G.; Fernando, S.; Velathanthiri, V.; Ranatunga, P.; Wijewickrama, E.; Gurugama, P.; Karunatilaka, D.; Aaskov, J. Synopsis of findings from recent studies on dengue in Sri Lanka. Dengue Bull. 2006, 30, 80. [Google Scholar]
- Setiatia, T.E.; Wagenaarb, J.F.; de Kruifb, M.D.; Mairuhub, A.T.; van Gorpb, E.C.; Soemantria, A. Changing Epidemiology of Dengue Haemorrhagic Fever in Indonesia. Dengue Bull. 2006, 30, 1. [Google Scholar]
- Sharp, T.M.; Tomashek, K.M.; Read, J.S.; Margolis, H.S.; Waterman, S.H. A New Look at an Old Disease: Recent Insights into the Global Epidemiology of Dengue. Curr. Epidemiol. Rep. 2017, 4, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Stanaway, J.D.; Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Coffeng, L.E.; Brady, O.J.; Hay, S.I.; Bedi, N.; Bensenor, I.M.; Castañeda-Orjuela, C.A. The global burden of dengue: An analysis from the Global Burden of Disease Study 2013. Lancet Infect. Dis. 2016, 16, 712–723. [Google Scholar] [CrossRef] [Green Version]
- Tomashek, K.M.; Gregory, C.J.; Sánchez, A.R.; Bartek, M.A.; Rivera, E.J.G.; Hunsperger, E.; Muñoz-Jordán, J.L.; Sun, W. Dengue deaths in Puerto Rico: Lessons learned from the 2007 epidemic. PLoS Negl. Trop. Dis. 2012, 6, e1614. [Google Scholar] [CrossRef]
- Leo, Y.-S.; Thein, T.L.; Fisher, D.A.; Low, J.G.; Oh, H.M.; Narayanan, R.L.; Gan, V.C.; Lee, V.J.; Lye, D.C. Confirmed adult dengue deaths in Singapore: 5-year multi-center retrospective study. BMC Infect. Dis. 2011, 11, 123. [Google Scholar] [CrossRef] [Green Version]
- Tomashek, K.M.; Rivera, A.; Torres-Velasquez, B.; Hunsperger, E.A.; Munoz-Jordan, J.L.; Sharp, T.M.; Rivera, I.; Sanabria, D.; Blau, D.M.; Galloway, R. Enhanced Surveillance for Fatal Dengue-Like Acute Febrile Illness in Puerto Rico, 2010–2012. PLoS Negl. Trop. Dis. 2016, 10, e0005025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Góes Cavalcanti, L.P.; de Melo Braga, D.N.; da Silva, L.M.A.; Aguiar, M.G.; Castiglioni, M.; Silva-Junior, J.U.; de Carvalho Araújo, F.M.; da Costa Pereira, R.A.; Malta, D.L.; de Lima Pompeu, M.M. Postmortem diagnosis of dengue as an epidemiological surveillance tool. Am. J. Trop. Med. Hyg. 2016, 94, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legrand, L.F.; Hotta, H.; Hotta, S.; Homma, M. Antibody-mediated enhancement of infection by dengue virus of the P815 murine mastocytoma cell line. Biken J. 1986, 29, 51–55. [Google Scholar] [PubMed]
- Guzman, M.G.; Vazquez, S. The complexity of antibody-dependent enhancement of dengue virus infection. Viruses 2010, 2, 2649–2662. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Roche, R.; Sanchez, L.; Burgher, Y.; Rosario, D.; Alvarez, M.; Kouri, G.; Halstead, S.B.; Gould, E.A.; Guzman, M.G. Virus role during intraepidemic increase in dengue disease severity. Vector Borne Zoonotic Dis. 2011, 11, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Tajima, S.; Nakayama, E.; Kotaki, A.; Moi, M.L.; Ikeda, M.; Yagasaki, K.; Saito, Y.; Shibasaki, K.-I.; Saijo, M.; Takasaki, T. Whole genome sequencing–based molecular epidemiologic analysis of autochthonous dengue virus type 1 strains circulating in Japan in 2014. Jpn. J. Infect. Dis. 2016. [Google Scholar] [CrossRef]
- Cruz, C.D.; Torre, A.; Troncos, G.; Lambrechts, L.; Leguia, M. Targeted full-genome amplification and sequencing of dengue virus types 1–4 from South America. J. Virol. Methods 2016, 235, 158–167. [Google Scholar] [CrossRef]
- Rodriguez-Roche, R.; Blanc, H.; Bordería, A.V.; Díaz, G.; Henningsson, R.; Gonzalez, D.; Santana, E.; Alvarez, M.; Castro, O.; Fontes, M. Increasing clinical severity during a dengue virus type 3 Cuban epidemic: Deep sequencing of evolving viral populations. J. Virol. 2016, 90, 4320–4333. [Google Scholar] [CrossRef] [Green Version]
- Dos Passos Cunha, M.; Guimarães, V.N.; Souza, M.; de Paula Cardoso, D.D.D.; de Almeida, T.N.V.; de Oliveira, T.S.; Fiaccadori, F.S. Phylodynamics of DENV-1 reveals the spatiotemporal co-circulation of two distinct lineages in 2013 and multiple introductions of dengue virus in Goiás, Brazil. Infect. Genet. Evol. 2016, 43, 130–134. [Google Scholar] [CrossRef]
- Allicock, O.M.; Lemey, P.; Tatem, A.J.; Pybus, O.G.; Bennett, S.N.; Mueller, B.A.; Suchard, M.A.; Foster, J.E.; Rambaut, A.; Carrington, C.V. Phylogeography and population dynamics of dengue viruses in the Americas. Mol. Biol. Evol. 2012, 29, 1533–1543. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Vasilakis, N. Dengue—Quo tu et quo vadis? Viruses 2011, 3, 1562–1608. [Google Scholar] [CrossRef] [PubMed]
- Chien, Y.-W.; Liu, Z.-H.; Tseng, F.-C.; Ho, T.-C.; Guo, H.-R.; Ko, N.-Y.; Ko, W.-C.; Perng, G.C. Prolonged persistence of IgM against dengue virus detected by commonly used commercial assays. BMC Infect. Dis. 2018, 18, 156. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | No. of Cases | Males | Females | DENV Serotypes | No. of SD/DHF Cases | No. of Deaths | Diagnostic Testing | ||
|---|---|---|---|---|---|---|---|---|---|
| ELISA IgM | NS1 | rRT–PCR | |||||||
| 2008 | 147 | 70 | 77 | n/a | 0 | 0 | 147 | – | – |
| 2009 | 76 | 35 | 40 | 3 | 3 | 0 | 76 | – | – |
| 2010 | 542 | 265 | 275 | 1,2 *,3,4 | 33 | 3 | 491 | 55 | 5 |
| 2011 | 217 | 103 | 114 | 1,2 *,4 | 9 | 5 | 206 | 16 | 11 |
| 2012 | 464 | 218 | 245 | 1 *,2,4 | 13 | 2 | 428 | 85 | 78 |
| 2013 | 1260 | 594 | 665 | 1 *,2,4 | 5 | 0 | 947 | 375 | 143 |
| 2014 | 523 | 248 | 274 | n/a | 0 | 0 | 521 | 14 | – |
| 2015 | 123 | 72 | 52 | n/a | 0 | 0 | 124 | 4 | – |
| 2016 | 642 | 406 | 227 | n/a | 0 | 0 | 642 | 3 | 23 |
| TOTAL | 3994 | 2011 | 1969 | 63 | 10 | 3582 | 548 | 237 | |
| Symptoms | No. of Patients | Frequency (%) |
|---|---|---|
| Fever | 3702 | 92.7 |
| Headache | 2471 | 61.9 |
| Joint pain | 2103 | 52.7 |
| Eye pain | 1655 | 41.4 |
| Muscle pain | 1533 | 38.4 |
| Gastrointestinal related symptoms * | 1163 | 29.1 |
| Rash | 981 | 24.6 |
| Anorexia | 846 | 21.2 |
| Bleeding | 467 | 11.7 |
| Respiratory symptoms | 308 | 7.7 |
| Thrombocytopenia | 256 | 6.4 |
| Jaundice | 179 | 4.5 |
| Lethargy | 89 | 2.2 |
| Cough | 82 | 2.1 |
| Hepatomegaly | 52 | 1.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Douglas, K.O.; Dutta, S.K.; Martina, B.; Anfasa, F.; Samuels, T.A.; Gittens-St. Hilaire, M. Dengue Fever and Severe Dengue in Barbados, 2008–2016. Trop. Med. Infect. Dis. 2020, 5, 68. https://doi.org/10.3390/tropicalmed5020068
Douglas KO, Dutta SK, Martina B, Anfasa F, Samuels TA, Gittens-St. Hilaire M. Dengue Fever and Severe Dengue in Barbados, 2008–2016. Tropical Medicine and Infectious Disease. 2020; 5(2):68. https://doi.org/10.3390/tropicalmed5020068
Chicago/Turabian StyleDouglas, Kirk Osmond, Sudip Kumar Dutta, Byron Martina, Fatih Anfasa, T. Alafia Samuels, and Marquita Gittens-St. Hilaire. 2020. "Dengue Fever and Severe Dengue in Barbados, 2008–2016" Tropical Medicine and Infectious Disease 5, no. 2: 68. https://doi.org/10.3390/tropicalmed5020068
APA StyleDouglas, K. O., Dutta, S. K., Martina, B., Anfasa, F., Samuels, T. A., & Gittens-St. Hilaire, M. (2020). Dengue Fever and Severe Dengue in Barbados, 2008–2016. Tropical Medicine and Infectious Disease, 5(2), 68. https://doi.org/10.3390/tropicalmed5020068