
A Rapid Review on the Efficacy and Safety of Pharmacological Treatments for Chagas Disease



Abstract
:1. Introduction
2. Materials and Methods
- Any outcomes regarding efficacy of trypanocidal treatment
- Any outcomes regarding safety of trypanocidal treatment
- Types of study
- Inclusion criteria: we included data from two study designs:
- ○
- Randomized controlled trials (RCT) comparing one or more trypanocidals to an experimental group with placebo or no treatment.
- ○
- Observational studies comparing those who received one trypanocidal to others who received another trypanocidal or a different dosage or no treatment, from the same or similar populations.
- Exclusion criteria: editorials, commentaries, case-reports, conference abstracts, letters, and reviews. In addition, animal and in vitro studies, as well as studies with no comparator group(s).
- Types of participantParticipants considered for inclusion were those infected with T. cruzi at any stage of the disease (acute, indeterminate, or chronic-determinate), and who had been diagnosed by positive serology and/or polymerase chain reaction (PCR).
- Types of interventionsWe considered trypanocidal treatment as any pharmaceutical intended to reduce or suppress the parasitic load, compared to a control group of no treatment, placebo, or variation in dosage.
- Adverse eventsAn adverse event is defined by the U.S. Food & Drug administration (FDA) as any untoward medical occurrence during the treatment course of a drug, whether or not it is considered drug related [19]. The FDA classifies serious AEs as medical occurrences that result in death, are life-threatening, require prolonged hospitalization, or result in persistent or significant incapacitation, disruption to normal life or a congenital anomaly/birth defect [19].
- Outcome measuresWe defined two outcomes of interest
- Infection-related: the reduction of parasitemia by PCR, sero-reversion, and/or reduction of antibody titres
- Patient-related:
- ○
- Efficacy outcomes were defined as reduction in mortality and reduction in the progression of chronic Chagas cardiomyopathy. Progression of chronic Chagas cardiomyopathy was determined as the development of cardiac abnormalities from patients that had zero abnormalities at baseline or the development of additional cardiac abnormalities for participants that had existing abnormalities at baseline
- ○
- Safety outcomes were defined as any potential AE reported by a participant receiving trypanocidal treatment. The AEs were categorized as: total AEs, serious AEs, gastrointestinal, neurological, general and treatment discontinuation. AEs experienced while taking a placebo were also documented.
- Period of publication: 2015–2020.
- Language of publication: English, Spanish or Portuguese.
3. Results
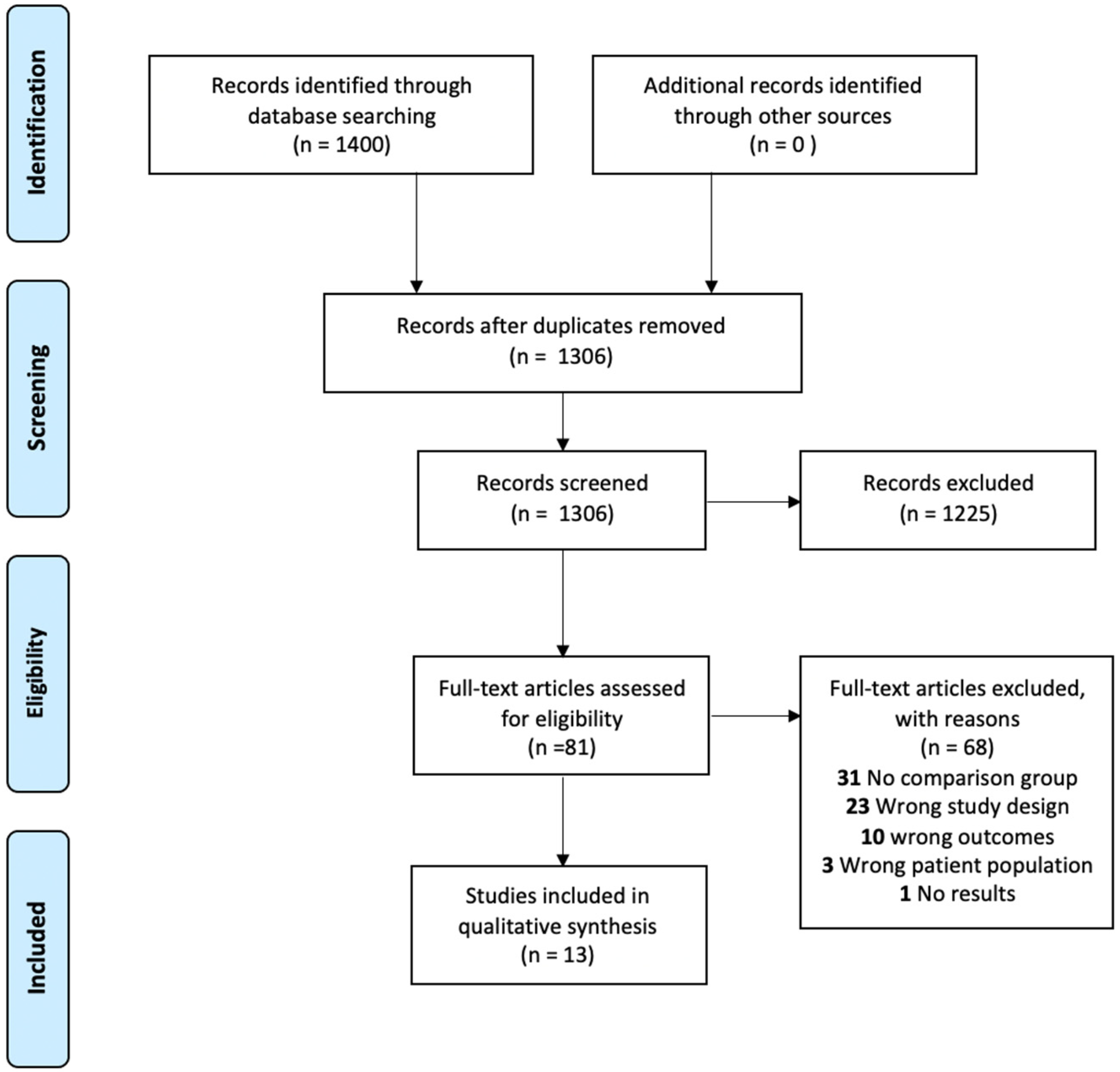
3.1. Included Studies
3.2. Efficacy Outcomes
3.3. Infection-Related Outcomes
3.4. Patient-Related Outcomes
3.4.1. Patient-Related Outcomes in RCTs
3.4.2. Patient-Related Outcomes in Observational Studies
3.4.3. Safety Outcomes
3.4.4. Benznidazole Standard Dose (5 mg/kg/day for 60 Days)
3.4.5. Variations in Benznidazole Dosing Regimens
3.4.6. Nifurtimox
3.4.7. Experimental Trypanocidals
3.4.8. Placebo
3.4.9. Adverse Events in Adults Compared to Children
3.5. Risk of Bias Assessment
4. Discussion
4.1. Limitations
4.2. Recommendations for Future Studies
- (1)
- Disclose all methodological aspects clearly and consistently
- (2)
- Standardize outcome measures used to enhance comparability
- (3)
- Collect and report data on both the efficacy of trypanocidals and the safety outcomes.
- (4)
- Report any and all AE management strategies done to mitigate toxicity and prevent treatment discontinuation.
- (5)
- Use comparable methodology when selecting assays to assess cure or treatment failure. For instance, selecting sero-reversion alone as an indicator of parasitological cure is particularly problematic as it may take years or never occur in adult patients.
- (6)
- When possible, studies should determine the infecting T. cruzi strain and make efforts to associate strain with treatment outcomes.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dorn, P.L.; McClure, A.G.; Gallaspy, M.D.; Waleckx, E.; Woods, A.S.; Monroy, M.C.; Stevens, L. The diversity of the Chagas parasite, Trypanosoma cruzi, infecting the main Central American vector, Triatoma dimidiata, from Mexico to Colombia. PLoS Negl. Trop. Dis. 2017, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutierrez, F.R.S.; Trujillo Güiza, M.L.; Escobar Martínez, M.D.C. Prevalence of Trypanosoma cruzi infection among people aged 15 to 89 years inhabiting the department of Casanare (Colombia). PLoS Negl. Trop. Dis. 2013, 7, e2113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotez, P.J.; Woc-Colburn, L.; Bottazzi, M.E. Neglected tropical diseases in Central America and Panama: Review of their prevalence, populations at risk and impact on regional development. Int. J. Parasitol. 2014, 44, 597–603. [Google Scholar] [CrossRef]
- Lidani, K.C.F.; Andrade, F.A.; Bavia, L.; Damasceno, F.S.; Beltrame, M.H.; Messias-Reason, I.J.; Sandri, T.L. Chagas disease: From discovery to a worldwide health problem. Front. Public Health 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Martins-Melo, F.R.; Alencar, C.H.; Ramos, A.N.; Heukelbach, J. Epidemiology of mortality related to Chagas disease in Brazil, 1999–2007. PLoS Negl. Trop. Dis. 2012, 6. [Google Scholar] [CrossRef] [Green Version]
- Meymandi, S.; Hernandez, S.; Park, S.; Sanchez, D.R.; Forsyth, C. Treatment of Chagas disease in the United States. Curr. Treat. Options Infect. Dis. 2018, 10, 373–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, M.C.P.; Beaton, A.; Acquatella, H.; Bern, C.; Bolger, A.F.; Echeverría, L.E.; Dutra, W.O.; Gascon, J.; Morillo, C.A.; Oliveira-Filho, J.; et al. Chagas cardiomyopathy: An update of current clinical knowledge and management. A scientific statement from the American Heart Association. Circulation 2018, 138, e169–e209. [Google Scholar] [CrossRef]
- Pan American Health Organization World Health Organization. Chagas Disease in the Americas: A Review of the Current Public Health Situation and a Vision for the Future. 2018. Available online: https://www.paho.org/hq/index.php?option=com_content&view=article&id=14399:enfermedad-chagas-en-americas-revision-de-situacion-vision-futuro&Itemid=72315&lang=en (accessed on 27 November 2020).
- Stanaway, J.D.; Roth, G. The burden of Chagas disease estimates and challenges. Glob. Heart 2015, 10, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Steverding, D. The history of Chagas disease. Parasit. Vectors 2014, 7. [Google Scholar] [CrossRef] [PubMed]
- Bonney, K.M. Chagas disease in the 21st Century: A public health success or an emerging threat? Parasite 2014, 21. [Google Scholar] [CrossRef] [PubMed]
- Francisco, A.F.; Jayawardhana, S.; Lewis, M.D.; Taylor, M.C.; Kelly, J.M. Biological factors that impinge on Chagas disease drug development. Parasitology 2017, 144, 1871–1880. [Google Scholar] [CrossRef] [PubMed]
- Morote, S.; Escribà, J.M.; García, G.; Roddy, P.; Albajar-Viñas, P.; Lima, M.Á. Tratamiento etiológico, efectos secundarios y seroconversión en pacientes con infección por el Trypanosoma cruzi. Enferm. Emerg. 2008, 10, 33–39. [Google Scholar]
- Yun, O.; Lima, M.A.; Ellman, T.; Chambi, W.; Castillo, S.; Flevaud, L.; Roddy, P.; Parreño, F.; Albajar Viñas, P.; Palma, P.P. Feasibility, drug safety, and effectiveness of etiological treatment programs for Chagas disease in Honduras, Guatemala, and Bolivia: 10-year experience of Médecins Sans Frontières. PLoS Negl. Trop. Dis. 2009, 3, e488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PAHO/WHO. Guidelines for the Diagnosis and Treatment of Chagas Disease; Pan American Health OrganizationWorld Health Organization: Washington, DC, USA, 2019; Available online: https://iris.paho.org/bitstream/handle/10665.2/49653/9789275120439_eng.pdf (accessed on 20 November 2020).
- Villar, J.C.; Perez, J.G.; Cortes, O.L.; Riarte, A.; Pepper, M.; Marin-Neto, J.A.; Guyatt, G.H. Trypanocidal drugs for chronic asymptomatic Trypanosoma cruzi infection. Cochrane Database Syst. Rev. 2014, 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khangura, S.; Konnyu, K.; Cushman, R.; Grimshaw, J.; Moher, D. Evidence summaries: The evolution of a rapid review approach. Syst. Rev. 2012, 1, 10. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Antony, J.; Zarin, W.; Strifler, L.; Ghassemi, M.; Ivory, J.; Perrier, L.; Hutton, B.; Moher, D.; Straus, S.E. A scoping review of rapid review methods. BMC Med. 2015, 13, 224. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food & Drug Administration. Title 21: Food and Drugs. Chapter 1 Subchapter D: Drugs for Human Use. 2020. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm?fr=312.32 (accessed on 2 June 2021).
- Morillo, C.A.; Marin-Neto, J.A.; Avezum, A.; Sosa-Estani, S.; Rassi, A.; Rosas, F.; Villena, E.; Quiroz, R.; Bonilla, R.; Britto, C.; et al. Randomized trial of benznidazole for chronic chagas’ cardiomyopathy. N. Engl. J. Med. 2015, 373, 1295–1306. [Google Scholar] [CrossRef] [Green Version]
- Morillo, C.A.; Waskin, H.; Sosa-Estani, S.; Del Carmen Bangher, M.; Cuneo, C.; Milesi, R.; Mallagray, M.; Apt, W.; Beloscar, J.; Gascon, J.; et al. Benznidazole and Posaconazole in eliminating parasites in asymptomatic T. cruzi carriers: The STOP-CHAGAS trial. J. Am. Coll. Cardiol. 2017, 69, 939–947. [Google Scholar] [CrossRef]
- Torrico, F.; Gascon, J.; Ortiz, L.; Alonso-Vega, C.; Pinazo, M.J.; Schijman, A.; Almeida, I.C.; Alves, F.; Strub-Wourgaft, N.; Ribeiro, I. Treatment of adult chronic indeterminate Chagas disease with benznidazole and three E1224 dosing regimens: A proof-of-concept, randomised, placebo-controlled trial. Lancet Infect. Dis. 2018, 18, 419–430. [Google Scholar] [CrossRef]
- Alarcón de Noya, B.; Ruiz-Guevara, R.; Noya, O.; Castro, J.; Ossenkopp, J.; Díaz-Bello, Z.; Colmenares, C.; Suárez, J.A.; Noya-Alarcón, O.; Naranjo, L.; et al. Long-term comparative pharmacovigilance of orally transmitted Chagas disease: First report. Expert Rev. Anti-Infect. Ther. 2017, 15, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Albareda, M.C.; Natale, M.A.; De Rissio, A.M.; Fernandez, M.; Serjan, A.; Alvarez, M.G.; Cooley, G.; Shen, H.; Viotti, R.; Bua, J.; et al. Distinct treatment outcomes of antiparasitic therapy in Trypanosoma cruzi-Infected children is associated with early changes in cytokines, chemokines, and T-Cell phenotypes. Front. Immunol. 2018, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antunes, A.P.; Ribeiro, A.L.P.; Sabino, E.C.; Silveira, M.F.; Oliveira, C.D.L.; Botelho, A.C.d.C. Benznidazole therapy for Chagas disease in asymptomatic Trypanosoma cruzi-seropositive former blood donors: Evaluation of the efficacy of different treatment regimens. Rev. Soc. Bras. Med. Trop. 2016, 49, 713–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, C.S.; Ribeiro, A.L.P.; Oliveira, C.D.L.; Oliveira, L.C.; Ferreira, A.M.; Bierrenbach, A.L.; Silva, J.L.P.; Colosimo, E.A.; Ferreira, J.E.; Lee, T.H.; et al. Beneficial effects of benznidazole in Chagas disease: NIH SaMi-Trop cohort study. PLoS Negl. Trop. Dis. 2018, 12, e0006814. [Google Scholar] [CrossRef] [Green Version]
- Colantonio, L.D.; Prado, N.; Segura, E.L.; Sosa-Estani, S. Electrocardiographic abnormalities and treatment with benznidazole among children with chronic infection by Trypanosoma cruzi: A retrospective cohort study. PLoS Negl. Trop. Dis. 2016, 10, e0004651. [Google Scholar] [CrossRef] [PubMed]
- Crespillo-Andújar, C.; López-Vélez, R.; Trigo, E.; Norman, F.; Díaz-Menéndez, M.; Monge-Maillo, B.; Arsuaga, M.; Pérez-Molina, J.A. Comparison of the toxicity of two treatment schemes with benznidazole for chronic Chagas disease: A prospective cohort study in two Spanish referral centres. Clin. Microbiol. Infect. 2019, 26, e1–e84. [Google Scholar] [CrossRef]
- Fragata-Filho, A.A.; França, F.F.; Fragata Cda, S.; Lourenço, A.M.; Faccini, C.C.; Costa, C.A. Evaluation of parasiticide treatment with Benznidazol in the electrocardiographic, clinical, and serological evolution of Chagas disease. PLoS Negl. Trop. Dis. 2016, 10, e0004508. [Google Scholar] [CrossRef] [PubMed]
- Losada Galván, I.; Madrid Pascual, O.; Herrero-Martínez, J.M.; Pérez-Ayala, A.; Lizasoain Hernández, M. Does progressive introduction of benznidazole reduce the chance of adverse events in the treatment of Chagas disease? Am. J. Trop. Med. Hyg. 2019, 100, 1477–1481. [Google Scholar] [CrossRef]
- Schmidt, A.; Dias Romano, M.M.; Marin-Neto, J.A.; Rao-Melacini, P.; Rassi, A., Jr.; Mattos, A.; Avezum, Á., Jr.; Villena, E.; Sosa-Estani, S.; Bonilla, R.; et al. Effects of trypanocidal treatment on echocardiographic parameters in Chagas cardiomyopathy and prognostic value of wall motion score index: A BENEFIT trial echocardiographic substudy. J. Am. Soc. Echocardiogr. 2019, 32, 286–295. [Google Scholar] [CrossRef]
- Soverow, J.; Hernandez, S.; Sanchez, D.; Forsyth, C.; Flores, C.A.; Viana, G.; Meymandi, S. Progression of baseline electrocardiogram abnormalities in Chagas patients undergoing antitrypanosomal treatment. Open Forum. Infect. Dis. 2019, 6. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. What Is a Serious Adverse Event? 2016. Available online: https://www.fda.gov/safety/reporting-serious-problems-fda/what-serious-adverse-event (accessed on 2 June 2021).
- Forsyth, C.J.; Hernandez, S.; Olmedo, W.; Abuhamidah, A.; Traina, M.I.; Sanchez, D.R.; Soverow, J.; Meymandi, S.K. Safety Profile of Nifurtimox for Treatment of Chagas Disease in the United States. Clin. Infect. Dis. 2016, 63, 1056–1062. [Google Scholar] [CrossRef] [Green Version]
- Jackson, Y.; Alirol, E.; Getaz, L.; Wolff, H.; Combescure, C.; Chappuis, F. Tolerance and safety of nifurtimox in patients with chronic chagas disease. Clin. Infect. Dis. 2010, 51, e69–e75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berenstein, A.J.; Falk, N.; Moscatelli, G.; Moroni, S.; Gonzalez, N.; Garcia-Bournissen, F.; Ballering, G.; Freilij, H.; Altcheh, J. Adverse Events Associated with Nifurtimox Treatment for Chagas Disease in Children and Adults. Antimicrob. Agents Chemother. 2021, 65. [Google Scholar] [CrossRef] [PubMed]
- Viotti, R.; Alarcon de Noya, B.; Araujo-Jorge, T.; Grijalva, M.J.; Guhl, F.; Lopez, M.C.; Ramsey, J.M.; Ribeiro, I.; Schijman, A.G.; Sosa-Estani, S.; et al. Towards a paradigm shift in the treatment of chronic Chagas disease. Antimicrob. Agents Chemother. 2014, 58, 635–639. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Lancheros, E.; Chatelain, E.; Ndao, M. Chagas disease treatment efficacy biomarkers: Myths and realities. In Chagas Disease—A Clincal Approach; Altcheh, J., Freilij, H., Eds.; Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food and Drug Administration. Highlights of Prescribing Information—Benznidazole. FDA. 2017. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/209570lbl.pdf (accessed on 2 June 2021).
- U.S. Food and Drug Administration. Highlights of Prescribing Information—Lampit (Nifurtimox). FDA. 2020. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/213464s000lbl.pdf (accessed on 2 June 2021).
- Torrico, F.; Gascon, J.; Barreira, F.; Blum, B.; Almeida, I.C.; Alonso-Vega, C.; Barboza, T.; Bilbe, G.; Correia, E.; Garcia, W.; et al. New regimens of benznidazole monotherapy and in combination with fosravuconazole for treatment of Chagas disease (BENDITA): A phase 2, double-blind, randomised trial. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Carmo Correa, D.E.D.; Maria Ayo, C.; Laguila Visentainer, J.E.; Ambrosio-Albuquerque, E.P.; Guimaraes Reis, P.; Brandao de Mattos, C.C.; Bestetti, R.B.; de Mattos, L.C.; Maria Sell, A. Human platelet antigen polymorphisms and the risk of chronic Chagas disease cardiomyopathy. Platelets 2020, 31, 272–275. [Google Scholar] [CrossRef] [PubMed]
- Ayo, C.M.; Dalalio, M.M.; Visentainer, J.E.; Reis, P.G.; Sippert, E.A.; Jarduli, L.R.; Alves, H.V.; Sell, A.M. Genetic susceptibility to Chagas disease: An overview about the infection and about the association between disease and the immune response genes. Biomed. Res. Int. 2013, 2013, 284729. [Google Scholar] [CrossRef] [PubMed]
- Bivona, A.E.; Alberti, A.S.; Cerny, N.; Trinitario, S.N.; Malchiodi, E.L. Chagas disease vaccine design: The search for an efficient Trypanosoma cruzi immune-mediated control. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165658. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | No. of Patients | Study Design | Country of Study (Main Nationalities of Participants) | Study Period | Treatment, Comparison and Dose |
|---|---|---|---|---|---|
| Alarcón de Noya, et al., 2017 [23] | 122 (92 children & 30 adults) | Cross-sectional | Venezuela (Venezuelan) | Dec. 2007–Jan. 2010 | BNZ (6 mg/kg/day) in three doses for 60 days NFX (8 mg/kg/day) for 90 days |
| Albareda, et al., 2018 [24] | 87 (Children 5–16 yoa) | Prospective cohort | Argentina (Argentinian) | 60 months (Start and end date not stated) | BNZ (5 mg/kg/day) for 60 days NFX (10 mg/kg/day) for 60 days |
| Antunes, et al., 2016 [25] | 244 (Adults ≥ 18 yoa) | Cross-sectional | Brazil (Brazilian) | 2008–2010 | Had received BNZ (n = 46; 3 removed) n = 43 ‡NT (n = 198) |
| Cardoso, et al., 2018 [26] | 1813 (Adults ≥ 18 yoa) | Cross-sectional (2013-2014 baseline) Cohort (2015–2016) † | Brazil (Brazilian) | 2013–2014 to 2015–2016 (2-year follow-up) | Had received BNZ (n = 493) NT (n = 1320) |
| Colantonio, et al., 2016 [27] | 111 (children 6–16 yoa) | Retrospective cohort | Argentina (Argentinian) | Data used from 1991-1996 RCT (median 8.6 yr. follow-up) | BNZ (5 mg/kg/day) for 60 days Placebo for 60 days |
| Crespillo-Andújar, et al., 2019 [28] | 471 (adults ≥ 18 yoa) | Prospective cohort | Spain Bolivian (97.5%), Paraguayan (1.5%), Salvadorian (0.5%), Honduran (0.5%) | Jan 2014–Mar 2018 | Had received BNZ (5mg/kg/day) for 60 days (standard dosing scheme) BNZ (escalating dose scheme) |
| Fragata-Filho, et al., 2016 [29] | 310 (Adults ≥ 18 yoa) | Retrospective cohort | Brazil (Brazilian) | Pre-2002 to 2013 (Average follow-up 19.59 years) | BNZ Treated (n = 263) 5 mg/kg/day for 60 days NT (n = 47) |
| Losada Galván, et al., 2019 [30] | 62 (adults ≥ 18 yoa) | Retrospective cohort | Spain (Bolivian (97%), Honduran (3%)) | July 2008-January 2017 | BNZ—Full dose 5 mg/kg/day for 60 days BNZ—Escalating dose |
| Morillo, et al., 2015 [20] | 2854 (adults 18–75 yoa) | RCT | Multiple countries Brazilian (47.6%), Argentinian (19.6%), Colombian (17.6%), Bolivian (12.5%), Salvadorian (2.7%) | 2004–2011 | BNZ—5 mg/kg/day for 60 days was modified in Feb. 2009 to the administration of a fixed dose of 300 mg/day and a variable duration of therapy (between 40 and 80 days) Placebo |
| Morillo, et al., 2017 [21] | 120 (adults ≥18 to ≤ 50 yoa) | RCT | Argentina (77.5%), Chile (9.1%), Spain (8.3%), Colombia, (5%), Guatemala, (5%), Mexico (5%) | 27 July 2011–24 Dec. 2013 | (1) POS 400 mg b.i.d. (2) BNZ 200 mg + placebo b.i.d. (3) BNZ 200 mg b.i.d. + POS 400 mg b.i.d. (4) Placebo 10 mg b.i.d. |
| Schmidt, et al., 2019 [31] | 1508 (adults 18–75 yoa) | Prospective sub study | Multiple Brazilian, (46.3%), Colombian, (22.3%), Argentinian, (19.2%), Bolivian (9.5%), Salvadorian (2,8%) | 2004–2011 | BNZ (5mg/kg/day) for 60 days or a modified regimen Placebo |
| Soverow, et al., 2019 [32] | 89 (adults 18–60 yoa) | Prospective cohort | USA (Latin American Immigrants; nationalities not specified) | 2008–2014 | Dependent upon drug availability BNZ—5 mg/kg/day for 60 days (n = 18) NFX—8–10 mg/kg/day in three daily doses for 12 weeks (n = 41) |
| Torrico, et al., 2018 [22] | 231 (adults ≥18 to ≤50 yoa) | RCT | Bolivia (Bolivian) | 19 July 2011–13 June 2013 | (1) High-dose E1224 (2) Short-dose E1224 (3) Low-dose E1224 (4) BNZ (5) Placebo |
| Infection-Related Efficacy (Randomized Controlled Trials) | ||
| Study | ||
| Morillo, et al., 2015 [20] | End of treatment PCR conversion rate: BNZ 66.2% and PLA 33.5% | 2-year conversion rate: BNZ 55.4% and PLA 35.3% 5-year conversion rate: BNZ 46.7% and PLA 33.1% (p < 0.001 for all comparisons). |
| Morillo, et al., 2017 [21] | RT-PCR conversion rate at 30 & 60 days: POS 93% & 90%, POS + BNZ 88.9% & 92.3%, and BNZ 89.7% & 89.3% (p < 0.001 for all compared to PLA) | 360 day conversion was only sustained in BNZ or BNZ + POS compared with PLA and POS |
| Torrico, et al., 2018 [22] | End of treatment parasite clearance (PCR) (65 days): PLA 26%, LD 90%, SD 89%, HD 76% and BNZ 91% (p < 0.001 for all compared to PLA) | Sustained clearance at 12 months: PLA 9%, LD 8%, SD 11%, HD 29% and BNZ 82% (p < 0.0001) |
| At 12 months follow-up analysis with conventional ELISA found no statistical difference trypanocidals and placebo | At 12 months follow-up there was a small but significant reduction in trypanolytic anti-α-gal antibodies comparing BNZ to placebo, (9% BNZ seroconverted vs. 4% of PLA) measured by CL-ELISA (p = 0.049) | |
| Infection-Related Efficacy (Observational Studies) | ||
| Alarcón de Noya, et al., 2017 [23] | Negative PCR conversion at follow-up (25 months): BNZ 9/10 (90%), NFX 59/112 (52.7%) | |
| Albareda, et al., 2018 [24] | Seroreversion ‡ at end of follow-up: BNZ 9/45 (20%), NFX 1/7 (14.29%) | |
| Antunes, et al., 2016 [25] | BNZ of ≤ 60 days and BNZ >60 days were both more efficacious than no treatment in reducing parasite load (via PCR), but no statistical differences were found between both treatments | |
| Patient-Related Efficacy (RCTs) | |
| Morillo et al., 2015 [20] | No significant between-group differences were observed in any component of the primary outcome No significant differences between groups with new ECG abnormalities Treatment with BNZ did not reduce cardiac clinical progression |
| Torrico et al., 2018 [22] | ECG outcomes were similar across treatment groups, with no clinically significant increases in QTcF during treatment. |
| Patient-Related Efficacy (Observational Studies) | |
| Antunes et al., 2016 [25] | No cardiac alterations were detected in the study population, regardless of group |
| Cardoso et al., 2018 [26] | 14/493 (2.8%) of the treated group died during the 2-year follow-up; 100/1320 (7.6%) of the control group died during the 2-year follow-up (p ≤ 0.001) There was a reduction in well-established markers of CD severity, such as typical ECG abnormalities, high NT-proBNP levels or both. BNZ treatment reduced NT-proBNP levels. |
| Colantonio et al., 2016 [27] | After statistical adjustment treatment with BNZfor 60 days was not associated with less ECG abnormalities as compared to no treatment over a median follow-up of 8.6 years. The prevalence of ECGs with abnormalities was higher among children treated with BNZ compared with those not treated in all assessment periods following the baseline evaluation. |
| Fragata-Filho et al., 2016 [29] | 20.92% of the treated patients developed ECG alterations. 3.19% of the untreated patients had worsening of ECG alterations. (p ≤ 0.0001) Death related to CD occurred in five participants with ECG alterations and in one with a normal ECG. (p = 0.001) |
| Schmidt et al., 2019 [31] | Those with even minimal wall motion abnormalities have poorer long-term outcomes. LV WMSI>1 was associated with a significantly increased primary outcome event rate and higher all-cause mortality (p ≤ 0.0001). BNZ had no significant effects on echocardiographic progression of CCC over 5.4 years. |
| Soverow, et al., 2019 [32] | Treated patients were less likely to have progression of their ECG disease (OR = 0.13, p < 0.001). Untreated patients had a higher likelihood of developing ECG abnormalities compared with their treated counterparts (56.7% vs. 11.9%, p ≤ 0.001). |
| Children NFX | Adults NFX | Statistical Significance |
|---|---|---|
| General: 75.3% [64/85] Gastrointestinal: 57.6% [46/85] Neurological: 35.3% [30/85] | General: 82.1% [23/28] Gastrointestinal: 60.7% [17/28] Neurological: 85.7% [24/28] | p = 0.455 p = 0.775 p = 0.000 |
| Children BNZ | Adults BNZ | Statistical significance |
| General: 43.5% [20/26] Gastrointestinal: 21.7% [10/26] Neurological: 17.4% [8/28] | General: 11.7% [2/17] Gastrointestinal: 41.2% [7/17] Neurological: 52.9% [9/17] | p = 0.020 p = 0.123 p = 0.005 |
| Statistical significance between NFX and BNZ General: p = 0.001 Gastrointestinal: p = 0.000 Neurological: p = 0.007 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malone, C.J.; Nevis, I.; Fernández, E.; Sanchez, A. A Rapid Review on the Efficacy and Safety of Pharmacological Treatments for Chagas Disease. Trop. Med. Infect. Dis. 2021, 6, 128. https://doi.org/10.3390/tropicalmed6030128
Malone CJ, Nevis I, Fernández E, Sanchez A. A Rapid Review on the Efficacy and Safety of Pharmacological Treatments for Chagas Disease. Tropical Medicine and Infectious Disease. 2021; 6(3):128. https://doi.org/10.3390/tropicalmed6030128
Chicago/Turabian StyleMalone, Cody J, Immaculate Nevis, Eduardo Fernández, and Ana Sanchez. 2021. "A Rapid Review on the Efficacy and Safety of Pharmacological Treatments for Chagas Disease" Tropical Medicine and Infectious Disease 6, no. 3: 128. https://doi.org/10.3390/tropicalmed6030128
APA StyleMalone, C. J., Nevis, I., Fernández, E., & Sanchez, A. (2021). A Rapid Review on the Efficacy and Safety of Pharmacological Treatments for Chagas Disease. Tropical Medicine and Infectious Disease, 6(3), 128. https://doi.org/10.3390/tropicalmed6030128