A Systematic Review of Human Infections by Pseudomonas mendocina


Abstract
:1. Introduction
2. Methods
2.1. Data Search
2.2. Study Selection
2.3. Study Outcomes
2.4. Data Extraction and Definitions
3. Results
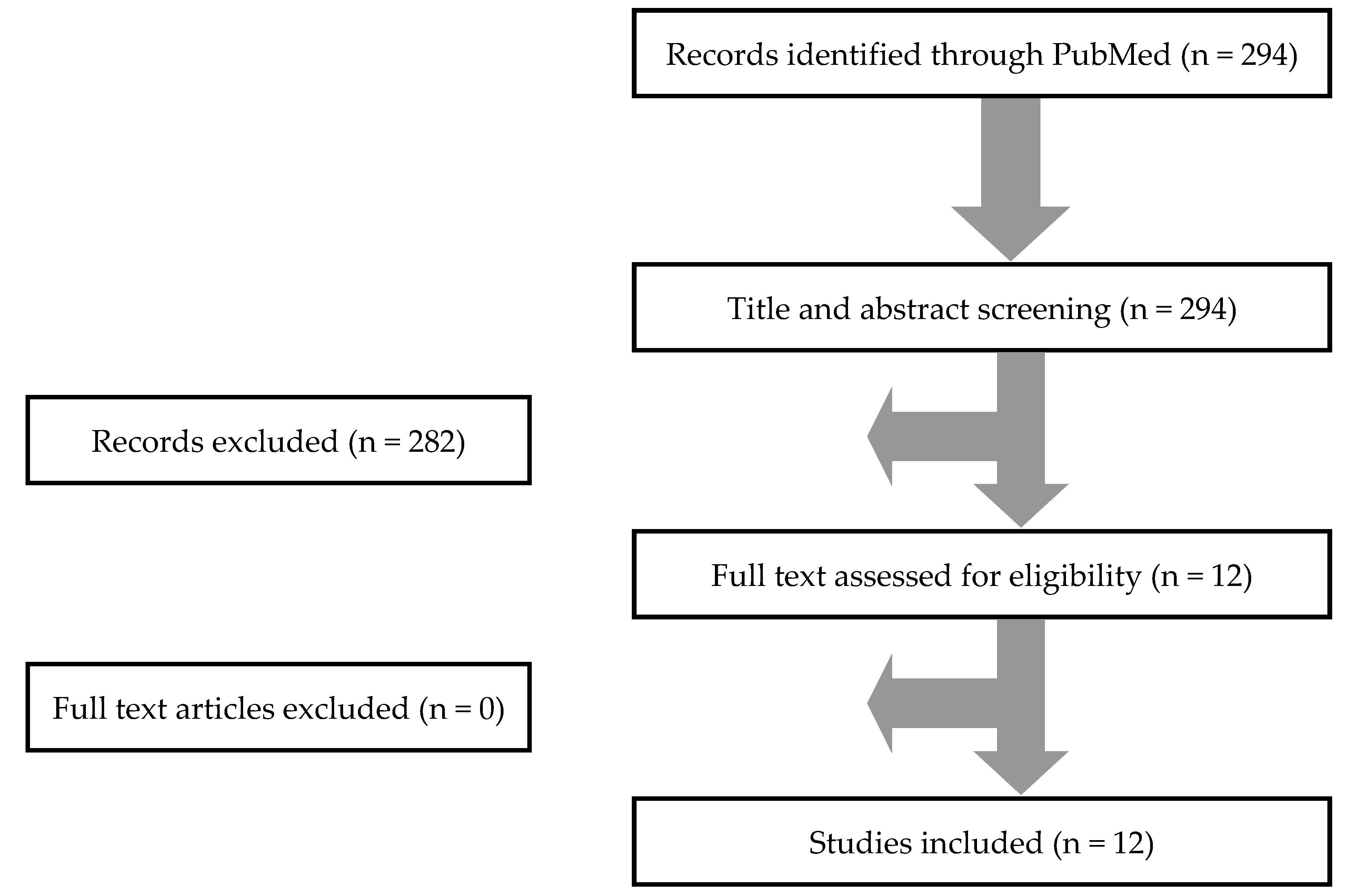
3.1. Literature Search
3.2. Included Studies’ Characteristics
3.3. Epidemiology, Microbiology, Treatment and Outcomes of P. mendocina Infections
3.4. Infective Endocarditis
3.5. CNS Infections
3.6. Miscellaneous Infections
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Palleroni, N.J.; Doudoroff, M.; Stanier, R.Y.; Solánes, R.E.; Mandel, M. Taxonomy of the aerobic pseudomonads: The properties of the Pseudomonas stutzeri group. J. Gen. Microbiol. 1970, 60, 215–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.R.; Lien, C.Y.; Tsai, W.C.; Lai, W.A.; Hsu, C.W.; Tsai, N.W.; Chang, C.C.; Lu, C.H.; Chien, C.C.; Chang, W.N. The clinical characteristics of adult bacterial meningitis caused by non-Pseudomonas (Ps.) aeruginosa Pseudomonas species: A clinical comparison with Ps. aeruginosa meningitis. Kaohsiung J. Med. Sci. 2018, 34, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Mert, A.; Yilmaz, M.; Ozaras, R.; Kocak, F.; Dagsali, S. Native valve endocarditis due to Pseudomonas mendocina in a patient with mental retardation and a review of literature. Scand. J. Infect. Dis. 2007, 39, 615–616. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269, W64. [Google Scholar] [CrossRef] [Green Version]
- Wallace, B.C.; Small, K.; Brodley, C.E.; Lau, J.; Trikalinos, T.A. Deploying an interactive machine learning system in an evidence-based practice center: Abstrackr. Proc. ACM Int. Health Inform. Symp. IHI 2012, 819–824. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Aragone, M.R.; Maurizi, D.M.; Clara, L.O.; Navarro Estrada, J.L.; Ascione, A. Pseudomonas mendocina, an environmental bacterium isolated from a patient with human infective endocarditis. J. Clin. Microbiol. 1992, 30, 1583–1584. [Google Scholar] [CrossRef] [Green Version]
- Johansen, H.K.; Kjeldsen, K.; Høiby, N. Pseudomonas mendocina as a cause of chronic infective endocarditis in a patient with situs inversus. Clin. Microbiol. Infect. 2001, 7, 650–652. [Google Scholar] [CrossRef] [Green Version]
- Rapsinski, G.J.; Makadia, J.; Bhanot, N.; Min, Z. Pseudomonas mendocina native valve infective endocarditis: A case report. J. Med. Case Rep. 2016, 10, 275. [Google Scholar] [CrossRef] [Green Version]
- Gani, M.; Rao, S.; Miller, M.; Scoular, S. Pseudomonas Mendocina Bacteremia: A Case Study and Review of Literature. Am. J. Case Rep. 2019, 20, 453–458. [Google Scholar] [CrossRef]
- Nseir, W.; Taha, H.; Abid, A.; Khateeb, J. Pseudomonas mendocina sepsis in a healthy man. ISR Med. Assoc. J. 2011, 13, 375–376. [Google Scholar] [PubMed]
- Almuzara, M.; Montaña, S.; Carulla, M.; Sly, G.; Fernandez, J.; Hernandez, M.; Moriano, A.; Traglia, G.M.; Bakai, R.; Ramirez, M.S. Clinical cases of VIM-producing Pseudomonas mendocina from two burned patients. J. Glob Antimicrob. Resist. 2018, 14, 273–274. [Google Scholar] [CrossRef] [PubMed]
- Chiu, L.Q.; Wang, W. A case of unusual Gram-negative bacilli septic arthritis in an immunocompetent patient. Singapore Med. J. 2013, 54, e164–e168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howe, T.S.; Ehrlich, G.D.; Koh, J.S.; Ng, A.C.; Costerton, W. A case of an atypical femoral fracture associated with bacterial biofilm--pathogen or bystander? Osteoporos. Int. 2013, 24, 1765–1766. [Google Scholar] [CrossRef]
- Chi, C.Y.; Lai, C.H.; Fung, C.P.; Wang, J.H. Pseudomonas mendocina spondylodiscitis: A case report and literature review. Scand. J. Infect. Dis. 2005, 37, 950–953. [Google Scholar] [CrossRef]
- Jerónimo, T.M.; Guedes, A.M.; Stieglmair, S.; Guerreiro, R.; Laranjo, C.; Bernardo, I.; Neves, P.L. Pseudomonas mendocina: The first case of peritonitis on peritoneal dialysis. Nefrologia 2017, 37, 647–649. [Google Scholar] [CrossRef]
- Sievert, D.M.; Ricks, P.; Edwards, J.R.; Schneider, A.; Patel, J.; Srinivasan, A.; Kallen, A.; Limbago, B.; Fridkin, S. National Healthcare Safety Network (NHSN) Team and Participating NHSN Facilities. Antimicrobial-resistant pathogens associated with healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect. Control Hosp. Epidemiol. 2013, 34, 1–14. [Google Scholar]
- Papakonstantinou, P.E.; Samonis, G.; Andrianaki, A.M.; Christofaki, M.; Dimopoulou, D.; Papadakis, J.; Gikas, A.; Kofteridis, D.P. Epidemiology, Microbiological and Clinical Features, Treatment, and Outcomes of Infective Endocarditis in Crete, Greece. Infect. Chemother. 2018, 50, 21–28. [Google Scholar] [CrossRef]
- Giannitsioti, E.; Skiadas, I.; Antoniadou, A.; Tsiodras, S.; Kanavos, K.; Triantafyllidi, H.; Giamarellou, H. Hellenic Endocarditis Study Group. Nosocomial vs. community-acquired infective endocarditis in Greece: Changing epidemiological profile and mortality risk. Clin. Microbiol. Infect. 2007, 13, 763–769. [Google Scholar] [CrossRef] [Green Version]
- El Bcheraoui, C.; Mokdad, A.H.; Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; Shirude, S.; Naghavi, M.; Murray, C.J.L. Trends and Patterns of Differences in Infectious Disease Mortality Among US Counties, 1980–2014. JAMA 2018, 319, 1248–1260. [Google Scholar] [CrossRef]
- Tzanakaki, G.; Mastrantonio, P. Aetiology of bacterial meningitis and resistance to antibiotics of causative pathogens in Europe and in the Mediterranean region. Int. J. Antimicrob. Agents 2007, 29, 621–629. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Value |
|---|---|
| Male, n (%) | 12 out of 16 (75%) |
| Age, mean (+/− SD) in years | 53.5 (19.9) |
| Medical History | |
| HIV infection, n (%) | 1 out of 16 (6.3%) |
| Central venous catheter, n (%) | 1 out of 16 (6.3%) |
| Previous antibiotic use, n (%) | 1 out of 16 (6.3%) |
| No known predisposing factors, n (%) | 7 out of 16 (43.8%) |
| Site of Infection | |
| Infective endocarditis, n (%) | 4 out of 16 (25%) |
| Central nervous system infection, n (%) | 4 out of 16 (25%) |
| Skin and soft tissue infections, n (%) | 3 out of 16 (18.8%) |
| Bacteremia (without endocarditis), n (%) | 2 out of 16 (12.5%) |
| Musculoskeletal infections, n (%) | 2 out of 16 (12.5%) |
| Peritoneal dialysis-associated peritonitis, n (%) | 1 out of 16 (6.3%) |
| Data on Infection | |
| Presence of fever, n (%) | 7 out of 10 (70%) |
| Presence of sepsis, n (%) | 4 out of 9 (44.4%) |
| Antimicrobial Resistance | |
| Ampicillin resistance, n (%) | 4 out of 5 (80%) |
| Co-trimoxazole resistance, n (%) | 1 out of 3 (33.3%) |
| Carbapenem resistance, n (%) | 1 out of 10 (10%) |
| Third or fourth generation cephalosporin resistance, n (%) | 0 out of 11 (0%) |
| Aminoglycoside resistance, n (%) | 0 out of 10 (0%) |
| Quinolone resistance, n (%) | 0 out of 7 (0%) |
| Piperacillin–tazobactam resistance, n (%) | 0 out of 6 (0%) |
| Colistin resistance, n (%) | 0 out of 1 (0%) |
| Treatment of P. mendocina IE | |
| Third or fourth generation cephalosporins, n (%) | 8 out of 15 (53.3%) |
| Quinolones, n (%) | 5 out of 15 (33.3%) |
| Aminoglycosides, n (%) | 3 out of 15 (20%) |
| Carbapenems, n (%) | 2 out of 15 (13.3%) |
| Colistin, n (%) | 2 out of 15 (13.3%) |
| Piperacillin–tazobactam, n (%) | 1 out of 15 (6.7%) |
| Aminopenicillins, n (%) | 1 out of 15 (6.7%) |
| Co-trimoxazole, n (%) | 1 out of 15 (6.7%) |
| Outcome | |
| Clinical cure, n (%) | 14 out of 15 (93.3%) |
| Deaths due to the infection, n (%) | 0 out of 15 (0%) |
| Deaths overall, n (%) | 1 out of 15 (6.7%) |
| Characteristic | Value |
|---|---|
| Male, n (%) | 3 out of 4 (75%) |
| Age, mean (+/− SD) in years | 46 (16.7) |
| Medical History | |
| Previous cardiac surgery, n (%) | 2 out of 4 (50%) |
| Prosthetic cardiac valve, n (%) | 1 out of 4 (25%) |
| No known predisposing factors, n (%) | 3 out of 4 (75%) |
| Concomitant bacteremia, n (%) | 4 out of 4 (100%) |
| Data on Infection | |
| Duration of symptoms, median (IQR) in days | 7 (5–45) |
| Patients with fever, n (%) | 4 out of 4 (100%) |
| Patients with sepsis, n (%) | 2 out of 3 (66.7%) |
| Antimicrobial Resistance | |
| Ampicillin resistance, n (%) | 3 out of 4 (75%) |
| Aminoglycoside resistance, n (%) | 0 out of 4 (0%) |
| Third or fourth generation cephalosporin resistance, n (%) | 0 out of 3 (0%) |
| Piperacillin–tazobactam resistance, n (%) | 0 out of 3 (0%) |
| Quinolone resistance, n (%) | 0 out of 3 (10) |
| Carbapenem resistance, n (%) | 0 out of 2 (0%) |
| Co-trimoxazole resistance, n (%) | 0 out of 1 (0%) |
| Colistin resistance, n (%) | 0 out of 1 (0%) |
| Treatment of P. mendocina Infections | |
| Third or fourth generation cephalosporin, n (%) | 2 out of 4 (50%) |
| Quinolones, n (%) | 2 out of 4 (50%) |
| Aminoglycoside, n (%) | 2 out of 4 (50%) |
| Piperacillin–tazobactam, n (%) | 1 out of 4 (25%) |
| Carbapenems, n (%) | 1 out of 4 (25%) |
| Surgical management, n (%) | 2 out of 4 (50%) |
| Duration of treatment, median (IQR) in days | 49 (42–82.3) |
| Outcome | |
| Clinical cure, n (%) | 4 out of 4 (100%) |
| Deaths due to the infection, n (%) | 0 out of 4 (0%) |
| Deaths overall, n (%) | 0 out of 4 (0%) |
| Characteristic | Value |
|---|---|
| Male, n (%) | 2 out of 4 (50%) |
| Age, mean (+/− SD) in years | 69.5 (11.3) |
| Medical History | |
| Community acquired infection, n (%) | 2 out of 4 (50%) |
| Hospital acquired infection, n (%) | 2 out of 4 (50%) |
| No known predisposing factors, n (%) | 2 out of 4 (50%) |
| Treatment of P. mendocina CNS Infection | |
| Third or fourth generation cephalosporins, n (%) | 3 out of 4 (75%) |
| Carbapenems, n (%) | 1 out of 4 (25%) |
| Outcome | |
| Clinical cure, n (%) | 4 out of 4 (100%) |
| Deaths due to the infection, n (%) | 0 out of 4 (0%) |
| Deaths overall, n (%) | 0 out of 4 (0%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioannou, P.; Vougiouklakis, G. A Systematic Review of Human Infections by Pseudomonas mendocina. Trop. Med. Infect. Dis. 2020, 5, 71. https://doi.org/10.3390/tropicalmed5020071
Ioannou P, Vougiouklakis G. A Systematic Review of Human Infections by Pseudomonas mendocina. Tropical Medicine and Infectious Disease. 2020; 5(2):71. https://doi.org/10.3390/tropicalmed5020071
Chicago/Turabian StyleIoannou, Petros, and Georgios Vougiouklakis. 2020. "A Systematic Review of Human Infections by Pseudomonas mendocina" Tropical Medicine and Infectious Disease 5, no. 2: 71. https://doi.org/10.3390/tropicalmed5020071
APA StyleIoannou, P., & Vougiouklakis, G. (2020). A Systematic Review of Human Infections by Pseudomonas mendocina. Tropical Medicine and Infectious Disease, 5(2), 71. https://doi.org/10.3390/tropicalmed5020071