
Malaria in the Time of COVID-19: Do Not Miss the Real Cause of Illness

 , ,
, ,  ,
,  and
and
Abstract
:Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Epidemiological Update 28.09.2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200928-weekly-epi-update.pdf?sfvrsn=9e354665_4 (accessed on 29 September 2020).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Zhong, N.S. Clinical characteristics of Coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Sardar, S.; Sharma, R.; Alyamani, T.Y.M.; Aboukamar, M. COVID-19 and Plasmodium vivax malaria co-infection. IDCases 2020, 21, e00879. [Google Scholar] [CrossRef]
- Correia, M.J.; Frade, L.; Guerreiro, R.; Araujo, I.; Baptista, T.; Fonseca, C.; Mansinho, K. A patient with severe malaria and COVID-19: How do you tell the difference between these infections? Eur. J. Case Rep. Intern. Med. 2020, 7, 002007. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Redelmeier, D.; Ruff, C.C.; Tobler, P.N. Cognitive biases associated with medical decisions: A systematic review. BMC Med. Inform. Decis. Mak. 2016, 16, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, G.R.; Monteiro, S.D.; Sherbino, J.; Ilgen, J.S.; Schmidt, H.G.; Mamede, S. The causes of errors in clinical reasoning: Cognitive biases, knowledge deficits, and dual process thinking. Acad. Med. 2017, 92, 23–30. [Google Scholar] [CrossRef] [PubMed]



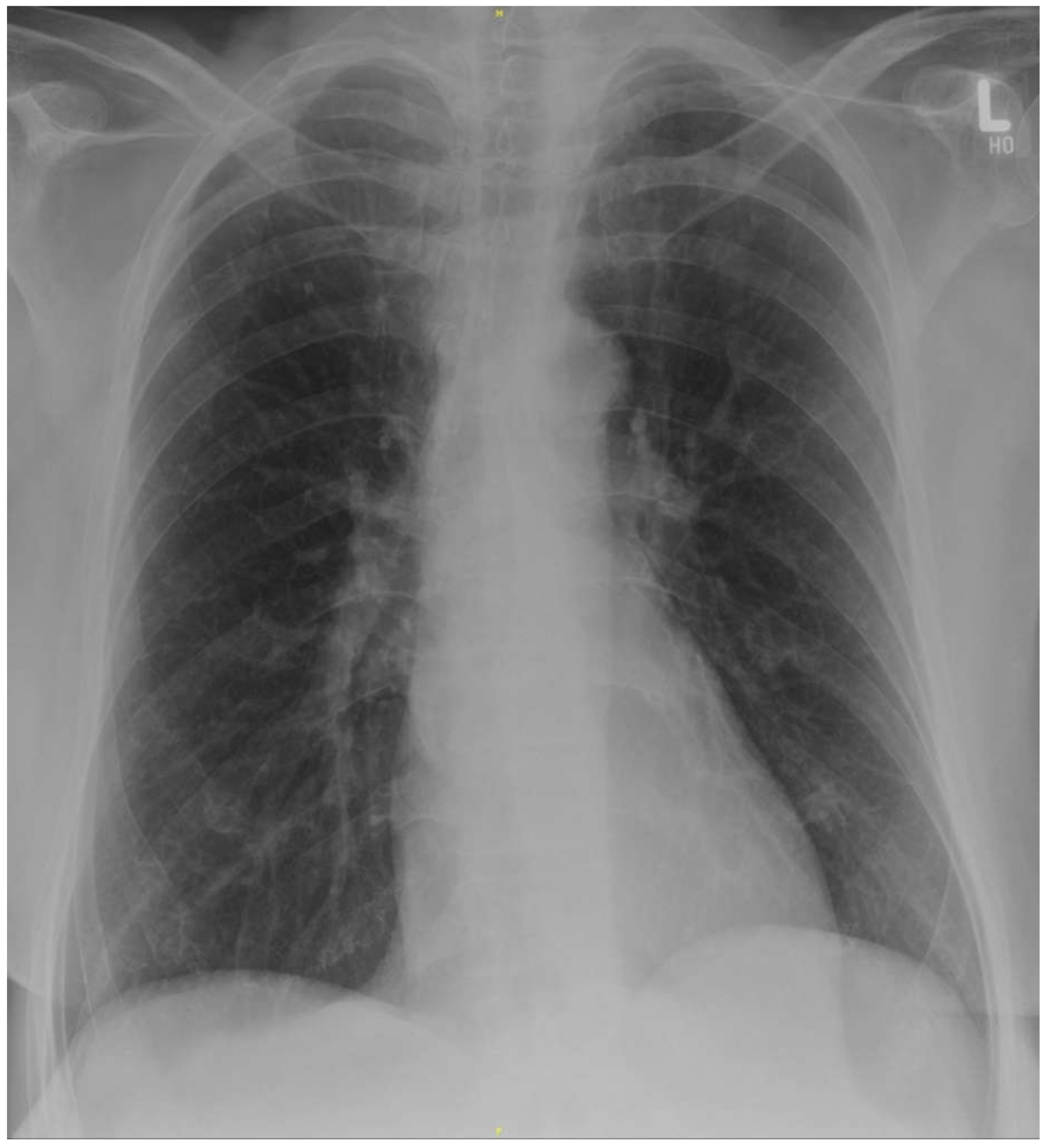{kind=link}
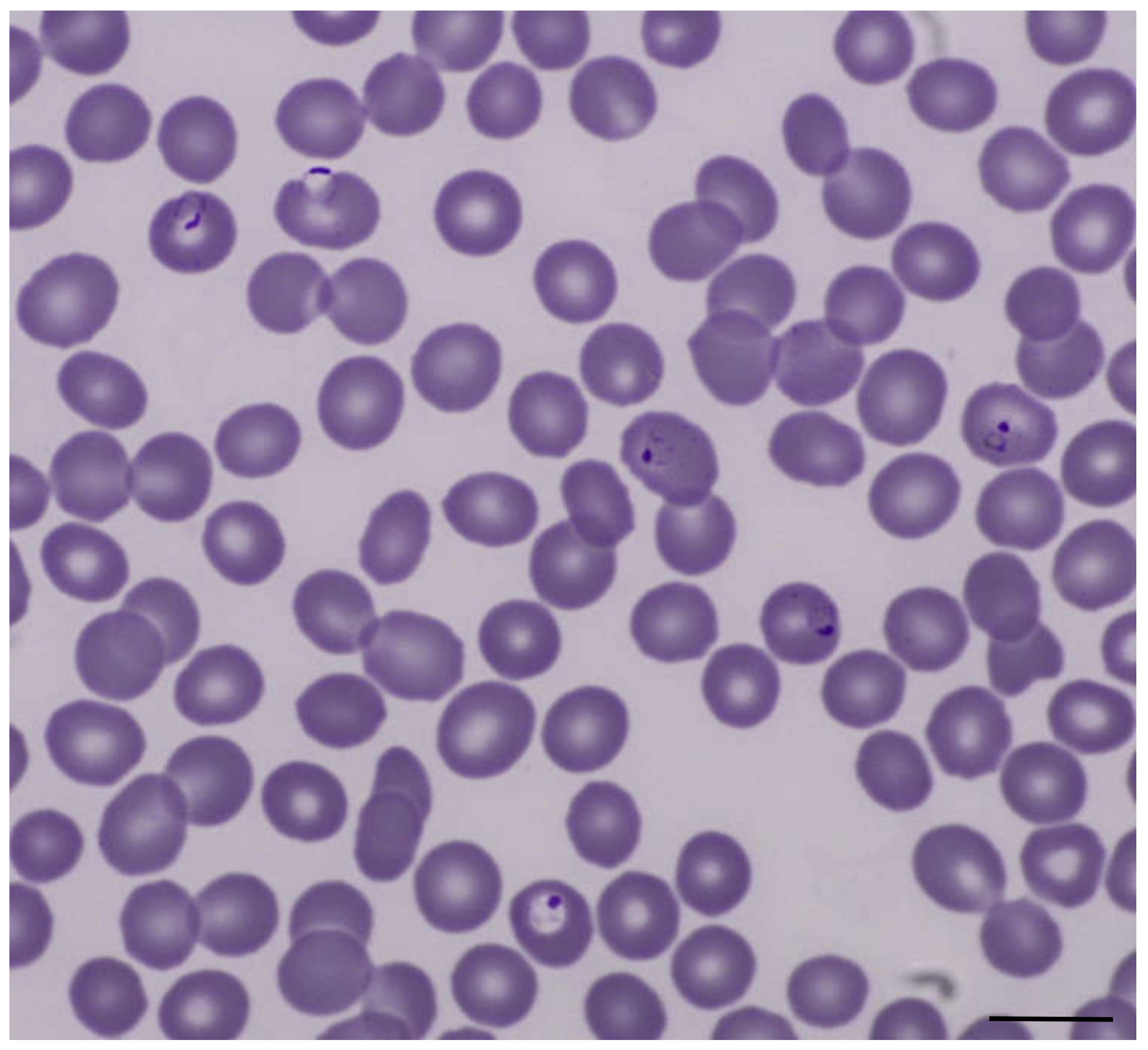{kind=link}
| Laboratory Parameter and Unit | Patient Value | Reference Range |
|---|---|---|
| Leucocyte count/µL | 2700 | 3800–11,000 |
| Hemoglobin g/dL | 13.9 | 12.3–15.3 |
| Platelet count/µL | 23,000 | 150,000–400,000 |
| Total bilirubin mg/dL | 1.5 | 0.3–1.2 |
| Alanine aminotransferase U/L | 40 | <35 |
| Aspartate aminotransferase U/L | 36 | <35 |
| Lactate dehydrogenase U/L | 358 | 120–246 |
| Creatinine mg/dL | 0.67 | 0.55–1.02 |
| C-reactive protein mg/L | 103 | <5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jochum, J.; Kreuels, B.; Tannich, E.; Huber, S.; Schulze zur Wiesch, J.; Schmiedel, S.; Ramharter, M.; Addo, M.M. Malaria in the Time of COVID-19: Do Not Miss the Real Cause of Illness. Trop. Med. Infect. Dis. 2021, 6, 40. https://doi.org/10.3390/tropicalmed6020040
Jochum J, Kreuels B, Tannich E, Huber S, Schulze zur Wiesch J, Schmiedel S, Ramharter M, Addo MM. Malaria in the Time of COVID-19: Do Not Miss the Real Cause of Illness. Tropical Medicine and Infectious Disease. 2021; 6(2):40. https://doi.org/10.3390/tropicalmed6020040
Chicago/Turabian StyleJochum, Johannes, Benno Kreuels, Egbert Tannich, Samuel Huber, Julian Schulze zur Wiesch, Stefan Schmiedel, Michael Ramharter, and Marylyn M. Addo. 2021. "Malaria in the Time of COVID-19: Do Not Miss the Real Cause of Illness" Tropical Medicine and Infectious Disease 6, no. 2: 40. https://doi.org/10.3390/tropicalmed6020040
APA StyleJochum, J., Kreuels, B., Tannich, E., Huber, S., Schulze zur Wiesch, J., Schmiedel, S., Ramharter, M., & Addo, M. M. (2021). Malaria in the Time of COVID-19: Do Not Miss the Real Cause of Illness. Tropical Medicine and Infectious Disease, 6(2), 40. https://doi.org/10.3390/tropicalmed6020040