
Clinical-Epidemiological Characteristics and Outcomes of Latent Tuberculosis Treatment at a Tertiary Center in Central-West Brazil from 2017 to 2019

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population and Location
2.3. Inclusion Criteria
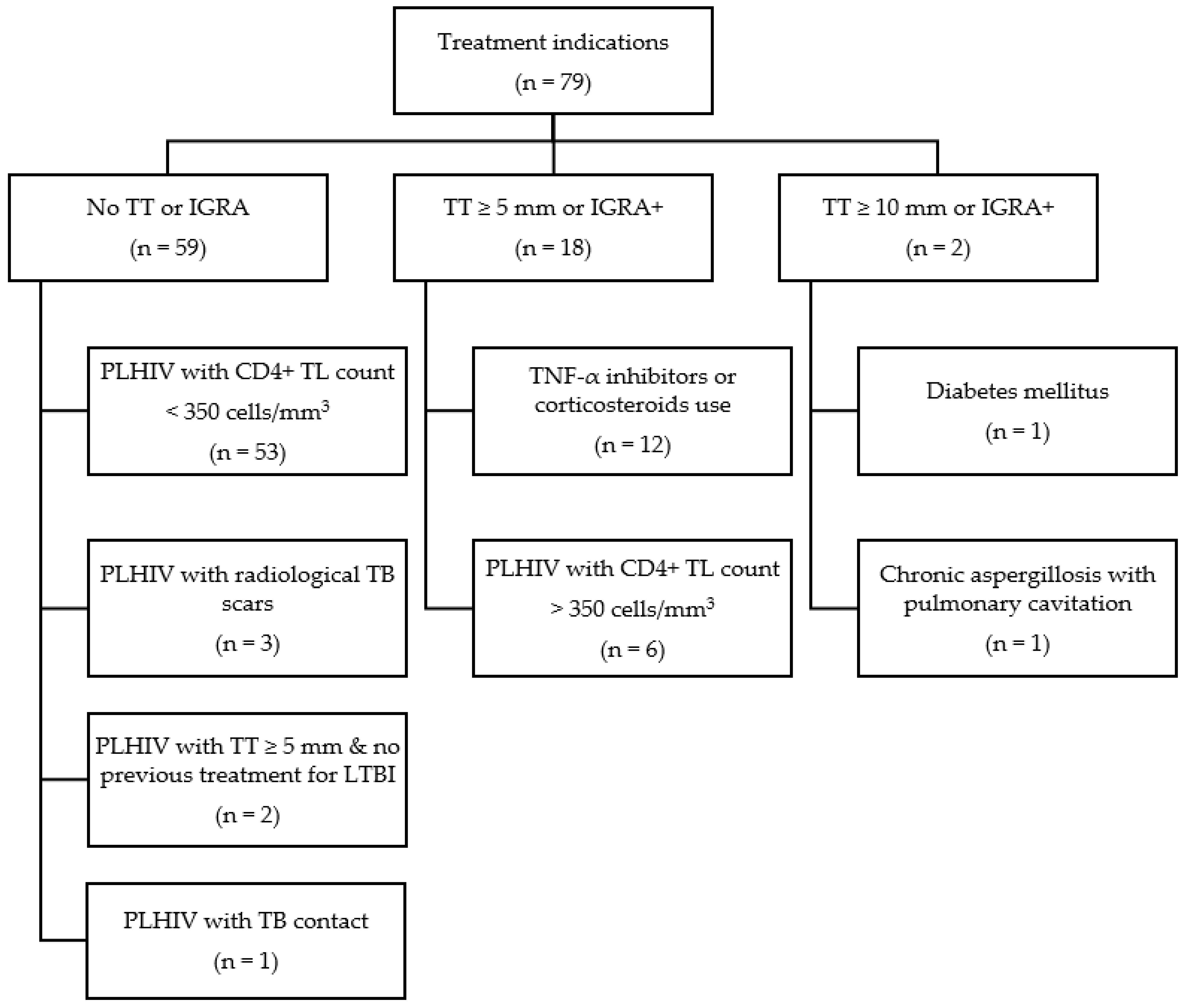
- (1)
- People living with HIV/AIDS (PLHIV) with:
- -
- CD4+ T lymphocyte count (CD4+ TL) of <350 cells/mm3, regardless of TT;
- -
- A TT of ≥5 mm; IGRA-positive;
- -
- A plain chest radiograph showing a TB scar without prior treatment;
- -
- A history of pulmonary TB contact.
- (2)
- Patients with a TT of ≥5 mm or who were IGRA-positive with the following risk factors:
- -
- Treatment with tumor necrosis factor-alpha (TNF-α) inhibitors or other immunosuppressive therapies, including corticosteroids (prednisone > 15 mg/day for >1 month);
- -
- A history of pulmonary TB contact;
- -
- On pre- or post-transplantation immunosuppressive therapy.
- (3)
- Patients with a TT of ≥10 mm or who were IGRA-positive with any of the risk factors below:
- -
- Silicosis, head and neck or hematological neoplasms, renal failure on dialysis, diabetes mellitus (DM), low weight, active smoking, and isolated calcification identified on plain chest radiography.
- (4)
- Patients with TT conversion (10 mm increment from the first to the second measurement).
2.4. Exclusion Criteria
2.5. Data Collection
- Sociodemographic data, including sex, age, self-declared ethnicity, and educational level;
- The patients’ daily habits and health history, such as smoking, previous Bacillus Calmette–Guérin (BCG) vaccination, the presence of comorbidities such as HIV infection, chronic kidney disease, DM, neoplasm, and hematological disease, the transplant schedule, and the use of immunosuppressants (TNF-α inhibitors and corticosteroids);
- Plain chest radiographic description;
- Laboratory test results;
- The proposed treatment regime.
2.6. Statistical Analysis
2.7. Ethical Aspects
3. Results
3.1. Socio-Epidemiological Aspects
3.2. Diagnostic Tests
3.3. Risk Factors for Active TB
3.4. Treatment Indications
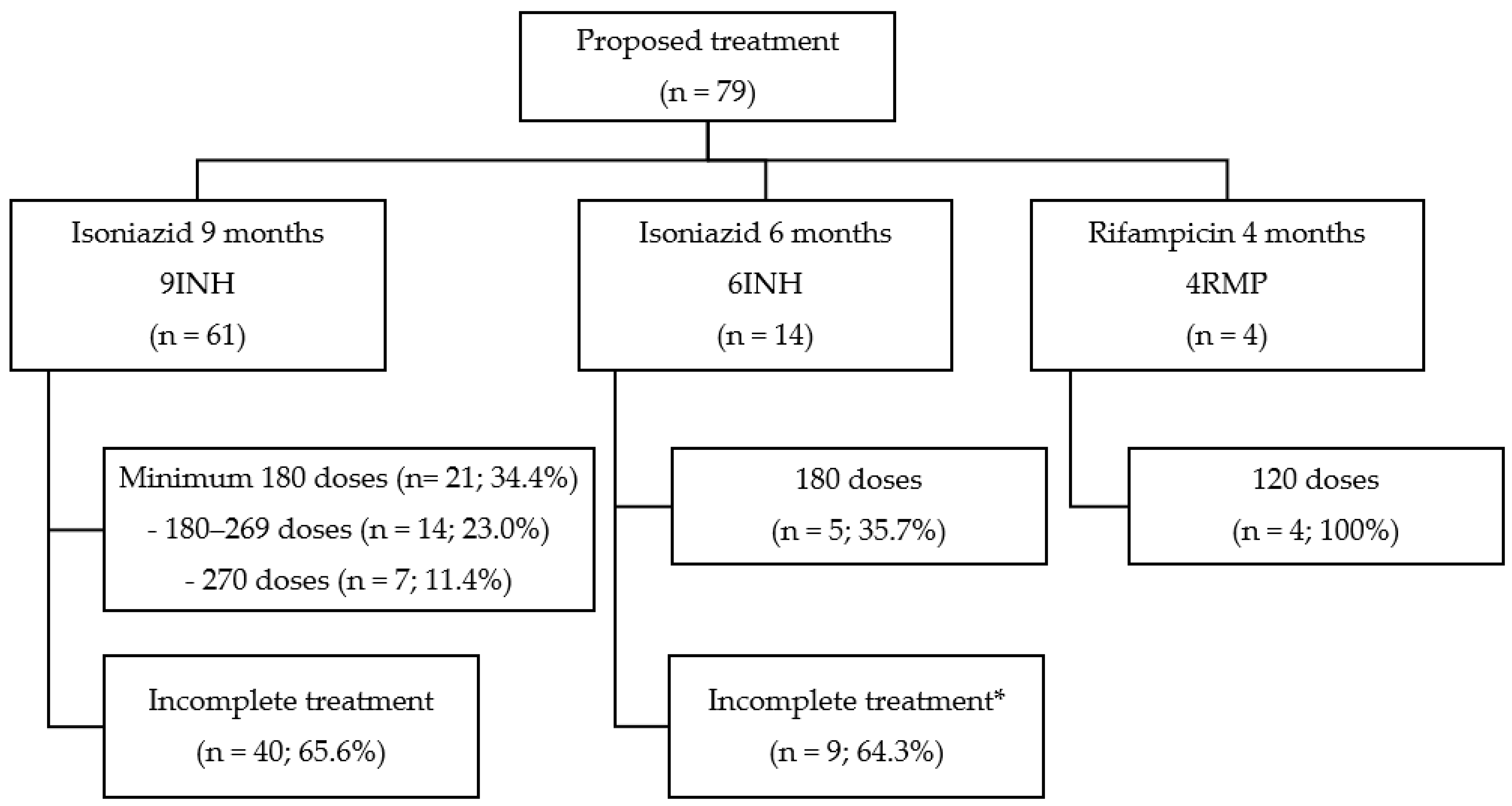
3.5. Proposed Treatments
3.6. Adverse Events
3.7. Active TB after Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anton, C.; Machado, F.D.; Ramirez, J.M.A.; Bernardi, R.M.; Palominos, P.E.; Brenol, C.V.; Mello, F.C.Q.; Silva, D.R. Latent tuberculosis infection in patients with rheumatic diseases. J. Bras. Pneumol. 2019, 45, e20190023. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Report 2021; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports (accessed on 17 August 2022).
- Aguiar, F.S.; Mello, F.C.Q. Latent tuberculosis and the use of immunomodulatory agents. J. Bras. Pneumol. 2019, 45, e20190361. [Google Scholar] [CrossRef] [PubMed]
- Shahid, N.U.A.; Naguit, N.; Jakkoju, R.; Laeeq, S.; Reghefaoui, T.; Zahoor, H.; Yook, J.H.; Rizwan, M.; Mohammed, L. Use of isoniazid monotherapy in comparison to rifamycin-based regimen for the treatment of patients with latent tuberculosis: A systematic review. Cureus 2022, 14, e25083. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Latent Tuberculosis Infection: Updated and Programmatic Guidelines for Consolidated Management; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/publications/i/item/9789241550239 (accessed on 8 July 2022).
- Ministério da saúde: Brasil. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis Coordenação-Geral de Vigilância das Doenças de Transmissão Respiratória de Condições Crônicas; Nota Informativa Nº 5/2021-CGDR/.DCCI/SVS/MS, de 06 de julho de 2021; Ministério da Saúde: Brasília, Brazil, 2021. Available online: https://www.saude.go.gov.br/files/sistemas/silt/NOTA-INFORMATIVA-N-5-RIFAPENTINA.pdf (accessed on 29 July 2022).
- Ministério da Saúde: Brasil; Secretaria de Vigilância em Saúde; Departamento de Vigilância Epidemiológica. Programa Nacional de Controle da Tuberculose. In Manual de Recomendações para o Controle da Tuberculose no Brasil; Ministério da Saúde: Brasília, Brazil, 2022. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/publicacoes-svs/tuberculose (accessed on 25 May 2022).
- Santos, D.T.D.; Garcia, M.C.; Costa, A.A.N.F.D.; Pieri, F.M.; Meier, D.A.P.; Albanese, S.P.R.; Arcêncio, R.A.; Dessunti, E.M. Latent tuberculosis infection in persons with HIV/AIDS, associated factors, and progression to active disease in a city in southern Brazil. Cad. Saude Publica 2017, 33, e00050916. [Google Scholar] [CrossRef] [Green Version]
- Ting, W.Y.; Huang, S.F.; Lee, M.C.; Lin, Y.Y.; Lee, Y.C.; Feng, J.Y.; Su, W.J. Gender disparities in latent tuberculosis infection in high-risk individuals: A cross-sectional study. PLoS ONE 2014, 9, e110104. [Google Scholar] [CrossRef]
- Goletti, D.; Navarra, A.; Petruccioli, E.; Cimaglia, C.; Compagno, M.; Cuzzi, G.; De Carli, G.; Fondaco, L.; Franzetti, F.; Giannetti, A.; et al. Latent tuberculosis infection screening in persons newly-diagnosed with HIV infection in Italy: A multicentre study promoted by the Italian Society of Infectious and Tropical Diseases. Int. J. Infect. Dis. 2020, 92, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Dessunti, E.; Meier, D.; Donath, B.; Costa, A. Latent tuberculosis infection: Treatment adherence and case progress. Rev. Enferm. UERJ 2013, 21, 711–717. [Google Scholar]
- Ping, P.A.; Zakaria, R.; Islam, M.A.; Yaacob, L.H.; Muhamad, R.; Mohamad, W.M.Z.W.; Yusoff, H.M. Prevalence and risk factors of latent tuberculosis infection (LTBI) in patients with type 2 diabetes mellitus (T2DM). Int. J. Environ. Res. Public Health 2021, 18, 305. [Google Scholar] [CrossRef]
- Ministério da Saúde: Brasil. Secretaria de Vigilância em Saúde. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. In Boletim Epidemiológico da Tuberculose; Ministério da Saúde: Brasília, Brazil, 2022. Available online: www.aids.gov.br/pt-br/pub/2022/boletim-epidemiologico-de-tuberculose-2022 (accessed on 21 July 2022).
- Teixeira, A.Q.; Samico, I.C.; Martins, A.B.; Galindo, J.M.; Montenegro, R.D.A.; Schindler, H.C. Tuberculose: Conhecimento e adesão às medidas profiláticas em indivíduos contatos da cidade do Recife, Pernambuco, Brasil. Cad. Saúde Colet 2020, 28, 116–129. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.W.; Kim, J.S. Treatment of latent tuberculosis infection and its clinical efficacy. Tuberc. Respir. Dis. 2018, 81, 6–12. [Google Scholar] [CrossRef]
- Devalraju, K.P.; Neela, V.S.K.; Krovvidi, S.S.; Vankayalapati, R.; Valluri, V.L. Defective expansion and function of memory like natural killer cells in HIV+ individuals with latent tuberculosis infection. PLoS ONE 2021, 16, e0257185. [Google Scholar] [CrossRef] [PubMed]
- Bares, S.H.; Swindells, S. Latent tuberculosis and HIV infection. Curr. Infect. Dis. Rep. 2020, 22, 17. [Google Scholar] [CrossRef]
- Souza, A.B.; Arriaga, M.B.; Amorim, G.; Araújo-Pereira, M.; Nogueira, B.M.F.; Queiroz, A.T.L.; Figueiredo, M.C.; Rocha, M.S.; Benjamin, A.; Moreira, A.S.R.; et al. Determinants of losses in the latent tuberculosis infection cascade of care in Brazil. BMJ Glob. Health 2021, 6, e005969. [Google Scholar] [CrossRef]
- Zhang, Z.; Fan, W.; Yang, G.; Xu, Z.; Wang, J.; Cheng, Q.; Yu, M. Risk of tuberculosis in patients treated with TNF-alpha antagonists: A systematic review and meta-analysis of randomised controlled trials. BMJ Open 2017, 7, e012567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministério da saúde: Brasil. Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis Coordenação-Geral de Vigilância das Doenças de Transmissão Respiratória de Condições Crônicas; Nota informativa Nº 2/2022-CGDR/DCCI/SVS/MS, de 08 de fevereiro de 2022; Ministério da Saúde: Brasília, Brazil, 2022. Available online: https://www.gov.br/aids/pt-br/centrais-de-conteudo/copy_of_notas-informativas/2022/ni_02-2022_recomendacoesigra_assistencia.pdf (accessed on 15 June 2022).
- Zhou, G.; Luo, Q.; Luo, S.; Teng, Z.; Ji, Z.; Yang, J.; Wang, F.; Wen, S.; Ding, Z.; Li, L.; et al. Interferon-γ release assays or tuberculin skin test for detection and management of latent tuberculosis infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2020, 20, 1457–1469. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Dorman, S.E. Latent tuberculosis infection. N. Engl. J. Med. 2021, 385, 2271–2280. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.; Johnston, J. Treatment of latent tuberculosis infection. Curr. Treat. Options Infect. Dis. 2017, 9, 371–379. [Google Scholar] [CrossRef] [Green Version]
- McClintock, A.H.; Eastment, M.; McKinney, C.M.; Pitney, C.L.; Narita, M.; Park, D.R.; Dhanireddy, S.; Molnar, A. Treatment completion for latent tuberculosis infection: A retrospective cohort study comparing 9 months of isoniazid, 4 months of rifampin and 3 months of isoniazid and rifapentine. BMC Infect. Dis. 2017, 17, 146. [Google Scholar] [CrossRef] [Green Version]
- Menzies, D.; Adjobimey, M.; Ruslami, R.; Trajman, A.; Sow, O.; Kim, H.; Baah, J.O.; Marks, G.B.; Long, R.; Hoeppner, V.; et al. Four months of rifampin or nine months of isoniazid for latent tuberculosis in adults. N. Engl. J. Med. 2018, 379, 440–453. [Google Scholar] [CrossRef]
- Picone, C.M.; Freitas, A.C.; Gutierrez, E.B.; Avelino-Silva, V.I. Access and adherence to isoniazid preventive therapy and occurrence of active TB in a cohort of people living with HIV: A retrospective cohort study in Sao Paulo, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2020, 62, e8. [Google Scholar] [CrossRef] [Green Version]
- Secretaria de Estado da Saúde. Superintendência de Vigilância em Saúde. Coordenação de Doenças Negligenciadas. Sistema de Informação da Infecção Latente da Tuberculose. In Situação de Encerramento dos Casos de ILTB em Goiás; Secretaria de Estado da Saúde: Goiás, Brasil, 2022. Available online: www.saude.go.gov.br (accessed on 29 August 2022).
- López, G.; Wood, M.; Ayesta, F.J. 10 years of innovation in the treatment of latent tuberculosis infection: A comparison between standard and short course therapies in directly observed therapy. Rev. Esp. Sanid. Penit. 2011, 13, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.R.; Trajman, A.; Cook, V.J.; Johnston, J.C.; Adjobimey, M.; Ruslami, R.; Eisenbeis, L.; Fregonese, F.; Valiquette, C.; Benedetti, A.; et al. Adverse events in adults with latent tuberculosis infection receiving daily rifampicin or isoniazid: Post-hoc safety analysis of two randomised controlled trials. Lancet Infect. Dis. 2020, 20, 318–329. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total LTBT (n = 79) n (%) | * Complete Treatment (n = 30, 38%) n (%) | Incomplete Treatment (n = 49, 62%) n (%) | p |
|---|---|---|---|---|
| Male sex (n = 54) | 54 (68.4) | 23 (42.6) | 31 (57.4) | 0.160 |
| Age (years) (n = 79)—median (IQR) | 40 (30–51) | 40 (28–52) | 40 (30–51) | 0.973 |
| <30 | 21 (26.6) | 9 (42.9) | 12 (57.1) | |
| 30–60 | 56 (70.9) | 20 (35.7) | 36 (64.3) | |
| >60 | 2 (2.5) | 1 (50.0) | 1 (50) | |
| Self-reported race/ethnicity (n = 55) | 0.790 | |||
| White | 26 (47.3) | 9 (34.6) | 17 (65.4) | |
| Mixed race | 21 (38.2) | 9 (42.9) | 12 (57.1) | |
| Black | 8 (14.5) | 4 (50.0) | 4 (50.0) | |
| Years of education (n = 43) | 0.159 | |||
| ≤12 years | 34 (79.1) | 16 (47.1) | 18 (52.9) | |
| >12 years | 9 (20.9) | 3 (33.3) | 6 (66.7) | |
| Type of entrance (n = 78) | 0.104 | |||
| New case | 73 (92.4) | 26 (35.6) | 47 (64.4) | |
| Re-entry following a change in the treatment scheme | 1 (1.3) | 0 (0.0) | 1 (100.0) | |
| Risk factors for active TB (n = 79) | ||||
| HIV infection | 65 (82.3) | 24 (36.9) | 41 (63.1) | 0.449 |
| Immunosuppressants | 12 (15.2) | 6 (50.0) | 6 (50.0) | 0.268 |
| Active smoking | 12 (15.2) | 4 (33.3) | 8 (66.7) | 0.719 |
| DM | 4 (5.1) | 3 (75.0) | 1 (25.0) | 0.151 |
| Chronic kidney disease | 3 (3.8) | 2 (66.7) | 1 (33.3) | 0.321 |
| CD4+ TL—median (IQR) (n = 65) | 257 (105–313) | 251 (149–333) | 239 (68–312) | 0.623 |
| ≤350 cells/mm3 | 55 (84.6) | 35 (63.6) | 20 (36.4) | 1.000 |
| >350 cells/mm3 | 10 (15.4) | 6 (60) | 4 (40) | |
| ART (n = 62) | 0.121 | |||
| TDF + 3TC + DTG | 44 (71.0) | 19 (43.2) | 25 (56.8) | |
| Other | 18 (29.0) | 4 (22.2) | 14 (77.8) | |
| BCG vaccine (n = 79) | 0.772 | |||
| Yes | 49 (62.0) | 18 (36.7) | 31 (63.3) | |
| No/not known | 30 (38.0) | 12 (40.0) | 18 (60.0) | |
| Plain chest radiograph description (n = 57) | 0.777 | |||
| Normal | 45 (78.9) | 17 (37.8) | 28 (62.2) | |
| Altered | 12 (21.1) | 4 (33.3) | 8 (66.7) | |
| Ruling out active TB (n = 79) | 0.534 | |||
| Yes | 22 (27.8) | 8 (36.4) | 14 (63.6) | |
| Ignored/unrealized | 57 (72.2) | 22 (38.6) | 35 (61.4) | |
| TT result (n = 42)—median (IQR) | 7 (0–13) | 9.5 (0–14) | 6 (0–10) | 0.641 |
| Recommendation for LTBT (n = 79) | 0.500 | |||
| No TT or IGRA | 59 (74.7) | 22 (37.3) | 37 (62.7) | |
| TT > 5 mm or IGRA-positive | 18 (22.8) | 7 (38.9) | 11 (61.1) | |
| TT >10 mm or IGRA-positive | 2 (2.5) | 1 (50.0) | 1 (50.0) | |
| Proposed treatment (n = 79) | 0.161 | |||
| INH 300 mg, 9 months | 61 (77.2) | 21 (34.4) | 40 (65.6) | 0.009 |
| INH 300 mg, 6 months | 14 (17.7) | 5 (35.7) | 9 (64.3) | |
| RMP 600 mg, 4 months | 4 (5.1) | 4 (100.0) | 0 (0.0) | |
| Drug dispensing median (IQR) | 145 (90–195) | 210 (180–270) | 99 (90–120) | 0.000 |
| Adverse effects (n = 15) | 15 (19) | 5 (33.3) | 10 (66.7) | 0.681 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borges, M.A.S.B.; Cunha, I.D.; Candini, L.H.; de Souza, V.A.; da Costa, P.S.S. Clinical-Epidemiological Characteristics and Outcomes of Latent Tuberculosis Treatment at a Tertiary Center in Central-West Brazil from 2017 to 2019. Trop. Med. Infect. Dis. 2022, 7, 432. https://doi.org/10.3390/tropicalmed7120432
Borges MASB, Cunha ID, Candini LH, de Souza VA, da Costa PSS. Clinical-Epidemiological Characteristics and Outcomes of Latent Tuberculosis Treatment at a Tertiary Center in Central-West Brazil from 2017 to 2019. Tropical Medicine and Infectious Disease. 2022; 7(12):432. https://doi.org/10.3390/tropicalmed7120432
Chicago/Turabian StyleBorges, Moara Alves Santa Bárbara, Iago Dib Cunha, Luís Henrique Candini, Vitor Alves de Souza, and Paulo Sérgio Sucasas da Costa. 2022. "Clinical-Epidemiological Characteristics and Outcomes of Latent Tuberculosis Treatment at a Tertiary Center in Central-West Brazil from 2017 to 2019" Tropical Medicine and Infectious Disease 7, no. 12: 432. https://doi.org/10.3390/tropicalmed7120432
APA StyleBorges, M. A. S. B., Cunha, I. D., Candini, L. H., de Souza, V. A., & da Costa, P. S. S. (2022). Clinical-Epidemiological Characteristics and Outcomes of Latent Tuberculosis Treatment at a Tertiary Center in Central-West Brazil from 2017 to 2019. Tropical Medicine and Infectious Disease, 7(12), 432. https://doi.org/10.3390/tropicalmed7120432