
Epidemiological Situation of Monkeypox Transmission by Possible Sexual Contact: A Systematic Review

 ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategy
2.4. Study Selection
2.5. Outcomes
2.6. Data Collection Process and Data Items
3. Results
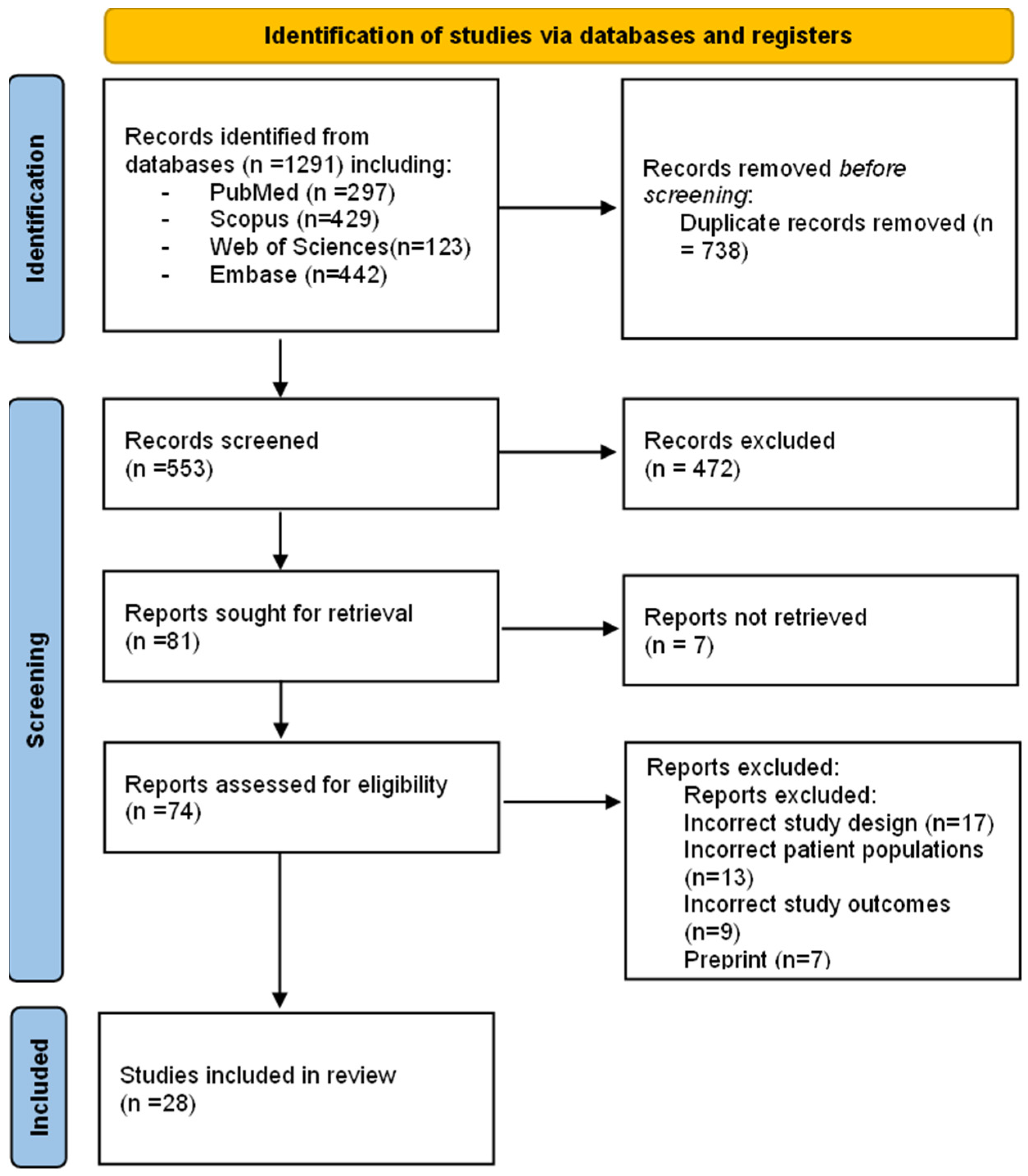
3.1. Study Selection
3.2. Study Characteristics
3.3. Demographical Characteristics and Diagnostic Method for Monkeypox
3.4. Clinical Manifestations, Localization of Skin Lesions and Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox-A potential threat? A systematic review. PLoS Negl Trop Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- Dhawan, M.; Bin Emran, T.; Islam, F. The Resurgence of Monkeypox Cases: Reasons, Threat Assessment, And Possible Preventive Measures. Travel Med. Infect. Dis. 2022, 49, 102367. [Google Scholar] [CrossRef]
- Monkeypox, n.d. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 29 June 2022).
- Monkeypox Outbreak Global Map|Monkeypox|Poxvirus|CDC n.d. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html?fbclid=IwAR1JReLa6ZZivFHO0JDDfBFjZ5xMn-fDtkdHtcmdlcqM6t1EqGfSYR9NMWM (accessed on 29 June 2022).
- Multi-Country Outbreak of Monkeypox, External Situation Report #1–6 July 2022-World|ReliefWeb n.d. Available online: https://reliefweb.int/report/world/multi-country-outbreak-monkeypox-external-situation-report-1-6-july-2022 (accessed on 7 July 2022).
- Gong, Q.; Wang, C.; Chuai, X.; Chiu, S. Monkeypox virus: A re-emergent threat to humans. Virol Sin. 2022, 37, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Mileto, D.; Riva, A.; Cutrera, M.; Moschese, D.; Mancon, A.; Meroni, L.; Giacomelli, A.; Bestetti, G.; Rizzardini, G.; Gismondo, M.R.; et al. New Challenges in Human Monkeypox Outside Africa: A Review and Case Report from Italy. Travel Med. Infect. Dis. 2022, 49, 102386. [Google Scholar] [CrossRef]
- Antinori, A.; Mazzotta, V.; Vita, S.; Carletti, F.; Tacconi, D.; Lapini, L.E.; D’Abramo, A.; Cicalini, S.; Lapa, D.; Pittalis, S.; et al. Epidemiological, Clinical and Virological Characteristics of Four Cases of Monkeypox Support Transmission Through Sexual Contact, Italy, May 2022. Eurosurveillance 2022, 27, 2200421. [Google Scholar] [CrossRef]
- Moore, M.; Zahra, F. Monkeypox. In StatPearls; StatPearls: Tampa, FL, USA, 2022. [Google Scholar]
- Bonilla-Aldana, D.K.; Rodrigue-Morales, A.J. Is Monkeypox Another Reemerging Viral Zoonosis with Many Animal Hosts Yet to Be Defined? Veter-Q. 2022, 42, 148–150. [Google Scholar] [CrossRef]
- Mauldin, M.R.; McCollum, A.M.; Nakazawa, Y.J.; Mandra, A.; Whitehouse, E.R.; Davidson, W.; Zhao, H.; Gao, J.; Li, Y.; Doty, J.; et al. Exportation of Monkeypox Virus from the African Continent. J. Infect. Dis. 2020, 225, 1367–1376. [Google Scholar] [CrossRef] [PubMed]
- León-Figueroa, D.A.; Bonilla-Aldana, D.K.; Pachar, M.; Romaní, L.; Saldaña-Cumpa, H.M.; Anchay-Zuloeta, C.; Diaz-Torres, M.; Franco-Paredes, C.; Suárez, J.A.; Ramirez, J.D.; et al. The Never-Ending Global Emergence of Viral Zoonoses After COVID-19? The Rising Concern of Monkeypox in Europe, North America and beyond. Travel Med. Infect. Dis. 2022, 49, 102362. [Google Scholar] [CrossRef]
- Diseases, T.L.I. Monkeypox: A Neglected Old Foe. Lancet Infect. Dis. 2022, 22, 913. [Google Scholar] [CrossRef]
- Amao, L.K.; Olatunji, D.I.; Igbodo, G.; Okoli, S.C.; Amaechi, I.; Goni, M.I.; Ehiakhamen, O.; Aderinola, O.; Ogunleye, A.; Ogunbode, O.; et al. Trend and enhanced surveillance of Monkeypox during COVID-19 pandemic in Nigeria. J. Public Health Afr. 2022, 13, 2184. [Google Scholar] [CrossRef]
- Saxena, S.K.; Ansari, S.; Maurya, V.K.; Kumar, S.; Jain, A.; Paweska, J.T.; Tripathi, A.K.; Abdel-Moneim, A.S. Re-Emerging Human Monkeypox: A Major Public-Health Debacle. J. Med. Virol. 2022, 1. [Google Scholar] [CrossRef]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.; Duncan, C.J.; et al. Clinical Features and Management of Human Monkeypox: A Retrospective Observational Study in the UK. Lancet Infect. Dis. 2022, 22, 1153–1162. [Google Scholar] [CrossRef]
- Huhn, G.D.; Bauer, A.M.; Yorita, K.; Graham, M.B.; Sejvar, J.; Likos, A.; Damon, I.K.; Reynolds, M.; Kuehnert, M.J. Clinical Characteristics of Human Monkeypox, and Risk Factors for Severe Disease. Clin. Infect. Dis. 2005, 41, 1742–1751. [Google Scholar] [CrossRef] [PubMed]
- Jezek, Z.; Grab, B.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M. Clinico-Epidemiological Features of Monkeypox Patients with an Animal or Human Source of Infection. Bull. World Health Organ. 1988, 66, 459–464. [Google Scholar] [PubMed]
- Xiang, Y.; White, A. Monkeypox Virus Emerges from the Shadow of Its More Infamous Cousin: Family Biology Matters. Emerg. Microbes Infect. 2022, 11, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Peter, O.J.; Kumar, S.; Kumari, N.; Oguntolu, F.A.; Oshinubi, K.; Musa, R. Transmission Dynamics of Monkeypox Virus: A Mathematical Modelling Approach. Model. Earth Syst. Environ. 2021, 8, 3423–3434. [Google Scholar] [CrossRef]
- Kumar, N.; Acharya, A.; Gendelman, H.E.; Byrareddy, S.N. The 2022 Outbreak and the Pathobiology of the Monkeypox Virus. J. Autoimmun. 2022, 131, 102855. [Google Scholar] [CrossRef] [PubMed]
- Minhaj, F.S.; Ogale, Y.P.; Whitehill, F.; Schultz, J.; Foote, M.; Davidson, W.; Hughes, C.M.; Wilkins, K.; Bachmann, L.; Chatelain, R.; et al. Monkeypox Outbreak—Nine States, May 2022. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 764–769. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Lopardo, G. Monkeypox: Another Sexually Transmitted Infection? Pathogens 2022, 11, 713. [Google Scholar] [CrossRef]
- Farahat, R.A.; Abdelaal, A.; Shah, J.; Ghozy, S.; Sah, R.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J.; McHugh, T.D.; Leblebicioglu, H. Monkeypox Outbreaks During COVID-19 Pandemic: Are We Looking at An Independent Phenomenon or an Overlapping Pandemic? Ann. Clin. Microbiol. Antimicrob. 2022, 21, 1–3. [Google Scholar] [CrossRef]
- Rao, A.K.; Petersen, B.W.; Whitehill, F.; Razeq, J.H.; Isaacs, S.N.; Merchlinsky, M.J.; Campos-Outcalt, D.; Morgan, R.L.; Damon, I.; Sánchez, P.J.; et al. Use of JYNNEOS (Smallpox and Monkeypox Vaccine, Live, Nonreplicating) for Preexposure Vaccination of Persons at Risk for Occupational Exposure to Orthopoxviruses: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 734–742. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Bížová, B.; Veselý, D.; Trojánek, M.; Rob, F. Coinfection of Syphilis and Monkeypox in HIV Positive Man in Prague, Czech Republic. Travel Med. Infect. Dis. 2022, 49, 102368. [Google Scholar] [CrossRef]
- Patrocinio-Jesus, R.; Peruzzu, F. Monkeypox Genital Lesions. N. Engl. J. Med. 2022, 387, 66. [Google Scholar] [CrossRef]
- Basgoz, N.; Brown, C.M.; Smole, S.C.; Madoff, L.C.; Biddinger, P.D.; Baugh, J.J.; Shenoy, E.S. Case 24-2022: A 31-Year-Old Man with Perianal and Penile Ulcers, Rectal Pain, and Rash. N. Engl. J. Med. 2022, 387, 547–556. [Google Scholar] [CrossRef]
- Heskin, J.; Belfield, A.; Milne, C.; Brown, N.; Walters, Y.; Scott, C.; Bracchi, M.; Moore, L.S.; Mughal, N.; Rampling, T.; et al. Transmission of Monkeypox Virus Through Sexual Contact—A Novel Route of Infection. J. Infect. 2022, 85, 334–363. [Google Scholar] [CrossRef] [PubMed]
- Hammerschlag, Y.; MacLeod, G.; Papadakis, G.; Sanchez, A.A.; Druce, J.; Taiaroa, G.; Savic, I.; Mumford, J.; Roberts, J.; Caly, L.; et al. Monkeypox Infection Presenting as Genital Rash, Australia, May 2022. Eurosurveillance 2022, 27, 2200411. [Google Scholar] [CrossRef] [PubMed]
- Vivancos, R.; Anderson, C.; Blomquist, P.; Balasegaram, S.; Bell, A.; Bishop, L.; Brown, C.S.; Chow, Y.; Edeghere, O.; Florence, I.; et al. Community Transmission of Monkeypox in the United Kingdom, April to May 2022. Eurosurveillance 2022, 27, 2200422. [Google Scholar] [CrossRef] [PubMed]
- Duque, M.P.; Ribeiro, S.; Martins, J.V.; Casaca, P.; Leite, P.P.; Tavares, M.; Mansinho, K.; Duque, L.M.; Fernandes, C.; Cordeiro, R.; et al. Ongoing Monkeypox Virus Outbreak, Portugal, 29 April to 23 May 2022. Eurosurveillance 2022, 27, 2200424. [Google Scholar] [CrossRef]
- Vallée, A.; Farfour, E.; Zucman, D. Monkeypox Virus: A Novel Sexually Transmitted Disease? A Case Report from France. Travel Med. Infect. Dis. 2022, 49, 102394. [Google Scholar] [CrossRef] [PubMed]
- Oprea, C.; Ianache, I.; Piscu, S.; Tardei, G.; Nica, M.; Ceausu, E.; Popescu, C.P.; Florescu, S.A. First Report of Monkeypox in a Patient Living with HIV From Romania. Travel Med. Infect. Dis. 2022, 49, 102395. [Google Scholar] [CrossRef]
- Girometti, N.; Byrne, R.; Bracchi, M.; Heskin, J.; McOwan, A.; Tittle, V.; Gedela, K.; Scott, C.; Patel, S.; Gohil, J.; et al. Demographic and Clinical Characteristics of Confirmed Human Monkeypox Virus Cases in Individuals Attending a Sexual Health Centre in London, UK: An Observational Analysis. Lancet Infect. Dis. 2022, 22, 1321–1328. [Google Scholar] [CrossRef]
- Noe, S.; Zange, S.; Seilmaier, M.; Antwerpen, M.H.; Fenzl, T.; Schneider, J.; Spinner, C.D.; Bugert, J.J.; Wendtner, C.-M.; Wölfel, R. Clinical and Virological Features of First Human Monkeypox Cases in Germany. Infection 2022, 1–6. [Google Scholar] [CrossRef]
- Jang, Y.R.; Lee, M.; Shin, H.; Kim, J.-W.; Choi, M.-M.; Kim, Y.M.; Kim, J.; Na, H.K. The First Case of Monkeypox in the Republic of Korea. J. Korean Med. Sci. 2022, 37. [Google Scholar] [CrossRef]
- Maronese, C.A.; Beretta, A.; Avallone, G.; Boggio, F.L.; Marletta, D.A.; Murgia, G.; Cusini, M.; Gori, A.; Carrera, C.G.; Di Benedetto, A.; et al. Clinical, Dermoscopic and Histopathological Findings in Localized Human Monkeypox: A Case from Northern Italy. Br. J. Dermatol. 2022, 10, 1342. [Google Scholar] [CrossRef]
- Peiró-Mestres, A.; Fuertes, I.; Camprubí-Ferrer, D.; Marcos, M.; Vilella, A.; Navarro, M.; Rodriguez-Elena, L.; Riera, J.; Català, A.; Martínez, M.J.; et al. Frequent Detection of Monkeypox Virus DNA In Saliva, Semen, And Other Clinical Samples From 12 Patients, Barcelona, Spain, May to June 2022. Eurosurveillance 2022, 27, 2200503. [Google Scholar] [CrossRef]
- Martínez, J.I.; Gil Montalbán, E.; Bueno, S.J.; Martínez, F.M.; Juliá, A.N.; Díaz, J.S.; Marín, N.G.; Deorador, E.C.; Forte, A.N.; García, M.A.; et al. Monkeypox Outbreak Predominantly Affecting Men Who Have Sex with Men, Madrid, Spain, 26 April to 16 June 2022. Eurosurveillance 2022, 27, 2200471. [Google Scholar] [CrossRef] [PubMed]
- Selb, R.; Werber, D.; Falkenhorst, G.; Steffen, G.; Lachmann, R.; Ruscher, C.; McFarland, S.; Bartel, A.; Hemmers, L.; Koppe, U.; et al. A Shift from Travel-Associated Cases to Autochthonous Transmission with Berlin as Epicentre of the Monkeypox Outbreak in Germany, May to June 2022. Eurosurveillance 2022, 27, 2200499. [Google Scholar] [CrossRef] [PubMed]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical Presentation and Virological Assessment of Confirmed Human Monkeypox Virus Cases in Spain: A Prospective Observational Cohort Study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef]
- Ogoina, D.; Yinka-Ogunleye, A. Sexual history of human monkeypox patients seen at a tertiary hospital in Bayelsa, Nigeria. Int. J. STD AIDS 2022, 2022, 095646242211193. [Google Scholar] [CrossRef]
- Orviz, E.; Negredo, A.; Ayerdi, O.; Vázquez, A.; Muñoz-Gomez, A.; Monzón, S.; Clavo, P.; Zaballos, A.; Vera, M.; Sánchez, P.; et al. Monkeypox outbreak in Madrid (Spain): Clinical and virological aspects. J. Infect. 2022. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Bilinska, J.; Tam, J.C.H.; Fontoura, D.D.S.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C.; et al. Clinical Features and Novel Presentations of Human Monkeypox in a Central London Centre During the 2022 Outbreak: Descriptive Case Series. BMJ 2022, 378, e072410. [Google Scholar] [CrossRef]
- Pfäfflin, F.; Wendisch, D.; Scherer, R.; Jürgens, L.; Godzick-Njomgang, G.; Tranter, E.; Tober-Lau, P.; Stegemann, M.S.; Corman, V.M.; Kurth, F.; et al. Monkeypox In-Patients with Severe Anal Pain. Infection 2022, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Philpott, D.; Hughes, C.M.; Alroy, K.A.; Kerins, J.L.; Pavlick, J.; Asbel, L.; Crawley, A.; Newman, A.P.; Spencer, H.; Feldpausch, A.; et al. Epidemiologic and Clinical Characteristics of Monkeypox Cases—United States, May 17 July 22, 2022. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 1018–1022. [Google Scholar] [CrossRef]
- Raccagni, A.R.; Candela, C.; Mileto, D.; Canetti, D.; Bruzzesi, E.; Rizzo, A.; Castagna, A.; Nozza, S. Monkeypox infection among men who have sex with men: PCR testing on seminal fluids. J. Infect. 2022. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, B.S.; Herrador, B.R.G.; Franco, A.D.; Fariñas, M.P.S.-S.; Valero, J.D.A.; Llorente, A.H.A.; de Agreda, J.P.A.P.; Malonda, R.C.; Castrillejo, D.; López, M.D.C.; et al. Epidemiologic Features and Control Measures during Monkeypox Outbreak, Spain, June 2022-Volume 28, Number 9—September 2022-Emerging Infectious Diseases journal-CDC. Emerg. Infect. Dis. 2022, 5, 6. [Google Scholar] [CrossRef]
- Vusirikala, A.; Charles, H.; Balasegaram, S.; Macdonald, N.; Kumar, D.; Barker-Burnside, C.; Cumiskey, K.; Dickinson, M.; Watson, M.; Olufon, O.; et al. Epidemiology of Early Monkeypox Virus Transmission in Sexual Networks of Gay and Bisexual Men, England, 2022-Volume 28, Number 10—October 2022-Emerging Infectious Diseases journal-CDC n.d. Emerg. Infect. Dis. 2022, 28. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Kong, J.D.; Mahroum, N.; Tsigalou, C.; Khamisy-Farah, R.; Converti, M.; Wu, J. Epidemiological Trends and Clinical Features of the Ongoing Monkeypox Epidemic: A Preliminary Pooled Data Analysis and Literature Review. J. Med. Virol. 2022. [Google Scholar] [CrossRef]
- Zambrano, P.G.; Acosta-España, J.D.; Moyano, F.M.; Jara, J.B.A. Sexually or intimately transmitted infections: A look at the current outbreak of monkeypox in 2022. Travel Med. Infect. Dis. 2022, 49, 102383. [Google Scholar] [CrossRef] [PubMed]
- Kupferschmidt, K. Why monkeypox is mostly hitting men who have sex with men. Science 2022, 376, 1364–1365. [Google Scholar] [CrossRef] [PubMed]
- Multi-country outbreak of monkeypox-External Situation Report 4, published 24 August 2022-World|ReliefWeb n.d. Available online: https://reliefweb.int/report/world/multi-country-outbreak-monkeypox-external-situation-report-4-published-24-august-2022 (accessed on 25 August 2022).
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.; Kantele, A.; Koopmans, M.; Asogun, D.; Yinka-Ogunleye, A.; Ihekweazu, C.; Zumla, A. Human Monkeypox: Epidemiologic and Clinical Characteristics, Diagnosis, and Prevention. Infect. Dis. Clin. N. Am. 2019, 33, 1027–1043. [Google Scholar] [CrossRef]
- Brockmeyer, N. As Monkeypox Goes Sexual: A Public Health Perspective. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1164–1166. [Google Scholar] [CrossRef]
- Matusali, G.; D’Abramo, A.; Terrosi, C.; Carletti, F.; Colavita, F.; Vairo, F.; Savellini, G.G.; Gandolfo, C.; Anichini, G.; Lalle, E.; et al. Infectious Toscana Virus in Seminal Fluid of Young Man Returning from Elba Island, Italy. Emerg. Infect. Dis. 2022, 28, 865–869. [Google Scholar] [CrossRef]
- Li, Y.; Olson, V.A.; Laue, T.; Laker, M.T.; Damon, I.K. Detection of Monkeypox Virus with Real-Time PCR assays. J. Clin. Virol. 2006, 36, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Shchelkunov, S.; Gavrilova, E.; Babkin, I. Multiplex PCR Detection and Species Differentiation of Orthopoxviruses Pathogenic to Humans. Mol. Cell. Probes 2005, 19, 1–8. [Google Scholar] [CrossRef]
- Kulesh, D.A.; Loveless, B.M.; Norwood, D.A.; Garrison, J.; Whitehouse, C.A.; Hartmann, C.; Mucker, E.; Miller, D.; Wasieloski, L.P.; Huggins, J.W.; et al. Monkeypox Virus Detection in Rodents Using Real-Time 3′-Minor Groove Binder Taqman® Assays on the Roche LightCycler. Lab. Investig. 2004, 84, 1200–1208. [Google Scholar] [CrossRef]
- Olson, V.A.; Laue, T.; Laker, M.T.; Babkin, I.V.; Drosten, C.; Shchelkunov, S.; Niedrig, M.; Damon, I.K.; Meyer, H. Real-Time PCR System for Detection of Orthopoxviruses and Simultaneous Identification of Smallpox Virus. J. Clin. Microbiol. 2004, 42, 1940–1946. [Google Scholar] [CrossRef]
- Shchelkunov, S.N.; Shcherbakov, D.N.; Maksyutov, R.A.; Gavrilova, E.V. Species-Specific Identification of Variola, Monkeypox, Cowpox, And Vaccinia Viruses by Multiplex Real-Time PCR Assay. J. Virol. Methods 2011, 175, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.; Abdelaal, A.; Reda, A.; Brakat, A.; Lashin, B.; Abdelazeem, B.; Mohanty, A.; Rodriguez-Morales, A. Monkeypox Viral Detection in Semen Specimens of Confirmed Cases: A Systematic Review and Meta-Analysis. 2022. Available online: https://www.researchsquare.com/article/rs-1970704/v1 (accessed on 28 July 2022).
- Koenig, K.L.; Beÿ, C.K.; Marty, A.M. Monkeypox 2022 Identify-Isolate-Inform: A 3I Tool for Frontline Clinicians for a Zoonosis with Escalating Human Community Transmission. One Health 2022, 15, 100410. [Google Scholar] [CrossRef]
- Patauner, F.; Gallo, R.; Durante-Mangoni, E. Monkeypox Infection: An Update for the Practicing Physician. Eur. J. Intern. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Abdelmoez Farahat, R.; Sah, R.; El-Sakka, A.A.; Yasmine Benmelouka, A.; Kundu, M.; Labieb, F.; Sameh Shaheen, R.; Abdelaal, A.; Abdelazeem, B.; Bonilla-Aldana, D.K.; et al. Human Mon-Keypox Disease (MPX). InfezMed 2022, 13, 1–44. [Google Scholar]


{kind=link}
| Base | Search Strategy |
|---|---|
| PUBMED | #1 (“Monkeypox” OR “Monkey Pox”) #2 (“sexual contact” OR “sexual intercourse” OR “sexual behavior” OR “transmission” OR “sexual transmission” OR “Sexual Intercourse” OR “Intercourse, Sexual” OR Coital OR Copulation OR “Sexual relations”) #3 = #1 AND #2 |
| SCOPUS | #1 TITLE-ABS-KEY (“Monkeypox” OR “Monkey Pox”) #2 TITLE-ABS-KEY (“sexual contact” OR “sexual intercourse” OR “sexual behavior” OR “transmission” OR “sexual transmission” OR “Sexual Intercourse” OR “Intercourse, Sexual” OR Coital OR Copulation OR “Sexual relations”) #3 = #1 AND #2 |
| WEB OF SCIENCE | #1 ALL = (“Monkeypox” OR “Monkey Pox”) #2 ALL = (“sexual contact” OR “sexual intercourse” OR “sexual behavior” OR “transmission” OR “sexual transmission” OR “Sexual Intercourse” OR “Intercourse, Sexual” OR Coital OR Copulation OR “Sexual relations”) #3 = #1 AND #2 |
| EMBASE | #1 ‘monkeypox’/exp OR ‘monkeypox’ OR ‘monkeypox virus’/exp OR ‘monkeypox virus’ #2 ‘sexual contact’ OR ‘sexual behavior’ OR transmission OR ‘sexual transmission’ OR ‘sexual intercourse’ OR ‘intercourse, sexual’ OR coital OR copulation OR ‘sexual relations’ #3 = #1 AND #2 |
| Authors | Year | Design | Country | Number of Cases (N) | Cases by Sexual Contact (N) | Age (Years) | Sex (M/F) | Sexual Behavior | Previous STIs | HIV | Recent Sexual Exposure | Diagnostic Method for Monkeypox |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antinori, A. et al. [8] | 2022 | Case reports | Italy | 4 | 1 | Median: 30 | M | MSM | Hepatitis C, syphilis | Positive | Yes | RT-PCR |
| 2 | M | MSM | Syphilis | Negative | Yes | RT-PCR | ||||||
| 3 | M | MSM | Syphilis, hepatitis B | Positive | Yes | RT-PCR | ||||||
| 4 | M | MSM | Hepatitis A | Negative | Yes | RT-PCR | ||||||
| Heskin, J. et al. [31] | 2022 | Case reports | United Kingdom | 2 | 1 | NR | M | MSM | None | Negative | Yes | RT-PCR |
| 2 | NR | M | MSM | None | Positive | Yes | RT-PCR | |||||
| Hammerschlag, Y. et al. [32] | 2022 | Case report | Australia | 1 | 1 | 30 | M | MSM | Syphilis | Positive | Yes | RT-PCR |
| Minhaj, F.S. et al. [22] | 2022 | Case reports | United States | 17 | 16 | Median 40 (28–61) | NR | GBMSM | NR | NR | Yes | RT-PCR |
| Vivancos, R. et al. [33] | 2022 | Case reports | United Kingdom | 86 | 66 | Median: 38 (32–43) | M (79/79) | GBMSM (66/79) | NR | NR | Yes | RT-PCR |
| Perez Duque, M. et al. [34] | 2022 | Case reports | Portugal | 27 | 27 | Median: 33 (22–51) | M | MSM (18/19), MSW (1/19) | NR | Positive (n = 14) | Yes | RT-PCR |
| Vallée, A. et al. [35] | 2022 | Case report | France | 1 | 1 | NR | M | MSM | HIV | Positive | Yes | RT-PCR |
| Oprea, C. et al. [36] | 2022 | Case report | Romania | 1 | 1 | 26 | M | MSM | HIV | Positive | Yes | RT-PCR |
| Bížová, B. et al. [28] | 2022 | Case report | Czech Republic | 1 | 1 | 34 | M | MSM | Syphilis | Positive | Yes | RT-PCR |
| Patrocinio-Jesus, R. et al. [29] | 2022 | Case report | Portugal | 1 | 1 | 31 | M | MSM | HIV | Positive | Yes | RT-PCR |
| Basgoz, S.N. et al. [30] | 2022 | Case report | United States | 1 | 1 | 31 | M | MSM | Syphilis, herpes simplex | Negative | Yes | RT-PCR |
| Mileto, D. et al. [7] | 2022 | Case report | Italy | 1 | 1 | 33 | M | MSM | HIV | Positive | Yes | RT-PCR |
| Girometti, N. et al. [37] | 2022 | Cohort study | United Kingdom | 54 | 54 | Median: 41 (34–45) | M | MSM | HIV (n = 13) syphilis (n = 14), herpes simplex (n = 24) and gonorrhea (n = 13) | Positive | Yes | RT-PCR |
| Noe, S. et al. [38] | 2022 | Case report | Germany | 2 | 1 | 26 | M | MSM | HIV | Positive | Yes | RT-PCR |
| 2 | 32 | M | MSM | NR | NR | NR | RT-PCR | |||||
| Jang, Y.R. et al. [39] | 2022 | Case report | Korea | 1 | 1 | 34 | M | MSM | None | NR | NR | RT-PCR |
| Maronese, C.A. et al. [40] | 2022 | Case report | Italy | 1 | 1 | 44 | M | MSM | Hepatitis C, HIV, syphilis | Positive | Yes | RT-PCR |
| Peiró-Mestres, A. et al. [41] | 2022 | Case report | Spain | 12 | 1 | 30 | M | MSM | None | Positive (n = 4) | Yes | RT-PCR |
| 2 | 30 | M | MSM | Syphilis | Yes | RT-PCR | ||||||
| 3 | 40 | M | MSM | None | Yes | RT-PCR | ||||||
| 4 | 40 | M | MSM | None | Yes | RT-PCR | ||||||
| 5 | 40 | M | MSM | None | Yes | RT-PCR | ||||||
| 6 | 30 | M | MSM | None | Yes | RT-PCR | ||||||
| 7 | 40 | M | MSM | None | Yes | RT-PCR | ||||||
| 8 | 50 | M | MSM | Syphilis | Yes | RT-PCR | ||||||
| 9 | 40 | M | MSM | None | Yes | RT-PCR | ||||||
| 10 | 30 | M | MSM | None | Yes | RT-PCR | ||||||
| 11 | 30 | M | MSM | None | Yes | RT-PCR | ||||||
| 12 | 30 | M | MSM | Chlamydia y gonorrhea | Yes | RT-PCR | ||||||
| Iñigo Martínez, J. et al. [42] | 2022 | Case report | Spain | 508 | 427 | Median: 35 (18–67) | M (n = 503) F (n = 5) | MSM (n = 397) | NR | Positive (n = 225) | Yes | RT-PCR |
| Selb, R. et al. [43] | 2022 | Case report | Germany | 521 | 349 | Median: 38 (32–44) | M | MSM (n = 349) | NR | NR | Yes | RT-PCR |
| Tarín-Vicente, E.J. et al. [44] | 2022 | Cohort study | Spain | 181 | 181 | Median: 37 (31–42) | M (n = 175) F (n = 6) | MSM (n = 166) MSW (n = 15) | HIV (n = 72) | Positive | Yes | RT-PCR |
| Ogoina, D. et al. [45] | 2022 | Cross-sectional study | Nigeria | 16 | 16 | Median: 28 (22–43) | M (n = 12)F (n = 4) | MSW (n = 16) | HIV (n = 3) | Positive (n = 3) | Yes | RT-PCR |
| Orviz, E. et al. [46] | 2022 | Observational study | Spain | 48 | 48 | Median: 35 (29–44) | M | MSM (n = 42) | HIV (n = 19) | Positive (n = 19) | Yes | RT-PCR |
| Patel, A. et al. [47] | 2022 | Case report | United Kingdom | 197 | 197 | Median: 38 (32–42) | M | MSM | HIV (n = 70) | Positive (n = 70) | Yes | RT-PCR |
| Pfäfflin, F. et al. [48] | 2022 | Case report | Germany | 1 | 1 | Range (41–50) | M | MSM | None | Positive | Yes | RT-PCR |
| 2 | 2 | Range (21–30) | M | MSM | None | Negative | Yes | RT-PCR | ||||
| 3 | 3 | Range (31–40) | M | MSM | None | Negative | Yes | RT-PCR | ||||
| 4 | 4 | Range (31–40) | M | MSM | Syphilis (blood), gonorrhea (rectal) | Negative | Yes | RT-PCR | ||||
| 5 | 5 | Range (21–30) | M | MSM | Gonorrhea, Ureaplasma, Mycoplasma hominis (all urethral) | Negative | Yes | RT-PCR | ||||
| 6 | 6 | Range (31–40) | M | MSM | Gonorrhea (rectal) | Positive | Yes | RT-PCR | ||||
| Philpott, D. et al. [49] | 2022 | Case report | United States | 1195 | 1123 | Median: 35 (30–41) | M (n = 1178) F (n = 5) | MSM | HIV (n = 490) | Positive (n = 490) | Yes | RT-PCR |
| Raccagni, A.R. et al. [50] | 2022 | Case report | Italy | 36 | 36 | Median: 41.5 (31.25–35.5) | M | MSM | HIV (n = 15) | Positive (n = 15) | Yes | RT-PCR |
| Rodríguez, B.S. et al. [51] | 2022 | Case report | Spain | 1256 | 1256 | Median: 37 | M (n = 1242) F (n = 14) | MSM | NR | NR | Yes | RT-PCR |
| Vusirikala, A. et al. [52] | 2022 | Case report | United Kingdom | 45 | 45 | Median: 37 | M | GBMSM | HIV (n = 11) | Positive (n = 11) | Yes | RT-PCR |
| Authors | Number of Cases (N) | Symptoms and Findings in Physical Examination | Days from Systemic Symptoms to Appearance of Lesion | Localization of Skin Lesions | Evolution of Lesions | Treatment |
|---|---|---|---|---|---|---|
| Antinori, A. et al. [8] | 1 | No | NR | Genital, thorax and calf area. | Asynchronous | Ciprofloxacin, acyclovir, and benzylpenicillin |
| 2 | Fever | 3 | Anal, back, legs and foot sole. | Asynchronous | NR | |
| 3 | Fever | 3 | Anal, head, thorax, legs, arms, hand, and genital area. | Asynchronous | anti-inflammatories and antihistamines | |
| 4 | Myalgia | 2 | Genital and pubic area. | Asynchronous | NR | |
| Heskin, J. et al. [31] | 1 | Lymphadenopathy, fever, headache, and diarrhea. Perioral white patches and painful lesions with perianal blisters. | 1 | Perioral and perianal. | Asynchronous | Intravenous ceftriaxone |
| 2 | Lymphadenopathy, fever, headache, and diarrhea. Perioral papules, papules on the mons pubis and penile shaft that evolved into painful ulcers. | 2 | Genital, pubic and tongue, oral and buccal mucous membranes. | Asynchronous | Intravenous ceftriaxone, antibiotic therapy. | |
| Hammerschlag, Y. et al. [32] | 1 | Fever and general malaise | 3 | Penis, trunk, face, extremities, hand, calf, nasal throat. | Asynchronous | Intramuscular ceftriaxone, oral doxycycline, oral cephalexin, intravenous cephalorin and oral analgesia. |
| Minhaj, F.S. et al. [22] | 17 | Rash (n = 17), Fatigue or malaise (n = 13), Chills (n = 12), Lymphadenopathy (n = 9), Headache (n = 8), Fever (n = 7), Body aches (n = 6), Sore throat or cough (n = 5), Sweat (n = 4). | NR | Arm (n = 9), Trunk (n = 9), Leg (n = 8), Face (n = 7), Hand (n = 6), Perianal (n = 6), Oral (n = 5), Neck (n = 5), Genital (penis or vagina) (n = 4), Feet (n = 4). | Asynchronous | NR |
| Vivancos, R. et al. [33] | 86 | NR | NR | NR | NR | NR |
| Perez Duque, M. et al. [34] | 27 | Exanthema (n = 14), inguinal lymphadenopathy (n = 14), fever (n = 13), genital ulcers (n = 6) | NR | Anus (n = 14) and genitalia (n = 12) | Asynchronous | NR |
| Vallée, A. et al. [35] | 1 | Fever, severe fatigue, chills, myalgia, sore throat, severe anal pain, and lymphadenopathy. | 5 | None | Asynchronous | No specific treatment. |
| Oprea, C. et al. [36] | 1 | High fever (up to 39 degrees Celsius), chills, rectal pain, vesiculopustular rash, dysphagia, severe pain in the anorectal region, marked hyperemia of the pharynx, with pseudomembranous appearance, and palatal petechiae, aphthous ulcers, lymphadenopathy. | 4 | Anogenital, buttocks, neck, trunk, upper and lower limbs, and sole of one foot. | Asynchronous | Symptomatic, fluid, and topical treatment for aphthous ulcers and pharyngeal hyperemia. |
| Bížová, B. et al. [28] | 1 | High fever, chills, lymphadenopathy, rash, painless perianal erosions, and perianal umbilicated papules. | 3 | The perianal and left side of the body | Asynchronous | Antibiotic therapy |
| Patrocinio-Jesus, R. et al. [29] | 1 | Painless genital rash, fever, sore throat, macular rash, lymphadenopathy. | 2 | Genitals and hands | Asynchronous | No specific intervention |
| Basgoz, N. et al. [30] | 1 | Rectal pain, vesiculopustular rash, rectal bleeding, foul-smelling and mucopurulent discharge, fever, chills, lymphadenopathy, and swelling in the groin. | 3 | Perianal, penis, arms, and legs. | Asynchronous | Penicillin G benzathine, ceftriaxone, valacyclovir, doxycycline, and intravenous acyclovir. |
| Mileto, D. et al. [7] | 1 | Asthenia, fever, general malaise, anorexia, papular lesions on both elbows, ulcerated perianal lesion, pharyngodynia, bilateral inguinal lymphadenopathy. | 3 | Perianal, face, both elbows, trunk, buttock, and right foot. | Asynchronous | Dolutegravir, rilpivirine, isolated in a negative pressure room. |
| Girometti, N. et al. [37] | 54 | Fatigue (n = 36), fever (n = 31), myalgia (n = 16), sore throat (n = 11), lymphadenopathy (n = 30) and skin lesions (n = 54). | 3 | Skin (n = 54), genitalia (n = 33), perianal (n = 24), upper and lower extremities (n = 27), facial (n = 11), oropharyngeal (n = 4) and torso (n = 14). | Asynchronous | No specific treatment was recorded and all individuals improved clinically. |
| Noe, S. et al. [38] | 1 | General malaise, fever, arthralgia, myalgia and back pain, headache, dysphagia, and presence of white spots on his tonsils. | 2 | Tonsils, trunk, limbs, and head. | Asynchronous | No specific treatment was recorded. |
| 2 | Fever, fatigue, cough, inguinal lymphadenopathy, and anal pain. | 2 | Trunk | Asynchronous | No specific treatment was recorded. | |
| Jang, Y.R. et al. [39] | 1 | Headache, fever, rash, lymphadenopathy, and chills. | 3 | Penis, oropharynx, nasopharynx, face, abdomen, and trunk. | Asynchronous | No specific treatment was recorded. |
| Maronese, C.A. et al. [40] | 1 | Fever, headache, malaise, and lymphadenopathy. | 5 | Penis, scrotum, and extremities. | Asynchronous | No specific treatment was recorded. |
| Peiró-Mestres, A. et al. [41] | 1 | Myalgia, fatigue | NR | Arm, perianal area and trunk | Asynchronous | No specific treatment was recorded. |
| 2 | Odynophagia, general malaise | Genital area | Asynchronous | No specific treatment was recorded. | ||
| 3 | Myalgia, fever, Proctitis | Anal area | Asynchronous | No specific treatment was recorded. | ||
| 4 | Proctalgia, odynophagia, general malaise | Perianal, chest and trunk | Asynchronous | No specific treatment was recorded. | ||
| 5 | Fever, myalgia, general malaise | Chest and legs | Asynchronous | No specific treatment was recorded. | ||
| 6 | Fever, proctitis | Wrist, pectoral, fingers, hand and perianal area | Asynchronous | No specific treatment was recorded. | ||
| 7 | Headache, general malaise | Ulcerated ventral tongue | Asynchronous | No specific treatment was recorded. | ||
| 8 | General malaise, fever | Trunk and genital area | Asynchronous | No specific treatment was recorded. | ||
| 9 | Myalgia, general malaise | Genital lesions | Asynchronous | No specific treatment was recorded. | ||
| 10 | General malaise, myalgia, proctitis | Perianal area | Asynchronous | No specific treatment was recorded. | ||
| 11 | NR | Genital area | Asynchronous | No specific treatment was recorded. | ||
| 12 | Myalgia, general malaise | Genital and anal area | Asynchronous | No specific treatment was recorded. | ||
| Iñigo Martínez, J. et al. [42] | 508 | Exanthema (n = 498), fever (n = 324), lymphadenopathy (n = 311), asthenia (n = 238), myalgia (n = 185), headache (n = 162), odynophagia (n = 143), and proctitis (n = 81) | NR | Anogenital and/or perineal area (n = 359), legs and/or arms (n = 222), face (n = 177), chest and/or abdomen (n = 159), back (n = 132), palms and/or plants (n = 124). | Asynchronous | No specific treatment was recorded. |
| Selb, R. et al. [43] | 521 | NR | NR | NR | NR | NR |
| Tarín-Vicente, E.J. et al. [44] | 181 | Influenza-like illness (n = 147), Fever (n = 131), Headache (n = 96), Sore throat (n = 66) and lymphadenopathy (n = 153) | NR | Genital (n = 100), Perianal (n = 66), Oral ulcer (n = 45), Perioral (n = 51), Hands and feet (n = 108), Trunk and extremities (n = 104) | Asynchronous | No specific treatment was recorded. |
| Ogoina, D. et al. [45] | 16 | Fever (n = 9), Genital rash (n = 4), facial rash (n = 3) | NR | Genital (n = 13) | Asynchronous | No specific treatment was recorded. |
| Orviz, E. et al. [46] | 48 | Fever (n = 25), Asthenia (n = 32), Myalgia (n = 25), Inguinal lymphadenopathies (n = 30), Other location of lymphadenopathies (n = 9), Headache (n = 25), Proctitis (n = 13), Urethritis (n = 7), Rash (n = 4), Nasal congestion (n = 4), and Cough (n = 8) | NR | Vesicular-umbilicated skin lesions location (n = 45), Genitals (n = 26), Upper extremities (n = 20), Perianal (n = 17), Trunk (n = 16), Facial (n = 12), Periorally (n = 9), Lower extremities (n = 10), and Palms and soles (n = 2) | Asynchronous | No specific treatment was recorded. |
| Patel, A. et al. [47] | 197 | Mucocutaneous manifestations (n = 197), Fever (n = 122), Headache (n = 49), Fatigue/lethargy (n = 46), Myalgia (n = 62), Arthralgia (n = 21), Back pain (n = 21), Rectal pain or pain on defecation (n = 71), and Lymphadenopathy (n = 114) | NR | Face (n = 71), Trunk (n = 70), Arms/legs (n = 74), Hands/feet (n = 56), Genitals (n = 111), Anus or perianal area (n = 82), and Oropharyngeal (n = 27) | Asynchronous | No specific treatment was recorded. |
| Pfäfflin, F. et al. [48] | 1 | Fever, Perianal pain, Anal abscess, and Lymphadenopathy | NR | Limbs | Asynchronous | Ibuprofen |
| 2 | Fever, malaise, anal pain, and anal fissure | NR | Left arm | Asynchronous | Metamizole, tramadol, lidocaine | |
| 3 | Anal pain, Rectal ulcer, and proctitis | NR | Limbs | Asynchronous | Ibuprofen, metamizole, lidocaine | |
| 4 | Fatigue, Anal pain, and Anal ulcer | NR | Arms, trunk, genital | Asynchronous | Metamizole, lidocaine, Penicillin G benzathine, ceftriaxone | |
| 5 | Fever, malaise, myalgia, sweats, Anal pain, Inflammation of sigmoid, rectum and anal canal | NR | Head, neck, trunk, limbs | Asynchronous | Metamizole, lidocaine, Ceftriaxone, azithromycin | |
| 6 | Myalgia, fever, malaise, Anal pain, Anal ulcer, proctitis | NR | Legs | Asynchronous | Metamizole, lidocaine, Ceftriaxone, azithromycin | |
| Philpott, D. et al. [49] | 1195 | Rash (n = 1004), Fever (n = 596), Chills (n = 550), Lymphadenopathy (n = 545), Malaise (n = 531), Myalgia (n = 507), Headache (n = 469), Rectal pain (n = 201), Pus or blood in stools (n = 184), Abdominal pain (n = 96), Rectal bleeding (n = 90), Tenesmus (n = 90), and vomiting or nausea (n = 83) | NR | Genitals (n = 333), Arms (n = 284), Face (n = 276), Legs (n = 265), Perianal (n = 225), Mouth, lips, or oral mucosa (n = 179), Palms of hands (n = 157), Trunk (n = 156), Neck (n = 130), Head (n = 97), and Soles of feet (n = 77) | Asynchronous | No specific treatment was recorded. |
| Raccagni, A.R. et al. [50] | 36 | NR | NR | Genital (n = 13), Rectal (n = 18), cutaneous (n = 20) | Asynchronous | No specific treatment was recorded. |
| Rodríguez, B.S. et al. [51] | 1256 | Report of some cases (n = 530): Fever (n = 302), lymphadenopathy (n = 216), Asthenia (n = 224), Muscle pain (n = 167), Throat pain (n = 136), and Headache (n = 140) | NR | Report of some cases (n = 530): Anogenital (n = 355), other than anogenital or oro/peribuccal (n = 293) | Asynchronous | No specific treatment was recorded. |
| Vusirikala, A. et al. [52] | 45 | NR | NR | NR | Asynchronous | No specific treatment was recorded. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
León-Figueroa, D.A.; Barboza, J.J.; Garcia-Vasquez, E.A.; Bonilla-Aldana, D.K.; Diaz-Torres, M.; Saldaña-Cumpa, H.M.; Diaz-Murillo, M.T.; Cruz, O.C.-S.; Rodriguez-Morales, A.J. Epidemiological Situation of Monkeypox Transmission by Possible Sexual Contact: A Systematic Review. Trop. Med. Infect. Dis. 2022, 7, 267. https://doi.org/10.3390/tropicalmed7100267
León-Figueroa DA, Barboza JJ, Garcia-Vasquez EA, Bonilla-Aldana DK, Diaz-Torres M, Saldaña-Cumpa HM, Diaz-Murillo MT, Cruz OC-S, Rodriguez-Morales AJ. Epidemiological Situation of Monkeypox Transmission by Possible Sexual Contact: A Systematic Review. Tropical Medicine and Infectious Disease. 2022; 7(10):267. https://doi.org/10.3390/tropicalmed7100267
Chicago/Turabian StyleLeón-Figueroa, Darwin A., Joshuan J. Barboza, Edwin A. Garcia-Vasquez, D. Katterine Bonilla-Aldana, Milagros Diaz-Torres, Hortencia M. Saldaña-Cumpa, Melissa T. Diaz-Murillo, Olga Campos-Santa Cruz, and Alfonso J. Rodriguez-Morales. 2022. "Epidemiological Situation of Monkeypox Transmission by Possible Sexual Contact: A Systematic Review" Tropical Medicine and Infectious Disease 7, no. 10: 267. https://doi.org/10.3390/tropicalmed7100267
APA StyleLeón-Figueroa, D. A., Barboza, J. J., Garcia-Vasquez, E. A., Bonilla-Aldana, D. K., Diaz-Torres, M., Saldaña-Cumpa, H. M., Diaz-Murillo, M. T., Cruz, O. C. -S., & Rodriguez-Morales, A. J. (2022). Epidemiological Situation of Monkeypox Transmission by Possible Sexual Contact: A Systematic Review. Tropical Medicine and Infectious Disease, 7(10), 267. https://doi.org/10.3390/tropicalmed7100267