Comparison of Latent Tuberculosis Infections among General versus Tuberculosis Health Care Workers in Myanmar

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Ethics Approval
2.3. Study Participants and Methods
2.4. Questionnaire Preparation
2.5. Data Collection
2.6. Variables and Measurements
2.7. Statistical Analysis
3. Results
3.1. Background Characteristics of HCWs
3.2. Prevalence of LTBI and Associated Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kompala, T.; Shenoi, S.V.; Friedland, G. Transmission of Tuberculosis in Resource-limited Settings. Curr. HIV/AIDS Rep. 2013, 10, 264–272. [Google Scholar]
- Al-Orainey, I.O. Diagnosis of latent tuberculosis: Can we do better? Ann. Thorac. Med. 2009, 4, 5–9. [Google Scholar]
- Gill, J.; Prasad, V. Testing Healthcare Workers for Latent Tuberculosis: Is It Evidence Based, Bio-Plausible, Both, Or Neither? Am. J. Med. 2019, 132, 1260–1261. [Google Scholar]
- Almufty, H.B.; Abdulrahman, I.S.; Merza, M.A. Latent Tuberculosis Infection among Healthcare Workers in Duhok Province: From Screening to Prophylactic Treatment. Trop. Med. Infect. Dis. 2019, 4, 85. [Google Scholar]
- Kiazyk, S.; Ball, T. Latent tuberculosis infection: An overview. Canada Commun. Dis. Rep. 2017, 43, 62–66. [Google Scholar]
- World Health Organization. Latent Tuberculosis Infection: Updated and Consolidated Guidelines for Programmatic Management; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/tb/publications/2018/latent-tuberculosis-infection/en/ (accessed on 30 May 2020).
- Nozaki, I.; Hachiya, M.; Kitamura, T. Factors influencing basic vaccination coverage in Myanmar: Secondary analysis of 2015 Myanmar demographic and health survey data. BMC Public Health 2019, 19, 242. [Google Scholar]
- Zwerling, A.; van den Hof, S.; Scholten, J.; Cobelens, F.; Menzies, D.; Pai, M. Interferon-gamma release assays for tuberculosis screening of healthcare workers: A systematic review. Thorax 2012, 67, 62–70. [Google Scholar]
- Jo, K.; Hong, Y.; Park, J.S.; Bae, I.; Sik, J.; Lee, S.; Cho, O.; Choo, E.J.; Heo, J.Y.; Woo, J.H.; et al. Prevalence of Latent Tuberculosis Infection among Health Care Workers in South Korea: A Multicenter Study. Tuberc. Respir. Dis. 2013, 3536, 18–24. [Google Scholar]
- Jo, K. Preventing the Transmission of Tuberculosis in Health Care Settings: Administrative Control. Tuberc. Respir. Dis. 2017, 3536, 21–26. [Google Scholar]
- Janagond, A.; Ganesan, V.; Vijay Kumar, G.; Ramesh, A.; Anand, P.; Mariappan, M. Screening of health-care workers for latent tuberculosis infection in a Tertiary Care Hospital. Int. J. Mycobacteriol. 2017, 6, 253–257. [Google Scholar]
- He, G.X.; van den Hof, S.; van der Werf, M.J.; Wang, G.J.; Ma, S.W.; Zhao, D.Y.; Hu, Y.L.; Yu, S.C.; Borgdorff, M.W. Infection control and the burden of tuberculosis infection and disease in health care workers in china: A cross-sectional study. BMC Infect. Dis. 2010, 10, 313. [Google Scholar]
- Rutanga, C.; Lowrance, D.W.; Oeltmann, J.E.; Mutembayire, G.; Willis, M.; Uwizeye, C.B.; Hinda, R.; Bassirou, C.; Gutreuter, S.; Gasana, M. Latent tuberculosis infection and associated factors among health care workers in Kigali, Rwanda. PLoS ONE 2015, 10, e0124485. [Google Scholar]
- Pathak, V.; Harrington, Z.; Dobler, C.C. Attitudes towards preventive tuberculosis treatment among hospital staff. PeerJ 2016, 4, e1738. [Google Scholar]
- World Health Organization. WHO Guidelines on Tuberculosis Infection Prevention and Control 2019 Update; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/311259/9789241550512-eng.pdf?ua=1 (accessed on 30 May 2020).
- Desta, M.; Ayenew, T.; Sitotaw, N.; Tegegne, N.; Dires, M.; Getie, M. Knowledge, practice and associated factors of infection prevention among healthcare workers in Debre Markos referral hospital, Northwest Ethiopia. BMC Health Serv. Res. 2018, 18, 465. [Google Scholar]
- Houben, R.M.G.J.; Dodd, P.J. The Global Burden of Latent Tuberculosis Infection: A Re-estimation Using Mathematical Modelling. PLoS Med. 2016, 13, e1002152. [Google Scholar]
- Whitaker, J.; Mirtskhulava, V.; Kipiani, M.; Harris, D.A.; Tabagari, N.; Kempker, R.R.; Blumberg, H.M. Prevalence and Incidence of Latent Tuberculosis Infection in Georgian Healthcare Workers. PLoS ONE 2013, 8, e58202. [Google Scholar]
- Park, J.S. The Prevalence and Risk Factors of Latent Tuberculosis Infection among Health Care Workers Working in a Tertiary Hospital in South Korea. Tuberc. Respir. Dis. 2018, 81, 274–280. [Google Scholar]
- Luksamijarulkul, P.; Supapvanit, C.; Loosereewanich, P.; Aiumlaor, P. Risk assessment towards tuberculosis among hospital personnel: Administrative control, risk exposure, use of protective barriers and microbial air quality. Southeast Asian J. Trop Med. Public Health 2004, 35, 1005–1011. [Google Scholar]
- Shi, C.L.; Xu, J.C.; Chen, H.; Ye, Z.J.; Chen, X.N.; Tang, P.J.; Ma, L.L.; Tang, Z.X.; Wu, M.Y.; Xu, P. Risk factors of latent tuberculosis infection and immune function in health care workers in Suzhou, China. J. Thorac. Dis. 2018, 10, 6742–6752. [Google Scholar]
- Id, P.M.; Id, L.L.; Motsomi, K.; Bosch, Z.; Milovanovic, M.; Ratsela, A.; Lala, S.; Variava, E.; Golub, E.; Webb, E.L.; et al. Prevalence and risk factors for latent tuberculosis infection among household contacts of index cases in two South African provinces: Analysis of baseline data from a cluster-randomised trial. PLoS ONE 2020, 725, e0230376. [Google Scholar]
- Farhat, M.; Greenaway, C.; Pai, M.; Menzies, D. False-positive tuberculin skin tests: What is the absolute effect of BCG and non-tuberculous mycobacteria? Int. J. Tuberc. Lung Dis. 2006, 10, 1192–1204. [Google Scholar]
- Faust, L.; Schreiber, Y.; Bocking, N. A systematic review of BCG vaccination policies among high-risk groups in low TB- burden countries: Implications for vaccination strategy in Canadian indigenous communities. BMC Public Health 2019, 19, 1504. [Google Scholar]


{kind=link}
| Variable | Total N = 498, n (%) | General HCW N = 250, n (%) | TB HCW N = 248, n (%) | p-Value | TST Negative N = 382, n (%) | TST Positive N = 116, n (%) | p-Value |
|---|---|---|---|---|---|---|---|
| HCW Type | <0.001 | ||||||
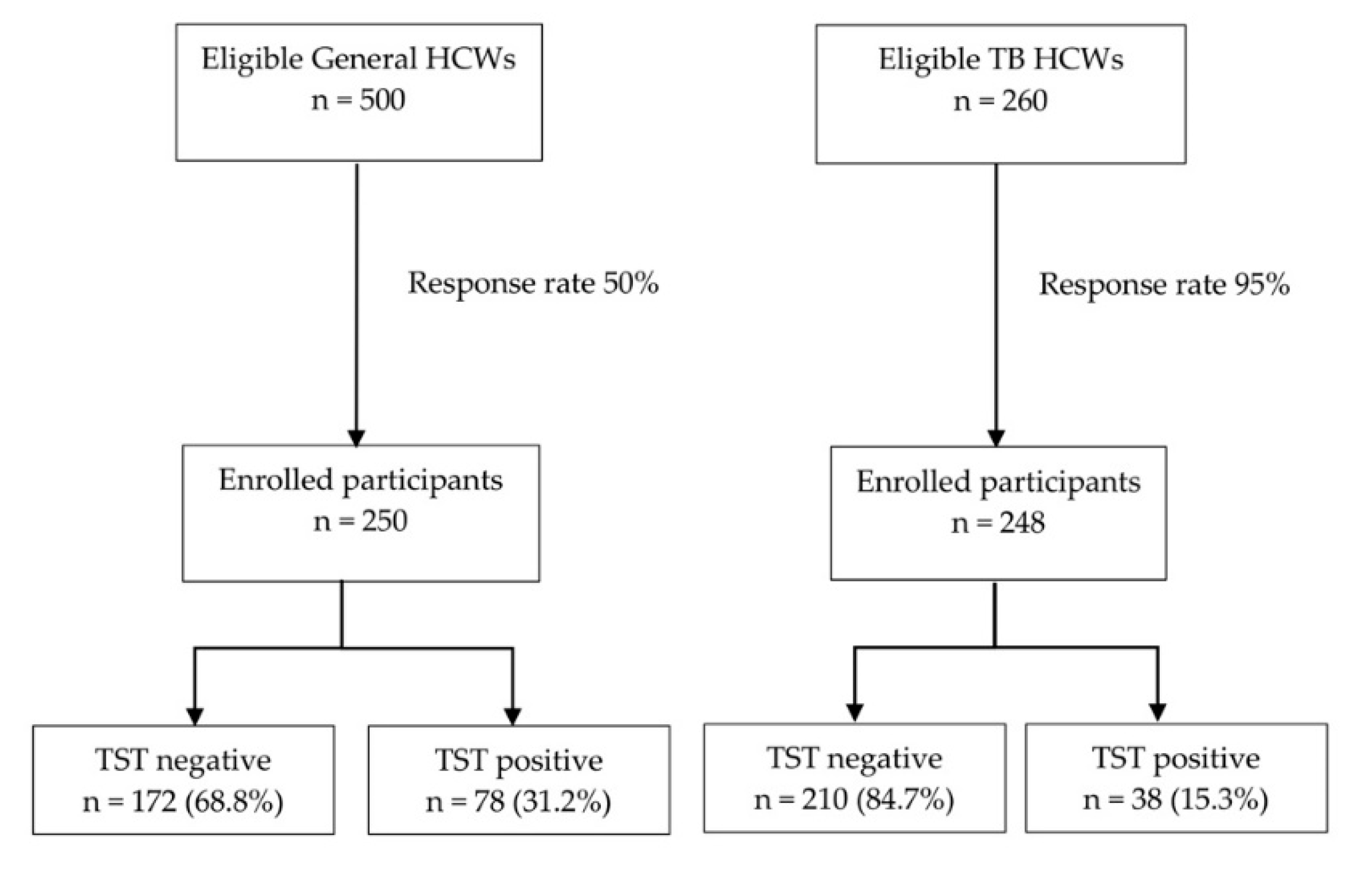
| TB | 248 (49.8) | - | - | 210 (84.7) | 38 (15.3) | ||
| General | 250 (50.2) | - | - | 172 (68.8) | 78 (31.2) | ||
| Age, years, Median (IQR) | 26 (23, 35) | 31 (25, 42) | 25 (23, 28) | <0.001 | 26 (23, 32) | 33.5 (25, 43) | <0.001 |
| Age group, years | <0.001 | <0.001 | |||||
| 20–29 | 327 (65.7) | 124 (49.6) | 203 (81.9) | 277 (72.5) | 50 (43.1) | ||
| 30–39 | 92 (18.5) | 60 (24.0) | 32 (12.9) | 62 (16.2) | 30 (25.9) | ||
| 40–49 | 64 (12.9) | 55 (22.0) | 9 (3.6) | 34 (8.9) | 30 (25.9) | ||
| 50+ | 15 (3) | 11 (4.4) | 4 (1.6) | 9 (2.4) | 6 (5.2) | ||
| Gender | 0.694 | 0.596 | |||||
| Female | 393 (78.9) | 195 (78.0) | 198 (79.8) | 304 (79.6) | 89 (76.7) | ||
| Male | 105 (21.1) | 55 (22.0) | 50 (20.2) | 78 (20.4) | 27 (23.3) | ||
| Graduated | <0.001 | <0.001 | |||||
| Yes | 390 (78.3) | 154 (61.6) | 236 (95.2) | 316 (82.7) | 74 (63.8) | ||
| No | 108 (21.7) | 96 (38.4) | 12 (4.8) | 66 (17.3) | 42 (36.2) | ||
| Profession | <0.001 | <0.001 | |||||
| Administrative staff | 30 (6.0) | 30 (12.0) | 0 (0) | 20 (5.2) | 10 (8.6) | ||
| Basic Health staff | 230 (46.2) | 4 (1.6) | 226 (91.1) | 194 (50.8) | 36 (31.0) | ||
| Doctor/Nurse/Lab staff | 158 (31.7) | 136 (54.4) | 22 (8.9) | 120 (31.4) | 38 (32.8) | ||
| Pharmacist | 8 (1.6) | 8 (3.2) | 0 (0) | 2 (0.5) | 6 (5.2) | ||
| Ward staff | 72 (14.5) | 72 (28.8) | 0 (0) | 46 (12.0) | 26 (22.4) | ||
| Total service years, Median (IQR) | 4 (3, 10) | 6 (3,15) | 4 (3,6) | <0.001 | 4 (3, 6) | 7.5 (4, 16) | <0.001 |
| Total service years | <0.001 | <0.001 | |||||
| <10 | 390 (78.3) | 166 (66.4) | 224 (90.3) | 322 (84.3) | 68 (58.6) | ||
| 10+ | 108 (21.7) | 84 (33.6) | 24 (9.7) | 60 (15.7) | 48 (41.4) | ||
| Exposure to presumptive TB cases | <0.001 | <0.001 | |||||
| No | 216 (43.4) | 180 (72.0) | 36 (14.5) | 148 (38.7) | 68 (58.6) | ||
| Yes | 282 (56.6) | 70 (28.0) | 212 (85.5) | 234 (61.3) | 48 (41.4) | ||
| Exposure to TB patients | <0.001 | 0.006 | |||||
| No | 234 (47) | 178 (71.2) | 56 (22.6) | 166 (43.5) | 68 (58.6) | ||
| Yes | 264 (53) | 72 (28.8) | 192 (77.4) | 216 (56.5) | 48 (41.4) | ||
| Exposure to MDR TB patients | 0.876 | 0.961 | |||||
| No | 392 (78.7) | 198 (79.2) | 194 (78.2) | 300 (78.5) | 92 (79.3) | ||
| Yes | 106 (21.3) | 52 (20.8) | 54 (21.8) | 82 (21.5) | 24 (20.7) | ||
| Previous BCG vaccination | <0.001 | 0.005 | |||||
| No | 208 (41.8) | 148 (59.2) | 60 (24.2) | 146 (38.2) | 62 (53.4) | ||
| Yes | 290 (58.2) | 102 (40.8) | 188 (75.8) | 236 (61.8) | 54 (46.6) | ||
| Household TB contact | 1 | 0.336 | |||||
| No | 450 (90.4) | 226 (90.4) | 224 (90.3) | 342 (89.5) | 108 (93.1) | ||
| Yes | 48 (9.6) | 24 (9.6) | 24 (9.7) | 40 (10.5) | 8 (6.9) | ||
| Previous history of TB | 0.751 | 0.99 | |||||
| No | 488 (98) | 244 (97.6) | 244 (98.4) | 374 (97.9) | 114 (98.3) | ||
| Yes | 10 (2) | 6 (2.4) | 4 (1.6) | 8 (2.1) | 2 (1.7) |
| Knowledge Item | TST Negative N = 382, n (%) | TST Positive N = 116, n (%) | p-Value |
|---|---|---|---|
| An infection control committee is necessary for TB control | 1 | ||
| No | 40 (10.5) | 12 (10.3) | |
| Yes | 342 (89.5) | 104 (89.7) | |
| Minimizing contact time with TB patients is necessary for TB control | <0.001 | ||
| No | 24 (6.3) | 20 (17.2) | |
| Yes | 358 (93.7) | 96 (82.8) | |
| Presumptive or confirmed TB cases should be separated | 0.82 | ||
| No | 22 (5.8) | 8 (6.9) | |
| Yes | 360 (94.2) | 108 (93.1) | |
| TB patients should be educated on cough etiquette | 0.99 | ||
| No | 14 (3.7) | 4 (3.4) | |
| Yes | 368 (96.3) | 112 (96.6) | |
| Presumptive or confirmed TB cases who are coughing should be given priority | 0.807 | ||
| No | 38 (9.9) | 10 (8.6) | |
| Yes | 344 (90.1) | 106 (91.4) | |
| TB screening of HCWs is one of the TB infection control measures | <0.001 | ||
| No | 44 (11.5) | 34 (29.3) | |
| Yes | 338 (88.5) | 82 (70.7) | |
| The doors and windows of a room should be open whenever a TB case is present | <0.001 | ||
| No | 80 (20.9) | 46 (39.7) | |
| Yes | 302 (79.1) | 70 (60.3) | |
| Fans can be used to reduce TB transmission | <0.001 | ||
| No | 110 (28.8) | 56 (48.3) | |
| Yes | 272 (71.2) | 60 (51.7) | |
| Surgical masks cannot protect HCWs from getting infected with TB | 0.479 | ||
| No | 142 (37.2) | 48 (41.4) | |
| Yes | 240 (62.8) | 68 (58.6) | |
| Respirators can protect HCWs from getting infected with TB | 0.864 | ||
| No | 64 (16.8) | 18 (15.5) | |
| Yes | 318 (83.2) | 98 (84.5) | |
| Behavior Item | TST Negative N = 382, n (%) | TST Positive N = 116, n (%) | p-Value |
|---|---|---|---|
| Prioritizes coughing patients | 0.02 | ||
| No | 100 (26.2) | 44 (37.9) | |
| Yes | 282 (73.8) | 72 (62.1) | |
| Educates TB patients about correct cough etiquette | 0.123 | ||
| No | 40 (10.5) | 6 (5.2) | |
| Yes | 342 (89.5) | 110 (94.8) | |
| Tests for TB in case you have cough | 0.337 | ||
| No | 118 (30.9) | 42 (36.2) | |
| Yes | 264 (69.1) | 74 (63.8) | |
| Opens the windows whenever a TB case is in the room | 0.02 | ||
| No | 112 (29.3) | 48 (41.4) | |
| Yes | 270 (70.7) | 68 (58.6) | |
| Turns on the fan while treating TB cases | 0.342 | ||
| No | 196 (51.3) | 66 (56.9) | |
| Yes | 186 (48.7) | 50 (43.1) | |
| Uses surgical mask whenever treating TB patients | 0.716 | ||
| No | 52 (13.6) | 18 (15.5) | |
| Yes | 330 (86.4) | 98 (84.5) | |
| Uses N95 whenever treating TB patients | 0.626 | ||
| No | 252 (66) | 80 (69) | |
| Yes | 130 (34) | 36 (31) | |
| Variable | Crude OR (95% CI) | Adj. OR (95% CI) | p-Value |
|---|---|---|---|
| Type of HCW: General HCW vs. TB HCW | 2.51 (1.62, 3.88) | 1.37 (0.8, 2.33) | 0.253 |
| Graduated: No vs. Yes | 2.72 (1.71, 4.31) | 1.78 (1.02, 3.1) | 0.043 |
| Total service years: 10+ vs. <10 | 3.79 (2.39, 6.01) | 3.23 (1.93, 5.38) | <0.001 |
| Knowing that TB screening of HCWs is a TB infection control measure: Yes vs. No | 0.31 (0.19, 0.52) | 0.28 (0.15, 0.54) | <0.001 |
| Educating cough etiquette to TB patients: Yes vs. No | 2.14 (0.89, 5.19) | 7.38 (2.61, 20.86) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phyu, M.H.; Sriplung, H.; Kyi, M.S.; San, C.C.; Chongsuvivatwong, V. Comparison of Latent Tuberculosis Infections among General versus Tuberculosis Health Care Workers in Myanmar. Trop. Med. Infect. Dis. 2020, 5, 116. https://doi.org/10.3390/tropicalmed5030116
Phyu MH, Sriplung H, Kyi MS, San CC, Chongsuvivatwong V. Comparison of Latent Tuberculosis Infections among General versus Tuberculosis Health Care Workers in Myanmar. Tropical Medicine and Infectious Disease. 2020; 5(3):116. https://doi.org/10.3390/tropicalmed5030116
Chicago/Turabian StylePhyu, Moe Hnin, Hutcha Sriplung, Myo Su Kyi, Cho Cho San, and Virasakdi Chongsuvivatwong. 2020. "Comparison of Latent Tuberculosis Infections among General versus Tuberculosis Health Care Workers in Myanmar" Tropical Medicine and Infectious Disease 5, no. 3: 116. https://doi.org/10.3390/tropicalmed5030116
APA StylePhyu, M. H., Sriplung, H., Kyi, M. S., San, C. C., & Chongsuvivatwong, V. (2020). Comparison of Latent Tuberculosis Infections among General versus Tuberculosis Health Care Workers in Myanmar. Tropical Medicine and Infectious Disease, 5(3), 116. https://doi.org/10.3390/tropicalmed5030116