
The Impact of COVID-19 Quarantine on Tuberculosis and Diabetes Mellitus Cases: A Modelling Study





Abstract
:1. Introduction
2. Material and Methods
2.1. Mathematical Model
2.2. Data Fitting
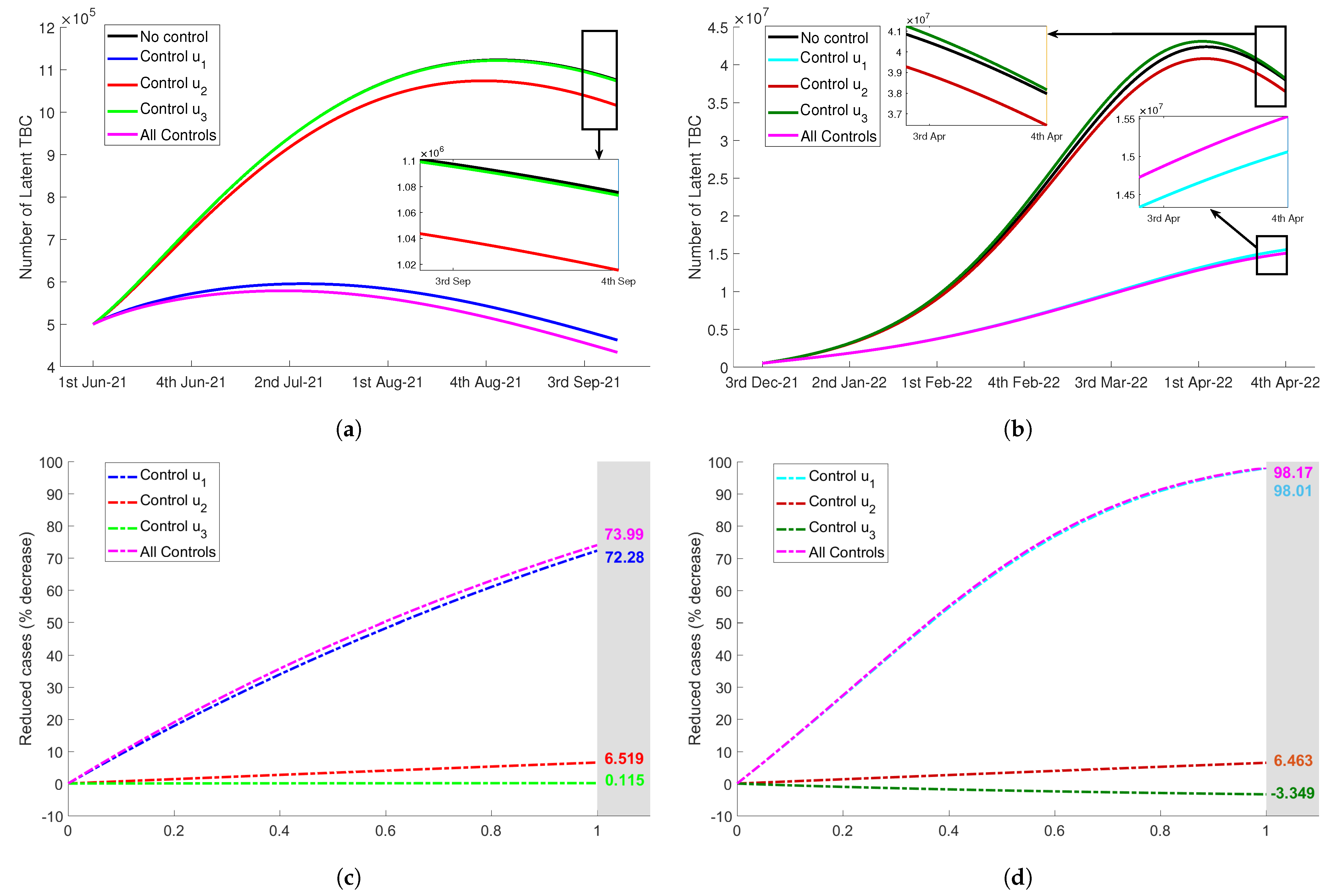
2.3. Control Strategies
- Control : proportion of awareness program for quarantined susceptible to restrict the interaction with tuberculosis suspects in the environment.
- Control : proportion of awareness program for latent tuberculosis by intensifying the latent identification and putting under treatment.
- Control : proportion of diagnosis program for infected tuberculosis by managing a specific team for diagnosis or optimizing the use of telemedicine.
- Control : proportion of awareness program for quarantined susceptible by implementing healthy lifestyle and exercising inside the house.
- Control : proportion of awareness program for diabetic people without complications by applying healthy diet and diet tracking in quarantine period.
3. Results
3.1. Numerical Simulation of Mathematical Model Accomodating Quarantine Process
3.2. Effect of Tuberculosis and Diabetes Control Strategies during COVID-19 Quarantine
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Description | Value | Unit | References |
|---|---|---|---|---|
| Human natural birth or mortality rate | (65 × 52) | week | [35,36,37] | |
| Rate of progression to infected from exposed | week | [38,39,40] | ||
| Mortality rate caused by COVID-19 infection | week | data | ||
| Recovery rate of infected and quarantined of COVID-19 | week | [40,41,42] | ||
| Rate of progression to infected from latent | week | [43,44] | ||
| Recovery rate of latent tuberculosis | week | [43,44] | ||
| Recovery rate of infected tuberculosis | week | [43] | ||
| Recovery rate of diagnosed tuberculosis | week | [43] | ||
| Mortality rate caused by tuberculosis infection | week | [45] | ||
| Probability of diabetic people developing complications | week | [46] | ||
| Probability of diabetic people recovered from complications | week | [46] | ||
| Mortality rate caused by diabetes mellitus | week | [46] |
Appendix A.2
Appendix A.3

Appendix A.4

References
- Anderson, D.E.; Sivalingam, V.; Kang, A.E.Z.; Ananthanarayanan, A.; Arumugam, H.; Jenkins, T.M.; Hadjiat, Y.; Eggers, M. Povidone-Iodine demonstrates rapid in vitro virucidal activity against SARS-CoV-2, the virus causing COVID-19 disease. Infect. Dis. Ther. 2020, 9, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.F.; Ho, Y.C. SARS-CoV-2: A storm is raging. J. Clin. Investig. 2020, 130, 2202–2205. [Google Scholar] [CrossRef] [PubMed]
- Sukandar, K.K.; Louismono, A.L.; Volisa, M.; Kusdiantara, R.; Fakhruddin, M.; Nuraini, N.; Soewono, E. A Prospective Method for Generating COVID-19 Dynamics. Computation 2022, 10, 107. [Google Scholar] [CrossRef]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 14 November 2022).
- Chiesa, V.; Antony, G.; Wismar, M.; Rechel, B. COVID-19 pandemic: Health impact of staying at home, social distancing and ’lockdown’ measures-a systematic review of systematic reviews. J. Public Health 2021, 43, e462–e481. [Google Scholar] [CrossRef] [PubMed]
- McQuaid, C.F.; Vassall, A.; Cohen, T.; Fiekert, K.; White, R.G. The impact of COVID-19 on TB: A review of the data. Int. J. Tuberc. Lung Dis. 2021, 25, 436–446. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Report 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Aznar, M.L.; Espinosa-Pereiro, J.; Saborit, N.; Jové, N.; Sánchez-Martinez, F.; Pérez-Recio, S.; Vitoria, A.; Sanjoaquin, I.; Gallardo, E.; Llenas-García, J.; et al. Impact of the COVID-19 pandemic on tuberculosis management in Spain. Int. J. Infect. Dis. 2021, 108, 300–305. [Google Scholar] [CrossRef]
- Runacres, A.; Mackintosh, K.A.; Knight, R.L.; Sheeran, L.; Thatcher, R.; Shelley, J.; McNarry, M.A. Impact of the COVID-19 pandemic on sedentary time and behaviour in children and adults: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 11286. [Google Scholar] [CrossRef]
- Eberle, C.; Stichling, S. Impact of COVID-19 lockdown on glycemic control in patients with type 1 and type 2 diabetes mellitus: A systematic review. Diabetol. Metab. Syndr. 2021, 13, 95. [Google Scholar] [CrossRef] [PubMed]
- Al-Rifai, R.H.; Pearson, F.; Critchley, J.A.; Abu-Raddad, L.J. Association between diabetes mellitus and active tuberculosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0187967. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Yasuda, K. Spiral dynamics inspired optimization. J. Adv. Comput. Intell. Intell. Inform. 2011, 15, 1116–1122. [Google Scholar] [CrossRef]
- Satuan Tugas Penanganan COVID-19. Available online: https://www.covid19.go.id/ (accessed on 10 July 2022).
- TB Indonesia Kementerian Kesehatan. Available online: https://www.tbindonesia.id/ (accessed on 10 July 2022).
- Lau, H.; Khosrawipour, P.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27, taaa037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzzetta, G.; Riccardo, F.; Marziano, V.; Poletti, P.; Trentini, F.; Bella, A.; Andrianou, X.; Del Manso, M.; Fabiani, M.; Bellino, S.; et al. Impact of a nationwide lockdown on SARS-CoV-2 transmissibility, Italy. Emerg. Infect. Dis. 2021, 27, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Megarbane, B.; Bourasset, F.; Scherrmann, J.M. Is lockdown effective in limiting SARS-CoV-2 epidemic progression? A cross-country comparative evaluation using epidemiokinetic tools. J. Gen. Intern. Med. 2021, 36, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Novelli, G.; Colona, V.L.; Pandolfi, P.P. A focus on the spread of the delta variant of SARS-CoV-2 in India. Indian J. Med. Res. 2021, 153, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Gowrisankar, A.; Priyanka, T.M.C.; Banerjee, S. Omicron: A mysterious variant of concern. Eur. Phys. J. Plus 2022, 137, 100. [Google Scholar] [CrossRef] [PubMed]
- Lyngse, F.P.; Mortensen, L.H.; Denwoood, M.J.; Christiansen, L.E.; Moller, C.H.; Skov, R.L.; Spiess, K.; Fomsgaard, A.; Lassauniere, R.; Rasmussen, M.; et al. SARS-CoV-2 Omicron VOC Transmission in Danish Households. medRxiv 2021, 21268278. [Google Scholar]
- Chaguza, C.; Coppi, A.; Earnest, R.; Ferguson, D.; Kerantzas, N.; Warner, F.; Young, H.P.; Breban, M.I.; Billig, K.; Koch, R.T.; et al. Rapid emergence of SARS-CoV-2 Omicron variant is associated with an infection advantage over Delta in vaccinated persons. Med 2022, 3, 325–334.e4. [Google Scholar] [CrossRef] [PubMed]
- Migliori, G.B.; Thong, P.M.; Akkerman, O.; Alffenaar, J.W.; Alvarez-Navascues, F.; Assao-Neino, M.M.; Bernard, P.V.; Biala, J.S.; Blanc, F.X.; Bogorodskaya, E.M.; et al. Worldwide effects of coronavirus disease pandemic on tuberculosis services, January-April 2020. Emerg. Infect. Dis. 2020, 26, 2709–2712. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.J.; Ritchey, M.D.; Goodman, A.B.; Dias, T.; Twentyman, E.; Fuld, J.; Schieve, L.A.; Imperatore, G.; Benoit, S.R.; Kite-Powell, A.; et al. Potential indirect effects of the COVID-19 pandemic on use of emergency departments for acute life-threatening conditions—United States, January–May 2020. Am. J. Transpl. 2020, 20, 2612–2617. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.W.M.; Migliori, G.B.; Ravligione, M.; MacGregor-Skinner, G.; Sotgiu, G.; Alffenaar, J.W.; Tiberi, S.; Adlhoch, C.; Alonzi, T.; Archuleta, S.; et al. Epidemic and pandemic viral infections: Impact on tuberculosis and the lung. Eur. Respir. J. 2020, 56, 2001727. [Google Scholar] [CrossRef] [PubMed]
- Esmail, H.; Cobelens, F.; Goletti, D. Transcriptional biomarkers for predicting development of tuberculosis: Progress and clinical considerations. Eur. Respir. J. 2020, 55, 1901957. [Google Scholar] [CrossRef] [Green Version]
- Migliori, G.B.; Thong, P.M.; Alffenaar, J.W.; Denholm, J.; Tadolini, M.; Alyaquobi, F.; Blanc, F.X.; Buonsenso, D.; Cho, J.G.; Codecasa, L.R.; et al. Gauging the impact of the COVID-19 pandemic on tuberculosis services: A global study. Eur. Respir. J. 2021, 58, 2101786. [Google Scholar] [CrossRef]
- Programmatic Innovations to Address Challenges in Tuberculosis Prevention and Care during the COVID-19 Pandemic. Available online: https://apps.who.int/iris/handle/10665/341307 (accessed on 10 July 2022).
- Augustynowicz-Kopec, E.; Jagielski, T.; Kozinska, M.; Kremer, K.; Soolingen, D.V.; Bielecki, J.; Zwolska, Z. Transmission of tuberculosis within family-households. J. Infect. 2012, 64, 596–608. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, D.J.; Kendall, C.W.; Marchie, A.; Jenkins, A.L.; Kendall, C.W.; Augustin, L.S.A.; Ludwig, D.S.; Barnard, N.D.; Anderson, J.W. Type 2 diabetes and the vegetarian diet. Am. J. Clin. Nutr. 2003, 78, 610S–616S. [Google Scholar] [CrossRef] [Green Version]
- Bendall, C.L.; Mayr, H.L.; Opie, R.S.; Bes-Rastrollo, M.; Itsiopoulos, C.; Thomas, C.J. Central obesity and the Mediterranean diet: A systematic review of intervention trials. Crit. Rev. Food Sci. Nutr. 2018, 58, 3070–3084. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American diabetes association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riddell, M.C.; Iscoe, K.E. Physical activity, sport, and pediatric diabetes. Pediatr. Diabetes 2006, 7, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.J.; Torres, D.F.M. Optimal control for a tuberculosis model with reinfection and post-exposure interventions. Math. Biosci. 2013, 244, 154–164. [Google Scholar] [CrossRef] [Green Version]
- Fauzi, I.S.; Fakhruddin, M.; Nuraini, N.; Wijaya, K.P. Comparison of dengue transmission in lowland and highland area: Case study in Semarang and Malang, Indonesia. Commun. Biomath. Sci. 2019, 2, 23–37. [Google Scholar] [CrossRef]
- Nuraini, N.; Fauzi, I.S.; Fakhruddin, M.; Sopaheluwakan, A.; Soewono, E. Climate-based dengue model in Semarang, Indonesia: Predictions and descriptive analysis. Infect. Dis. Model. 2021, 6, 598–611. [Google Scholar] [CrossRef]
- Gill, B.S.; Jayaraj, V.J.; Singh, S.; Ghazali, S.M.; Cheong, Y.L.; Md Iderus, N.H.; Sundram, B.M.; Aris, T.B.; Mohd Ibrahim, H.; Hong, B.H.; et al. Modelling the effectiveness of epidemic control measures in preventing the transmission of COVID-19 in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 5509. [Google Scholar] [CrossRef]
- Fauzi, I.S.; Nuraini, N.; Ayu, R.W.S.; Lestari, B.W. Temporal trend and spatial clustering of the dengue fever prevalence in West Java, Indonesia. Heliyon 2022, 8, e10350. [Google Scholar] [CrossRef] [PubMed]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. The incubation period of 2019-nCoV infections among travellers from Wuhan, China. Eurosurveillance 2020, 25, 2000062. [Google Scholar] [PubMed] [Green Version]
- Read, J.M.; Bridgen, J.R.; Cumming, D.A.; Ho, A.; Jewell, C.P. Novel coronavirus 2019-nCoV: Early estimation of epidemiological parameters and epidemic forecasts. Philosopical Trans. R. Soc. Biol. Sci. 2021, 376, 20200265. [Google Scholar] [CrossRef]
- Fuady, A.; Nuraini, N.; Sukandar, K.K.; Lestari, B.W. Targeted vaccine allocation could increase the COVID-19 vaccine benefits amidst its lack of availability: A mathematical modeling study in Indonesia. Vaccines 2021, 9, 462. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Bi, Y.; Liu, Y. Modeling and dynamic analysis of tuberculosis in mainland China from 1998 to 2017: The effect of DOTS strategy and further control. Theor. Biol. Med. Model. 2020, 17, 1–10. [Google Scholar] [CrossRef]
- Li, J. The spread and prevention of tuberculosis. Chin. Remedies Clin. 2013, 13, 482–483. [Google Scholar]
- Tewa, J.J.; Bowong, S.; Mewoli, B. Mathematical analysis of two-patch model for the dynamical transmission of tuberculosis. Appl. Math. Model. 2012, 36, 2466–2485. [Google Scholar] [CrossRef]
- Widyaningsih, P.; Affan, R.C.; Saputro, D.R.S. A mathematical model for the epidemiology of diabetes mellitus with lifestyle and genetic factors. J. Phys. Conf. Ser. 2018, 1028, 012110. [Google Scholar] [CrossRef]







| Parameter | Description | Level of Quarantine | ||
|---|---|---|---|---|
| No | Micro | Macro | ||
| Quarantine rate from susceptible to quarantined susceptible | 0.00 | 0.30 | 0.75 | |
| Quarantine rate from infected coronavirus to quarantined infected | 0.95 | 0.85 | 0.75 | |
| Parameter | Description | Delta (95% CI) | Omicron (95% CI) |
|---|---|---|---|
| Infection rate of susceptible by contact with infected | |||
| Infection rate of susceptible by contact with quarantined infected | |||
| Infection rate of quarantined susceptible by contact with infected | |||
| Infection rate of quarantined susceptible by contact with quarantined infected | |||
| Infection rate of susceptible by contact with infected TB | |||
| Infection rate of susceptible by contact with diagnosed TB | |||
| Infection rate of quarantined susceptible by contact with infected TB | |||
| Infection rate of quarantined susceptible by contact with diagnosed TB | |||
| Diagnosis rate of infected TB | |||
| Probability of susceptible developing diabetes | |||
| Probability of quarantined susceptible developing diabetes |
| Variant | Indicator | No Quarantine | Micro Quarantine | Macro Quarantine |
|---|---|---|---|---|
| Delta (B.1.617.2) | Total infected individuals in 17 weeks | 6,691,270 | 3,246,557 | 2,397,179 |
| Peak of infection | 4th week of July 2021 | 3rd week of July 2021 | 2nd week of July 2021 | |
| Highest potential number of cases | 734,323 | 386,249 | 288,169 | |
| Number of cases at the end of observation | 117,673 | 16,968 | 9201 | |
| Percentage of reduced cases | - | 51.48% | 64.17% | |
| Omicron (B.1.1.529) | Total infected individuals in 19 weeks | 11,188,961 | 3,383,183 | 2,282,320 |
| Peak of infection | 1st week of March 2022 | 4th week of February 2022 | 3th week of February 2022 | |
| Highest potential number of cases | 1,382,465 | 426,239 | 286,566 | |
| Number of cases at the end of observation | 88,804 | 4155 | 2021 | |
| Percentage of reduced cases | - | 69.76% | 79.60% |
| Variant | Compartment | No Quarantine | Micro Quarantine | Macro Quarantine |
|---|---|---|---|---|
| Delta (B.1.617.2) | Infected tuberculosis | |||
| Diagnosed tuberculosis | ||||
| Diabetes without complications | ||||
| Diabetes with complications | ||||
| Omicron (B.1.1.529) | Infected tuberculosis | |||
| Diagnosed tuberculosis | ||||
| Diabetes without complications | ||||
| Diabetes with complications |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuraini, N.; Fauzi, I.S.; Lestari, B.W.; Rizqina, S. The Impact of COVID-19 Quarantine on Tuberculosis and Diabetes Mellitus Cases: A Modelling Study. Trop. Med. Infect. Dis. 2022, 7, 407. https://doi.org/10.3390/tropicalmed7120407
Nuraini N, Fauzi IS, Lestari BW, Rizqina S. The Impact of COVID-19 Quarantine on Tuberculosis and Diabetes Mellitus Cases: A Modelling Study. Tropical Medicine and Infectious Disease. 2022; 7(12):407. https://doi.org/10.3390/tropicalmed7120407
Chicago/Turabian StyleNuraini, Nuning, Ilham Saiful Fauzi, Bony Wiem Lestari, and Sila Rizqina. 2022. "The Impact of COVID-19 Quarantine on Tuberculosis and Diabetes Mellitus Cases: A Modelling Study" Tropical Medicine and Infectious Disease 7, no. 12: 407. https://doi.org/10.3390/tropicalmed7120407
APA StyleNuraini, N., Fauzi, I. S., Lestari, B. W., & Rizqina, S. (2022). The Impact of COVID-19 Quarantine on Tuberculosis and Diabetes Mellitus Cases: A Modelling Study. Tropical Medicine and Infectious Disease, 7(12), 407. https://doi.org/10.3390/tropicalmed7120407