
Wounds, Antimicrobial Resistance and Challenges of Implementing a Surveillance System in Myanmar: A Mixed-Methods Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting
2.2.2. AMR Surveillance in Myanmar
2.2.3. Specific Setting
2.2.4. Procedure for Wound Cultures
2.2.5. Definitions
2.3. Study Population
2.4. Data Variables, Sources of Data and Data Collection
2.5. Analysis and Statistics
3. Results
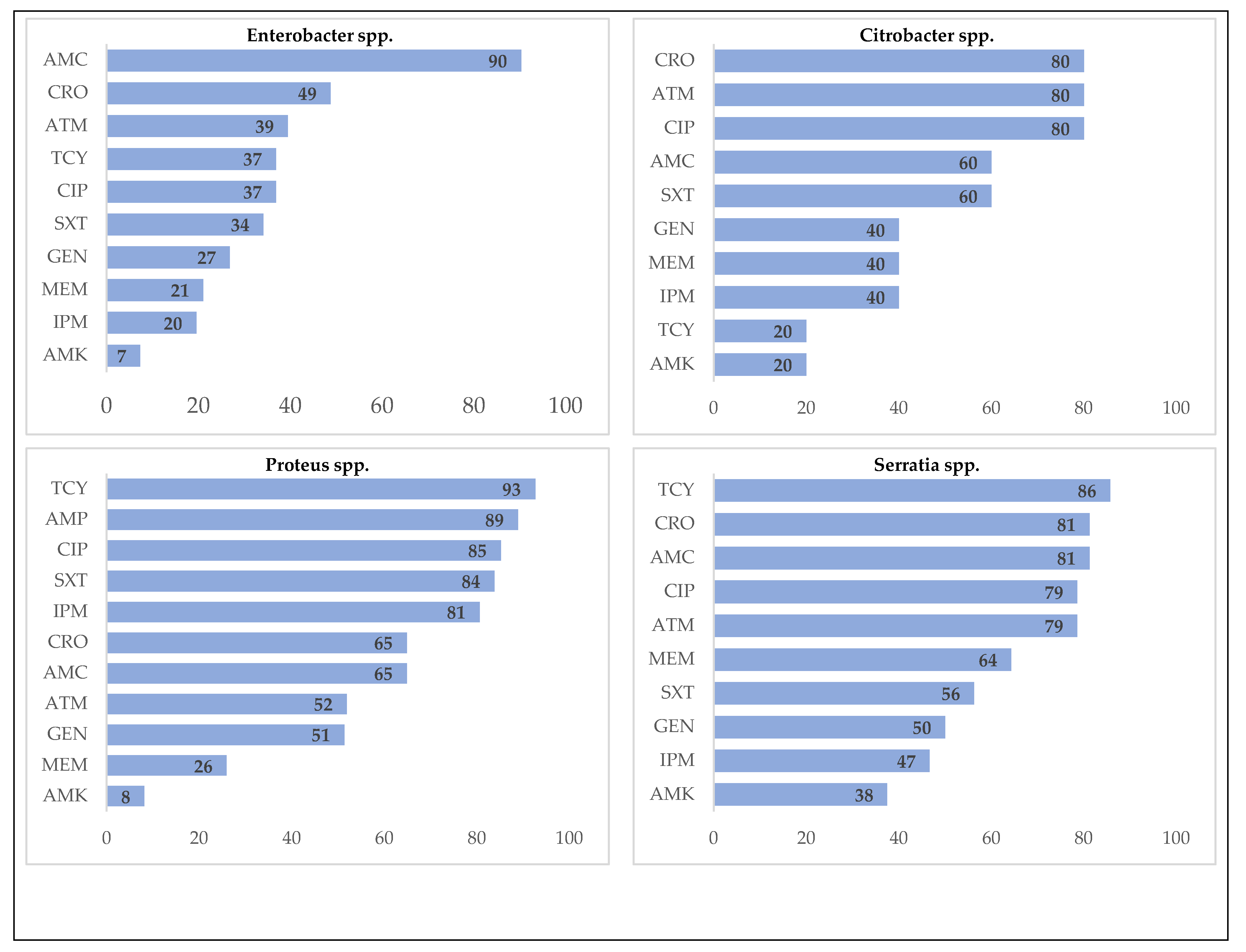
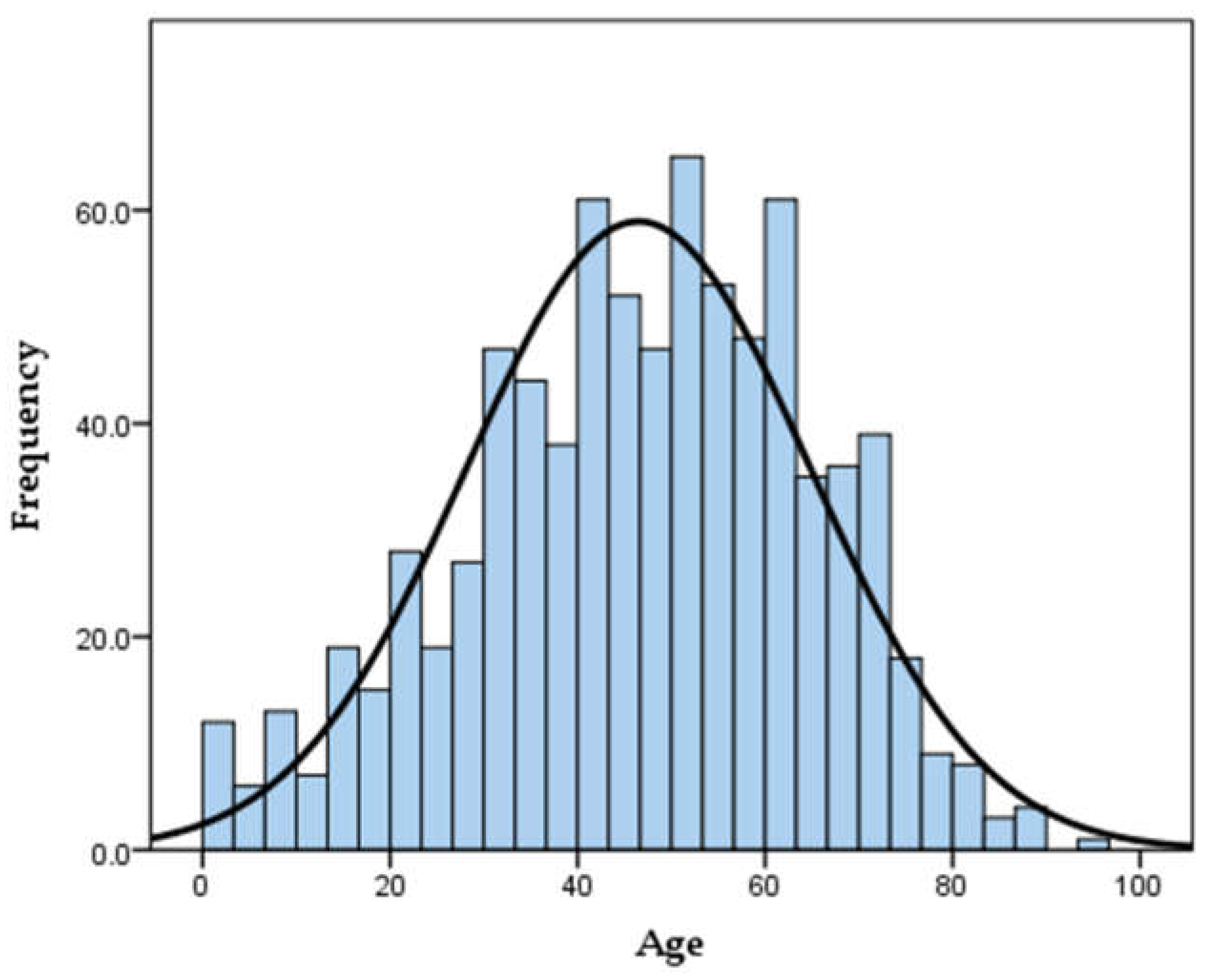
3.1. Quantitative Findings
3.2. Qualitative Findings
3.2.1. Challenges in Implementing the AMR Surveillance System
“We have not standardized the configuration (laboratory configuration for antimicrobials test and data entry) and we only taught them how to build configuration. Each hospital built their configuration as they liked and therefore, they are not uniform with each other. Therefore, when we hold the meeting this time, we will discuss how to standardize the configuration style and the antibiotic list.”(Participant 6)
“My department’s workload is heavy, and only one microbiologist, one officer and one medical technician were present…… Ask my officer if you want to know more about data. I don’t know.”(Participant 9)
“For the reviews and research, the data are not readily available. To know how many organisms there are, I must count from the registration book and make a tally. Electronic data does not exist. That makes me have a headache.”(Participant 5)
3.2.2. Suggestions to Improve AMR Surveillance
Strengthening Capacity for Surveillance
“It is required to get software training for management and analysis of AMR data. Microbiologists also need capacity building for AMR surveillance…. Major constraint is technical.”(Participant 4)
“This hospital uses computerized ICD code 10 for diagnosis reporting system. Like that, if we have a proper software for the collection of patient’s data, it would be very convenient for us. Or we should have one data collector for this.”(Participant 7)
Use of Hospital Antibiogram Data
“We publish antibiogram data biannually or annually which are already sent to NHL by our microbiologist. We send these data to every ward in the hospital so that they can take actions. We can adjust the antibiotic usage by reviewing this antibiogram data…So, every hospital should have antibiogram.”(Participant 3)
Standardized Guidelines and Formats
“It would be nice if something like a proforma can be distributed evenly. In that form, all the necessary information like background information, and diagnosis should be included. The format needs to be consistent.”(Participant 3)
Multisectoral Approach
“Antibiotics are widely used not only in human sector but also in animal, fishery and agricultural sectors. We need to carefully think about how to do legislation on antibiotic use in collaboration with FDA. There should be strong multisectoral collaboration to control irrational use of antibiotics like taking antibiotics without prescription and not complete the full course of antibiotics.”(Participant 4)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Open Access Statement
Appendix A
Appendix A.1. Key Informant Interview: Interview Guide
Appendix A.2. Introduction
Appendix A.3. General and Demographic Information
- Please tell me about yourself.
- Age, rank, level of education, role in the antimicrobial surveillance system, number of years in this system.
Appendix A.4. Information Related to AMR Surveillance System
- Please describe your main routine activities, role, and responsibilities in the antimicrobial surveillance system
- Now let talk about the challenges you have been facing in carrying out properly these activities.
- o
- What challenges do you face regarding communication, data reporting, or data monitoring of the antimicrobial surveillance system?
- o
- What are the technical challenges faced in the antimicrobial surveillance system? As technical aspects, I refer to laboratory technical capacities, the competencies, availability, and motivation of human resources (physicians, nurses, laboratory technicians, and data reporting officers).
- o
- Could you also explain about the challenges related to the logistics aspects such difficulties in availability and management of technology for a functional surveillance system?
- o
- If there is any other challenge you or other staff have been facing regarding antimicrobial surveillance system, please explain.
- What measures have been put in place to address these challenges?
Appendix A.5. Suggestions
- From your experience, what do you think are the possible feasible solutions to address these challenges?
- What concrete recommendations and to whom may you formulate to improve wound-related antimicrobial surveillance system in general?
- Is there any other information you would like to share with me? If yes please share.
Appendix A.6. Conclusions
Appendix B


References
- Centers for Disease Control and Prevention (CDC). Antibiotic/Antimicrobial Resistance (AR/AMR). Available online: https://www.cdc.gov/drugresistance/about.html (accessed on 16 April 2019).
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). The 2019 AR Threats Report. Available online: www.cdc.gov/DrugResistance/Biggest-Threats.html (accessed on 24 April 2021).
- O’Neill, J. Review on Antimicrobial Resistance. In Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Delamou, A.; Camara, B.S.; Sidibé, S.; Camara, A.; Dioubaté, N.; El Ayadi, A.M.; Tayler-Smith, K.; Beavogui, A.H.; Baldé, M.D.; Zachariah, R. Trends of and factors associated with cesarean section related surgical site infections in Guinea. J. Public Health Afr. 2019, 10, 818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Department of Violence and Injury Prevention and Disability World Health Organization. WHO Guideline: Prevention and Management of Wound Infection. Available online: https://www.who.int/hac/techguidance/tools/guidelines_prevention_and_management_wound_infection.pdf (accessed on 16 April 2019).
- Woodmansey, E.J.; Roberts, C.D. Appropriate use of dressings containing nanocrystalline silver to support antimicrobial stewardship in wounds. Int. Wound J. 2018, 15, 1025–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, H.; Janssen, I.; Cooper, P.; Kainyah, C.; Pellio, T.; Quintel, M.; Monnheimer, M.; Groß, U.; Schulze, M.H. Antimicrobial-resistant bacteria in infected wounds, Ghana, 2014. Emerg. Infect. Dis. 2018, 24, 916. [Google Scholar] [CrossRef] [PubMed]
- Mama, M.; Abdissa, A.; Sewunet, T. Antimicrobial susceptibility pattern of bacterial isolates from wound infection and their sensitivity to alternative topical agents at Jimma University Specialized Hospital, South-West Ethiopia. Ann. Clin. Microbiol. Antimicrob. 2014, 13, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, A.; Endris, M.; Gebrecherkos, T.; Tiruneh, M.; Moges, F. Bacterial Isolates and Their Antimicrobial Susceptibility Patterns of Wound Infections among Inpatients and Outpatients Attending the University of Gondar Referral Hospital, Northwest Ethiopia. Int. J. Microbiol. 2017, 2017, 8953829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shittu, A.; Kolawole, D.; Oyedepo, E. A study of wound infections in two health institutions in Ile-Ife, Nigeria. Afr. J. Biomed. Res. 2002, 5. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 19 April 2019).
- World Health Organization (WHO). Enhance infection prevention and control. Available online: http://www.emro.who.int/world-health-days/2011/enhance-infection-prevention-and-control.html (accessed on 19 April 2019).
- Leekha, S.; Terrell, C.L.; Edson, R.S. General principles of antimicrobial therapy. Mayo Clin. Proc. 2011, 86, 156–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Antimicrobial Resistance Surveillance. Available online: https://www.who.int/medicines/areas/rational_use/AMR_Surveillance/en/ (accessed on 19 April 2019).
- Vernet, G.; Mary, C.; Altmann, D.M.; Doumbo, O.; Morpeth, S.; Bhutta, Z.A.; Klugman, K.P. Surveillance for antimicrobial drug resistance in under-resourced countries. Emerg. Infect. Dis. 2014, 20, 434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oluwatosin, O. Surgical wound infection: A general overview. Ann. Ib. Postgrad. Med. 2005, 3, 26–31. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Antimicrobial Resistance. Available online: http://www.emro.who.int/health-topics/drug-resistance/regional-situation.html#:~:text=Antimicrobial%20resistance%20(AMR)%20is%20the,and%20may%20spread%20to%20others (accessed on 29 October 2019).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ananthi, B.; Ramakumar, M.; Kalpanadevi, V.; Abigail, R.S.; Karthiga, L.; Victor, H.K. Aerobic bacteriological profile and antimicrobial susceptibility pattern in postoperative wound infections at a tertiary care hospital. Proteus 2017, 3, 4–11. [Google Scholar]
- Abdu, A.; Egbagba, J.; Fente, B. Identification and antimicrobial susceptibility profile of bacterial pathogens isolated from wound infections in a tertiary hospital, Bayelsa South southern, Nigeria. Trop. J. Pathol. Microbiol. 2019, 5, 966–975. [Google Scholar] [CrossRef] [Green Version]
- Kassam, N.A.; Damian, D.J.; Kajeguka, D.; Nyombi, B.; Kibiki, G.S. Spectrum and antibiogram of bacteria isolated from patients presenting with infected wounds in a Tertiary Hospital, northern Tanzania. BMC Res. Notes 2017, 10, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aung, M.S.; Zi, H.; Nwe, K.M.; Maw, W.W.; Aung, M.T.; Min, W.; Nyein, N.; Kawaguchiya, M.; Urushibara, N.; Sumi, A. Drug resistance and genetic characteristics of clinical isolates of staphylococci in Myanmar: High prevalence of PVL among methicillin-susceptible Staphylococcus aureus belonging to various sequence types. New Microbes New Infect. 2016, 10, 58–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandra, S.; Alvarez-Uria, G.; Turner, P.; Joshi, J.; Limmathurotsakul, D.; van Doorn, H.R. Antimicrobial resistance surveillance in low-and middle-income countries: Progress and challenges in eight South Asian and Southeast Asian countries. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, R.A.; Teshal, A.M.; Dinku, S.F.; Abera, N.A.; Negeri, A.A.; Desta, F.G.; Seyum, E.T.; Gemeda, A.W.; Keficho, W.M. Antimicrobial resistance surveillance in Ethiopia: Implementation experiences and lessons learned. Afr. J. Lab. Med. 2018, 7, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organism Groups | Organisms | Number | (%) |
|---|---|---|---|
| Total (isolates) | 1014 * | 100 | |
| Gram-positive | Staphylococcus aureus | 153 | 15.1 |
| Coagulase-negative staphylococci | 236 | 23.3 | |
| Streptococcus spp. | 16 | 1.6 | |
| Enterococcus spp. | 37 | 3.6 | |
| Gram-negative | Enterobacteriaceae | ||
| Escherichia coli | 127 | 12.5 | |
| Klebsiella spp. | 80 | 7.9 | |
| Enterobacter spp. | 43 | 4.2 | |
| Citrobacter spp. | 6 | 0.6 | |
| Proteus spp. | 37 | 3.6 | |
| Serratia spp. | 16 | 1.6 | |
| Non-Enterobacteriaceae | |||
| Acinetobacter baumannii | 72 | 7.1 | |
| Other Acinetobacter spp. | 5 | 0.5 | |
| Pseudomonas aeruginosa | 102 | 10.1 | |
| Other Pseudomonas spp. | 11 | 1.1 | |
| Burkholderia cepacia | 10 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandar, W.-P.; Saw, S.; Kumar, A.M.V.; Camara, B.S.; Sein, M.-M. Wounds, Antimicrobial Resistance and Challenges of Implementing a Surveillance System in Myanmar: A Mixed-Methods Study. Trop. Med. Infect. Dis. 2021, 6, 80. https://doi.org/10.3390/tropicalmed6020080
Sandar W-P, Saw S, Kumar AMV, Camara BS, Sein M-M. Wounds, Antimicrobial Resistance and Challenges of Implementing a Surveillance System in Myanmar: A Mixed-Methods Study. Tropical Medicine and Infectious Disease. 2021; 6(2):80. https://doi.org/10.3390/tropicalmed6020080
Chicago/Turabian StyleSandar, Win-Pa, Saw Saw, Ajay M. V. Kumar, Bienvenu Salim Camara, and Myint-Myint Sein. 2021. "Wounds, Antimicrobial Resistance and Challenges of Implementing a Surveillance System in Myanmar: A Mixed-Methods Study" Tropical Medicine and Infectious Disease 6, no. 2: 80. https://doi.org/10.3390/tropicalmed6020080
APA StyleSandar, W. -P., Saw, S., Kumar, A. M. V., Camara, B. S., & Sein, M. -M. (2021). Wounds, Antimicrobial Resistance and Challenges of Implementing a Surveillance System in Myanmar: A Mixed-Methods Study. Tropical Medicine and Infectious Disease, 6(2), 80. https://doi.org/10.3390/tropicalmed6020080